
Abstract
Abstract
Purpose:
We compared our experience with intra- and extracorporeal stenting in laparoscopic transabdominal pyeloplasty in children and adolescents. As the placement of transanastomotic stents during laparoscopy can be difficult, we developed a technique for laparoscopic transrenal stent placement.
Subjects and Methods:
Eighty-six consecutive patients who underwent laparoscopic transabdominal pyeloplasty in our institution from December 2003 to November 2012 were retrospectively analyzed. Initially we antegradely placed the double J catheter (n=48), whereas in later patients transrenal/transcutaneous stents were inserted (n=38), either via a cannula from the flank (n=33) or from the inside-out by transrenal puncture using a specially constructed spear (n=5). End points of the analysis were stent-related technical problems and complications and the need for reoperation.
Results:
Sixty-two boys and 24 girls with a mean age of 5.6 years (range, 78 days–17.3 years) and mean weight of 22.1 kg (range, 5.5–71 kg) underwent laparoscopic transabdominal pyeloplasty. The most common technical problem in the double J group was inability to place the double J catheter in 9 of the 48 patients. In combination with other complications such as dislocations, urinary tract infections, or catheter occlusions, this led to an overall complication rate of 35% in the group that underwent double J catheter insertion versus 13% in the group with transrenal stenting (P<.05). In the whole series, 4 patients required a redo pyeloplasty, all of them in the double J group.
Conclusions:
We recommend transrenal stents to facilitate stent removal without general anesthesia and to minimize complications such as stent dislocation. The initial experience with our simple device for transrenal puncture and stent placement is promising.
Introduction
L
Subjects and Methods
Patients
The local ethics committee at our institution approved this study (protocol number 1744-2013). In total, 86 consecutive children (62 boys and 24 girls) underwent laparoscopic transabdominal pyeloplasty in our institution from December 2003 to November 2012. Patient characteristics are summarized in Table 1. Twenty-nine patients were operated on from the right side, and 57 were operated on from the left side. The total mean age was 5.6 years (range, 78 days–17.3 years), and the total mean weight was 22.1 kg (range, 5.5–71 kg). In total, eight different pediatric surgeons performed the operation during this time period.
Techniques
Three different ways of anastomotic stenting were used. Initially, double J catheters were introduced via a trocar and placed antegradely during the laparoscopic procedure. Catheters were removed in a subsequent cystoscopy with the patient under general anesthesia (n=39) after a mean of 35.8 days (range, 20–73 days). Then, 38 patients underwent intraoperative implantation of transrenal stents either introduced via a cannula from the flank (n=33) or from the inside-out by transrenal puncture using a specially constructed spear (n=5) (Fig. 1). The transrenal stents were removed 1 week after the procedure, and the patients were hospitalized to assure drainage.
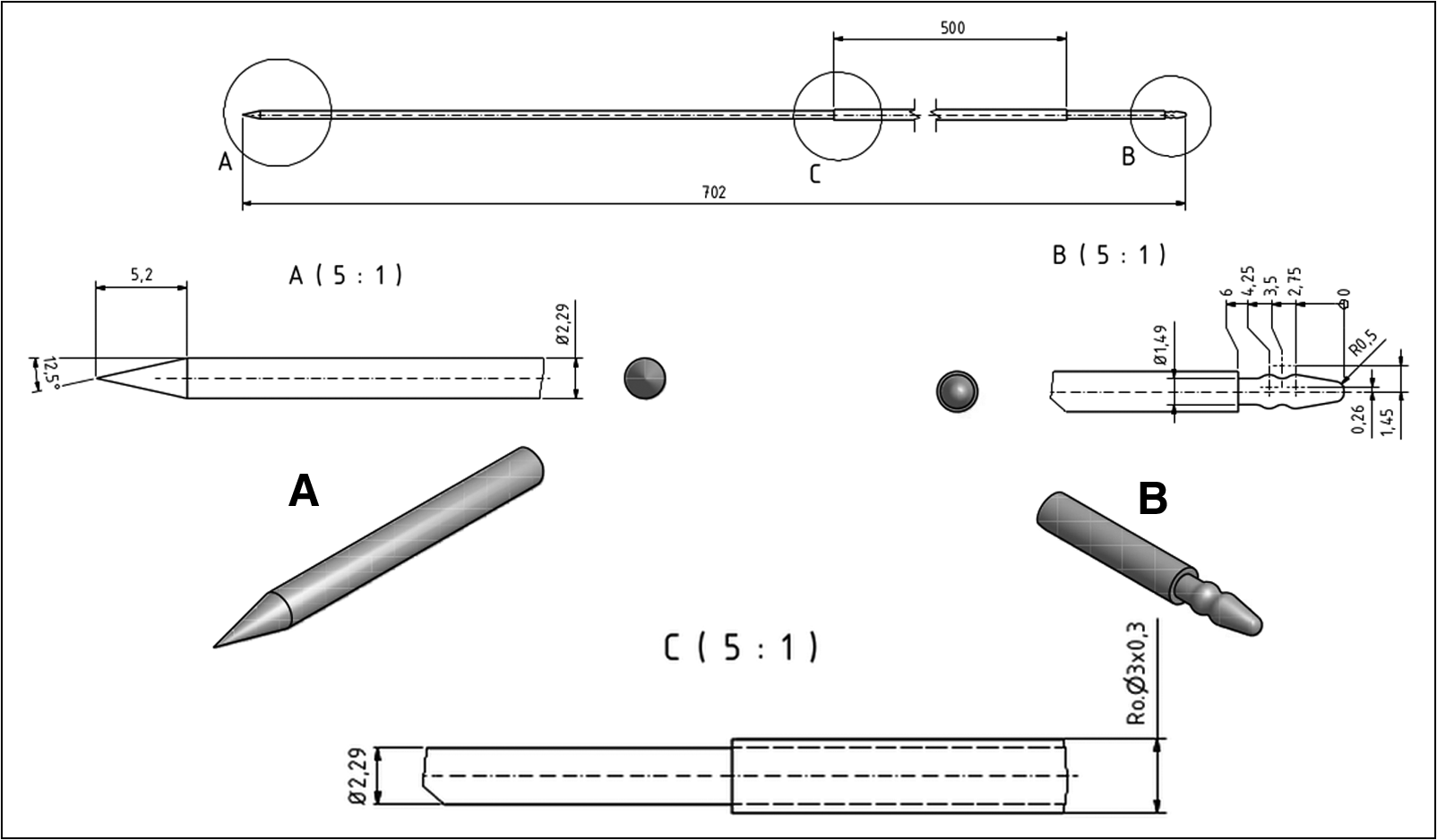
Schematic illustration of the newly constructed spear for transrenal externalized catheter insertion. Crucial details are
Follow-up
The urinary drainage of the affected side was monitored in follow-up 3 months after surgery by renal isotope scan and regular sonographic controls. The follow-up was completed in our institution in 76 (7 double J catheter and 3 transrenal) of the 86 patients. It ended systematically 1 year after the operation if neither hydronephrosis was present nor urinary tract infections had occurred.
