
Abstract
Abstract
Purpose:
To describe a laparoscopic surgical technique for ureterocystoplasty in pediatric patients with the Mitrofanoff procedure.
Patients and Methods:
The procedure was performed in 4 patients (2 females and 2 males), 8–11 years old (average, 9.5 years), with a history of myelomeningocele and secondary neurogenic bladder. The patients were evaluated before the surgery with renal ultrasound, voiding cystourethrography, and renal scintigraphy. All subjects reported left hydronephrosis with severe dilatation of ureter and the collector system, left megaureter with grade V vesicoureteral reflux, and left functional exclusion, with right renal normal function. The urodynamic investigations revealed low bladder size and bladder leak point pressure (BLPP) above 40 cm H2O. The laparoscopic ureterocystoplasty augmentation procedure and the Mitrofanoff procedure with the proximal ureter were performed in these patients. Complications and outcomes were recorded and compared with those of the postoperative urodynamic test.
Results:
The 2–4 years of follow-up of the patients and its urodynamic postoperative evaluation reported at least 75% of the capacity according to their age, compliance that varied between 15 to 20 mL/cm H2O, and a BLPP of less than 40 cm H2O. This last parameter is considered of low risk to damage the upper urinary tract. There was no leaking of urine by the stoma over the 4 hours of catheterization.
Conclusions:
Even though enterocystoplasty is the gold standard to increase the capacity of the neurogenic bladder, it has an elevated morbidity. So the use of a dilative ureter to increase bladder size and create a Mitrofanoff stoma in patients with neurogenic bladder, pop-off phenomenon, and renal ipsilateral atrophy could be considered by the laparoscopic approach.
Introduction
V
Patients and Methods
In the period of September 2008 to December 2012 we performed the procedure in two girls 10 and 11 years of age and two boys 8 and 9 years of age. All of them were referred to our institutions with a history of neurogenic