
Abstract
Abstract
Background:
Laparoscopic transcystic common bile duct exploration has become a safe and ideal treatment of common bile duct stones. This study was designed to explore the clinical value of modified laparoscopic transcystic common bile duct exploration as a first line of treatment for patients with common bile duct stones.
Patients and Methods:
A retrospective, case-control study of clinically comparable groups of patients who underwent the laparoscopic transcystic approach with micro-incision of the cystic duct and its confluence part in common bile duct exploration (LTM-CBD) (n=110) and laparoscopic common bile duct exploration (LCBD) (n=100) under the care of one surgeon was performed. All clinical data were analyzed retrospectively.
Results:
There was no significant difference in terms of operation time between the two groups (P>.05). Postoperative hospital stay and abdominal drainage time were shorter in the LTM-CBD group than in the LCBD group (P<.05). Postoperative bile leakage was seen in 1 case (1 of 110) in the LTM-CBD group and 10 cases (10 of 100) in the LCBD group (P<.05). Twenty patients underwent T-tube drainage in the LCBD group, and primary closure was performed in the other patients; however, all cases in the LTM-CBD group underwent primary closure. The median follow-up was 12 months; 2 patients in the LCBD group who suffered from bile leakage presented with obstructive jaundice due to bile duct stenosis 6 months postoperatively.
Conclusions:
LTM-CBD, which can avoid postoperative T-tube drainage, decrease complications, shorten hospitalization time, and enhance the existing quality, is a minimally invasive, safe, and effective treatment.
Introduction
T
In the present study, we investigated the role of the laparoscopic transcystic approach with micro-incision of the cystic duct and its confluence part in CDB exploration (LTM-CBD) as the routine treatment for patients with CBD stones and compared clinical outcomes in patients who underwent LTM-CBD and those who underwent LCBD.
Patients and Methods
Clinical design
From January 2009 to February 2013, 210 consecutive patients (120 women and 90 men) with CBD stones and gallbladder were included in the study. Blood exams, electrocardiograms, chest X-rays, and abdominal ultrasounds were performed on all patients. Magnetic resonance cholangiopancreatography was performed routinely to detect CBD stones in order to plan the procedure. Two clinically comparable groups of patients were studied: those undergoing LTM-CBD (n=110) and those undergoing LCBD (n=100) under the care of one surgeon.
Operative techniques
Transcystic approach
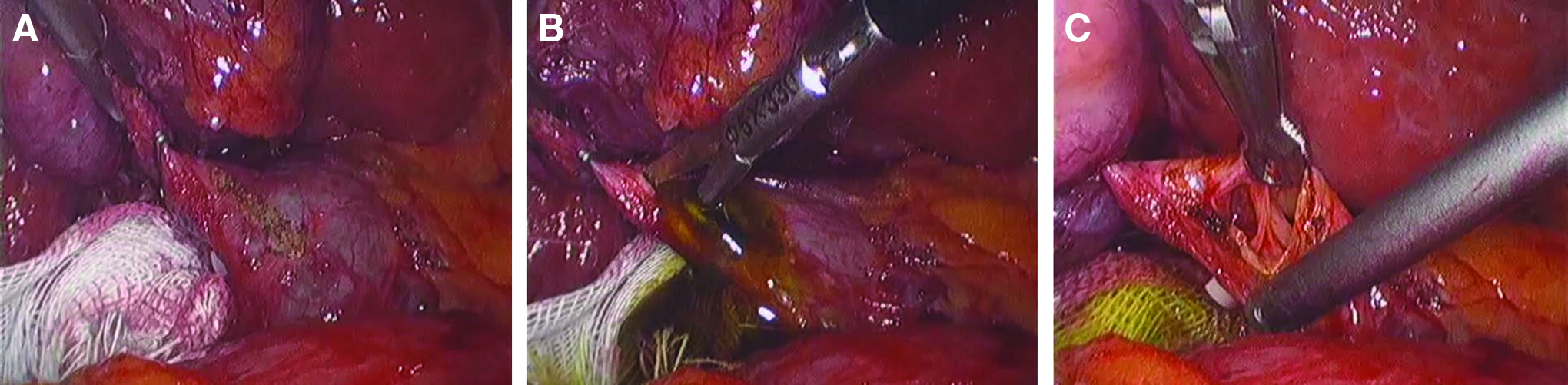
After general endotracheal anesthesia was administered to the patient, the operation was carried out by using the four-port technique: the first was a 10-mm supraumbilical camera port with a CO2 insufflation of 12 mm Hg (1 mm Hg=0.133 kPa), and the other three 5-mm ports (right upper quadrant) were inserted under videolaparoscopic (Karl Storz, Tuttlingen, Germany) vision. Laparoscopic cholecystectomy was performed in the standard anterograde fashion. Surgical gauze was inserted into the foramen of Winslow to prevent the stones from sliding into the lesser omental sac. After the cystic duct was exposed sufficiently, we slit the cystic duct, and the confluence part was cut open 3–5 mm at the supra and inferior margins (Fig. 1). A flexible choledochoscope with a high-resolution video camera was inserted through the cystic duct into the CBD. Careful manipulation of the choledochoscope was needed, avoiding any grasping with forceps. The stones were captured individually in a wire basket through the choledochoscope (Fig. 2). The basket and stones were withdrawn together from the cystic duct incision (Fig. 2). Once the stones had been retrieved, the incision was sutured (Fig. 3), and the cystic duct was ligated with a Hem-o-lok® (Tyco, Teleflex Medical, Research Triangle Park, NC).
