
Abstract
Abstract
Purpose:
As application and awareness of single-incision pediatric endosurgery (SIPES) are increasing, various techniques and indications have been independently described by select centers around the world. In order to facilitate a cooperative approach toward advancing and investigating the practice of SIPES, we conducted a survey among members of the International Pediatric Endosurgery Group (IPEG), asking them about their experience and attitudes toward single-incision endosurgery.
Materials and Methods:
After institutional review board approval, an invitation to participate in an online survey was sent to all IPEG members. Questions focused on demographic information, practice patterns, indications, and equipment used regarding SIPES.
Results:
Of the 560 contacted active IPEG members, 115 completed the survey (recall 21%). The respondents represented pediatric surgeons from 32 countries on six continents. Of respondents, 97% had heard of, while 71% had performed, SIPES. Reasons for not having performed SIPES included disbelief in benefit (59%), lack of proficiency (34%), and inadequate resources (28%). The most commonly performed SIPES procedures were appendectomy (85%), cholecystectomy (66%), splenectomy (42%), pyloromyotomy (35%), and intestinal surgery (13%), as well as Nissen fundoplication and gynecologic adnexal pathology (7%). The equipment and techniques utilized showed large variation and included some self-devised, innovative, low-resource approaches. Complications with SIPES reported by the survey participants included technical difficulties, wound infection, and prolonged operating time.
Conclusions:
SIPES is being performed worldwide for a large spectrum of common indications in pediatric surgery. The equipment and techniques used vary with geographic location and resources. Some encountered complications are common to those seen with conventional minimally invasive surgery, whereas others may be SIPES-specific. Different respondents reported diverging views on pain, operating time, and cost.
Introduction
T
In order to facilitate a cooperative approach toward advancing and investigating the practice of SIPES, it is necessary to understand its current prevalence in terms of geography, technique, and acceptance. We therefore conducted a survey among members of the International Pediatric Endosurgery Group (IPEG), asking them about their experience and opinions toward SIPES. We also conducted a literature search and traced the geographic origin of all published articles on SIPES to date.
Materials and Methods
After institutional review board approval (Weill Cornell Medical College protocol number 1108011904), an invitation to participate in an anonymous online survey was sent out to all IPEG members. Questions focused on demographic information including location, practice patterns, indications, and equipment used regarding SIPES. There was no reward given to respondents, and a follow-up notice was sent out 4 weeks after the initial invitation to participate. The survey queried information on practice type, geographic location, responder's experience in general and with SIPES, perceptions concerning SIPES in terms of applicability, indication, advantages and disadvantages, and encountered complications, as well as specific experience with single-site appendectomy, cholecystectomy, and splenectomy. Eight weeks after the initial invitation, the survey was closed, and the resulting data were pooled into an electronic database for analysis and interpretation.
The literature search was conducted in PubMed using the search algorithm “(single incision OR single site) AND (laparoscopic OR endosurgery) surgery AND (children OR pediatric).” Abstracts were manually scanned for relevance, and publications were grouped by country of origin.
Results
Of the 560 contacted active IPEG members, 115 completed the survey (recall 21%). The respondents represent pediatric surgeons from 32 countries on six continents. SIPES was practiced in 31 countries (Fig. 1). Ninety-three respondents (81%) worked in an academic/university setting, 15% in an urban community practice, 2% in a rural community practice, and 1% in either an urban private pediatric hospital or a multispecialty group practice.

Map showing the location of survey respondents practicing single-incision pediatric endosurgery (countries in gray, specific postal codes are marked as black dots).
In terms of level of experience, 6% of respondents were in training, 24% had been in practice less than 5 years, 17% for 5–10 years, and 17% for 10–15 years, and 36% had been practicing for over 15 years.
Ninety-nine percent of respondents had heard of SIPES, and 71% personally performed SIPES procedures. Of the 32 respondents who had not performed SIPES, 24 (75%) were from university/academic hospitals, and 6 (19%) were from urban community practice, whereas 83% of those who performed SIPES were practicing in an academic/university setting.
