
Abstract
Abstract
Purpose:
To describe our initial experience of “off-clamp, non-renorrhaphy” laparoscopic partial nephrectomy (OCNR-LPN) with perirenal fat and Gerota's fascia reapproximation technique.
Patients and Methods:
Between August 2012 and March 2013, 24 consecutive patients underwent OCNR-LPN at our institution. After the renal mass excision, biologic hemostatics such as FLOSEAL™ and TISSEEL™ (both from Baxter Healthcare Corp., Deerfield, IL) were used, and the perirenal fat and Gerota's fascia were sutured for reapproximation.
Results:
All 24 consecutive patients underwent OCNR-LPN successfully. The warm ischemic time for all cases was 0 minute. Thirteen patients were noted to have a low (4–6) RENAL nephrometry score (RNS), and 11 patients had a moderate (7–9) RNS. The mean tumor size among this cohort was 2.9 (range, 1.2–6.0) cm, and the mean estimated blood loss was 243 (range, 50–700) mL. The mean hospital stay was 6.9 (range, 5–10) days. The mean percentage of postoperative estimated glomerular filtration rate change increased by 0.9%. No positive surgical margins were noted, and 2 patients with Grade III complication by the Clavien–Dindo classification were treated by endoscopic or radiological intervention.
Conclusions:
OCNR-LPN with the perirenal fat and Gerota's fascia reapproximation technique is feasible. Our initial experience with OCNR-LPN demonstrates encouraging results of minimal renal function loss and complications.
Introduction
N
Patients and Methods
Patient characteristics
After obtaining institutional review board approval and informed consent from all included patients, we reviewed prospectively collected medical records. Between August 2012 and March 2013, 24 consecutive patients underwent OCNR-LPN at our institution. Patients with clinical T1 renal tumors were candidates for OCNR-LPN, whereas individuals with complex tumors and high (10–12) RENAL nephrometry score (RNS) were excluded owing to technical difficulty. 17 In all cases, medical history, physical examination, laboratory data, abdominal computed tomography scan, and RNS were reviewed prospectively. After baseline data were obtained, the associated perioperative outcomes were analyzed, including estimated blood loss, hospital stay, preoperative and postoperative renal function (serum creatinine and estimated glomerular filtration rate [eGFR] by the modification of diet in renal disease method), and complication incidence (by the Clavien–Dindo classification). 18 Patients converted to hilar clamp or renorrhaphy LPN due to uncontrolled bleeding or opened calyceal system were excluded.
Surgical technique
First, the affected kidney was exposed via a transperitoneal approach. In brief, the hilar soft tissue was dissected, and the renal vessels were skeletonized, so that in the case of uncontrolled bleeding, a self-made Rummel tourniquet is hung on the renal vessels for quick vessel clamping with loaded Hem-o-lok® (Teleflex® Medical, Research Triangle Park, NC) clips (Fig. 1A). 19 After some initial experience, selected patients with low (4–6) RNS renal tumors were chosen to undergo renal mass excision without renal vessel manipulation. Using a monopolar hook electrode, dot or linear cauterization was used for mass margin scoring (Fig. 1B). The renal mass was then excised using cold 10-mm Metzenbaum scissors with approximately 5-mm safety margins (Fig. 1C). After tumor excision, the tumor bed was assessed for margins and an opened calyceal system. If the calyceal system had been compromised, the procedure was converted to hilar control LPN with quick loaded Hem-o-lok clips using the self-made Rummel tourniquet. Biologic hemostatics such as fibrin sealant (TISSEEL™; Baxter Healthcare Corp., Deerfield, IL), human thrombin, and bovine gelatin (FLOSEAL™; Baxter) were used for any bleeding in the area of mass excision (Fig. 1D). The space of the excised mass was then filled with SURGICEL® (Ethicon, a Johnson & Johnson Company, Cincinnati, OH) bolsters or Gelfoam® (Pharmacia & Upjohn Co., a Division of Pfizer, New York, NY) (Fig. 1E), after which both the perirenal fat and Gerota's fascia were reapproximated without parenchymal renorrhaphy using 3-0 polyglactin 910 (Vicryl™; Ethicon) continuous sutures (Fig. 1F).

The surgical approach in brief for “off-clamp, non-renorrhaphy” laparoscopic partial nephrectomy with perirenal fat and Gerota's fascia reapproximation.