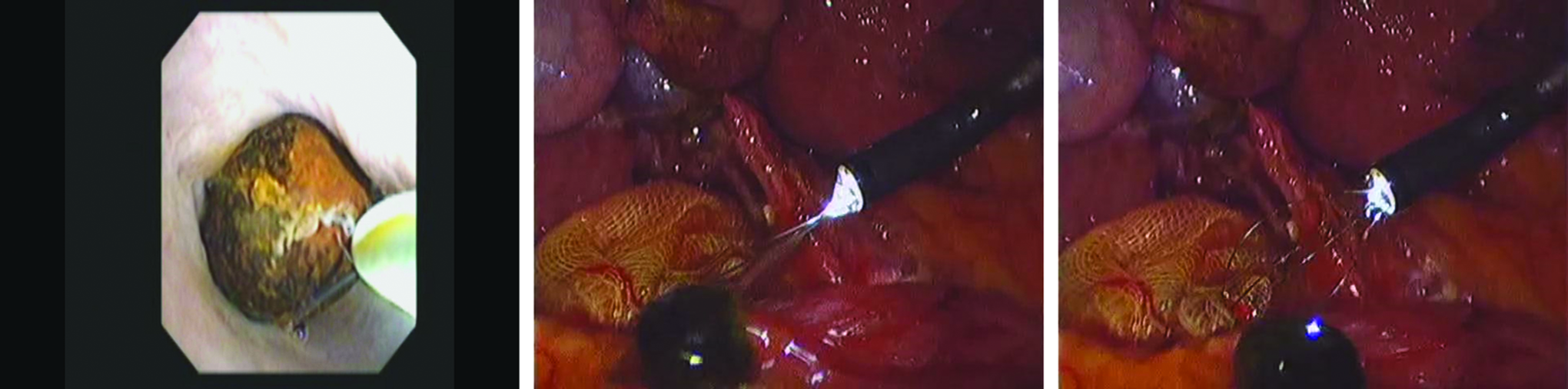
The stones were retrieved individually in a wire basket through the choledochoscope, and the basket and stones were withdrawn together from the cystic duct incision.

The incision was primarily closed with an interrupted suture.
LCBD
When the CBD was approached directly, the supraduodenal CBD wall was precoagulated to prevent bleeding, and then a longitudinal incision based on the stone was made using a microscissor. Then a flexible choledochoscope with a high-resolution video camera was introduced through the trocar. Proximal and distal choledochoscopy was performed with saline irrigation. Retrieval of residual stones, when present, was accomplished using a basket through the working channel of the choledochoscope.
T-tube drainage
A T-tube of appropriate size (5–7 mm in diameter) was inserted totally into the abdomen. The T limbs were maneuvered, with the use of grasping forceps, into the choledochotomy. After proper positioning, the choledochotomy was closed, using interrupted 4-0 absorbable sutures that were tied intracorporeally.
Primary ductal closure without biliary drainage
If the CBD was completely cleared, there was no debris or sludge in the CBD, and the papilla of Vater had no evidence of stenosis, the choledochotomy was primarily closed with an interrupted suture without biliary drainage.
A cavernous suction drain was placed beside the CBD incision in all patients after removal of the gallbladder and stones.
Follow-up
All patients were routinely assessed 12 months after discharge. B-ultrasonic examination and liver function tests were carried out in every patient.
Statistical analysis
Data were expressed as mean±standard deviation values. The two-tailed unpaired Student's t test or one-way analysis of variance was used to evaluate the statistical significance of differences, which was set with a value of P<.05.