Approximately half of respondents thought that SIPES is suitable for any age group. However, 21% believed the lower age limit for SIPES to be in the 0–2 year range, 17% in the 3–5 year range, and 7% in the 6–10 year range, and 6% stated that SIPES should be limited to those 11 years and older (Fig. 2).
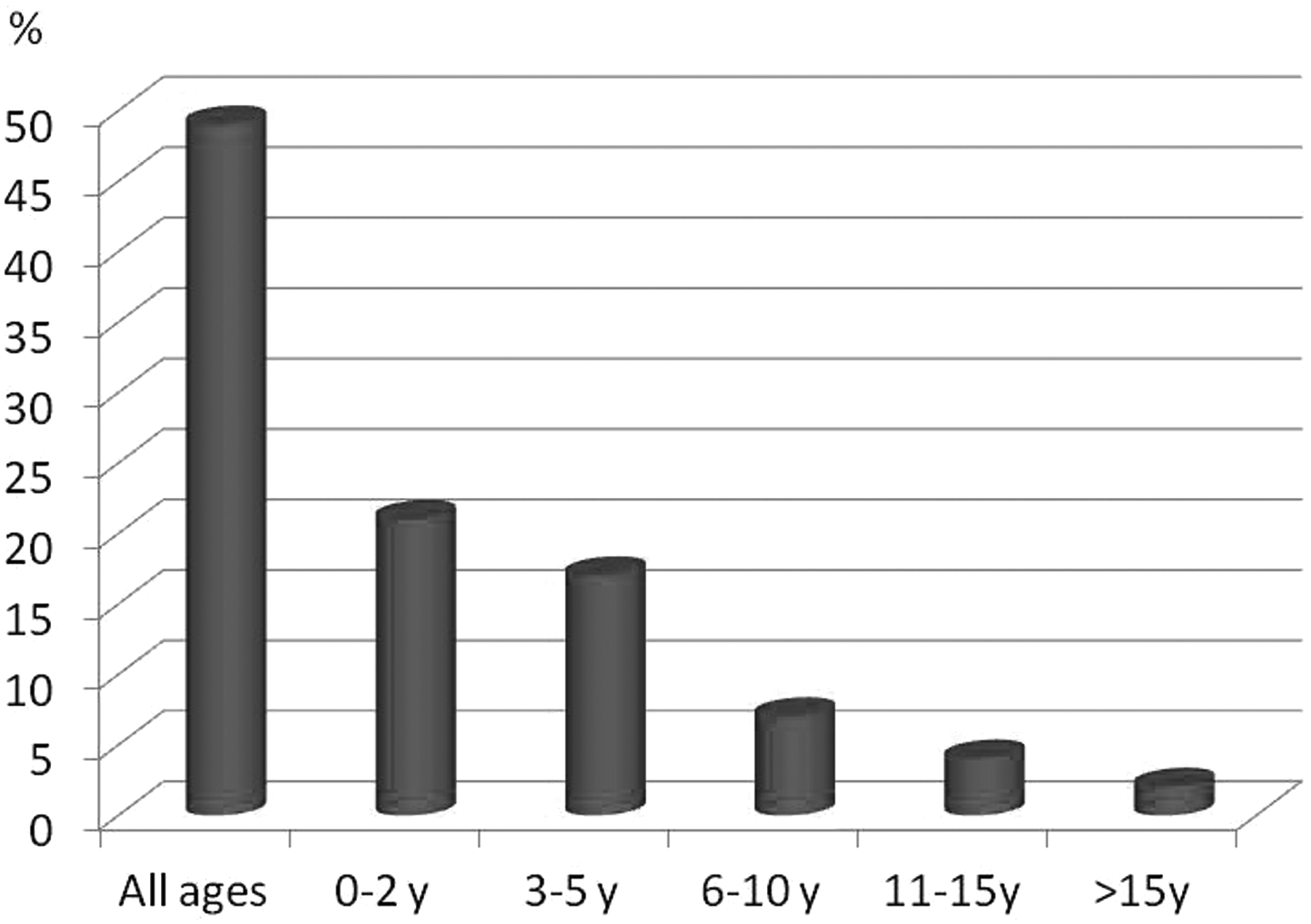
Lower age limit for single-incision pediatric endosurgery procedures by percentage of surgeon response. Almost half of all queried surgeons would perform single-incision pediatric endosurgery procedures at any age, whereas nearly a quarter would avoid using the technique in children under 2 years of age.