bladder secondary to myelomeningocele and continuous urinary tract infection. The patients were evaluated with renal ultrasound, voiding cystourethrography, renal scintigraphy, and urodynamic study.
The pathologic findings were severe left hydronephrosis, grade V left vesicoureteral reflux, and left renal exclusion. The urodynamic investigation revealed low bladder size, low compliance (2–5 mL/cm H2O), and bladder leak point pressure (BLPP) above 40 cm H2O.
With the consent of the parents, we planned to perform a vesical augmentation and the Mitrofanoff procedure using the left megaureter.
Technical considerations
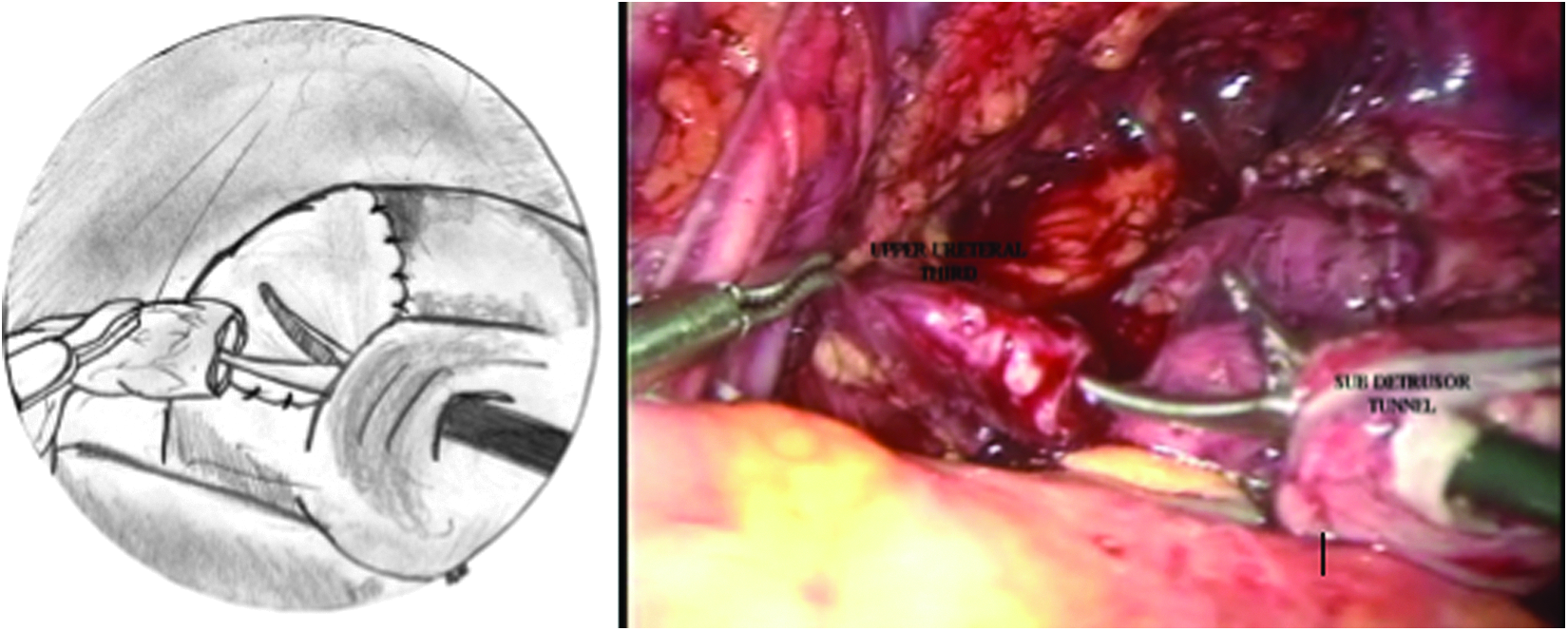
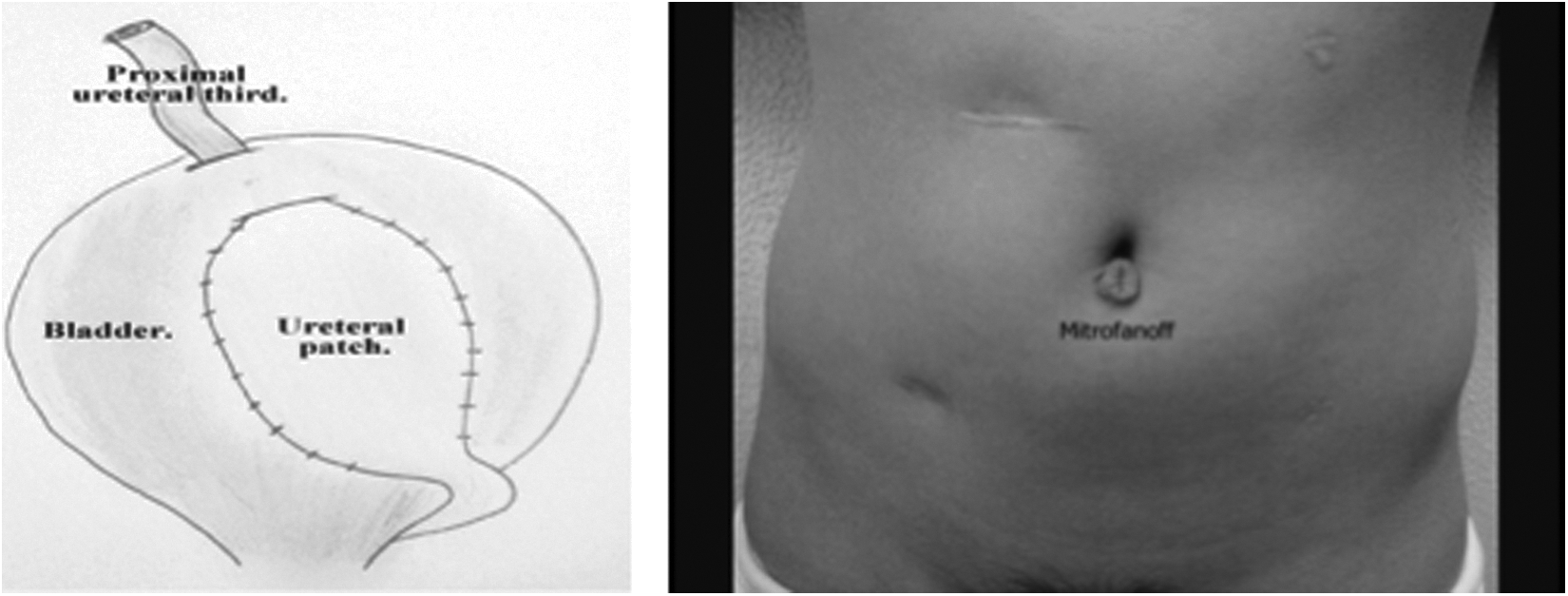
We used a 10-mm umbilical port and three or four extra ports (5 mm), a 30° laparoscope, and 5-mm instruments. Once the trocars were inserted in the abdominal cavity, a Cattell's maneuver was performed in order to expose the left kidney. A standard nephrectomy was made preserving the left megaureter (Fig. 1). The vesical dome was then