
Abstract
Abstract
Background:
Recently, robot-assisted neck dissection (ND) using a transaxillary approach in thyroid cancer patients with lateral neck metastases (LNM) was demonstrated to be feasible. The aim of this study was to compare the surgical outcomes of a modified transaxillary and retroauricular (TARA) versus a conventional transcervical approach in papillary thyroid carcinoma (PTC) patients with LNM.
Patients and Methods:
In total, 47 patients with PTC underwent total thyroidectomy with central compartment ND and modified radical ND except Level I. Twenty-two NDs were performed via the TARA approach, and 25 unilateral NDs were performed via the conventional transcervical approach.
Results:
The TARA and the open ND groups consisted of 22 and 25 patients, respectively. The operation time for ND in the TARA group was longer than that in the open ND group (209.4±38.2 minutes versus 143.1±30.5 minutes; P=.000). The mean scar satisfaction score in the TARA group was higher than in the conventional ND group (3.9±1.0 versus 2.8±1.0; P=.000). There were no differences in the mean number of retrieved lymph nodes.
Conclusions:
The robot-assisted ND via the TARA approach can be an alternative option that produces excellent esthetic results for the management of LNM in PTC patients.
Introduction
C
According to studies examining the pattern of nodal metastasis in PTC, although the incidences of lymph node metastasis in Level IIB were 21% 4 and 22%, 5 the incidence of metastatic disease in Level II ranges from 52% to 72.2%.6,7 These sizeable figures prompted us to devise a modified approach, called the transaxillary and retroauricular (TARA) approach, which was shown to be feasible for the management of nodal metastasis in head and neck cancer. 8
The aim of this study was to compare the surgical outcomes of the TARA approach with those of a conventional transcervical approach for the management of LNM in PTC. We describe the application of the TARA approach to the management of LNM in PTC with the expectation that it would lead to superior clearance of Level II nodes.
Patients and Methods
Patients
After approval was obtained from the Institutional Review Board of Severance Hospital, Yonsei University College of Medicine, Seoul, Korea, patients with PTC and LNM were enrolled in this study. From June 2010 to April 2012, in total, 47 patients with PTC underwent total thyroidectomy with central compartment neck dissection (CCND) or total thyroidectomy with modified radical neck dissection (MRND) except Level I at our institution.
The inclusion criteria were as follows: (1) biopsy-proven PTC in LNM, (2) no previous treatment for PTC, and (3) nodal metastases without extracapsular spread on preoperative imaging studies. Patients with the following criteria were excluded: (1) recurrent tumor, (2) distant metastasis at the initial presentation, or (3) suspected extracapsular spread of LNM.
The selection of the approach method for neck dissection (ND) was based on the patient's preference after the patient was fully informed about the advantages and disadvantages of each approach. Informed consent was obtained from every patient.
The following variables were assessed: age, gender, operation time for ND, total amount of postoperative drainage, duration of drainage, duration of hospital stay, perioperative complications, primary tumor size, and mean numbers of retrieved and metastatic lymph nodes by neck level. Postoperative thyrotropin (thyroid-stimulating hormone [TSH])-suppressed serum thyroglobulin (TG) levels were checked at 1 month after surgery and before radioactive iodine remnant ablation (RRA) was performed. All patients underwent high-dose (150 mCi) RRA postoperatively. TSH-stimulated serum TG levels after RRA were also checked. Scar satisfaction scores were measured at 3 months postoperatively using a 5-point scale (1=extremely dissatisfied, 2=dissatisfied, 3=average, 4=satisfied, and 5=extremely satisfied). The mean follow-up period was 16.8±11.7 months. A single surgeon (Y.W.K.) performed all operations in this study.
