
Abstract
Abstract
Background and Aim:
Advancements in minimally invasive surgery have led to increases in popularity of single-incision laparoscopic surgery (SILS) and natural orifice translumenal surgery (NOTES®; American Society for Gastrointestinal Endoscopy [Oak Brook, IL] and Society of American Gastrointestinal and Endoscopic Surgeons [Los Angeles, CA]) due to their postulated benefits of better cosmesis, less pain, and quicker recovery. This questionnaire-based study investigated Danish surgeons' attitudes toward these new procedures.
Subjects and Methods:
A 26-item questionnaire was developed and distributed electronically via e-mail to a total of 1253 members of The Danish Society of Surgeons and The Danish Society of Young Surgeons.
Results:
In total, 352 (approximately 30%) surgeons completed the questionnaire, 54.4% were over 50 years of age, and 76.6% were men. When choosing surgery, the most important factors taken into consideration were the risk of complication and short convalescence, whereas the least important factors were cosmesis and option of local anaesthesia. If the surgeons themselves were to undergo cholecystectomy, 35.5% would choose SILS, and 14.5% would choose NOTES provided that the risk was equal to traditional laparoscopy (3%). The fraction of surgeons willing to learn SILS and NOTES was 44.6% and 32.7%, respectively. The desire to learn was higher among less experienced and surgically active surgeons. Of the responders, 68.8% considered SILS and 43.2% considered NOTES would become standard techniques for cholecystectomy within 6 years.
Conclusions:
The importance of risk of complications has not surprisingly a high priority among surgeons in this questionnaire. Why this is has to be investigated further before implementing SILS and NOTES as standard of care.
Introduction
F
Neither SILS nor NOTES is the standard of care for cholecystectomies in Denmark, and NOTES cholecystectomy has only been carried out in a few humans in a protocolled study. A few surgical departments have introduced SILS, or example, for cholecystectomies and colorectal resections looking into differences between four-port laparoscopy and SILS with regard to complications, operating times, blood loss, recovery time, and postoperative pain.
Before the implementation of these procedures in Denmark, other factors also need to be taken into account. Apart from investigating the patients' opinions on recent developments of SILS and NOTES, an exploration of surgeons' perceptions of and willingness to perform NOTES and SILS is warranted. Some surveys have already been made in different parts of the world, which show a positive attitude toward minimally invasive surgery among surgeons with regard to performing cholecystectomies.9–13 However, Danish surgeons' attitudes toward this subject have never been further studied. The present questionnaire-based study reports on Danish surgeons' knowledge and willingness to learn the new procedures and which surgical technique they would prefer, if they themselves were patients in need of a cholecystectomy.
Subjects and Methods
A 26-item questionnaire was developed electronically and thereafter approved by The Danish Data Protection Agency (protocol number 2010-41-5530). The first half of the survey (Table 1) focused on demography, previous experience of surgery or endoscopy as a patient, significance of postoperative pain, scarring and risk of complications when choosing surgery, previous knowledge of SILS and NOTES, and personal preference for a cholecystectomy procedure. The second half of the survey focused on the surgeons' surgical experience and interest in learning SILS and NOTES. The questionnaire was designed to skip forward to the next relevant question, dependent on the given answer.
LESS, laparoscopic endoscopic surgery; NOTES, natural orifice translumenal surgery; SILS, single-incision laparoscopic surgery.
Survey population
The survey was presented electronically to all members of The Danish Society of Surgeons and The Danish Society of Young Surgeons after permission was obtained from each organization. Members of The Danish Society of Surgeons are mainly fully qualified surgeons, whereas members of The Danish Society of Young Surgeons are trainees. There are 990 surgeon specialists in Denmark, whereas the exact number of doctors in training remains unknown. To connect to the secure online survey (available at the Relationwise Web site [www.relationwise.dk]), a hyperlink was distributed by direct e-mail message to 823 of the members of The Danish Society of Surgeons and as part of a newsletter to 430 of the members of The Danish Society of Young Surgeons, both briefly describing the study. In total, 1253 survey requests were sent out. Because it was estimated that approximately 100 physicians were members of both associations, the number of recipients of the questionnaire was approximately 1153.
Study design
Participation in the study was voluntary and without compensation. The members of both associations were sent a reminder after 4 weeks to improve the response rate, but as the survey was anonymous it was not possible to send explicitly to those who had not yet answered the questionnaire. All recipients were asked only to open the hyperlink if they had not yet completed the survey.