Results
In total, 24 consecutive patients underwent OCNR-LPN without requiring hilar clamp or renorrhaphy. There was also no conversion to laparoscopic radical nephrectomy or open surgery. Patient characteristics and perioperative outcomes are summarized in Table 1. The warm ischemic time for all cases was 0 minute. Thirteen patients had low (4–6) RNS, and 11 patients had moderate (7–9) RNS. The mean tumor size was 2.9 (range, 1.2–6.0) cm, and the mean operative time was 80 (range, 40–120) minutes. The mean estimated blood loss was 243 (range, 50–700) mL. The mean hospital stay was 6.9 (range, 5–10) days. The underlying tumor was found to be clear cell renal cell carcinoma in 20 patients and papillary renal cell carcinoma in 4 patients. All specimens had negative surgical margins. After pathologic staging, 2 patients were found to be stage T3a, 4 were pT1b, and 18 were pT1a. The mean preoperative serum creatinine level and eGFR were 0.88 mg/dL and 91.3 mL/minute/1.73 m2, whereas respective values at 1 month postoperatively were 0.93 mg/dL and 92.1 mL/minute/1.73 m2. The mean percentage changes of serum creatinine level and eGFR at 1 month after surgery were both increases: 5.7% (−14.3% to +36.8%) and 0.9% (−29.7% to +19.5%), respectively.
eGFR, estimated glomerular filtration rate.
In total, 6 patients (25%) developed postoperative complications: one Grade I complication by the Clavien–Dindo classification (paralytic ileus), three Grade II complications (blood transfusions), and two Grade III complications (1 case of postoperative urine leakage and 1 case of perirenal abscess). It is notable that the patient with postoperative urine leakage had an RNS of 9 and minimal postoperative drainage through the Jackson–Pratt drain, which was removed on the postoperative third day. However, this patient showed minimal asymptomatic perirenal urine leakage on abdominal computed tomography scan and 99m-technetium-diethylenetriamine pentaacetic acid at 1 month postoperatively (Fig. 2A and B). The patient was treated with temporary ureteral stenting under local anesthesia. Another patient with a perirenal abscess had an RNS of 5. In this case, the abscess was diagnosed after discharge when the patient developed characteristic symptoms, such as flank pain, nausea, and vomiting. Such abscesses can be caused by inadequate percutaneous drainage of perirenal hemorrhage at the operation site. Accordingly, the patient was treated by percutaneous drainage and antibiotics (Fig. 2C and D).
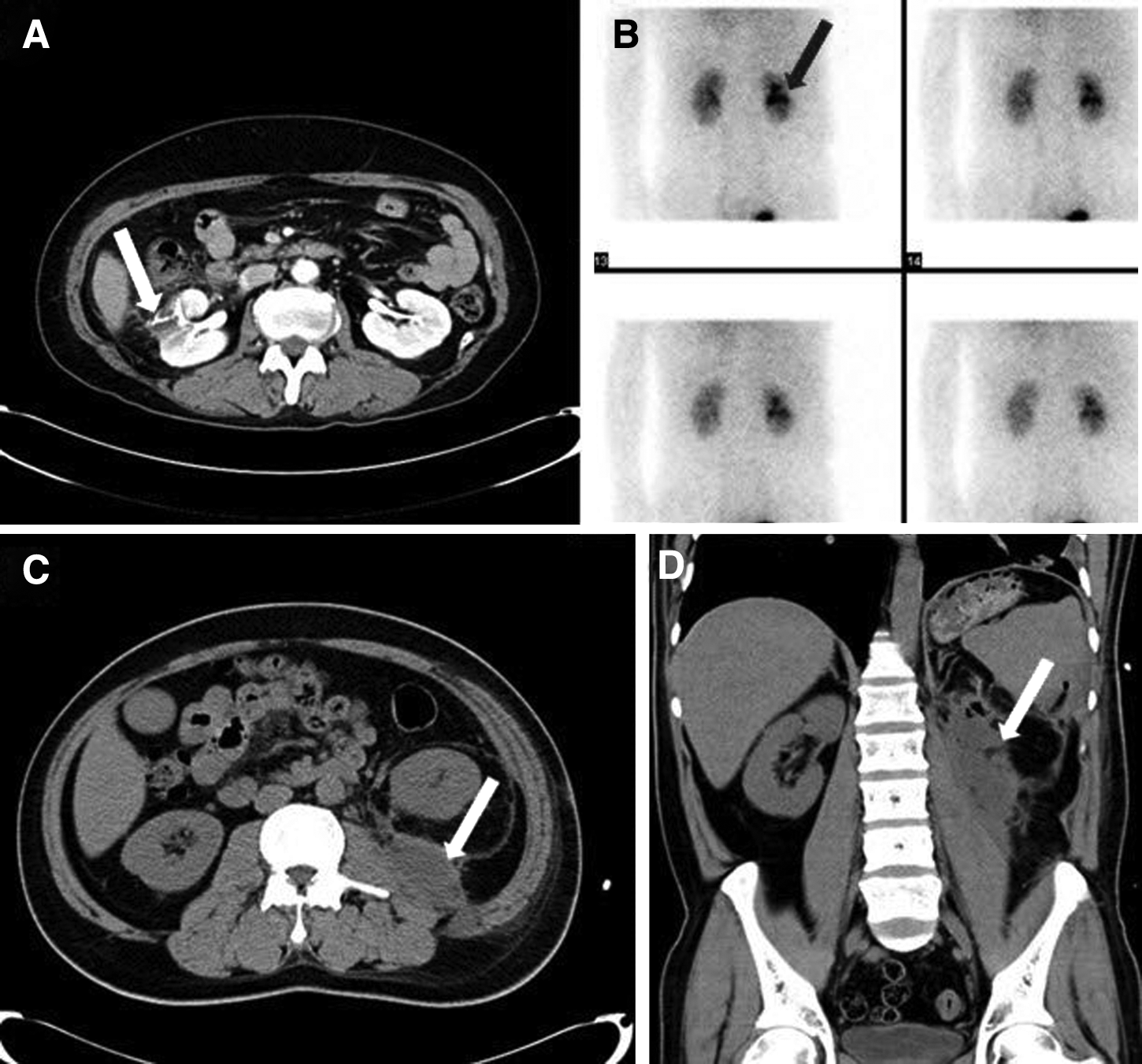
Two patients with Grade III complication by the Clavien–Dindo classification.
Discussion
LPN has now become a preferred surgical technique over laparoscopic radical nephrectomy, as the former is superior in terms of preservation of renal function and overall survival. However, the reduction of eGFR often cannot be avoided in the affected kidney if the renal pedicle is clamped.
Shao et al. 20 introduced the segmental artery clamping technique to minimize ischemic renal injury, which better preserves renal function than any previous surgical methods. Gill et al. 21 also described the zero ischemia technique, in which meticulous microdissection and clip ligation are performed, and reported almost no difference in renal function before and after surgery. The purpose of such techniques is to minimize the ischemic damage inflicted on the normal renal parenchyma. However, both of these procedures require further vessel dissection and can be difficult for inexperienced surgeons.
