
Abstract
Abstract
Background:
Central pancreatectomy has been accepted as an alternative procedure for treating benign or low-grade malignant tumors in the pancreatic neck or proximal body of the pancreas, which preserves pancreatic parenchyma and function. In this study, we present our experience of laparoscopic central pancreatectomy with pancreaticojejunostomy.
Patients and Methods:
From April 2011 to February 2013, 8 patients underwent laparoscopic central pancreatectomy with a Roux-en-Y modified “dunking” or duct-to-mucosa pancreaticojejunostomy for benign or low-grade malignant tumors in the pancreatic neck or proximal body of the pancreas at the Department of General Surgery, Sir Run Run Shaw Hospital, Hangzhou, China. Surgical procedure, postoperative course, and follow-up data were collected.
Results:
Laparoscopic central pancreatectomy was performed successfully in all the patients. The pancreaticojejunostomy was executed with a modified “dunking” pancreaticojejunostomy (n=7) or duct-to-mucosa pancreaticojejunostomy (n=1). The mean operative time was 286±27 minutes (range, 250–330 minutes), with a mean blood loss of 57±21 mL (range, 30–100 mL). Mortality was 0%, and perioperative morbidity was 37.5% (pancreatic fistula [grade A], bleeding of a splenic vein branch, and retroperitoneal infection). The median postoperative hospital stay was 10 days (range, 6–38 days). At a median follow-up of 7.5 months (range, 2–24 months), all patients were alive without any exocrine or endocrine insufficiency or recurrence.
Conclusions:
Laparoscopic central pancreatectomy is feasible and safe. The modified “dunking” pancreaticojejunostomy can be performed safely in this approach.
Introduction
Laparoscopic pancreatic resection, including enucleation, DP, and PD, has been recently described; some of the patients in this series could have benefited from these procedures.8–10 In theory, laparoscopic CP (LCP) is thought to be a function-preserving and minimally invasive pancreatectomy. Owing to difficulty of pancreaticoenteric reconstruction, studies on LCP have not been as readily available.11–18 The purpose of this article is to present our experience of 8 complete LCPs with pancreaticojejunostomy (PJ).
Patients and Methods
Patients
From April 2011 to February 2013, 8 patients underwent LCP for benign or low-grade malignant tumors in the pancreatic neck or proximal body of the pancreas at the Department of General Surgery, Sir Run Run Shaw Hospital, School of Medicine, Zhejiang University, Hangzhou, China. All patients underwent preoperative assessment including laboratory examination, ultrasonography, computed tomography, and magnetic resonance imaging for characterization and localization of the lesions. Institutional Review Board approval and informed consent from the patients were obtained to perform LCP.
Operative technique
Position of the patient, surgeons, and trocars
The patient, under general anesthesia, was placed in the supine position with the head slightly elevated. The surgeon and the second assistant who held the laparoscope stood on the right side of the patient, and the first assistant stood on the left. Carbon dioxide pneumoperitoneum was established (CO2 at 15 mm Hg) using a Veress needle. One initial 10-mm trocar was placed for laparoscope below the umbilicus. A 30° telescope was inserted to examine the peritoneal cavity to rule out metastasis disease. After general examination, the other four trocars (one 12 mm, three 5 mm) were inserted into the left upper flank, left flank, right upper flank, and right flank quadrants; the five trocars arranged in a V-shape (Fig. 1).

Placement of trocars.
Dissection phase
The gastrocolonic ligament was divided for entrance to the lesser sac with a Harmonic® Ace® scalpel (Ethicon Endo-Surgery, Inc., Cincinnati, OH). The mobilization of the pancreas began at the superior border until the common hepatic artery and the proximal splenic artery were visualized (Fig. 2A). Then the pancreas was mobilized at the inferior border to visualize the superior mesenteric vein, the splenomesenteric confluence, and the portal vein (Fig. 2B). After a tunnel was created behind the neck of the pancreas, the pancreas was transected 1 or 2 cm proximal to the right side of the tumor with an endoscopic linear stapler (Endocutter 60 stapler, white or blue cartridge; Ethicon Endo-Surgery) (Fig. 2C). According the extent of pancreatic disease, the central part of the pancreas was dissected from the splenic artery and vein by division of vascular branches with the Harmonic scalpel. The distal transection (1 or 2 cm distal to the left side of the tumor) of the pancreas was performed with the Harmonic scalpel (Fig. 2D).