Statistical methods
Data were collected anonymously and coded numerically when automatically transferred from the Web-based database to the statistical software (SPSS version 19.0; SPSS, Inc., Chicago, IL). Only responses from completed surveys were taken into account. The chi-squared test for categorical variables and the Kruskal-Wallis and Mann–Whitney tests for numerical variables were applied. A value of P<.05 was considered statistically significant.
Results
In total, 352 surgeons (approximately 30%) completed the questionnaire. The demographic data of the respondents are given in Table 2. The most important factor taken into consideration when deciding on future surgery was the risk of complication, whereas the least important factor was local anesthesia as the only method of anesthesia, with no significant difference between the genders (Fig. 1).
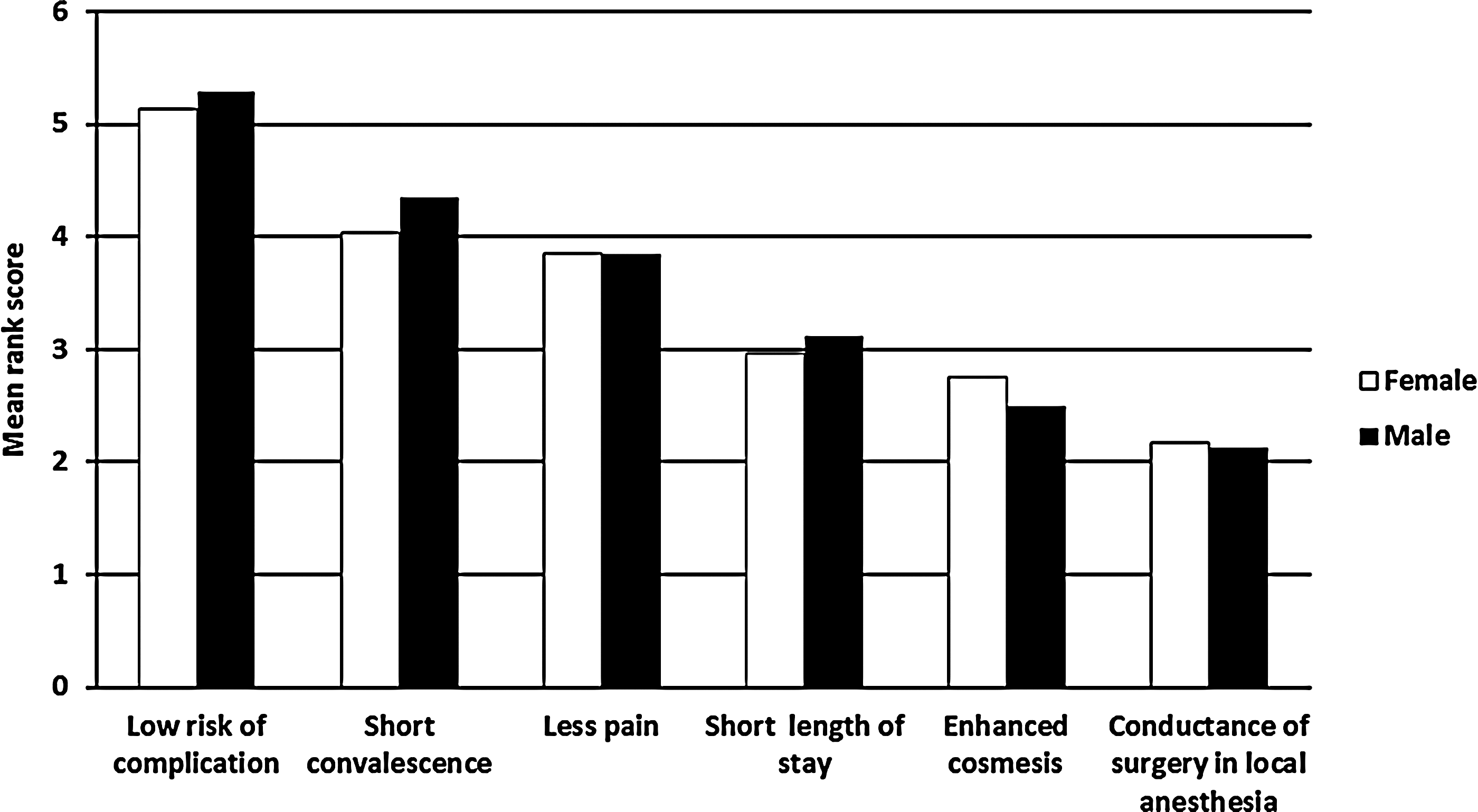
Surgeons' rating of considerations regarding choice of surgical technique for cholecystectomy. Each respondent ranked the given answers consecutively on a scale from 1 (least important) to 6 (most important).