dissected, and a subdetrusor tunnel was created with the intention to use it as a hydrostatic valve for the Mitrofanoff procedure (Fig. 2). The megaureter was detubularized on its middle section, preserving the proximal to renal and distal ureter sections tubularized with the ureterovesical junction intact to ensure better vascularization (Fig. 3). The bladder was then obliquely opened to the ureterovesical left junction, with enough length to hold the patch ureteral (Fig. 4). The patch ureteral was anastomosed to the bladder using 3-0 monocryl or PDS suture with intracorporeal sutures (Fig. 5). Once the anastomosis was completed, the upper section of the ureter was passed through the previously created subdetrusor tunnel and exteriorized through the umbilical port, creating the Mitrofanoff stoma (Fig. 6). The final reconstruction appearance is shown in Figure 7.
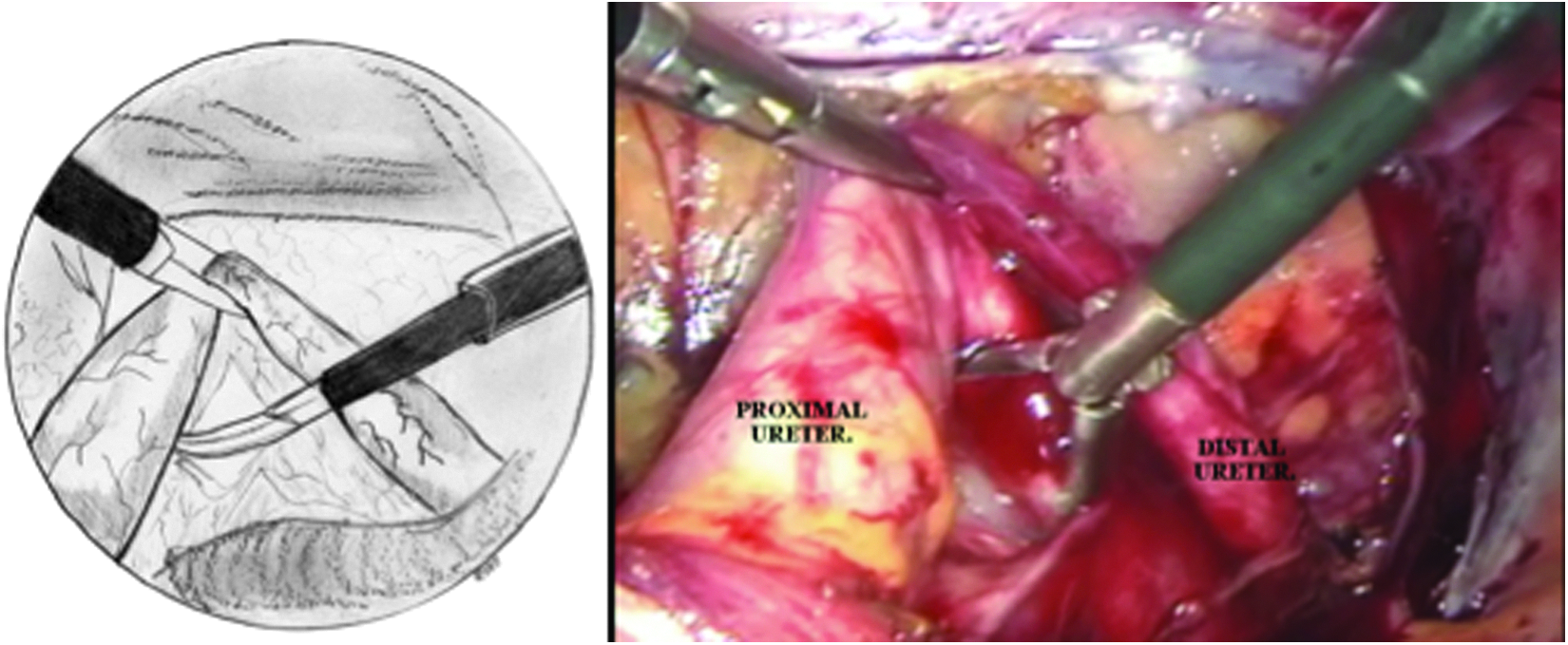
Ureteral dissection.

Submuscular tunnel creation.
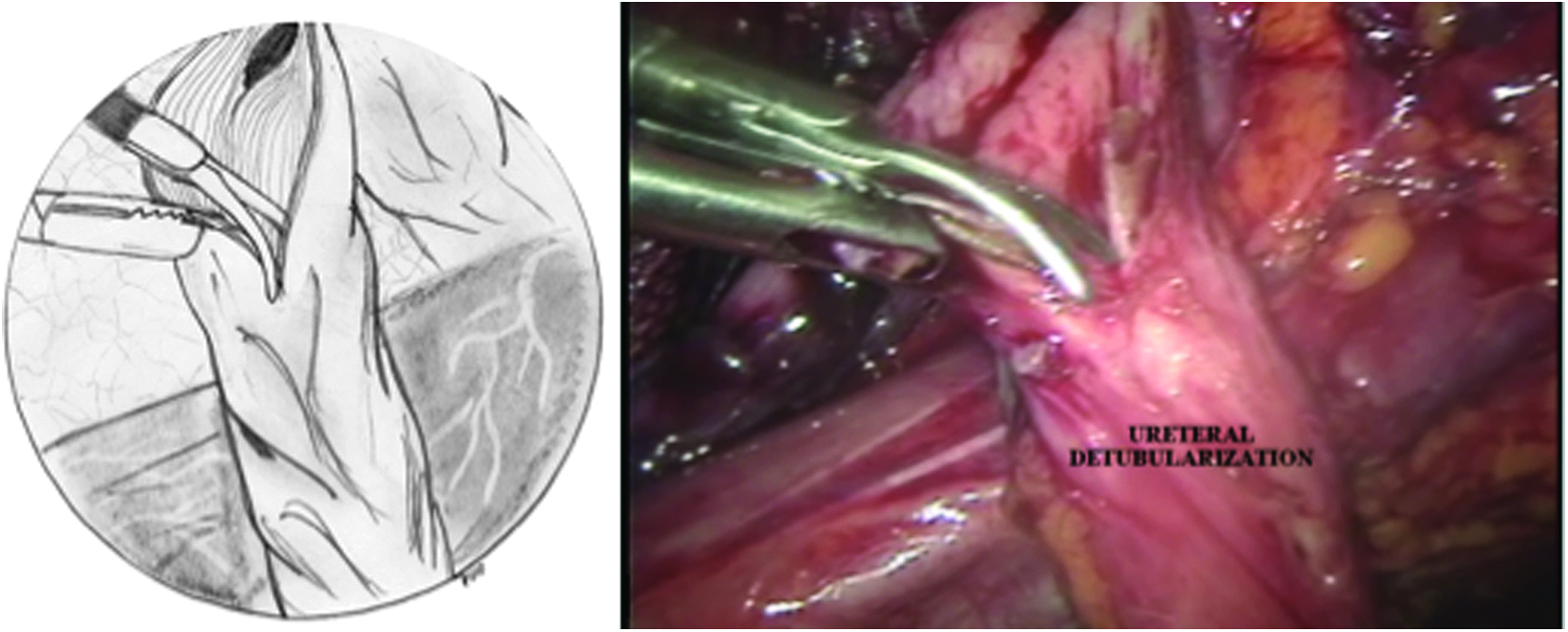
Detubularization of the ureter.
