
Abstract
Abstract
Purpose:
Over the last 15 years thoracoscopic lobectomy for congenital and acquired lesions has become an accepted modality in pediatric thoracic surgery. There is still debate about the need to perform a complete lobectomy for some of these lesions, and some advocate observation rather than resection, despite possible long-term complications of untreated lesions. High-resolution computed tomography (CT) scans and physical findings at the time of surgery, along with new advanced techniques, now allow for discrete partial anatomic resections, which may preserve normal lung. This study evaluates the feasibility and early results using these techniques in selected cases.
Patients and Methods:
With institutional review board approval, the records of all patients undergoing thoracoscopic lung resection were reviewed. From January 2006 to December 2012, 23 patients, ranging from 1 month to 16 years of age and weighing 3.8–42 kg, underwent thoracoscopy for planned resection. Pathology was congenital cystic lung disease in 19 patients, bronchiectasis in 3 patients, and arteriovenous malformation in 1 patient. In each case findings on CT scan and at the time of surgery warranted consideration of lung-preserving surgery. Procedures were performed through three ports using single lung ventilation and CO2 insufflation to achieve lung collapse. The LigaSure™ device (Covidien, Norwalk, CT) was the primary instrument used to seal and divide the lung parenchyma and seal vessels.
Results:
All procedures were completed successfully thoracoscopically. An anatomic segmental resection was achieved in 22 of 23 cases. Operative time ranged from 30 to 300 minutes (mean, 120 minutes). Segmental resections included the left upper lobe apical/posterior (n=4), lingula (n=3), left lower lobe superior (n=5), medial or posterior basal (n=3), right middle lobe medial (n=1), right upper lobe apical (n=1), right lower lobe superior (n=4), and posterior basal (n=2). Two patients had more than one segment excised. Chest tubes were left in for 24 hours in 16 cases, 48 hours in 4 cases, and 5 days in 1 case. Hospital stay ranged from 1 to 6 days (mean, 2 days). Follow-up CT scans obtained at 1–6 years (mean, 28 months) show no residual disease in 20 of 21 patients. One patient underwent a nonanatomic resection and had evidence of recurrent congenital pulmonary airway malformation at the 4-year follow-up. This patient underwent a secondary thoracoscopic resection.
Conclusions:
Thoracoscopic lung-conserving therapy is technically feasible and safe in infants and children. The magnification provided by a thoracoscopic approach makes identification of segmental anatomic planes easier, aiding in safe dissection and resection. Anatomic resection appears to be associated with a low morbidity. It may be appropriate in the case of bilateral or extensive disease or in cases where the diseased tissue is clearly limited to an anatomic segment. Continued long-term follow-up is needed.
Introduction
T
Patients and Methods
With institutional review board approval the records of all patients undergoing thoracoscopic lung resection over the last decade were obtained, and those undergoing a less than complete lobectomy were reviewed. From January 2006 to December 2012, 23 patients, ranging from 1 month to 16 years of age and weighing 3.8–42 kg, underwent thoracoscopy for planned lung resection. The diagnosis preoperatively based on imaging studies was congenital pulmonary airway malformation (CPAM) and bronchopulmonary malformation in 19 cases, bronchiectasis in 3 cases, and arteriovenous malformation in 1 case. In most cases, findings on computed tomography (CT) warranted consideration of lung-preserving surgery. The final decision to attempt a segmental resection was based on anatomic findings at the time of thoracoscopy. The senior author was present in all cases. Procedures were performed through three ports using single lung ventilation and CO2 insufflation to achieve lung collapse. The plane of segmental resection was based on anatomic segmental blood and airway supply, not on gross parenchymal disease. In most cases the segmental arterial supply was first ligated to identify the plane of parenchymal dissection, then the airway, and then the parenchyma. The LigaSure™ device (Covidien, Norwalk, CT) was the primary instrument used to seal and divide the lung parenchyma and seal vessels.