Results
Both groups were clinically comparable in terms of age, sex, and American Society of Anesthesiologists scoring (Table 1). All operations were successful, and none was converted to open surgery. LTM-CBD was performed successfully in 110 patients; all cases in the LTM-CBD group underwent primary closure. LCBD was performed in 100 patients. T-tube placement was performed in 20 patients; primary closure was performed in other patients. The mean operative time was 100±30.4 minutes in the LTM-CBD group and 120±42.2 minutes in the LCBD group. There was no significant difference between the two groups (Table 2). Mean postoperative hospital stay was significantly lower in the LTM-CBD group compared with the LCBD group (3.6±0.9 days versus 7.9±1.0 days; P<.05) (Table 2). There was one postoperative complication among the LTM-CBD patients. One patient had bile leakage needing simple drainage for 7 days without re-operation. Bile leakage was observed in 10 of the 80 patients who received primary ductal closure in the LCBD group; however, in the patients with a T-tube there were no bile leaks after surgery. The suction drain was removed within 24–48 hours if no bile leakage was observed. In our series, we found that abdominal drainage time was longer in the LCBD group than in the LTM-CBD group because of bile leakage (4.5±1 days versus 1.8±0.5 days; P<.05) (Table 2). Retained CBD stones were not found in all groups on postoperative cholangiography. No other postoperative complications were observed in the two groups. There was no mortality during the hospital stay or at the follow-up 12 months postoperatively in all patients. In the follow-up period, recurrent CBD stones were found in 3 patients in the LTM-CBD group and 4 patients in the LCBD group. Two patients in the LCBD group who suffered from bile leakage presented with obstructive jaundice due to bile duct stenosis 6 months postoperatively.
ASA, American Society of Anesthesiologists; F, female, LCBD, laparoscopic common bile duct exploration; LTM-CBD, laparoscopic transcystic approach with micro-incision of the cystic duct and its confluence part in common bile duct exploration; M, male.
CBD, common bile duct; LCBD, laparoscopic common bile duct exploration; LTM-CBD, laparoscopic transcystic approach with micro-incision of the cystic duct and its confluence part in common bile duct exploration.
Discussion
The best treatment of choledocholithiasis must be simple, reliable, readily available, and cost-effective for most patients. Unfortunately, there is no consensus in the medical community as to how best to deal with CBD stones. ERCP for choledocholithiasis is still a widely used technique but is associated with a high complication rate (19%) and mortality (3%). Laparoscopic cholecystectomy can be combined with single-stage laparoscopic exploration of the CBD, either as a choledochotomy or as a transcystic procedure.9,10 Single-stage laparoscopic procedures have been compared with two-stage methods combining laparoscopic cholecystectomy with pre- or postoperative ERCP, and in randomized clinical trials the single-stage technique have been shown to have the advantages of shorter hospital stay and, according to some studies, lower postoperative morbidity.11,12 Although successful laparoscopic CBD exploration has been reported by many authors, from the earlier 1990s, most surgeons have considered this operation too demanding and have not yet accepted it as a preferable surgical approach for the removal of CBD stones.13,14 In particular, the transcystic approach seems to be ideal, as it enables us to clear the CBD stones and offers the same postoperative course as laparoscopic cholecystectomy does. 15 An important advantage of the transcystic approach is that it leaves the CBD and the sphincter of the duodenal papilla intact. Moreover, unsuspected CBD stones found by intraoperative cholangiography were extracted successfully by the transcystic approach in almost all patients.16,17 However, this approach has several technical limitations, and factors contributing to the failure of this approach sometimes were found to be unfavorable cystic duct anatomy, presence of stones of diameter >0.6 cm, or a large number of stones. In this study, we modified this approach: we slit the cystic duct, and the confluence part was cut open 3–5 mm at the supra and inferior margins. With this approach, it is easy to insert the choledochoscope into the cystic duct without balloon dilation. The clearing of the CBD using this approach, as described here, allows us to address CBD stones larger than 6 mm in diameter with a single procedure.
Laparoscopic transcystic CBD exploration and clearance of the bile duct have been reported to be successful in 70%–84% of all patients in whom it is attempted.18,19 In our series, LTM-CBD was performed successfully in all patients; our results suggested that using this modified technique may raise the operational success rate. All cases in the LTM-CBD group underwent primary closure. Primary closure was performed in 80 patients with LCBD. Martin et al. 20 stated that this is a simpler and less hazardous alternative to the use of the T-tube. However, in the present series, bile leaks occurred more frequently in the LCBD group than in the LTM-CBD group. Although all of the bile leaks ceased within a few postoperative days, this complication prolonged hospitalization. If the CBD diameter is smaller than 8 mm, a T-tube should be used in order to avoid the risk of postoperative stricture after suturing in the LCBD group. T-tube placement leads to a longer hospital stay, sometimes more than 4 weeks, in order to form a tract. However, we have never used the T-tube in the LTM-CBD group, although some CBD diameters are 6–8 mm, and no patient has bile duct stenosis in this group. These results suggested that this operative procedure could avoid the possibility of anterior CBD injury and postoperative stenosis.
Conclusions
In conclusion, the present study shows that LTM-CBD, which can avoid postoperative T-tube drainage, decrease complications, shorten hospitalization time, and enhance the existing quality, is a minimally invasive, safe, and effective treatment. Larger numbers of cases are needed to definitively validate this technique, but the preliminary results are very promising.
Footnotes
Disclosure Statement
No competing financial interests exist.