Outcome parameters
End points of the analysis were stent-related technical problems and complications such as hydronephrosis, urinary leakage, stent dislocation, urinary tract infection (defined as a combination of pain, febrile temperatures, pyuria, and identification of pathogenic bacteria in the urine), or relevant bleeding (transfusion or sonographic signs of blood clot retention up to bladder tamponade). Other parameters were conversion to open surgery, revisional surgery including redo pyeloplasties, duration of hospital stay, and operating time.
Statistics
Statistical analysis was performed using SigmaStat® (Systat® Software, San Jose, CA). Intergroup comparison was performed by either the Mann–Whitney rank sum test or Fisher's exact test. A P value of <.05 was considered significant.
Results
Surgeons and operating time
Participating surgeons who operated on more than 10 pyeloplasties were considered experienced with this technique.
The rate of operations that were performed by experienced surgeons was 85% among the group with double J catheter insertion and 45% among the group with transrenal externalized stenting and therefore significantly different (P<.001). The mean operating time among experienced surgeons was 155.3 minutes (range, 87–265 minutes) versus 219.9 minutes (range, 150–330 minutes) for less experienced operators (P<.001). In total, the mean duration of the operation was significantly (P<.05) longer in the group of externalized stents (195.7 minutes [range, 113–330 minutes]) versus the double J group (161 minutes [range, 87–295 minutes]) (Table 2).
UPJO, ureteropelvic junction obstruction.
Hospital stay
The mean duration of hospital stay for patients in the transrenal group was 7.3 days (range, 2–16 days) and therefore significantly longer than in the group with double J insertion (mean, 4.0 days [range, 2–15 days]). Discharge was not based solely on the clinical course, but also on the fear or inability of the parents to handle the patient with an external drain.
Technical problems and complications
With double J catheter
In 9 patients who underwent laparoscopic placement of the double J, it was impossible to place the stent correctly, and these patients were left without a stent. Of these, 3 patients needed further surgery (i.e., nephrostomy, open revision, and a redo pyeloplasty). There were two stent dislocations and one stent occlusion, all requiring surgical intervention. Two patients developed an urinary tract infection with Pseudomonas, and 4 patients showed a recurrent ureteropelvic junction obstruction. One patient developed hydronephrosis, and there was one urinary leakage. Conversion to open surgery was necessary in 1 patient with prior liver transplantation and malrotation. The overall complication rate was 35%.
With transrenal stent
In patients with transrenal stent introduced by puncture with the cannula from the flank, generally a minor intraoperative bleeding occurred that stopped spontaneously without further complications. One patient developed a bladder tamponade that was managed conservatively. There was no bleeding or any other complication in patients in whom the transrenal stent was placed from inside-out. Two cases needed a conversion to open surgery because of difficulty in visualization during the anastomosis. There was one stent dislocation as well as 1 case of hydronephrosis. The overall complication rate was 13%.
Revisional surgery or redo pyeloplasties
In the complete series, 4 patients needed a redo pyeloplasty (5%), but there were other surgical interventions necessary.