Operative techniques
Robot-assisted total thyroidectomy, CCND, and MRND via the TARA approach
The detailed procedures for the TARA approach were described previously, 6 and the overall concept is depicted in Figure 1. In brief, a retroauricular (RA) incision was made around the RA sulcus and the hairline. After flap elevation (Fig. 2A), the posterior belly of the digastric muscle was sought by dissecting the lower border of the submandibular gland. The spinal accessory nerve (SAN) was identified at the posterior border of the sternocleidomastoid muscle (Fig. 2B). The entire course of the SAN was identified and skeletonized (Fig. 2C). While the sternocleidomastoid muscle was retracted laterally, Levels IIB, VA, and IIA, as well as the upper Level III, were dissected consecutively (Fig. 2D). A 7-cm incision was made at the anterior border of the axillary fossa, and the skin flap was elevated above the pectoralis major. The flap elevation was continued superiorly up to the previously dissected upper neck levels and medially to the contralateral thyroid gland. After a working space was created, a self-retaining retractor (Chung's retractor) was placed. A 30° endoscope was placed in the central arm of the da Vinci® surgical robot (Intuitive Surgical, Sunnyvale, CA) and inserted in the midline skin incision. Harmonic® (Ethicon, a Johnson & Johnson Company, New Brunswick, NJ) curved shears and Maryland forceps were placed on either side of the endoscope. The robot-assisted dissection of Levels III, IV, and VB via the transaxillary incision then proceeded (Fig. 3).
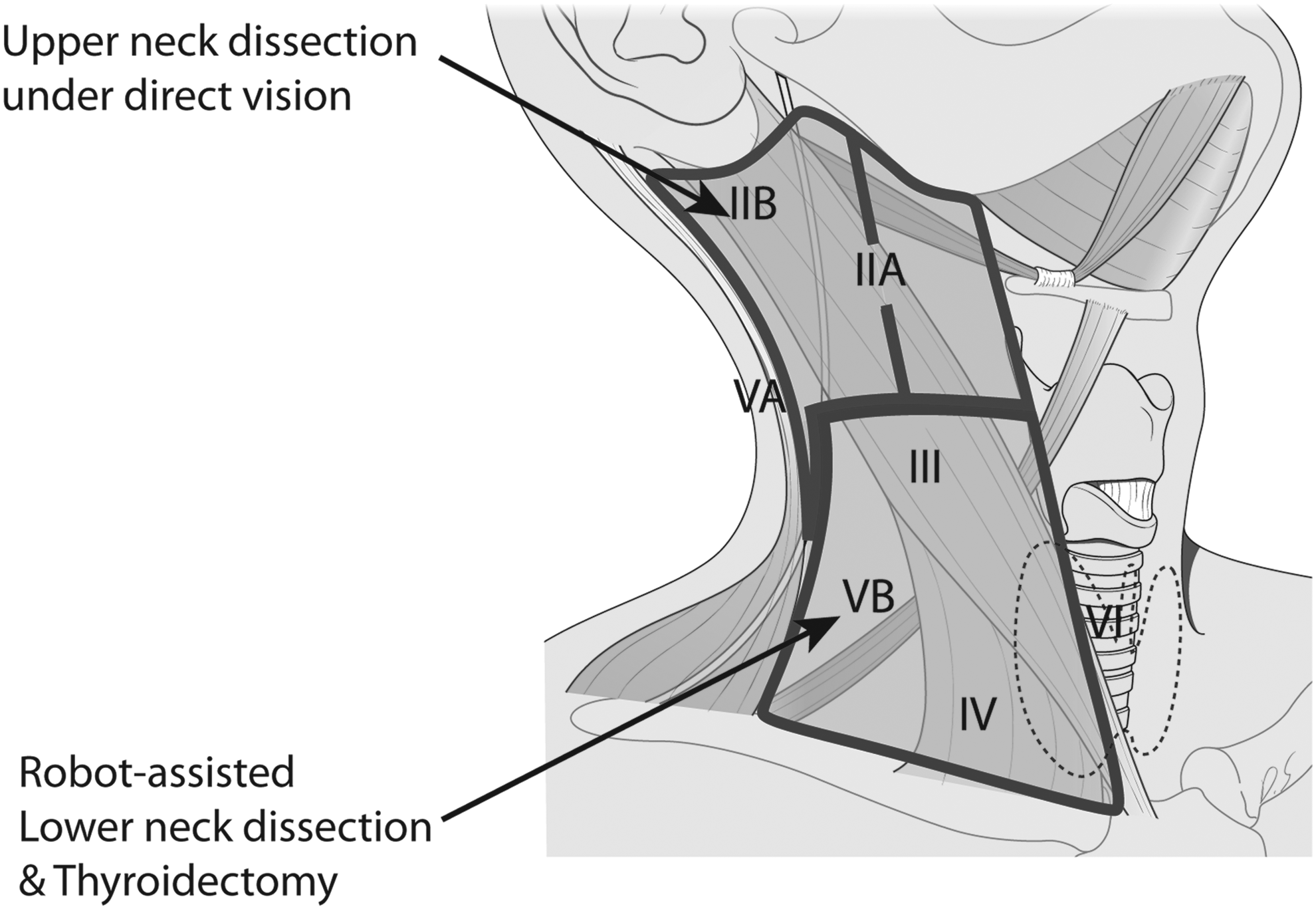
Schematic drawing of the transaxillary and retroauricular approaches. Upper neck dissection (Levels IIA, IIB, and VA, as well as the upper III level) can be performed under direct visualization through the retroauricular incision (upper outline). The medial aspect of the carotid space in Level IIA can be accessed via both the retroauricular and transaxillary approaches for the competent clearance of lymphofatty tissues. Robot-assisted lower neck dissection (Levels IV and VB) and thyroidectomy can be performed through the transaxillary incision (lower outline).
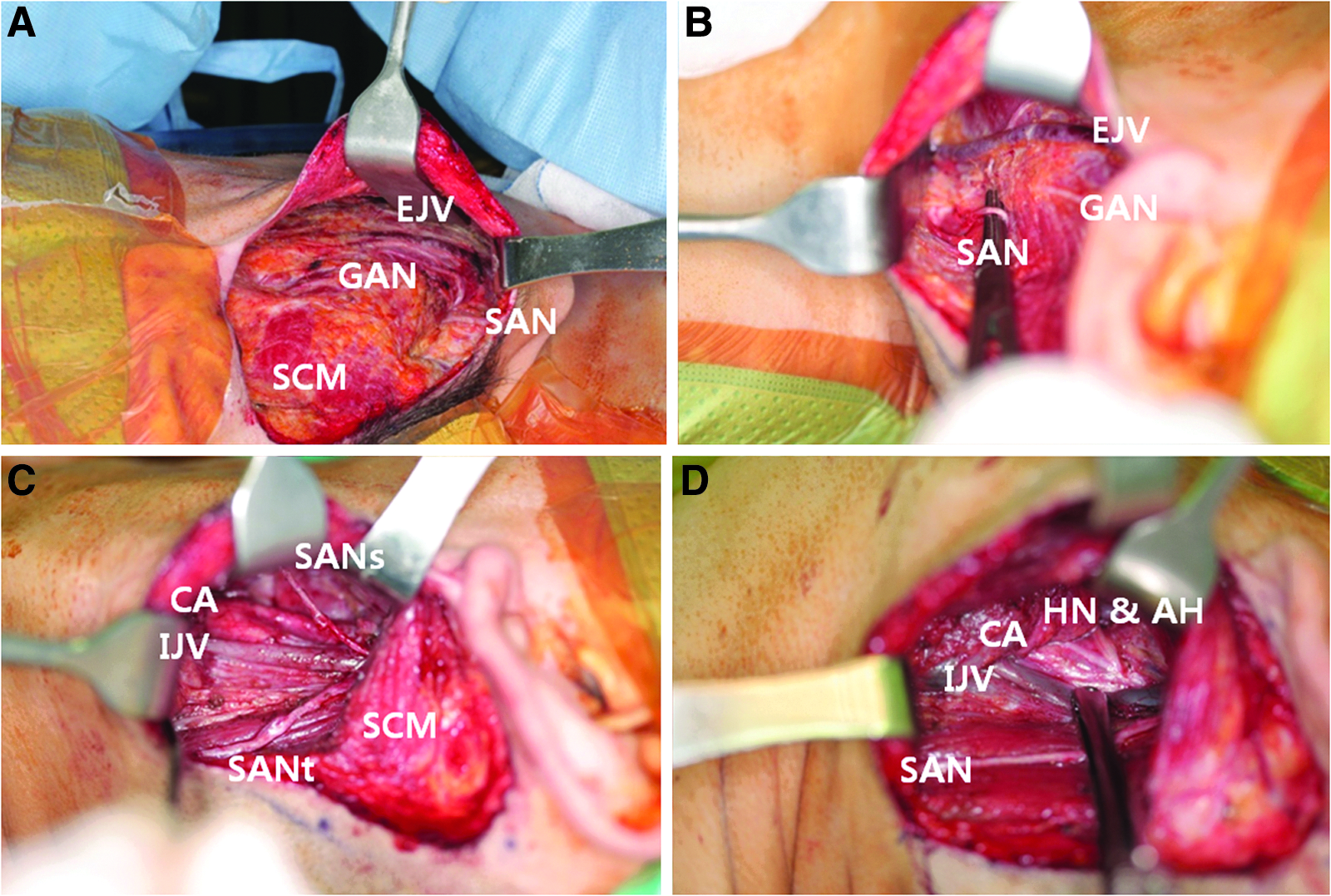
Upper neck dissection via a retroauricular approach under direct visualization.
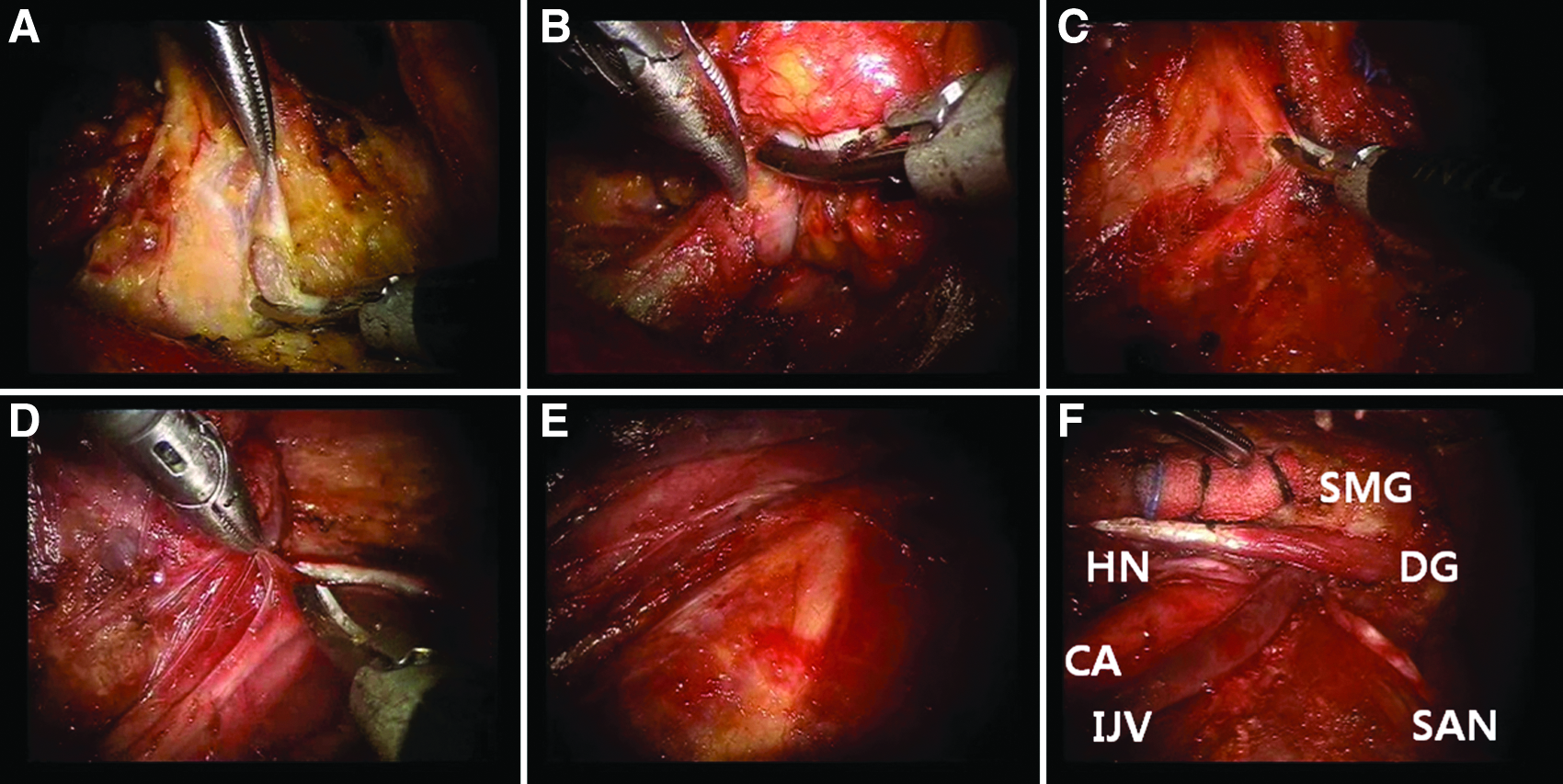
Robot-assisted neck dissection via a transaxillary port in the left side.
