
Abstract
Abstract
Introduction:
Nephroureterectomy (NUx) with full bladder cuff excision is the gold-standard treatment for upper urinary tract urothelial cancer. Although minimally invasive techniques for NUx have demonstrated comparable outcomes to those of the open technique, the robotic technique is limited by the need for intraoperative patient repositioning and robot redocking to manage the distal ureter and bladder cuff. We describe our novel technique of robotic NUx that allows for complete access to the kidney and full bladder cuff excision.
Patients and Methods:
This modified technique was performed on a consecutive series of patients undergoing robotic NUx for upper urinary tract urothelial cancer from August 2012 to January 2014. Operative parameters and pathologic data were recorded, and patients were followed up for surveillance. After insufflation, the robotic trocars are placed in a standardized fashion, allowing for a one-time switch of instruments to facilitate distal ureteral dissection and a wide bladder cuff excision without patient repositioning or robot redocking.
Results:
Twenty-six patients have undergone NUx using our modified technique. Mean blood loss and operative time were 66 mL and 230 minutes, respectively. There were no intraoperative complications or open conversions, and there were no positive surgical margins. The average follow-up time was 7.8 months (range, 2–17 months), and 4 cases of cancer recurrence in the bladder were identified.
Conclusions:
This novel technique for robotic NUx offers a standardized and easy-to-implement approach for NUx that requires a minimal learning curve for an experienced robotic surgeon, while affording a comparable oncologic control without the need for patient repositioning or additional port placement.
Introduction
U
Despite achieving similar outcomes to the open procedure, several important limitations have been encountered with minimally invasive NUx (laparoscopic, robotic). This includes the need for intraoperative patient repositioning following vascular control of the renal hilum and kidney dissection in order to approach the distal ureter and bladder. Additionally, robot-assisted NUx frequently requires redocking of the robotic system to address the bladder cuff. Because these obstacles often result in increased intraoperative time, many surgeons chose either to manage the bladder through a separate, open incision or to reposition the patient and robotic system.
We describe a novel technique of robot-assisted NUx that allows for complete access to both the kidney and bladder without necessitating any patient or robotic repositioning.
Patients and Methods
We performed a modified technique for robotic NUx in 26 consecutive patients diagnosed with UTUC. This series represents the experience of two surgeons (K.K.B. and A.B.) at two tertiary-care referral centers. Baseline patient demographic data are listed in Table 1.
Pathologic stage based on final pathologic review of surgical specimen. There were no positive margins for any patient.
EBL, estimated blood loss; LOS, length of hospital stay; OR, operating room.
Surgical technique
After induction with general anesthesia, the patient is placed in flank positioning with the affected side up. Foam padding is applied to all pressure points, and the bed is slightly flexed. Using the Veress needle technique, the abdomen is insufflated, and pneumoperitoneum is established prior to port placement. The first port is a 12-mm camera port placed 2 cm caudal and lateral to the umbilicus. Next is an 8-mm robotic port, which is placed 5 cm cephalad to the camera port, just inferior to the costal margin. A second 8-mm robotic port is then placed 5 cm from the camera port at a 45° angle toward the anterior superior iliac spine. The third robotic port is placed 5 cm from the second robotic port at a 45° angle toward the midline (pelvis). A fifth and final 12-mm assistant port is placed halfway between the camera port and the first robotic port, just lateral to the level of the umbilicus. A detailed diagram of our modified port placement is shown in Figure 1. For right-sided cases, the bipolar Maryland grasper forceps is placed through the first robotic port (just inferior to the costal margin), representing the left hand, and a monopolar scissors is placed through the second robotic port (on a 45° angle from the camera to the anterior superior iliac spine), representing the right hand. A ProGrasp™ grasper (Intuitive Surgical) is placed through the third robotic port (fourth arm). The setup is identical for left-sided cases, but the instrument placements are mirrored.
