
Abstract
Abstract
Background:
Feeding jejunostomy is an alternative enteral nutritional supplementation method for patients with functional gastrointestinal tracts. In this study, we introduced the novel, safe technique of single-incision laparoscopic-assisted jejunostomy (SIL-AJ) tube placement.
Subjects and Methods:
We conducted a prospective record search and a retrospective review of all patients who received surgical jejunostomy tube placement in Chang Gung Memorial Hospital, Linkou, Taiwan, from October 2011 to December 2012. SIL-AJ, multiple-incision laparoscopic jejunostomy (MIL-J), and open jejunostomy (O-J) were performed concurrently. We compared the demographic data, operative time, postoperative pain control, and postoperative complications among these groups.
Results:
Forty patients who received surgical jejunostomy in this period were enrolled in the study. There were 14 patients with SIL-AJ, 10 with MIL-J, and 16 with O-J. There were no differences in age, sex, American Society of Anesthesiologists status, body mass index, or malignancy distribution among the SIL-AJ, MIL-J, and O-J groups. The total operative times for the SIL-AJ, MIL-J, and O-J procedures were 53.3±11.5, 117.3±45.8, and 52.9±16.1 minutes, respectively; SIL-AJ and O-J had similar operative times, which were significantly shorter than the operative times in the MIL-J group (P<.001). The proportions of patients who began feeding within 24 hours in the SIL-AJ, MIL-J, and O-J groups were 100%, 70%, and 37%, respectively; the SIL-AJ group had a higher feeding rate at 24 hours than the two other groups (P=.001). The SIL-AJ and MIL-J groups had fewer postoperative complications than the O-J group (P=.011).
Conclusions:
SIL-AJ is a feasible and safe procedure that can be performed in patients who require alternative enteral feeding. Reduced postoperative pain, acceptable incisions, and quick feeding were observed in patients with SIL-AJ. Transumbilical SIL-AJ uses cost-effective appliances, and it is a relatively simple technique to learn and in which togain proficiency.
Introduction
E
Laparoscopic feeding jejunostomy was introduced by O'Regan and Scarrow 8 in 1990. Since then, several articles have been published in the literature to improve its clinical application and decrease its learning curve.9–11 Currently, multiple-incision laparoscopic jejunostomy (MIL-J) is a mainstay of surgical feeding jejunostomy implantation. Minimally invasive surgery has allowed the used of reduced ports and even enabled single-incision procedures to be performed. Single-incision laparoscopic techniques have been successfully performed in several intraabdominal operations.12–14 Reduction of the incision decreases peritoneal trauma and postoperative pain.5,15,16 Until now, few cases have been reported with regard to the use of single-incision laparoscopic surgery for jejunostomy tube implantation. 17
In this study, we present a novel technique for single-incision laparoscopic-assisted jejunostomy (SIL-AJ) tube placement, and we discuss the efficacy and safety of this minimally invasive technique.
Subjects and Methods
Data collection
We prospectively collected data and retrospectively reviewed all patients undergoing surgical feeding jejunostomy tube placement from October 2011 until December 2012 at Chang Gung Memorial Hospital in Linkou, Taiwan. The study was approved by the internal review board of Chang Gung Memorial Hospital. During this period, we performed SIL-AJ, MIL-J, and open jejunostomy (O-J) feeding tube placement concurrently. All of the patients were followed up at our hospital. Demographic data, the reason for jejunostomy placement, information regarding complications, previous abdominal surgical history, and medical, operative, and postoperative data were prospectively recorded in a computerized database. In addition, perioperative-associated operations, conversion to laparotomy, and operative time were recorded. The postoperative data included postoperative feeding time, opioid consumption (equivalent to morphine dosage), and complications. Complications were defined as wound infections, wound dehiscence, and peritoneal leakage of the jejunostomy. We excluded patients who underwent jejunostomy as an adjunct to specialized surgeries, such as esophageal and gastric resections, or after pancreaticoduodenectomy. Patients undergoing jejunostomy and other procedures concurrently were included, but the operative time was recorded as the operative time for only the jejunostomy.