Total thyroidectomy and CCND procedures were performed via the transaxillary incision. A 1-cm skin incision was made in the areolar area, and ProGrasp™ (Intuitive Surgical) forceps were placed through the trocar. After exposure of its upper pole, the thyroid gland was drawn downward using the forceps. The superior thyroid vessels were ligated with Harmonic curved shears. The tracheal wall was identified as a midline reference point. The inferior thyroid artery was then ligated close to the thyroid gland. The thyroid gland was dissected from the trachea in Berry's ligament area, taking care not to injure the recurrent laryngeal nerve (RLN). The isthmus was resected, and the lobectomy specimen was extracted. A contralateral lobectomy was performed through the same incision by subcapsular dissection, preserving the parathyroid glands and the RLN. CCND was performed with preservation of the preidentified RLN. After removal of the specimen, the operative field was irrigated with sterile saline. A closed suction drain was placed through the transaxillary incision. After the subcutaneous layer was closed, the transaxillary incision was closed with a vertical mattress stitch, and the RA incision was closed with a simple suture technique.
Total thyroidectomy, CCND, and MRND via the conventional transcervical approach
A curvilinear single transverse incision about 10 cm in length was made two fingerbreadths above the sternal notch on the anterior neck. A skin flap was elevated superiorly to the lower border of submandibular gland, inferiorly to the clavicle, and laterally to the medial border of the trapezius muscle on the side of the ND. MRND was done first, and a total thyroidectomy with CCND was then performed using a Harmonic scalpel. The surgical field was then irrigated with sterile saline, and a closed suction drain was placed next to the skin incision. The subcutaneous layer was closed, and the skin was approximated with Steri-strips™ (3M, St. Paul, MN).
Statistical analysis
Statistical analyses were performed using Student's t test, the chi-squared test, Fisher's exact test, or the Mann–Whitney U test. Two-sided P values <.05 were deemed statistically significant.
Results
Patients, operative parameters, postoperative outcomes, and complications
Patient information, operative parameters, postoperative outcomes, and complications are shown in Table 1. The TARA group consisted of 17 females and 5 males with a mean age of 40.1 years. The open ND group consisted of 12 females and 13 males with a mean age of 45.3 years.
ND, neck dissection; RAND, robot-assisted neck dissection; RRA, radioactive iodine remnant ablation; RLN, recurrent laryngeal nerve; TG, thyroglobulin; TSH, thyroid-stimulating hormone.