Results
All procedures were completed successfully thoracoscopically. An anatomic segmental resection was achieved in 22 of 23 cases. Operative time ranged from 30 to 300 minutes (mean, 120 minutes). Segmental resections included the left upper lobe apical/posterior (n=4), lingula (n=3), left lower lobe superior (n=5), medial or posterior basal (n=3), right middle lobe medial (n=1), right upper lobe apical (n=1), right lower lobe superior (n=4), and posterior basal (n=2). Two patients had more than one segment excised. Chest tubes were left in for 24 hours in 17 cases, 48 hours in 5 cases, and 5 days in 1 case. Hospital stay ranged from 1 to 6 days (mean, 2 days). Follow-up CT scans obtained at 1–6 years (mean, 28 months) showed no residual disease in 20 of 21 patients. One patient underwent a nonanatomic resection and had evidence of recurrent CPAM at the 4-year follow-up. This patient underwent a secondary thoracoscopic resection.
Discussion
Complete excision of congenital lung malformations remains the gold standard treatment in pediatric surgery.6,7 Thoracoscopic lobectomy in children for such lung disease has been established and well described. Most surgeons agree on the benefits of a thoracoscopic approach over traditional thoracotomy, including less pain, shorter hospital stay, better cosmetic result, and decreased long-term morbidity, including shoulder girdle weakness chest wall deformity.8–10 We have previously documented the success of a thoracoscopic lobectomy with an average length of stay of 2.4 days, with minimal morbidity and no mortality. 9
However, many pediatric centers advocate a conservative nonoperative approach for asymptomatic congenital lung lesions, feeling that the asymptomatic prenatally diagnosed lesion is benign and does not warrant surgery.11,12 We feel nonoperative management is unacceptable because of the incidence of significant infection, up to 30%,13,14 and malignancy, which is rare but clearly documented.15–19 Others have advocated partial resections of grossly abnormal lung either by open thoracotomy or thoracoscopically.20,21 This approach seems unsatisfactory, as some of the disease is microscopic and not grossly visible, making complete resection difficult. We therefore feel an anatomic segmental resection is preferable when preoperative imaging and gross findings at the time of surgery strongly suggest the disease is limited to a single segment. Based on the embryologic development of the lung it is reasonable to assume that CPAM and bronchopulmonary malformation are a malformation of lung bud development and therefore, in some cases, may be limited to an anatomic segment. The pathogenesis of CPAM is uncertain but appears to result from an abnormality of the branching morphogenesis of the lung and represents a maturational defect. 22 The different types of CPAMs are thought to originate from different levels of the tracheobronchial tree and at different stages of lung development. Although the CPAM portion of the lung does not participate in normal gas exchange, there are connections to the tracheobronchial tree that can lead to air-trapping and respiratory distress in the newborn period. All of these anatomic relationships suggest that in certain cases resection along segmental planes would result in complete excision of the abnormal lung.
The exact embryologic basis for the development of bronchopulmonary malformation of the lower respiratory tract is also unclear. The lesion likely occurs early in embryologic development prior to the separation of the aortic and pulmonary circulations. 23 One explanation is that there is an abnormality in lung bud formation.24–26 This might result in not only bronchopulmonary malformation but also a spectrum of anomalies, including CPAM, bronchogenic cyst, foregut duplication, and even congenital lobar emphysema. Another explanation is that a portion of the developing lung bud is mechanically separated from the rest of the lung by compression from cardiovascular structures, traction by aberrant systemic vessels, or inadequate pulmonary blood flow. Either of these would suggest that there exists a plane between normal and abnormal lung, and if this could clearly be identified then normal parenchyma could be preserved along anatomic planes.
The other lesions we encountered were bronchiectasis from bronchial stenosis or atresia in 3 cases and a giant arteriovenous malformation in 1 case. These lesions were clearly limited to a single segment or segments, and anatomic segmentectomy resulted in complete resection and cure.
Segmental resection for lung preservation is a well-documented technique in adult thoracic surgery, often used in cases of isolated malignancy.27–30 These reports prove the safety and efficacy of this technique in adults, but there are no such reports in the pediatric surgical literature.