Of those having performed SIPES, the case load in the last month was 0–1 cases for 27%, 2–5 cases for 36%, 6–10 cases in 16%, and more than 10 SIPES cases for 21% of respondents. Reasons for not having performed SIPES included disbelief in benefit (59%), lack of proficiency (34%), and having inadequate resources (28%). Perceived benefits and drawbacks are presented in Table 1.
The most commonly performed SIPES procedures were appendectomy (85%), cholecystectomy (66%), splenectomy (42%), pyloromyotomy (35%), and intestinal surgery (13%), as well as Nissen fundoplication (7%) and gynecologic adnexal pathology (7%) (Fig. 3). Other isolated or lower-volume SIPES procedures that IPEG members have performed included urologic surgery (pyeloplasty), hernia/varicocele repair, pulmonary resection, diaphragmatic hernia repair, gastrostomy tube placement, liver resection, adrenalectomy, tissue biopsy, sleeve gastrectomy, abdominal mass resection, and ventriculoperitoneal shunt placement.
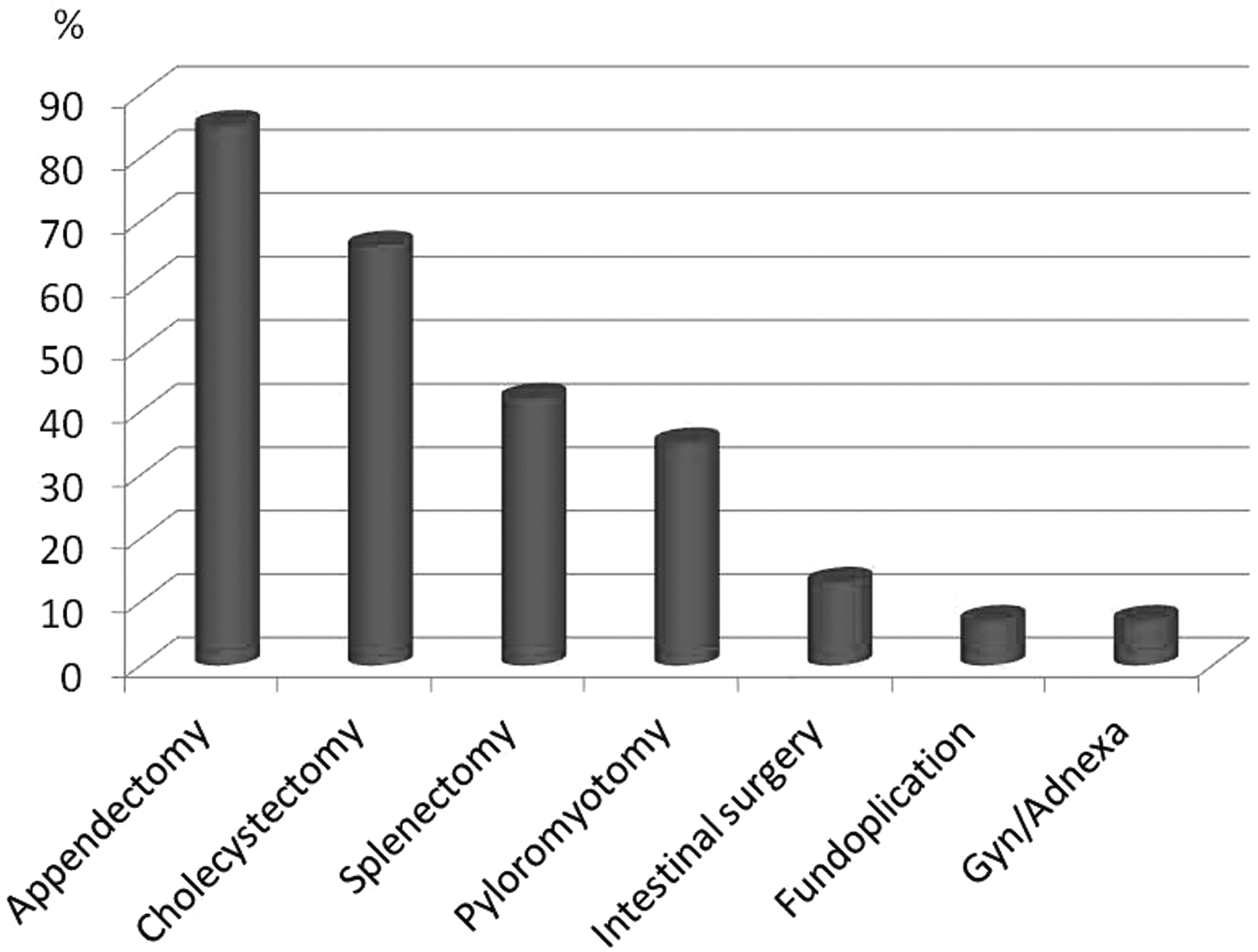
Proportion of surgeons queried performing specific single-incision pediatric endosurgery procedures. The most frequently performed procedure is appendectomy, followed by cholecystectomy and splenectomy. About one-third of respondents routinely performed pyloromyotomy using single-incision pediatric endosurgery. Gyn/Adnexa, gynecologic adnexal.
Appendectomy was the most common SIPES procedure performed. Of respondents who performed this procedure, 47% also use SIPES for perforated appendicitis. Characteristics that would prevent respondents from using SIPES for appendectomy were a retrocecal appendix seen on prior imaging, obesity, previous abdominal surgeries/adhesions, marked distention/intestinal obstruction, an appendiceal mass, or small size of the patient. Approximately 44% resect the appendix intracorporally, whereas the remainder completes the resection extracorporally. Forty-seven percent of respondents who perform SIPES appendectomies use commercially available single-site trocars, whereas 8% create their own. Sixty-three percent of respondents who perform SIPES appendectomy use special equipment, which include reusable bent instruments, single-use articulating instruments, a bariatric laparoscope, an instrument channel operating laparoscope, an articulating camera, a percutaneous sling to retract the appendix, or magnets. The remainder use conventional laparoscopic equipment.