Procedure
All tubes were implanted in the operating room by the same surgical team using the same procedure. Patients under general anesthesia were placed in the lithotomy position. All of the patients received 1 g of cefazolin sodium intravenously prior to surgery as prophylaxis. The jejunostomy tube exit site was located in the left upper quadrant, at least 2 cm lateral to the rectus muscle sheath and 2–3 cm superior to the level of the umbilicus, which was marked before the operation.
A 15-mm vertical umbilical incision was made, and the peritoneum was entered under direct visualization. We inserted one finger into the peritoneal cavity to prevent retraction of the viscera or omentum. An Alexis wound retractor (XS size; Applied Medical, Rancho Santa Margarita, CA) was inserted to make the incision as wide as possible, and then a homemade glove port was placed. Two 5-mm trocars and one 11-mm trocar for 10-mm rigid scopes were placed (Fig. 1). Under a pneumoperitoneum of 12 mm Hg, the operator evaluated the entire abdomen and applied enterolysis if any adhesion was encountered. Then, the greater omentum was lifted cephalically for adequate visualization of the intestinal loops.

Homemade glove port for single-incision laparoscopic surgery.
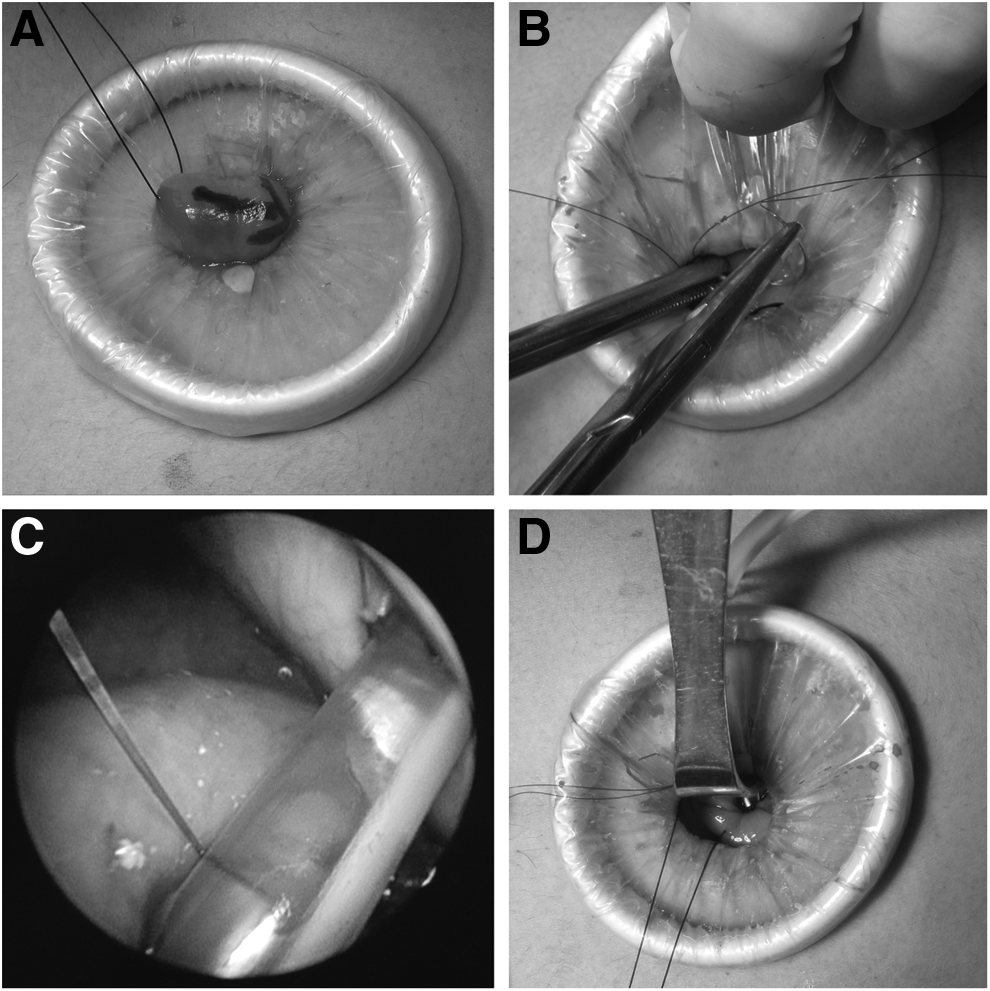
Once this step was accomplished, a two-handed technique was used to run the bowel proximally until the ligament of Treitz was identified. Then, a point 30 cm distal to the ligament of Treitz was identified and marked (Fig. 2A), which would later serve as the enterotomy site. Next, one needle puncture was made into the peritoneal cavity at the jejunostomy exit site, which was located at the internal peritoneal opening site of the jejunostomy. One 3-0 silk suture was placed on the parietal peritoneum and the jejunum serosal layer, which anchored the suture to the anterior abdominal wall. Two sutures were temporarily clamped without making a knot. The loop of the bowel was mobilized to the umbilicus, and the glove port was removed. We performed two purse-string sutures on the jejunum via this umbilical incision using conventional open instrumentation (Fig. 2B). We passed one Fr 