Reports in infants and children have been limited to nonanatomic resections. Johnson et al., 31 who have the largest report of nonanatomic resections, had an average chest tube duration of 3.7 days and an average hospital stay of 4.2 days, both nearly double that reported in this series. They also had one bronchopleural fistula requiring re-operation and recurrent disease in at least 1 patient. We believe nonanatomic resection runs a higher risk of postoperative complications as well as a higher risk of leaving behind diseased lung.
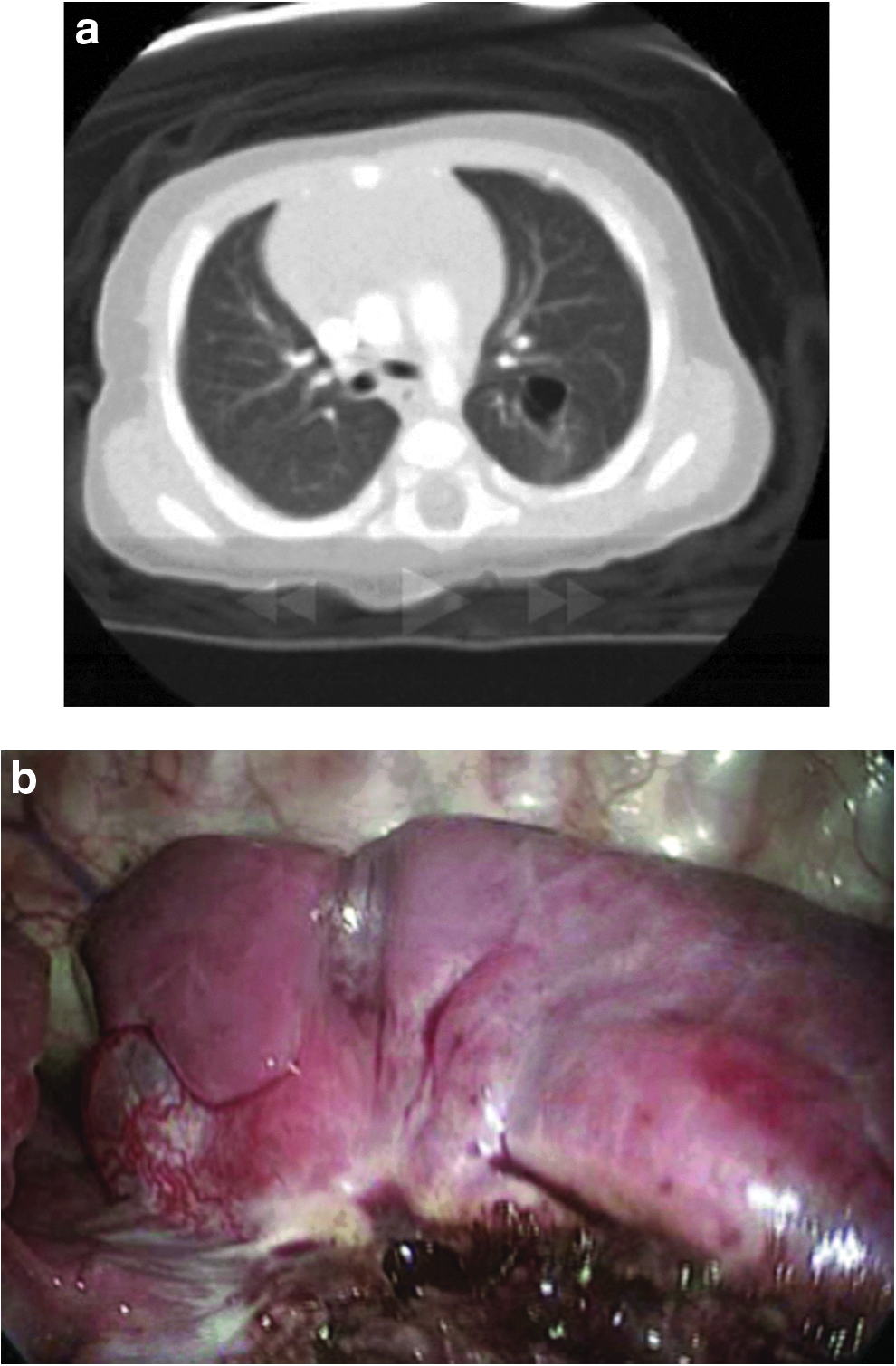
In our series preoperative imaging and findings at the time of surgery strongly suggested the diseased lung was isolated to a particular segment of the lung (Fig. 1). Based on this we felt a more limited resection might achieve the benefits of eliminating the long-term risk of infection and malignancy while preserving nonaffected parenchyma.