Cholecystectomy is the second most commonly performed SIPES procedure. Factors preventing respondents from performing SIPES cholecystectomy include acute/gangrenous cholecystitis, obesity, adhesions/prior operations, very small patients, and choledocholithiasis. Gallbladder retraction is achieved by transabdominal suture, a percutaneous needle (Mini-Lap™; Stryker® Endoscopy, San Jose, CA) grasper, a grasper through the umbilical site, a magnetic retractor, intraabdominal sutures, a needle T-fastener, or a combination of these techniques. Five respondents create their own trocars using gloves and household items, whereas most used commercial single-site trocars. Special instruments used for SIPES cholecystectomy were reusable bent instruments, single-use articulating instruments, a long bariatric laparoscope, and a Mini-Lap grasper, as well as an instrument channel operating laparoscope.
SIPES splenectomy is the third most common procedure performed by the survey respondents. Reasons respondents may not perform a SIPES splenectomy are for a massive splenomegaly, coagulopathy, patient size (excluding obese and very small patients), and idiopathic thrombocytopenic purpura. Most respondents use commercially available single-site ports or stacked standard laparoscopic trocars, whereas two create their own trocars specifically for this procedure. One respondent routinely has interventional radiology colleagues coil the splenic vessels immediately prior to the procedure. Special instruments used are multi-use bent instruments, single-use articulating instruments, vessel sealers, a flexible laparoscope, a long bariatric laparoscope, and magnetic retractors.
Figure 4 depicts the relationship between relative procedure volume and experience for appendectomy (Fig. 4A), cholecystectomy (Fig. 4B), splenectomy (Fig. 4C), pyloromyotomy (Fig. 4D), adrenalectomy (Fig. 4E), gynecologic procedures (Fig. 4F), and fundoplication (Fig. 4G).