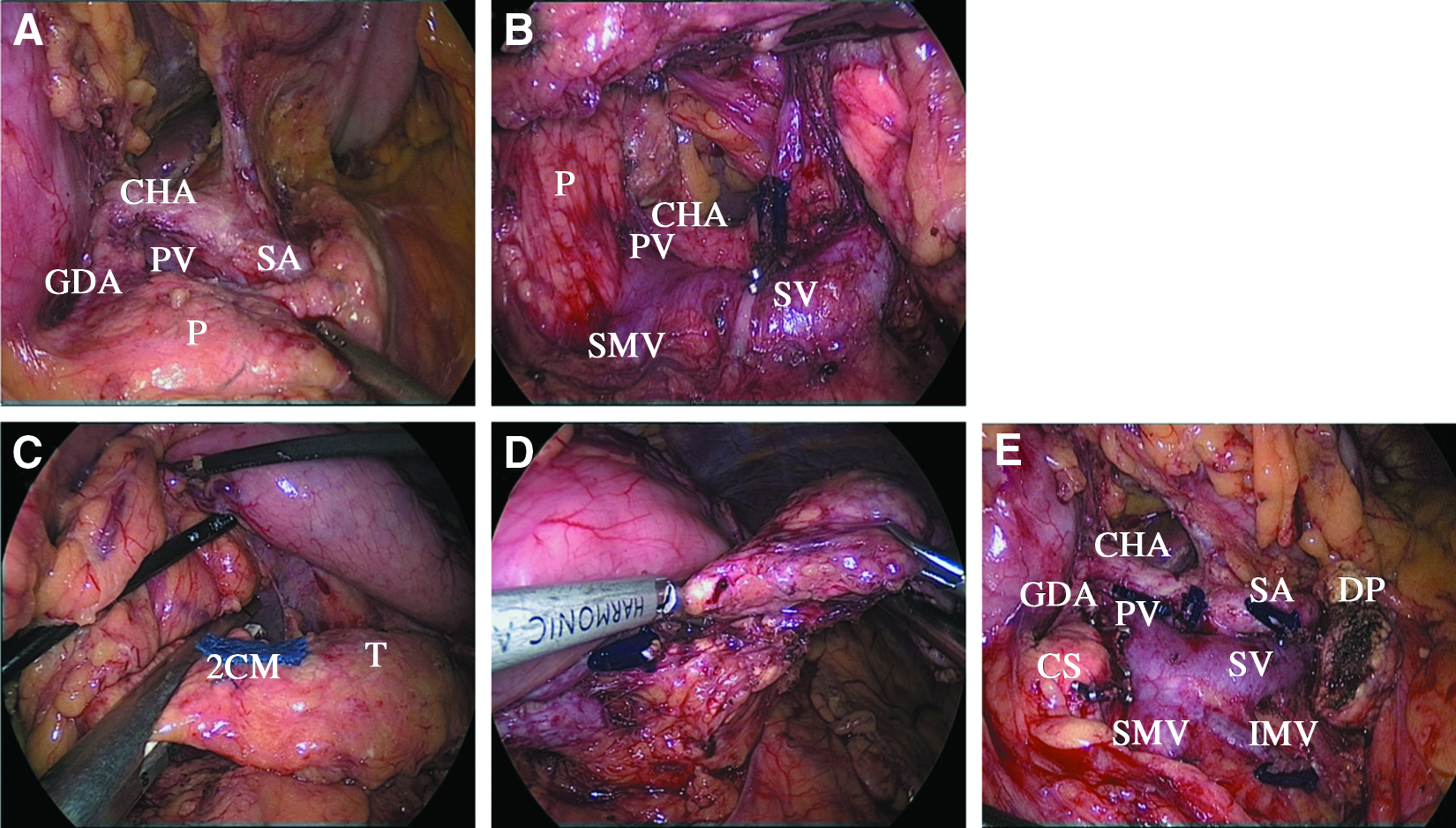
Pancreas dissection and transection performed by laparoscopic central pancreatectomy:
Reconstructive phase
Depending on whether the duct of Wirsung could be identified, two methods were used to accomplish the pancreaticojejunal reconstruction: either modified “dunking” PJ19,20 or duct-to-mucosa PJ.15,20 For the modified “dunking” PJ, a row of 3-0 coated polyglactin 910 (Vicryl™; Ethicon Products, Johnson & Johnson, Somerville, NJ) suture was placed with interrupted stitches between the jejunal serosa and the posterior side of the pancreatic capsule for apposition (Fig. 3A). The jejunum was opened with a Harmonic scalpel, suitable for distal pancreatic stump. The posterior layer was performed with continuous or interrupted 3-0 Vicryl suture between the pancreas (parenchyma and capsule) and the full thickness of the jejunum (Fig. 3B). The anterior layer was performed in the same way as the posterior layer. For the duct-to-mucosa PJ, the posterior outer row of 3-0 Vicryl suture was placed with interrupted stitches between the jejunal serosa and the posterior side of the pancreatic capsule. A small hole was created in the jejunum for anastomosis (Fig. 3C). A 3-mm silicon tube was inserted into the pancreatic duct and the downstream jejunum. Six stitches of 3-0 Vicryl suture were placed between the jejunal mucosa and the main pancreatic duct (Fig. 3D). The anterior outer row of 3-0 Vicryl suture was placed with interrupted stitches between the jejunal serosa and the anterior side of the pancreatic capsule.

Pancreaticojejunostomy (PJ) performed by laparoscopic central pancreatectomy:
Finally, side-to-side jejunojejunostomy was performed with an endoscopic linear stapler (Endocutter 60 stapler, white cartridge).