Most of the surgeons were acquainted with the new minimally invasive techniques as 100% were familiar with traditional laparoscopy, 92.0% with SILS, and 89.2% with NOTES. When asked to choose as a patient among the three different techniques for a hypothetical cholecystectomy with equal risks, 176 (50.0%) favored traditional laparoscopy, 125 (35.5%) favored SILS, and 51 (14.5%) favored NOTES, with no significant difference between the genders. When asked about the reasons for choosing the different techniques, the majority chose laparoscopy because of its safety (n=145, 82.4%), cosmesis was not considered important (n=73, 41.5%), or SILS/NOTES was thought to be too risky (n=50, 28.4%). The most common reasons given for choosing SILS were the expectations of less pain (n=69, 55.2%), better cosmesis (n=67, 53.6%), or lower risks (n=31, 24.8%). For NOTES the expectation of better cosmesis (n=34, 66.7%), less pain (n=26, 51.0%), lower risks (n=14, 27.5%), and the unique technique (n=14, 27.5%) were the most frequent answers. With regard to choosing NOTES because of the expectation of better cosmesis, there was a significant difference between male (n=22, 57.9%) and female (n=12, 92.3%) surgeons (P=.023). Likewise, there was a higher rate of surgeons with less experience who gave cosmesis as a reason for choosing SILS (<10 years of experience, 77.4%; 10–30 years, 48.4%; >30 years, 40.6%; P=.004) and NOTES (<10 years of experience, 88.9%; 10–30 years, 67.7%; >30 years, 45.5%; P=.013).
There was no significant difference between surgeons who had undergone surgery or endoscopy and those who had not, with regard to their choice of surgical technique. If the perioperative risk was raised to 6%, a few would still choose SILS (9.6%) or NOTES (5.9%), and none would favor these techniques if the risks were up to 9% or 12%.
The fraction of surgeons who would like to learn SILS and NOTES was 44.6% and 32.7%, respectively. The surgeons with less experience reported the highest desire to learn the new techniques (Fig. 2). The remaining surgeons did not want to learn SILS (36.6%), did not know whether they wanted to learn or not (12.2%), or were already in the process of being taught the procedure (6.5%). With regard to NOTES, these