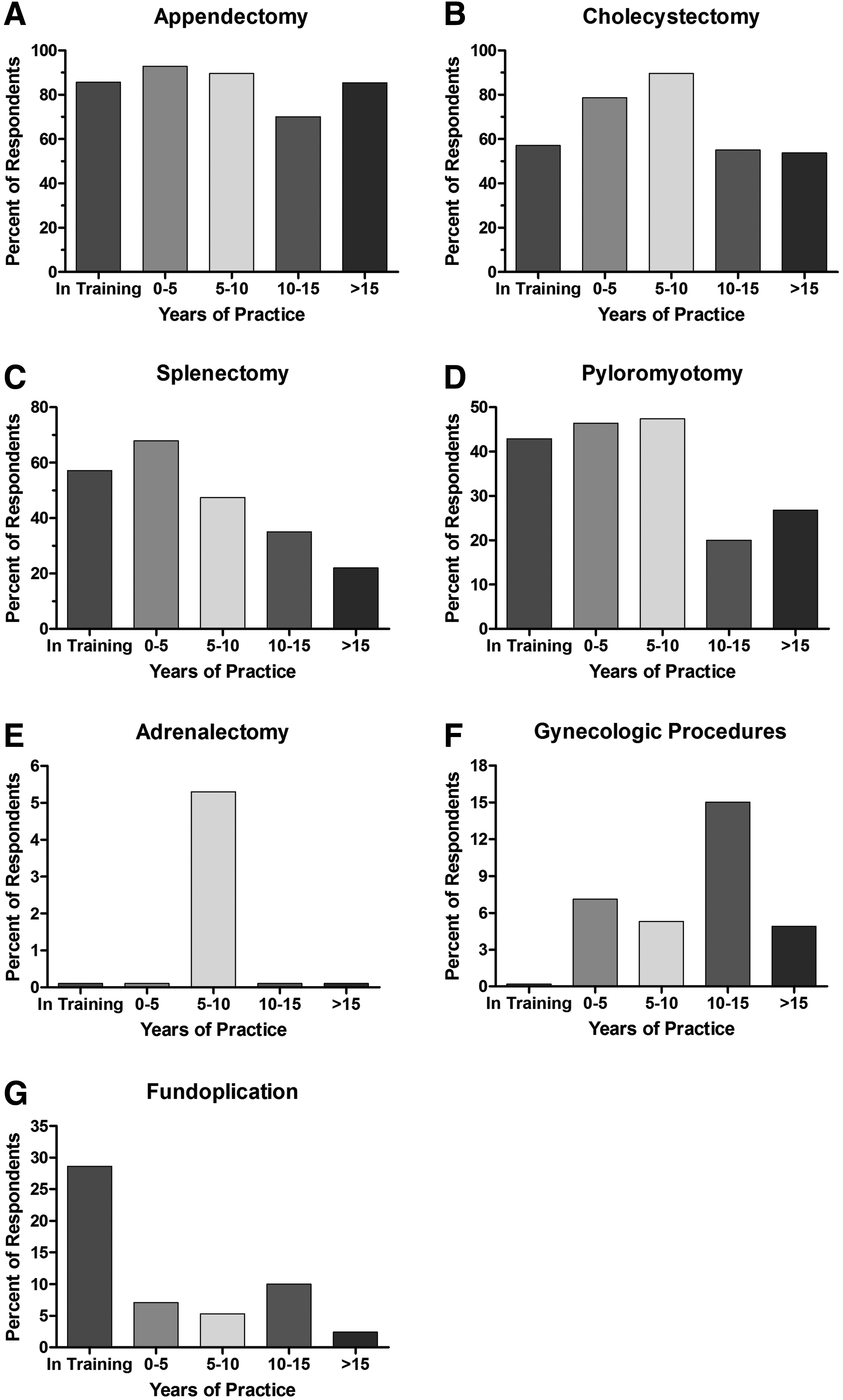
Percentage of respondents performing
In total, 29 complications were reported from 24 (21%) respondents by answering an open-ended question regarding their experience with surgery-related complications during SIPES. The most common complication reported was wound infection, which was reported 14 times (12% of respondents, 48% of complications). The remaining complications included bleeding (3%), prolonged operating time (3%), technical difficulties (2%), increased pain (2%). umbilical hernia (2%), seroma (1%), and wound dehiscence (1%).