The operation time for ND in the TARA group was significantly longer than in the open ND group (209.4±38.2 minutes versus 143.1±30.5 minutes; P=.000). The identification of the SAN, hypoglossal nerve, and RLN was successful in all cases. The mean postoperative serum TG levels (TSH-suppressed before RRA) in the TARA group and the open ND group were 0.31±0.58 ng/mL and 0.67±0.97 ng/mL, respectively (P=.119). The mean postoperative serum TG level (TSH stimulated) in the TARA group was 2.51±3.97 ng/mL and in the open ND group was 1.27±2.32 ng/mL (P=.207).
The mean amounts of drainage from the surgical site in the TARA group and the open ND group were 622.6±263.5 mL and 658.8±204.7 mL, respectively (P=.599). The mean drainage duration was 6.7±1.4 days in the TARA group and 7.4±1.9 days in the open ND group (P=.180). The durations of hospital stay in the TARA group and the open ND group were 9.2±1.8 days and 8.5±1.8 days, respectively (P=.192). In the TARA group, postoperative complications included 2 cases of postoperative seroma, 1 case of hematoma, 6 cases of transient hypoparathyroidism, and 1 case of chyle leakage. In the open ND group, there were 4 cases of seroma, 1 case of hematoma, 7 cases of transient hypoparathyroidism, and t2 cases of chyle leakage. All seroma cases resolved after needle aspiration. Each case of postoperative hematoma, regardless of procedure approach, was the result of minor bleeding from the skin flap and was successfully managed with a compressive dressing. All cases of transient hypocalcemia resolved within 2 months. Chyle leakages were managed with a fat-free diet and by placing a compressive dressing over the supraclavicular fossa; all resolved within 1 week. Six patients in the TARA group and 4 patients in the open ND group experienced postoperative numbness of the earlobe. Two patients in the TARA group and 2 patients in the open ND group experienced transient hoarseness, but none of these cases persisted for longer than a month. In all cases, the SAN, RLN, and hypoglossal nerve were successfully identified and preserved. There were no cases of temporary mouth corner deviation in either group. There were no cases of transaxillary or periareolar approach-specific