14 nasogastric tube through the exit site and created an enterotomy using electrocautery. We manipulated the nasogastric tube into the intestinal lumen and tied off the purse-string sutures to create a seal around the catheter and to prevent any leakage. The loop of the bowel was gently returned to the abdomen with the feeding tube in place. The glove port was replaced, and the pneumoperitoneum was reestablished. The tip of the tube was checked to prevent kinking, misdirection, or other problems. Then, we positioned three diamond-shaped anchoring sutures to fix the intestinal loop to the abdominal wall intracorporeally or transumbilically (Fig. 2C). After all procedures, we removed the glove port again, and all of the anchor sutures were then tied tightly so that the entry site of the catheter into the jejunum was sealed from the rest of the abdominal cavity (Fig. 2D).
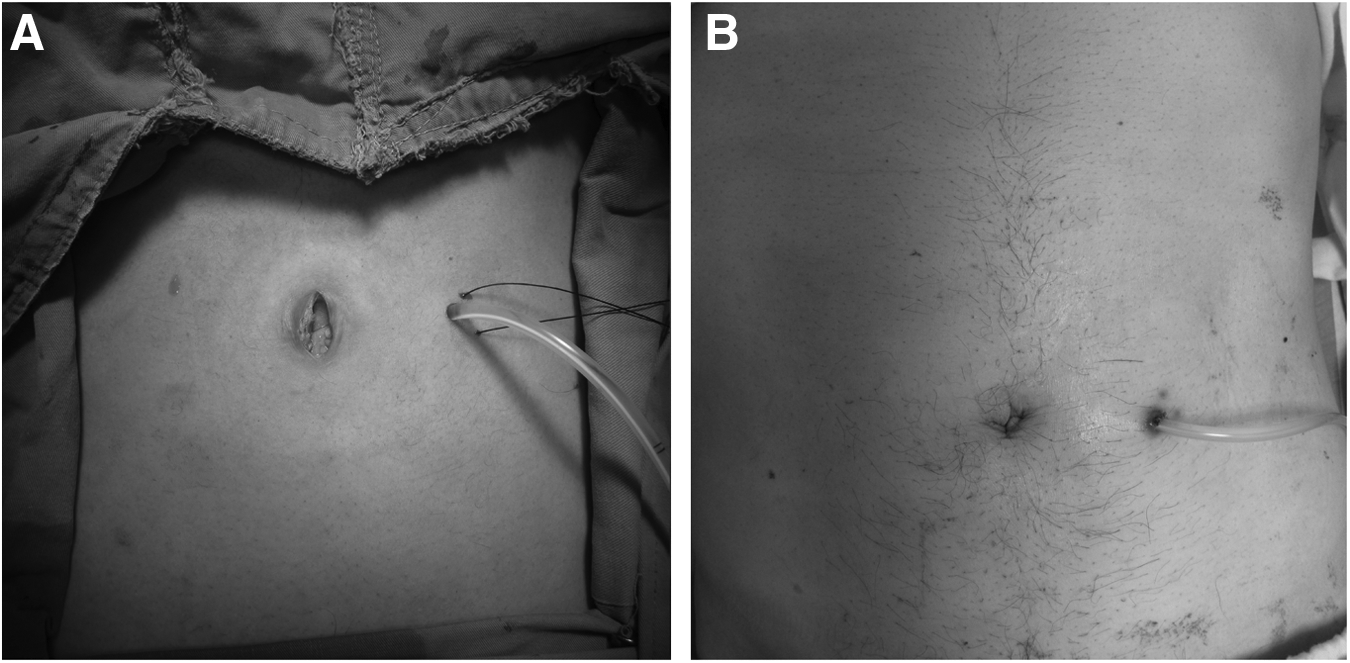
After these steps, we instilled 50 mL of saline into the tube. If the instillation time was >30 seconds, blockade or kinking was suspected, and the tube was modified as necessary. The tube was secured to the skin using a permanent stitch (Fig. 3). Finally, the fascial defect at the umbilicus was closed with two figure-eight 0 polyglactin 910 (Vicryl™; Ethicon, Somerville, NJ) sutures, and the skin was closed with 3-0 poliglecaprone 25 (Monocryl™; Ethicon) sutures.
For the MIL-J and O-J groups, we performed equivalent procedures, except for the lengths and numbers of incisions. For the MIL-J group, we inserted one 11-mm trocar in the right middle abdomen and another two 5-mm trocars in the right abdomen. For the O-J group, we created a minilaparotomy in the upper midline with a size of approximately 6 cm. We placed two purse-string sutures and four anchoring sutures, as described above, to ensure the security and consistency of our jejunostomy quality in the MIL-J, O-J, and SIL-AJ groups. All of our patients used a Fr 14 nasogastric tube as the jejunostomy tube.
Tube feeding was permitted if the tube could be flushed with water smoothly or if the bowels began moving after surgery. The patients were educated by a dietician and a nurse regarding feeding and tube care.