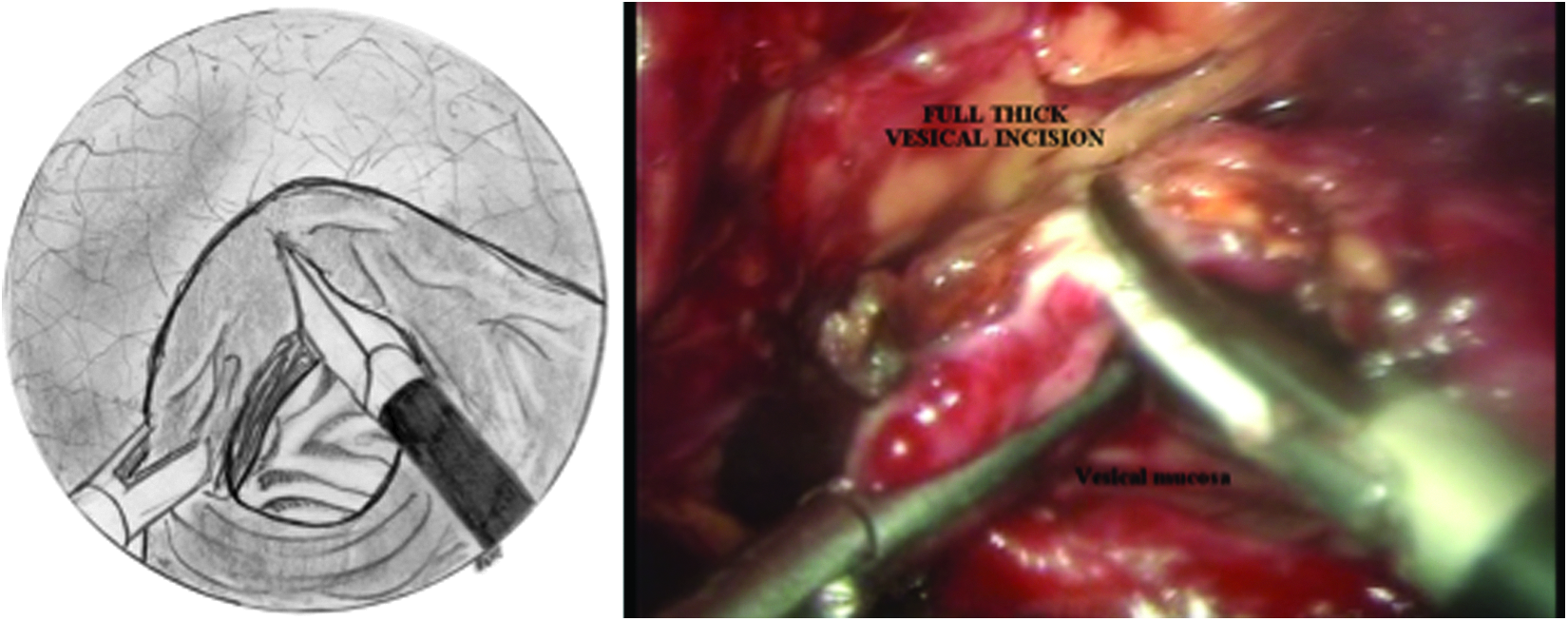
Incision of the vesical dome.