Congenital pulmonary airway malformation limited to apical segments of the
We have chosen to perform resections based on segmental anatomy whenever possible. We believe this minimizes the risk of leaving affected lung parenchyma and decreases the risk of short- and long-term complications. By identifying the segmental bronchus and vessels we eliminated any significant air leak or bleeding from the resection margins. Also, in smaller patients we were able to divide the lung parenchyma using a 5-mm tissue sealing device across the plane of ischemia, eliminating the need to try and fit a large 12-mm stapler into a confined space with limited visibility.
Because of this approach the chest tubes were removed in under 48 hours in all but 1 patient, and the mean hospital stay was 2 days. There were no significant operative or postoperative complications. The patient with the giant arteriovenous malformation (Fig. 2) had prolonged serosanguinous drainage, which resolved after 4 days, and was discharged on postoperative Day 5; this was also the case that took 5 hours to perform. One patient did not have a truly anatomic resection. On preoperative CT scan it was felt the infant had a CPAM primarily in the superior segment of the left lower lobe. However, at the time of surgery the patient was found to have no major fissure and appeared to have cystic disease in both the apical posterior segment of the upper and superior segment of the lower lobe. There were congenital clefts between the segments of what appeared to be cystic and normal lung, and these were used to help define the plane of dissection. However, pure anatomic planes were not identified and resected, and even though a complete resection of all grossly involved tissue was performed, there was evidence of recurrent cystic disease on a CT scan 4 years later. This patient underwent a re-resection and is still being followed up.

Thoracoscopic view of giant arteriovenous malformation of the right lower lobe.
Unfortunately, following up these patients is an imperfect science. We are currently obtaining a CT scan at 1 year postoperatively, and if there is no evidence of persistent or recurrent disease, then no further follow-up imaging is done.
It is clear that a segmental resection is not currently appropriate in the majority of cases of congenital cystic lung disease as the disease is too extensive. In our overall series we have chosen to perform lung-sparing surgery in less than 10% of cases. We believe our experience demonstrates that when the diseased lung, either congenital or acquired, is limited to an anatomic segment (Fig. 3), the technique of thoracoscopic segmentectomy is safe and effective. It results in lung conservation without significant risk, yet it is hoped eliminating the long-term risk of infection and malignancy. With improving imaging and technique it is possible that a larger percentage of patients presenting with CPAM and BPS will be candidates for segmentectomy.
Although there appears to be little long-term morbidity from performing a complete lobectomy in infants and children with CPAM or BPS, 32 especially if the procedure is done thoracoscopically, there are no detailed physiologic studies to validate this assumption, only gross observations. Although we still believe that lobectomy is preferable to leaving in diseased lung prone to infection and malignancy, we also favor preserving lung tissue if it is safe, effective, and eliminates these long-term risks.
In conclusion, we recommend the following algorithm for consideration of a segmental resection. First, the infant or child should be relatively asymptomatic at the time of surgery. Preoperative imaging should include a high-resolution CT scan. If the scan suggests that the disease is limited to a single anatomic segment, then a lung-sparing procedure should be considered and discussed with the parents. They should understand the possible benefits of preserving normal lung versus the need for later surveillance, including follow-up CT scan at 1 year, and the possibility of retained abnormal lung tissue. If they consent, then the final determination to proceed with segmentectomy depends on the findings at thoracoscopy and the feasibility and safety of performing a limited anatomic resection. The fallback position should always be lobectomy if there are any technical issues or concern for leaving behind diseased lung.
Footnotes
Disclosure Statement
No competing financial interests exist.