percentages were 52.3%, 13.6%, and 1.4%, respectively. The reason why the surgeons did not wish to learn SILS was primarily that they either found the procedure irrelevant (n=93, 54.1%), outside their field (n=45, 26.2%), or too risky (n=17, 9.9%). A total of 28 (16%) could not specify any reason. The corresponding reasons given for the surgeons not desiring to learn NOTES were 104 (44.8%), 48 (20.7%), 60 (25.9%), and 41 (17.7%).
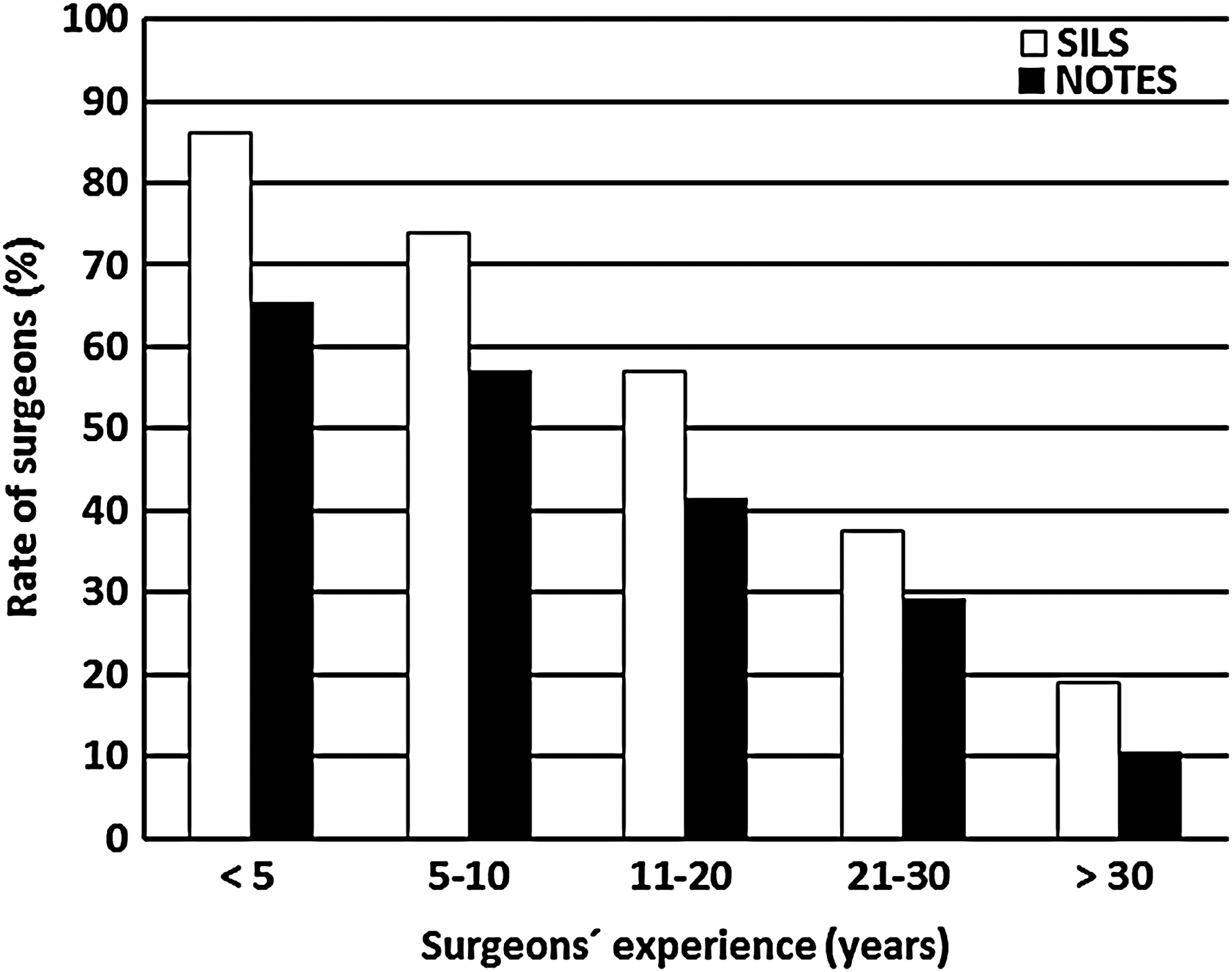
Fraction of surgeons willing to learn single-incision laparoscopic surgery (SILS) and natural orifice translumenal surgery (NOTES) versus duration of surgical practice.
There was an association between being surgically active during the 2 months prior to answering the questionnaire and the willingness to learn the new procedures. Of the 276 surgeons active in open surgery, 49.3% wished to learn SILS compared with 27.6% of the surgeons not actively doing open surgery (P<.005). For the 225 surgeons active in laparoscopy, 60.0% were willing to learn SILS, whereas only 17.3% of the surgeons not active in laparoscopy expressed such an interest (P<.005). The corresponding rates for surgeons actively performing endoscopy were 51.1% and 25.6% (P<.005). Likewise, the operatively active surgeons were more interested than the inactive surgeons in learning NOTES (for open surgery, 36.6% versus 18.4%; for laparoscopy, 42.2% versus 15.7%; and for endoscopy, 38.9% versus 14.4% (P<.01).
Even though a considerable number of surgeons would like to learn these new procedures, only a small fraction actually believed these new procedures will be the method of first choice for certain procedures in the near future. With regards to SILS, 64 (18.2%) of all the surgeons presumed this would occur within the next year, 183 (52.0%) within the next 3 years, and 242 (68.8%) within the next 6 years. This left 30 (8.5%) surgeons who did not think SILS has a future and 80 (22.7%) who did not know when or if it will become first choice. For NOTES the corresponding rates were smaller (13 [3.7%], 63 [17.9%], and 152 [43.2%], respectively). A total of 70 (19.9%) surgeons did not believe NOTES will ever become the first choice, and 130 (36.9%) did not have an opinion on this.