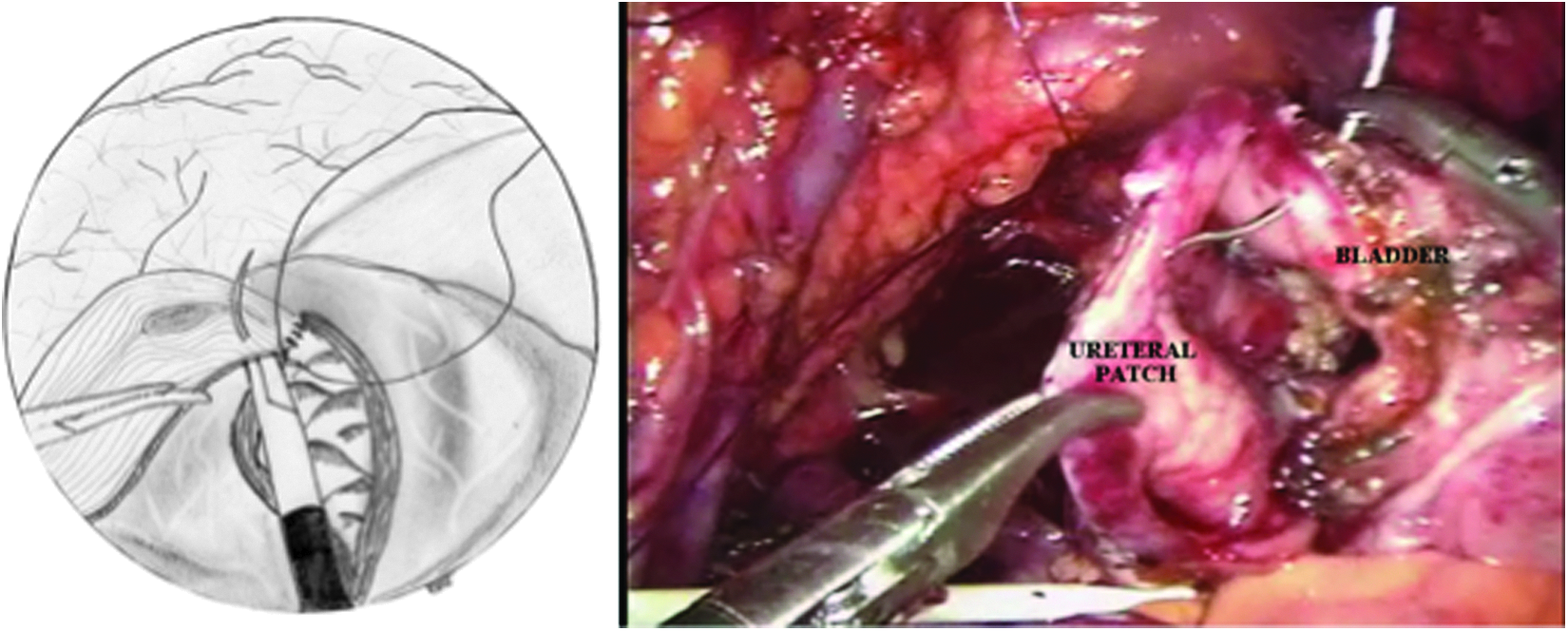
Ureterovesical anastomosis.
Creation of the Mitrofanoff procedure's continent mechanism.
Final aspect.