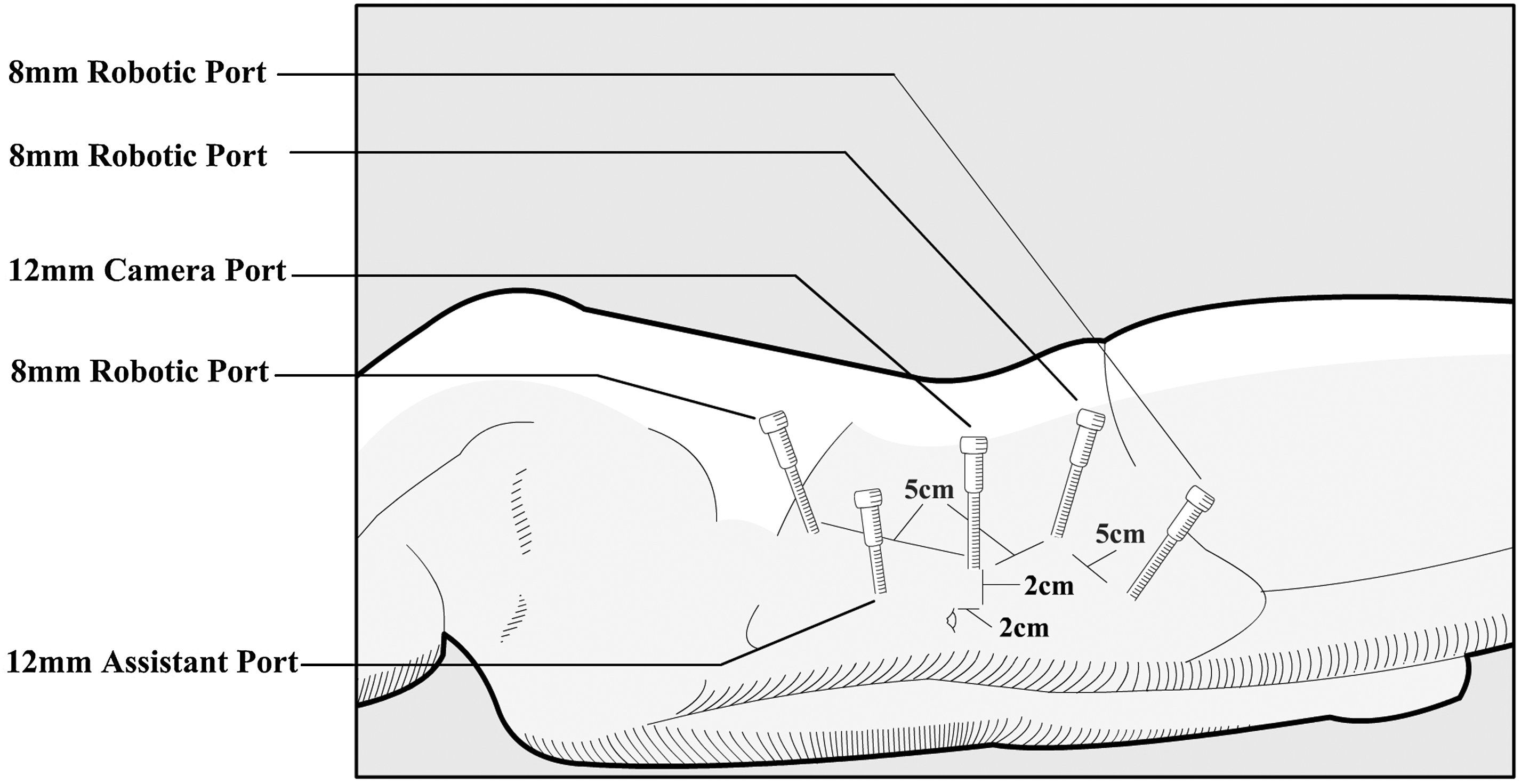
Schematic demonstrating the port placement for the modified robotic nephroureterectomy technique.
The initial part of the procedure should be performed in standard fashion, including exposure of the renal hilum and mobilization of the kidney from its surrounding structures. We routinely use a GIA™ stapling device (Covidien, Mansfield, MA) for vascular control, although this can be performed by the surgeon's preferred method. The ureter can be dissected to the bifurcation of the common iliac artery during this step.
Once the kidney and proximal ureter have been successfully dissected, a single exchange between the monopolar scissors and ProGrasp graspers is performed. This crucial switch allows the ProGrasp grasper to still be used as a static retractor, while allowing the two working instruments (i.e., monopolar scissors and Maryland grasper) better access to the pelvis; this allows the surgeon to perform the bladder cuff excision without repositioning the patient or redocking of the robot. Following this single instrument switch, the ureter is carefully dissected over the iliac vessels, along the hypogastric artery, and down to the bladder. Once the ureterovesical junction is reached, the detrussor muscle is identified and dissected off the bladder mucosa, allowing a wide margin of bladder cuff to be exposed. The bladder cuff is marked off, and a single 3-0 unidirectional barb suture is placed as a holding stitch. The cuff is dissected away, along with the ureteral stent, if present, from the mucosa and removed, en bloc, along with the kidney and ureter. Finally, the bladder is closed using the previously placed holding stitch in a water-tight fashion with full-thickness closure of the defect.