complications (i.e., brachial plexus injury or skin flap injury) except chest wall seroma in 1 case in the TARA group. Overall, there were no significant differences in the development of postoperative complications between both groups. The mean scar satisfaction score in the TARA group was higher than that in the conventional ND group (3.9±1.0 versus 2.8±1.0; P=.000) (Fig. 4). The mean follow-up was 15.9±5.2 months in the TARA group, compared with 17.6±15.3 months in the conventional group (P=.607).
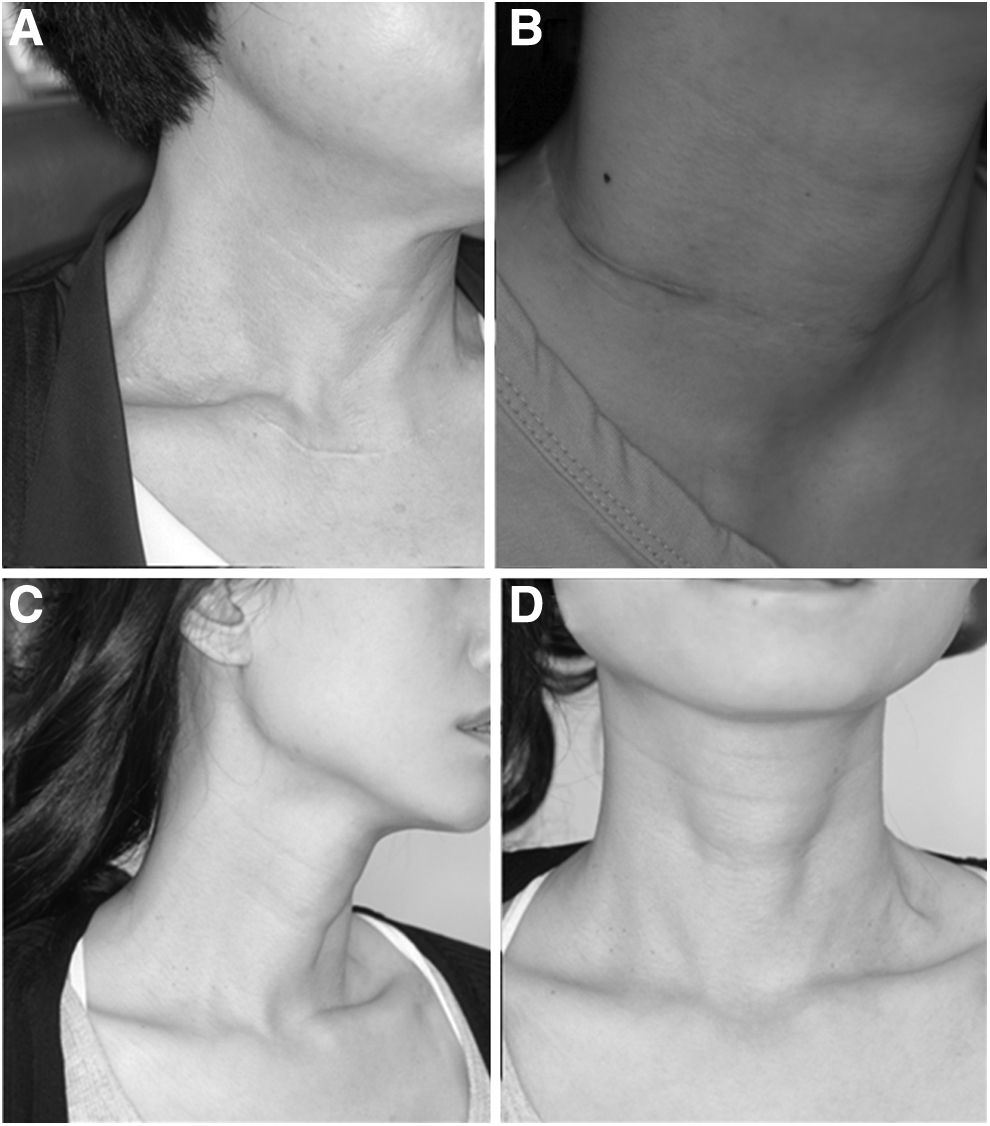
Postoperative photographs of patients who underwent total thyroidectomy with modified radical neck dissection.
Pathologic characteristics
The pathologic characteristics are summarized in Table 2. The mean primary tumor size was 11.68±6.80 mm in the TARA group and 12.20±7.48 mm in the open ND group (P=.806). Eleven cases in the TARA group and 7 cases in the open ND group had multiple thyroid gland lesions (P=.144). Six cases in the TARA group and 9 cases in the open ND group had evidence of thyroid capsular invasion (P=.550). Three cases in the TARA group and 2 cases in the open ND group had expanding margin (P=.654). There were no significant differences in the mean number of retrieved lymph nodes by neck level or in the absolute total number of lymph nodes retrieved except in the mean number of retrieved lymph nodes of Level IIB. The mean number of retrieved lymph nodes of Level IIB was 4.09±2.43 in the TARA group and 2.36±1.85 in the open ND group (P=.008). Incidences of lymph node metastasis in (1) Level IIB, (2) Level VA, and (3) the sum of Level IIB or VA were (1) 19.1% (9/47) (22.7% [5/22] in the TARA group, 16.0% [4/25] in the open ND group), (2) 4.3% (2/47) (0% [0/22] in the TARA group, 8.0% [2/25] in the open ND group), and (3) 21.3% (10/47) [22.7% (5/22) in TARA group, 20.0% (5/25) in the open ND group], respectively. The differences in the number of pathologic lymph nodes by neck level and in the mean number of total pathologic lymph nodes were not statistically significant.
CCND, central compartment neck dissection; LN, lymph node; MRND, modified radical neck dissection except Level I; ND, neck dissection; RAND, robot-assisted neck dissection.