Results
The average time for the surgery was 4 hours. The follow-up of the patients was 2–4 years (average, 3 years). The increment of bladder obtained was at least of 75% of the capacity according to their age with mean compliance that varied between 15 to 20 mL/cm H2O. BLPP was below 30 cm H2O, considered to indicate low risk for the upper urinary tract. Mean bladder capacity improved from 146 to 312 mL (113% increase), as outlined in Table 1. None of the patients required further augmentation surgery. Three patients were symptomatically well, and only the 8-year-old male patient had mild progressively dilation of the upper tract and was symptomatic with one urinary infection per year. We added oxybutynin to the clean intermittent self-catheterization, which maintained the patient in stable condition. There was no leaking of urine by the stoma during the 4 hours of catheterization.
The compliance was measured to reach volumes of 50 and 100 mL before and after surgery.
BLPP, bladder leak point pressure; F, female; M, male; Preop, preoperatively; Postop, postoperatively.
Discussion
The technical options for augmentation cystoplasty include bowel augmentation, vesicomyomectomy, seromuscular augmentation, and the use of bioprosthetic materials. These last three technical options were created in order to avoid the use of bowel tissue in the urinary tract, creating at the same time a bladder with normal compliance and capacity. Despite these efforts, each technique has its own advantages and complications. Nowadays the only feasible augmentation techniques are those that use the stomach, ileum, colon, ureter, and the seromuscular augmentation. The report of the ureter as a bladder patch in the 1990s was promising.8–10 Theoretically the ureter was the best tissue available for the vesical augmentation because it eliminates the electrolytic disorders, mucus production, the risk of metaplasia, and the disruption of the intestinal tract that are present with the bowel augmentation. Besides, it already has urothelium and potential elasticity. Because there is no heterotopic tissue, the reported risk of late bladder neoplasia in enterocystoplasty would theoretically be decreased.11,12
Unlike gastrocystoplasty and enterocystoplasty, no spontaneous perforation has been reported to date in ureteral augmentations.13,14
The main benefits of bladder augmentation covered with urothelium are associated with the absence of mucus production and the decreased possibility of urinary infection and lithiasis. In addition, it avoids the metabolic disturbances secondary to the absorption of urine by the intestinal mucosa or the great number of urinary, metabolic, and gastrointestinal complications related to gastrocystoplasty.15–19
Husmann et al. 20 tried to establish the preoperative conditions in order to ensure a successful ureteral vesical augmentation. They determined that the presence or absence of vesicoureteral reflux, the diameter of the ureter sized by ultrasound in the patient, and its compliance were the key factors that should be analyzed preoperatively. They established that those ureters with a diameter of >1.5 cm had better compliance and capacity than those with a diameter of <1.5 cm. It is important to know whether the ureter refluxes or not because it is now known that a refluxing ureter has higher levels of type III collagen fibers, which reduce the compliance and distensibility of the ureter. In practice, Husmann et al. 20 found that ureterocystoplasty has little to no merit in patients with neuropathic bladder dysfunction, and it is best considered in the presence of a nonrefluxing megaureter greater than 1.5 cm in width or in the presence of mild bladder noncompliance (20 mL/cm H2O or greater), where bladder dysfunction is not related to a neuropathic etiology. 21 However, in the experience of Ramalingam et al. 7 there was an improvement of compliance and capacity in spite of reflux. Similarly, we think that in cases with neuropathic bladder, renal atrophy, and the pop-off phenomenon, the ureter could be used first more easily than bowel and appendix to increase bladder size, and its proximal end could be used to create the Mitrofanoff stoma by the laparoscopic approach (Fig. 8).