Results
In our initial experience with 26 patients, all cases were successfully performed without the need for open conversion, repositioning of the patient, or redocking of the robot. Mean operative time was 230 minutes (range, 128–310 minutes), and mean estimated blood loss was 66 mL (range, 25–100 mL). There were no intraoperative complications, and no patient received a blood transfusion. There were no positive surgical margins on pathological review of the surgical specimen. Median length of stay was 2 days (range, 1–15 days). There were no postoperative complications, and for the 3 patients who had hospital stays >10 days, their course was prolonged because of medical comorbidities. For example, 1 patient experienced an upper gastrointestinal bleed, which was not believed to be the result of our modified technique, as he had prior history of peptic ulcer disease. Patients underwent follow-up surveillance cystoscopy and urine cytology at 3-month intervals during the first year postoperatively, imaging at 6 months and 18 months postoperatively, and annual follow-up thereafter. The average interval of follow-up is 7.8 months (range, 2–17 months). On follow-up, 4 patients had evidence of tumor recurrence in the bladder based on imaging and cystoscopic surveillance.
Discussion
Although open NUx has been the gold standard in the management of UTUC, there has been much progress toward the use of minimally invasive techniques in this arena. Since the first laparoscopic NUx in 1991 to the advent of the da Vinci robotic surgical platform, the management of upper tract malignancy has evolved to provide for improved patient convalescence and operating room efficiency, while maintaining comparable oncologic outcomes to those of the open operation.3–8 With respect to robotic NUx, there are two major limitations that contribute to its lack of utilization: namely, the need for intraoperative patient repositioning and robot redocking. These steps are required to allow the console surgeon to “reach” the pelvis in order to complete dissection of the distal ureter and excision of the bladder cuff. Yet, the time and manual labor required to reposition an intubated patient and move the robot are both onerous and potentiate iatrogenic injury to the patient. In fact, several robotic surgeons choose to make a midline incision and perform an open bladder cuff excision in order to avoid this process.
We describe a standardized scheme to place ports that provides a simple and easily reproducible solution to these limitations. This technique allows for instrument access cephalad to the superior pole of the kidney, as well as caudal to the insertion of the ureter into the bladder, thereby providing ample range of motion to perform the entire procedure without instrument clashing. In addition, this port placement necessitates only a single instrument switch during the entire procedure, while avoiding any repositioning of the patient or robot intraoperatively.
Recently, there have been similar reports in the literature describing a pure robotic approach to performing a NUx without the need for repositioning or redocking. Park et al. 9 described a direct comparison of two robotic approaches, one with and one without intraoperative patient repositioning, and concluded that both approaches had similar outcomes with respect to hospital stay, estimated blood loss, and surgical margins. The authors also reported that avoiding intraoperative patient repositioning and robot redocking resulted in an average decrease of 50 minutes in the operative time. 9 A report by Hemal et al. 10 also demonstrated the reproducibility of performing a robotic NUx without moving the patient intraoperatively. Those authors similarly concluded that this approach resulted in improved surgical and oncologic outcomes, relative to previously reported robotic approaches. 10 However, unlike our technique, which only requires a single instrument switch, the authors in those two series9,10 described the need to manually exchange all instruments when attempting the distal ureteral and bladder cuff dissection. Our novel port placement may explain why our reported mean blood loss (66 mL) was lower than the other single-position robotic approaches.9–11
In addition to decreasing operative time and avoiding patient repositioning, our technique facilitates dissection of the distal ureter and bladder cuff. During the transition to a single-position robotic procedure, there have been multiple approaches described to manage the bladder cuff, including full bladder cuff excision, transurethral resection incision of the ureteral orifice, and extravesical stapling. 12 In a review of various methods of bladder cuff management, extravesical stapling resulted in poorer oncologic control with higher rates of local and metastatic urothelial cancer recurrence when compared with full bladder cuff excision and reconstruction. 10 In light of these findings, we believe that complete resection of the bladder cuff affords the best oncologic control and should be done during every NUx. We, therefore, have developed a way to successfully perform this maneuver during robotic NUx without necessitating any patient repositioning or a conversation to an open bladder cuff excision.
It is important to mention that our experience is limited by a small number of cases from two institutions. Nevertheless, our described technique is reproducible and affords the option of managing all aspects of the procedure robotically without any intraoperative repositioning. Moreover, we believe this modified technique for robotic NUx affords a minimal learning curve for experienced robotic surgeons, as evidenced by a generally downward trend of operative times observed between the earliest and most recent patients in our cohort. A larger cohort of patients with longer follow-up must be assessed to validate our initial findings.
Conclusions
Our approach demonstrates a reproducible robotic technique for complete NUx with bladder cuff excision in a single docking position using only a single instrument change. The described port placement of our procedure offers a standardized and easy-to-implement approach for NUx that requires a minimal learning curve for an experienced robotic surgeon, while affording increased operating room efficiency and comparable oncologic control to that of open NUx.
Footnotes
Disclosure Statement
No competing financial interests exist.