The specimen was removed through the slightly enlarged umbilical incision with an endoscopic plastic bag. All the resected specimen and its margins were sent for intraoperative frozen section examination. Two drainage tubes were left close to the proximal pancreatic remnant and PJ in all patients.
Postoperative pancreatic fistula was defined as any measurable volume of draining amylase-rich (more than three times the upper normal serum value) fluid on or after postoperative Day 3. 21 The fasting blood glucose level (normal range ≤110 mg/dL) was used to evaluate pancreatic endocrine function. The clinical evaluation was used to assess the pancreatic exocrine function. Patients with diarrhea, weight loss, and fatty stools were considered to have pancreatic exocrine insufficiency.
Results
The clinical characteristics and outcomes of all 8 patients are summarized in Table 1. There were 4 men and 4 women with a mean age of 51.0±14.5 years (range, 25–70 years). Seven (87.5%) of the 8 patients were asymptomatic; 1 patient had abdominal pain. Each of the tumors was less than 3 mm away from the main pancreatic duct and deep in the parenchyma, which contraindicated enucleation. Postoperative pathological diagnoses included serous cystadenoma (n=3), solid pseudopapillary tumor (n=2), mucinous cystadenoma (n=2), and intraductal papillary mucinous neoplasm (n=1). The mean tumor size was 19.6±5.4 mm (range, 12–28 mm), with a mean length of the resected pancreas of 58.1±7.0 mm (range, 50–65 mm). All patients received complete resection with negative surgical margin.
F, female; IPMN, intraductal papillary mucinous neoplasm; LC, laparoscopic cholecystectomy; M, male; MCA, mucinous cystadenoma; NR, no recurrence; NPEI, no pancreatic exocrine or endocrine insufficiency; PJ, pancreaticojejunostomy; SCA, serous cystadenoma; SPT, solid pseudopapillary tumor.