The literature search using the described algorithm yielded 259 titles, of which 136 were relevant to SIPES. Table 2 is an overview of the countries of origin of the publications. The most prolific countries on the topic of SIPES were the United States, China, and Japan.
Discussion
SIPES is being performed worldwide for a large spectrum of common procedures in pediatric surgery. Although the main clusters of SIPES surgeons are located in the United States, Central Europe, and Southeast Asia, pediatric surgeons in remote areas and developing countries such as Bangladesh also perform these procedures. Literature on SIPES has been reported from groups within the United States, China*, Turkey, Germany, Japan, Colombia*, Belgium, United Kingdom, India*, Argentina, Russia, Sweden, Israel*, Korea, and Iran*1–13 (the * indicates that some SIPES centers were missed in our survey and are not represented in this study).
It is important to note that many terms, acronyms, and abbreviations have been proposed for SIPES. The most common ones are “single-incision laparoscopic surgery” (SILS), laparoendoscopic single-site surgery (LESS), or single-site laparoscopic surgery (SSLS). We believe that using the term SILS is problematic because one of the device companies has trademarked the term (SILS™; Covidien, Mansfield, MA), and its descriptive use for the technique therefore presents a conflict of interest. Furthermore, using the term “laparoscopic” instead of “endosurgical” omits thoracoscopic and retroperitoneoscopic operations, which were specifically included in this study. The term SIPES is not trademarked, is universal in the sense that it comprises the entire spectrum of single-incision endosurgical operations, and has been used and published as a term by surgeons of different specialties and backgrounds14–20 and disciplines, such as cardiothoracic surgeons. 21
Most SIPES surgeons work at academic university medical centers and are more likely to be experienced, with almost half of them in practice over 10 years. The majority did less than 5 SIPES cases in a month, although about one-fifth performed more than 10 cases. Lack of resources was a substantial obstacle for performing SIPES cases. Some pediatric surgeons overcame these limitations by constructing innovative, self-made umbilical access ports, particularly in developing countries.
Our study intends to report the current global state of the art of SIPES. However, due to methodical limitations, it can only be a snapshot of the current practice. For one, an invitation to participate in the survey was only sent out to the members of IPEG. The fact that the survey was conducted among surgeons who are members of an innovative, laparoscopic society naturally will skew the results. It would be difficult to obtain addresses of all pediatric endosurgeons around the world. Also, the recall of 21% is relatively low, causing recall bias. This is underscored by the fact that some countries were not represented in the survey, although surgeons from those particular countries had published on SIPES. There may have been language barriers as well for non–English-speaking surgeons. However, it can be presumed that pediatric endosurgeons performing SIPES are inclined to be IPEG members, and that of those, active SIPES surgeons would be more likely to take part in the survey out of interest in the field.
Pediatric surgeons are performing SIPES for a variety of procedures, using and limiting this technique based on an assortment of reasons including age, procedure, pathology, body habitus, technical capability, and perceived increased risk. The use of single-incision laparoscopic surgery was introduced initially in adults as early as 1969, 22 but it eventually followed in the pediatric population. It was first described in children by Esposito 23 in Naples, Italy, with an appendectomy using a single trocar in 1998. It is debatable whether the U-stitch gastrostomy introduced by Georgeson 24 in 1993 may be quoted as the first description of SIPES because the only incision except for the gastrostomy itself is made in the navel. Further indications have since been described in the literature, including cholecystectomy, splenectomy, gastrostomy tube placement, genitourologic procedures, intestinal procedures, pulmonary resections, Nissen fundoplication, hepaticojejunostomy, ventriculoperitoneal shunt placements, Heller myotomy, and diaphragmatic repairs.13,25–38 Our survey results demonstrate that additional pediatric procedures are being performed worldwide, which include liver resections, adrenalectomies, and sleeve gastrectomies.