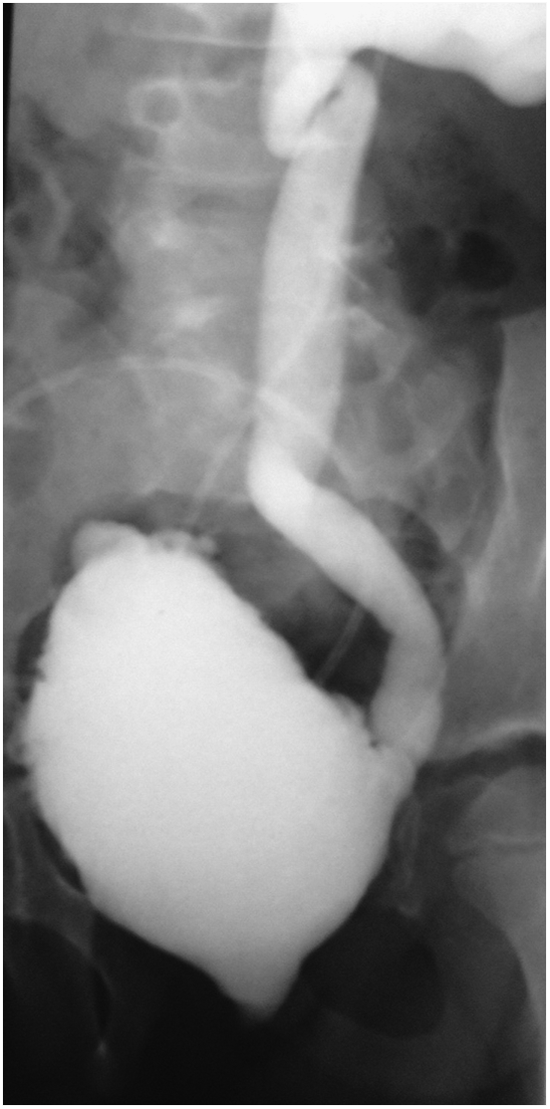
Pop-off phenomenon.
Tekgül et al. 22 established that ureterocystoplasty is the technique of choice in patients with unilateral renal exclusion associated with megaureter and vesicoureteral reflux and also in patients with both healthy kidneys but with a megaureter that can be use to perform a transureteroureterostomy. The latter was supported by Gosalbez and Kim, 23 who concluded that the presence of both healthy kidneys is not a contraindication to performing an ureterocystoplasty. Both series reported an increase in vesical capacity of 263% and 350%, respectively. In contrast, Pascual et al. 24 in their series of 22 patients treated with ureterocystoplasty reported that only 50% of them obtained at least 76% of the expected bladder capacity for age and weight. In our small number of patients the increment was ≥75%.
The continuous evolution of laparoscopic techniques is now occurring in almost every surgical area. The laparoscopic approach repeats the previously proven steps of the open techniques with the obvious modifications to work in a narrower space. Such evolution has been progressive, initially trying with simple procedures and later trying with more complex procedures that challenge the surgeons' expertise.6,7 Docimo et al. 2 performed the first laparoscopic enterocystoplasty back in 1995. Series of the laparoscopic approach have been reported by Gill et al., 3 Elliot et al., 4 Chung et al., 5 Ramalingam et al., 25 and Lorenzo et al. 26 Nevertheless, there are a few reports of laparoscopic intracorporeal ureterocystoplasty in valve bladder syndrome before kidney transplantation 6 but none to our knowledge with the Mitrofanoff procedure using the proximal ureteral portion.
In this article we report a laparoscopic technique that leaves the distal section of the ureter tubularized, thus preserving its vascularity, as proposed by Adams et al. 27 and Wolf and Turzan, 28 assuring the vitality of the ureteral patch, and uses the proximal section of the ureter as the Mitrofanoff stoma with good results. The follow-up has proved therapeutic benefits comparable to those obtained with the open approach, with the benefits of the laparoscopic technique.
Footnotes
Acknowledgments
The authors wish to thank the Mexican Social Security Institute and the Medica Sur and Star Medical Pediatric Hospitals for the facilities granted for the realization of this procedure.
Disclosure Statement
No competing financial interests exist.