LCP was performed successfully in all the patients. The splenic vessels and the spleen were preserved in all patients. The pancreaticojejunal reconstruction was executed with a modified “dunking” PJ (n=7) or duct-to-mucosa PJ (n=1). Two patients underwent combined resection of the gallbladder for cholelithiasis during the LCP. The mean operative time was 286±27 minutes (range, 250–330 minutes). The mean blood loss was 57±21 mL (range, 30–100 mL). No operative mortality was noted.
One patient developed hemorrhage due to bleeding of a splenic vein branch on the first postoperative day; she underwent emergency laparoscopic exploration and ligation of the splenic vein branch using small titanium vascular clips. One patient developed retroperitoneal infection; he underwent laparotomy on postoperative Day 10. We found fluid collection in the resection bed. Therefore, debridement was done, and two drainage tubes were placed. Two weeks after surgery, no residual collection was found on the computed tomography scan. One patient experienced postoperative pancreatic fistula (grade A) that was managed conservatively and ultimately cured. The drainage tube was removed on postoperative Day 12.
The nasogastric tube was removed on the first postoperative day. Oral intake started 2 or 3 days after surgery. The median postoperative hospital stay was 10 days (range, 6–38 days). At a median follow-up of 7.5 months (range, 2–24 months), all patients were alive with no recurrence. None of the patients developed exocrine or endocrine insufficiency.
Discussion
The treatment of benign or low-grade malignant tumors in the pancreatic neck or proximal body of the pancreas is a challenging issue. Both PD and DP would increase the risk of postoperative pancreatic deficiency.1–5 So function-preserving pancreatectomy, especially LCP or laparoscopic enucleation, is thought to be an ideal procedure in these instances because patients with these tumors can be expected to survive long term.
The first LCP as described by Baca and Bokan 11 in 2003 was performed with PJ after resecting pancreatic cystadenoma. During the last decade, only 21 patients who underwent LCP have been reported in the literature (Table 2).11–18 Most of these articles are case reports and small series. The two largest series of LCP, including 6 and 9 cases, respectively, reported morbidity rates of 33.3% and 33.3% with pancreatic fistula rates of 33.3% and 22.2%, respectively, with no mortality.14,15 A review of 512 patients from 21 series who underwent open CP reported an overall morbidity rate of 41% (range, 13%–62%), a pancreatic fistula rate of 27% (range, 0%–62%), and a reoperation rate of 4% (range, 0%–21%). 6 Our series with 8 cases showed a morbidity rate of 37.5%, the pancreatic fistula rate of 12.5%, and a reoperation rate of 25%, similar to what have been reported in the literature.6,14,15 Although the morbidity was high, experienced management of the complications eventually resulted in safe recovery. At a median follow-up of 7.5 months (range, 2–24 months), we have not observed any recurrence or pancreatic endocrine or exocrine insufficiency, which matches the findings in the literature.6,11–18 Our data and literature indicate that LCP is a safe technique with morbidity and long-term results similar to those with the open procedure.
Data are median (range) values.
One case with laparoscopic-assisted surgery.
Data are mean (range) values.
NA, not available; PG, pancreaticogastrostomy; PJ, pancreaticojejunostomy.
For laparoscopic enucleation to be executed safely, the lesion must be at least 2–3 mm away from the main pancreatic duct and not too deep in the parenchyma. 8 The three largest series of laparoscopic enucleation for cystic tumors and nonfunctional neuroendocrine pancreatic tumors, including 21, 21, and 30 cases, reported mortality rates of 0%–4%, morbidity rates of 17%–33%, pancreatic fistula rates of 13%–29%, reoperation rates of 0%–4%, and length of hospital stay of 6–9 days.8,22,23 In our series, each of the tumors was less than 3 mm away from the main pancreatic duct and deep in the parenchyma, which contraindicated enucleation. Our series with 8 cases showed a morbidity rate of 37.5%, a pancreatic fistula rate of 12.5%, and a reoperation rate of 25%, which seemed to be higher than those with laparoscopic enucleation.8,22,23 The reason for the high morbidity was that this study included only the initial experience with LCP. We believe the morbidity rate would decrease after the learning curve period.