With double J catheter
One patient developed a urinary leakage requiring open revision. Three patients required a temporary percutaneous nephrostomy. Two patients underwent laparoscopic ureterotomy for a dislocated catheter. In 4 cases a recurrent ureteropelvic junction obstruction made an open revision necessary. The overall reoperation rate was 17%.
With transrenal stent
One stent dislocation led to an open revision of the pyeloplasty. Another patient required a temporary percutaneous nephrostomy. The overall reoperation rate was 5%.
Discussion
The placement of a transanastomotic stent in laparoscopic pyeloplasty in children and infants can be challenging and the cause of complications.5,9 To solve this technical problem several different techniques of ureteral stenting have been described. One common technique involves placement of a double J catheter in an antegrade or retrograde fashion. Although in adults the antegrade placement has been reported to be uncomplicated, Chandrasekharam 5 described difficulties in the antegrade placement of double J catheters in infants, with a lower failure rate using the retrograde approach. 10 Failure was usually due to the inability to cross the ureterovesicular junction. However, besides the internal stenting via double J, external stenting is popular in children. In a large retrospective series, Braga et al. 11 compared an externalized pyeloureteral stent and internal double J catheters in 470 consecutive open pyeloplasties in children, concluding equivalence of overall complication and success rates, but lower costs and no second anesthesia in external stenting. Similar results were reported by Yiee and Baskin, 12 who performed a cost-effectiveness analysis regarding the usage of no stent, an external transanastomotic stent, or a double J catheter in open pyeloplasty and identified a cost advantage of external urinary derivation.
In our study the overall rate of technical problems and complications is 26%, which is comparable to the results reported by Turner et al. 13 Our detailed analysis demonstrated an overall higher rate of technical problems and complications of antegrade placement of double J catheter implantation versus the transrenal stenting. The most common technical problem was the inability to place the stent, resulting in 9 patients left without stents, with a high rate requiring revisional surgery (33%). There were also complications in patients with successful placement of the double J catheter requiring surgical interventions, such as stent migration or dislocation, which led to an overall increase in reoperations in the group with double J stenting versus transrenal stenting (17% versus 5%). The unacceptably high rate of stent-related complications was the reason to abandon the internal stent procedure in our institution.
Regarding external urinary drainage, the transrenal placement of the catheter poses other technical challenges. Several methods have been described. Hadley et al. 14 used a sharp deflux needle to puncture the renal tissue and then introducing the catheter with a guidewire in a Seldinger technique. With this method they placed 9 of 10 stents correctly. Two patients showed poor drainage with need to flush the catheters. One patient developed a recurrent ureteropelvic junction obstruction and required following intervention. One urinary tract infection occurred during catheter drainage. 14 Another option, the transcutaneous-transrenal puncture with an Angiocath™ (BD, Franklin Lakes, NJ) catheter and the antegrade placement of a guidewire with consecutive placement of the catheter, has been introduced by Noh et al. 15 for robotic pyeloplasty. We used a similar approach in the initial phase of our transrenal stenting by inserting the catheter through a cannula that was inserted transcutaneously and through the renal parenchyma into the renal pelvis. Although this method was straightforward, the sharp tip of the cannula and its slightly higher diameter compared with the stent caused regularly minor bleeding. Another drawback of this method was the need to puncture toward the pelvis and the renal hilus with its potential risk of damage to the renal artery or vein. Using our spear abrogated both of these disadvantages. It allows an easy positioning of the puncture site in the renal pelvis, and, as the spear has the same diameter as the catheter and a noncutting tip, there is no bleeding after the placement.
Despite the easier placement of the transrenal stent we observed a longer operation time in patients with transrenal percutaneous nephrostomy. However, this appears to be due to the experience of surgeons rather than the technique of transrenal stenting: the experience level in the double J group was significantly higher compared with the transrenal group, and the duration of operation was significantly lower in patients operated on by experienced surgeons. Nonetheless, the number of stent-related complications were significantly lower in the transrenal group, emphasizing the feasibility and safety of transrenal percutaneous nephrostomy. An increased level of experience among this group might have equalized the operation time differences. However, the clear advantage of the transrenal approach that we found was a markedly decreased complication rate despite the lower rate of expertise.
The longer hospital stay observed in the transrenal group was not due to postoperative immobilization, but rather due to the fact that we offered parents who felt insecure about the handling of the external urinary drainage to remain hospitalized until the stent was removed. Although the increased hospitalization will markedly increase the costs of the transrenal drainage, the ability to remove the catheter without the risk of another general anesthesia appears to be especially important in infants. 16
The limitation of our study is the retrospective design. Patients were operated on consecutively according to the prevailing technique starting with double J insertion and later with transrenal stenting. Therefore other factors, such as the inherent improvement of operation techniques and modifications, could contribute to the significantly improved outcome in the later series.
Conclusions
Based on our experience we recommend transrenal stenting in laparoscopic pyeloplasty in infants and children and encourage the use of our simple method of inside-out puncture.
Footnotes
Disclosure Statement
No competing financial interests exist.