Discussion
Recent progress in endoscopic and robotic technologies has enabled substantial advances in surgical techniques. With the introduction of endoscopic thyroidectomy, 9 minimally invasive surgeries aiming to minimize scar visibility have been extensively studied and widely applied in the field of thyroid surgery.10–12 In particular, Kang et al. 13 reported 338 cases of robotic thyroid surgery using a gasless transaxillary approach. They were the first to extend the indications for robot-assisted endoscopic surgery to include ND. 2 Adopting their method, we identified limitations to complete extirpation of upper-neck-level nodes by a cadaveric study and accumulation of our own experience. 3 According to studies documenting nodal metastasis patterns in PTC, the incidence of Level II including IIB lymph nodes cannot be disregarded, suggesting a need for a modified approach to completely remove upper-neck-level nodes.6–9 Following our report on the feasibility of the TARA approach in head and neck cancer, 8 we applied the TARA approach in the management of PTC with LNM, expecting competent extirpation of Level II lymph nodes.
There were no significant differences between the TARA group and the conventional ND group regarding the number of retrieved lymph nodes by neck level. Studies by Kang et al. 2 reported an average of 7.3 lymph nodes retrieved from Level IIA, and they did not routinely dissect Level IIB. Inclusion of Level IIB in our study may be one of the factors leading to a higher retrieval of Level II lymph nodes, although we cannot compare our results statistically with these earlier studies. However, we speculate that good accessibility under direct vision for Level II dissection and less concern regarding injury to the SAN and the hypoglossal nerve in the TARA approach may have helped with competent clearance of lymph nodes in that area.
Except for the operation time for ND, the operative parameters were comparable between the groups. The mean time required for ND in the TARA group was significantly longer than in the conventional ND group, mainly because of the flap elevation and docking time. Unlike open ND, the TARA approaches requires space for the robotic instrumentation. However, the time for flap elevation as well as the console time is decreasing with the accumulation of clinical experience, and we are currently planning a more in-depth study of the learning curve of RAND procedures via the TARA approach.
RAND via the TARA approach is not without weaknesses, particularly with regard to invasiveness. As we commented in our previous study, 12 the terms “endoscopic” and “robotic” do not necessarily imply “minimally invasive.” Although we can expect superior oncologic outcomes (i.e., competent retrieval of lymph nodes) with the TARA approach, it does tend to be more invasive than the more limited TA approach, which is already considered an aggressive approach compared with the conventional external approach. The TARA approach also faces criticism due to its excessive level of tissue dissection. However, the competent clearance of lymph nodes in which occult metastasis may exist cannot be overemphasized, even at the expense of procedural invasiveness. Although a prospective study regarding oncologic outcomes of open, transaxillary, and TARA approaches should be elucidated, we still speculate that the complete removal of lymph nodes in Level IIB and VA can be done via the TARA approach in cases of multiple LNM. However, we also advocate that the TA approach may be an option in cases in which there is no evidence of Level IIb or Va metastasis from preoperative imagings.
There are some limitations to this study. This was a retrospective review of two groups that were not randomized or matched. The decision as to surgical approach was made mainly by informed patient preference, which may have led to selection bias. In particular, in Korea, the procedural cost for RAND is about seven times that of conventional ND. In addition, unlike open ND, in which a landmark stitch within the specimen can be made to indicate the boundary of each neck level, the sorting of neck levels in robot-assisted ND is somewhat arbitrary. However, at our center, after the specimen is extracted, the surgeon divides each neck compartment very carefully in order to achieve accuracy. Finally, in this preliminary report, we were able to compare only the immediate surgical outcomes between the TARA group and the conventional ND group. We compared the postoperative serum TG levels of both groups before and after RRA and found no significant differences. Therefore, the reliability of the TARA approach as a method of surgical extirpation for PTC with LNM can be substantiated.
In conclusion, we successfully performed RAND via a novel TARA approach in PTC patients with LNM. The surgical outcomes of this approach were comparable with those of conventional ND. This approach is an alternative option with an excellent esthetic result for the management of LNM in PTC patients. The long-term outcomes of RAND via the TARA approach should be further assessed to determine its oncologic safety.
Footnotes
Acknowledgments
The authors thank D.S. Jang for his excellent medical illustration.
Disclosure Statement
No competing financial interests exist.