In the literature on LCP, there are two types of reconstruction for distal pancreatic stump: (1) pancreatogastrostomy between the distal stump and stomach and (2) Roux-en-Y anastomosis of the distal stump and jejunum.11–18 A 6 case series of LCP with pancreatogastrostomy was associated with a median operative time of 225 minutes, oral feeding on postoperative Day 11, and a median length of hospital stay of 18 days. 14 Rotellar et al. 15 reported a 9 case series of laparoscopic Roux-en-Y duct-to-mucosa PJ after CP with a mean operative time of 435 minutes, oral feeding on the first postoperative day, and a median length of hospital stay of 5 days. Compared with laparoscopic PJ, pancreatogastrostomy seems to be easier and faster for just one anastomosis but with delayed recovery. Rault et al. 1 found that PJ allows better pancreatic exocrine function preservation than pancreatogastrostomy after PD. So in our series, we preferred laparoscopic PJ after CP. CP is indicated in patients usually with a nondilated duct of Wirsung, which is difficult to identify. The comparison between duct-to-mucosa and end-to-side (modified “dunking”) PJ reconstruction after PD revealed no significant difference in the rate of complications. 19 Therefore, most cases in our series were executed with modified “dunking” PJ yielding a pancreatic fistula rate of 14.3% (1/7). Moreover, the mean operative time of our series was 286 minutes with oral feeding on the second or third postoperative day and a median length of hospital stay of 10 days. We believe that the laparoscopic modified “dunking” PJ for the distal pancreas is an alternative procedure.
In our experience, there are three key points during the LCP. (1) The mobilization of the central portion of the pancreas started gently from the superior and inferior border to the back of the central portion of the pancreas; the vessels, including the common hepatic artery, the proximal splenic artery, the superior mesenteric vein, the splenomesenteric confluence, and the portal vein, should be visualized in advance. (2) The proximal pancreas was transected with an endoscopic linear stapler. According to our experience in laparoscopic DP, 24 we generally choose a white (nail height, 1 mm) or blue (nail height, 1.5 mm) cartridge with no stitching reinforcement. Sometimes a titanium clip may be used to clip the bleeding point of the proximal pancreatic stump. (3) Laparoscopic PJ is the most difficult step of the procedure and requires a highly skilled suture technique. In our series, either modified “dunking” PJ or duct-to-mucosa PJ was used to accomplish the pancreaticojejunal reconstruction with a pancreatic fistula rate of 12.5%. Without identifying and suturing the nondilated duct of Wirsung, modified “dunking” PJ was easier to execute. Before the anastomosis, 2 cm of distal pancreatic stumps should be mobilized. A row of interrupted stitches between the jejunal serosa and the posterior side of the pancreatic capsule was performed just for apposition. No stitching was performed between the jejunal serosa and the anterior side of the pancreatic capsule, which usually allowed the jejunum to roll up the pancreas in the dunking PJ. The suture between the pancreas (parenchyma and capsule) and full thickness of the jejunum was performed with interrupted stitches in the first 2 patients and continuous stitches in the last 5 patients. Moreover, there was no pancreatic fistula in the last 5 patients. In our opinion, continuous stitches could reduce technical complexity and may be more suitable for anastomosis.
In conclusion, our series shows that LCP is feasible and safe for benign or low-grade malignant tumors in the pancreatic neck or proximal body of the pancreas. Laparoscopic modified “dunking” PJ can be performed safely by highly skilled pancreatic and laparoscopic surgeons. The LCP with modified “dunking” PJ is promising but needs to be validated by more clinical data.
Footnotes
Acknowledgments
This project was supported by key project grant (2011C13036-2) from the Science and Technology Department of Zhejiang Province.
Disclosure Statement
No competing financial interests exist.