Conversely, the OC technique, which does not involve the microdissection of renal vessels, has not been associated with ischemic damage to the kidneys. Being able to easily control the bleeding in laparotomies, Smith et al. 22 were able to apply the OC technique in this setting, allowing for a more thorough analysis of oncologic and functional perspectives; in that study, OC was associated with superior preservation of renal function and did not affect oncologic outcome. In another solitary kidney subgroup analysis by Wszolek et al., 23 OC was not associated with any differences in oncologic outcomes and showed smaller reductions in eGFR (11.8%) when compared with hilar clamping (27.7%). In the present study, the early postoperative eGFR data were superior to those in our previous studies, which did not use OC. 24 Postoperative eGFR even increased in some patients, so these data may reflect postoperative hydration. Overall, postoperative eGFR changed very little, showing an increase of only 0.9%. However, as with all laparoscopic surgeries, the risk of intraoperative bleeding remains challenging. Although excellent outcomes have been reported with LPN after superselective angioembolization, the invasive nature of the access to the renal artery required for the angio-catheter is cumbersome in this technique. 25
To date, several reports have indicated that OC-LPN is both feasible and yields excellent preservation of renal function. Specifically, data from Rais-Bahrami et al. 14 indicate that OC was associated with excellent renal function preservation compared with the hilar clamping technique; the difference in renal function deterioration was largest in the case of pT1B when looking at by stages. Simone et al. 26 also suggested that OC without parenchymal suture be used in patients with low RNS; they reported excellent results for this challenging technique. In the associated study, only patients with renal mass sizes of ≤4cm and intraparenchymal depths ≤1.5 cm were included, and 94 patients (94%) had an RNS of 4. However, indications for this technique can be expanded to patients with moderate RNS based on our experience. The mean RNS in our study was 6; 45.8% of patients had moderate RNS, and 25% of patients had a renal mass >4 cm (stage pT1b or pT3a).
We applied fibrin sealant or human thrombin and bovine gelatin for continuous bleeding of the excision surface, then the renal defect was filled with surgical bolster, and reapproximation of the perirenal fat and Gerota's fascia was performed. After surgery, an abdominal computed tomography scan performed 1 month postoperatively often reveals a small hematoma-like lesion in the resected tumor site, which is likely resulted from blood clot aggregation from Surgicel bolsters or Gelfoam (Fig. 3B) and is almost absorbed within 3 months (Fig. 3C). In certain patients, the renal mass was directly approached, eliminating the need for renal vessel manipulation. For these cases, the entire surgical procedure could be performed in 1 hour. Although there is a risk of bleeding when renorrhapy is not performed, complications such as additional bleeding, parenchymal injury, and pseudoaneurysm formation can be reduced by avoiding suturing. For the reapproximation of perirenal fat and Gerota's fascia, it is recommended that the perirenal fat should be preserved except for the deposits around the tumors.