Our survey also revealed that appendectomy is the most commonly performed SIPES procedure. Various reports have demonstrated the SIPES appendectomy to be both feasible and safe.39–41 Lacher et al. 42 reported a single-institution experience in 415 patients undergoing SIPES appendectomy. The study concluded that SIPES appendectomy is achievable with acceptable operative times and without increased complication rates. Of note is that SIPES appendectomy was carried out without additional port placement in 96% of patients. 42 A recent randomized control trial agrees that SIPES appendectomy is feasible, although the operating times were longer for SIPES in this study; however, no difference was seen in readmissions, tolerance of diet, fevers, or postoperative pain. 43 Both intracorporeal and extracorporeal techniques have been described for SIPES appendectomy, with slightly more than half of our respondents preferring an extracorporeal operation. Garey et al. 44 discussed the extracorporeal technique as a way to minimize the use of specialized instruments for SIPES. Almost half of the survey respondents are performing SIPES for perforated appendicitis, which has been shown to be feasible in the pediatric population 45 with no statistical difference between rate of wound infections, abscesses, length of postoperative stay, or operative times for perforated or interval appendectomy.
SIPES cholecystectomy and splenectomy are also well described in the literature, and our study shows that there is a wide diversity of techniques being performed. Nougues et al. 46 described the initial 25 patients undergoing SIPES cholecystectomy in a single institution using a percutaneous 2-mm grasper to retract the gallbladder; there were no complications reported or conversions to an open procedure. Five patients required the use of additional trocars. Similarly, Garcia-Henriquez et al. 47 reported 54 SIPES cholecystectomies using standard straight instruments without any conversions to open surgery; however, 2 patients required additional port sites. The authors reported a longer operative time in the single-incision group. Emami et al. 48 compared the single-incision approach with the standard laparoscopic approach. Their single-incision procedure was performed using a polypropylene suture through the abdominal wall to suspend the gallbladder. This group also found longer operative times in the single incision group but no difference in duration of hospitalization. Reibetanz et al. 49 described a flexible restraint system for the gallbladder fundus to achieve triangulation in SIPES cholecystectomy. Additional ways our respondents describe gallbladder retraction include a magnetic retractor, an intraabdominal suture, a needle T-fastener, or a combination of these techniques. SIPES splenectomy has also been well described, and, again, our respondents are using an assortment of methods. Bell et al. 50 described 7 patients undergoing single-incision splenectomy and compared them with standard laparoscopic splenectomy. They described stomach retraction with a suture to expose the short gastric vessels. Operative time improved with experience, and none of the single-incision patients had any complications or required additional trocars or conversion to an open approach. For both of these procedures, Garey et al. 44 described the use of standard instruments by placing a grasper beside the single incision port.
It is interesting that simple operations such as appendectomy and cholecystectomy were performed by surgeons of all levels of experience more uniformly than the more complex procedures. Younger surgeons with less than 10 years in practice were more likely to perform SIPES splenectomies and pyloromyotomies, whereas gynecologic SIPES procedures were more likely to be performed by the older surgeons. Almost one-third of respondents in-training were doing fundoplications. It will be interesting to see if the next generation of pediatric endosurgeons will tackle even more complex, reconstructive procedures in the future.
Some encountered complications are common to those seen with conventional minimally invasive surgery, whereas others may be SIPES-specific. The complications detailed in this survey have been described in standard laparoscopic procedures as well. It is difficult to ascertain whether these complications would have occurred using standard laparoscopic techniques. Although not per se a complication, prolonged operating times were included as a potential adverse effect of SIPES. Further prospective studies should be completed to better understand the relative risk of SIPES compared with standard laparoscopy.
The utilized equipment and techniques used internationally for SIPES show large variation and include some self-devised, innovative, low-resource approaches. This survey not only serves to report the current state of SIPES in the IPEG community, but also serves as a plea for networking among centers in an effort to standardize techniques, clarify the need for innovative instruments, and study these novel approaches systematically.
Footnotes
Acknowledgments
The authors would like to thank the members of the IPEG research committee for their revisions of the survey form, particularly Pablo Laje, Shawn D. St. Peter, David Juang, and Edward Esteves. This research was funded by a grant from Karl Storz Endoscopy.
Disclosure Statement
No competing financial interests exist.