Discussion
This is the first study that surveys Danish surgeons and their attitudes toward two recently developed techniques of cholecystectomy. It has significant clinical relevance as it illustrates a positive attitude toward SILS and NOTES in younger Danish surgeons. The majority rated low risk as the most important factor when choosing the mode of operation, with cosmesis and possibility of local anesthesia as the least important factors. Most would therefore choose conventional four-port laparoscopy as the mode of cholecystectomy, reasoning that it is safe and cosmesis is not important. However, 50.0% preferred SILS or NOTES because they anticipated better cosmesis or less pain. They would, however, not choose these procedures if there was a higher operative risk compared with traditional laparoscopy.
This study shows that risk of complications is a factor that weighs heavily in the minds of surgeons, illustrated by the finding that more surgeons were willing to learn NOTES or SILS procedures than the number who would actually choose to undergo such a procedure themselves. Similar survey studies on patients have shown that they would be willing to except a higher risk than surgeons,2,14–19 with this difference perhaps reflecting the fact that surgeons are more aware of the degree of complications referred to. It is interesting, however, that nearly 10% of surgeons in the present study would choose to undergo these new procedures for a cholecystectomy, if these technique were associated with a hypothetical 6% complication risk compared with a corresponding 3% risk during conventional laparoscopy.
Gerö et al. 11 in Hungary investigated surgeons' attitudes toward NOTES compared with laparoscopy and found that 37% were willing to use NOTES, 49% would choose NOTES if undergoing a cholecystectomy, and 54% thought there was a demand for NOTES. Fan et al. 10 in Hong Kong found 46.5% of surgeons were willing to learn NOTES, 22.2% would choose NOTES as the mode of cholecystectomy, and 29.4% thought NOTES would be mainstream in surgery within the next 10 years. The surgeons also ranked factors of importance when choosing surgery in the same order, with risk, postoperative pain, and recovery time as most important and length of stay, cost, type of anesthesia, and cosmesis as least important. The same order in factors of importance was found by Volckmann et al. 9 in the United States. They also found a substantial interest among surgeons to learn NOTES (72%), but in agreement with the other studies, significantly fewer wanted to undergo NOTES procedures if they themselves were patients (26%). A total of 47% believed that NOTES would become mainstream in the future. This shows that our results are quite comparable with the other three studies, but distinctive concerning choosing NOTES over laparoscopy in a patient situation. This is probably because there was a third option (SILS) available in our survey when surgeons were asked about preferred method of operation, in contrast to the other surveys. We did, however, decide not to include open surgery as an option in our questionnaire because we wanted the decisions for the surgeon to be as close to everyday life as possible. Open cholecystectomy is only rarely offered as the primary option for the patient, but only used in terms of conversion during difficult laparoscopic surgery.
A limitation of the study is the response rate of approximately 30%, but it is hard to have made the settings easier accessible than they were with electronic questionnaires and e-mail reminders. The 352 responders were distributed throughout all ages and years of experience, suggesting that the survey represents the opinion of Danish surgeons. It is, however, plausible that surgeons either very enthusiastic or skeptical about these new techniques primarily decided to answer the questionnaire, raising the risk of bias. Moreover, despite the fact that the hypothetical risk of perioperative complications was set to 3% for all three techniques, most surgeons in a patient role preferred conventional laparoscopy, perhaps suggesting that the choices were biased by concerns of complications being more critical after NOTES or SILS than complications after conventional laparoscopy.
The risk profiles for SILS and NOTES need to be investigated further. Even though some work has already been done in this field with regard to cholecystectomy, the area is still not fully explored. In a review Joseph et al. 20 have recently found a slight increase in bile duct injuries during SILS compared with conventional laparoscopy, also pointing out that most trials done have been in patients without cholecystitis. Pollard et al. 6 reviewed articles on both SILS and NOTES procedures for cholecystectomy, observing a complication rate quite similar in SILS and NOTES but marginally lower than in conventional laparoscopy. The specific rates of bile duct lesion after conventional laparoscopy, SILS, and NOTES were 0.2%, 0.5%, and 0.8%, respectively. Fransen et al. 3 also reviewed articles on SILS and reported a favorable number of complications but also concluded that more randomized trials are needed to define the future role of these new techniques.
In conclusion, this questionnaire-based study demonstrates a potential platform for further development of both SILS and NOTES by less experienced and surgically active Danish surgeons, most of whom considered SILS as a standard procedure for cholecystectomy in the near future. Safety had the highest priority for surgeons, and until we know whether SILS and NOTES are as safe as conventional laparoscopy, surgeons must be cautious in implementing these techniques.
Footnotes
Disclosure Statement
No competing financial interests exist.