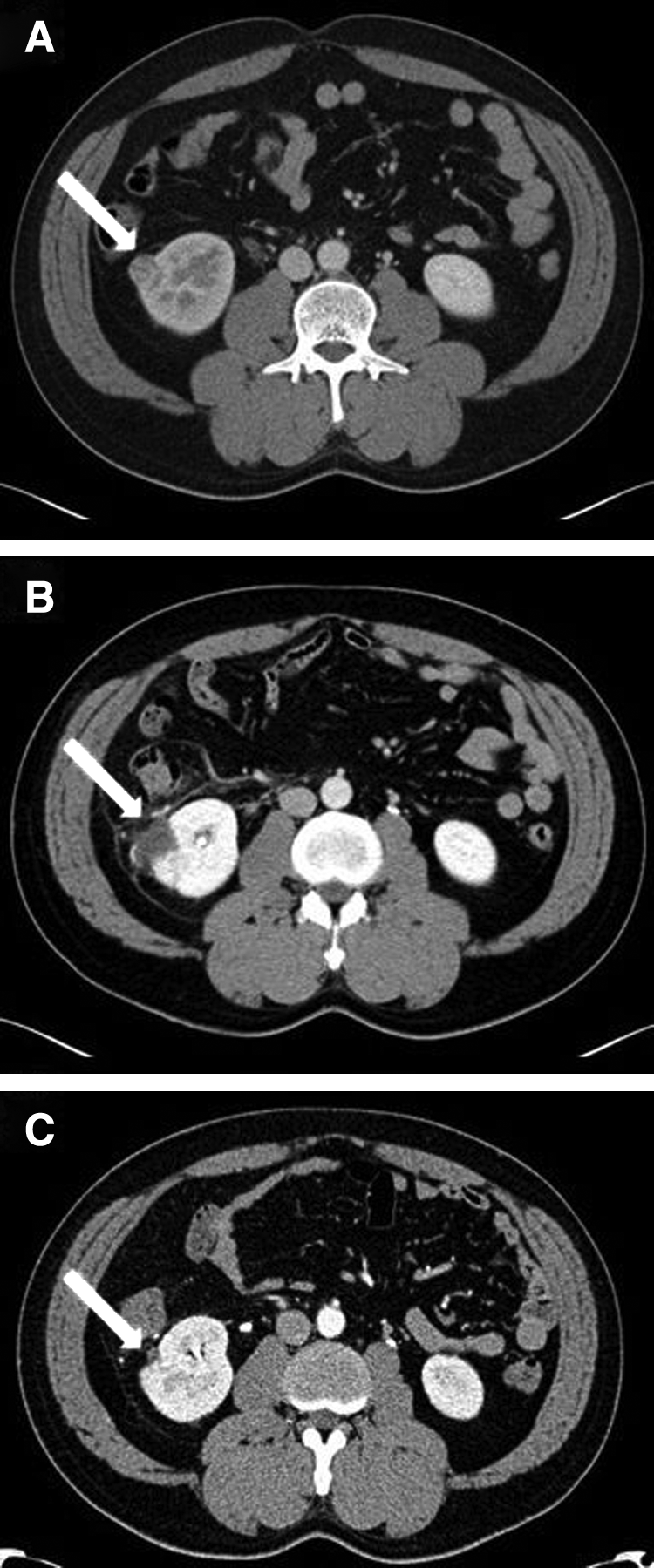
Typical findings on postoperative computed tomography scan in patients who underwent “off-clamp, non-renorrhaphy” laparoscopic partial nephrectomy with perirenal fat and Gerota's fascia reapproximation.
Inexperienced surgeons should try to narrow indications first and carefully consider cases of low RNS before surgery. Moreover, additional data from OCNR-LPN should be collected to further analyze and compare postoperative renal function, oncologic outcomes, and complications.
Conclusions
Surgeons with LPN experience may benefit from performing OCRN-LPN with reapproximation of perirenal fat and Gerota's fascia in selected patients. Our initial experience of OCNR-LPN revealed virtually no changes in postoperative renal function and minimal complications compared with conventional LPN.
Footnotes
Acknowledgments
This study was supported by a grant from Kosin University College of Medicine (2012).
Disclosure Statement
No competing financial interests exist.