Statistical analysis
Pearson's chi-squared test was used as appropriate to compare categorical variables, which are presented as numbers or proportions. Quantitative variables are presented as mean±standard deviation values or as medians with interquartile ranges and compared by a one-way analysis of variance; post hoc testing was performed using the Least Significant Difference test. Statistical analysis was performed using SPSS version 20.0 software for Macintosh (SPSS Inc., Chicago, IL). P<.05 was defined as statistically significant.
Results
In total, 86 patients underwent jejunostomy during this period; 46 patients underwent jejunostomy as an adjunct to specialized surgery, whereas 40 patients underwent surgery only for a feeding jejunostomy. We enrolled these 40 patients into this study. Fourteen patients received SIL-AJ, 10 received MIL-J, and 16 patients received O-J in the current series.
Fourteen patients, including 2 females and 12 males with a median age of 61 years (range, 39–86 years), underwent SIL-AJ. Of these 14 patients, 7 had oropharyngeal malignancies, 5 had esophageal malignancies, and 2 presented with neurological deficits. The median operative time was 57.5 minutes (interquartile range, 45–61 minutes). There were no pulmonary or wound infections, postoperative intraabdominal abscess formations, or mortalities in this series. The median follow-up time was 6.5 months (interquartile range, 4–14 months). There were no failures of jejunostomy during this period, and no incisional hernias or adhesions were observed (Table 1).
ASA, American Society of Anesthesiologists; BMI, body mass index.
As Table 2 shows, there were no differences in age, sex, American Society of Anesthesiologists status, body mass index, or malignancy distribution among the SIL-AJ, MIL-J and O-J groups. There was no perioperative mortality in any of the patients. There were higher rates of previous abdominal surgical history in the O-J (23.5%) and SIL-AJ (21.3%) groups, followed by the MIL-J group (10.0%), but there was no statistically difference (P=.676). The total operative times in SIL-AJ, MIL-J, and O-J were 53.3±11.5, 117.3±45.8, and 52.9±16.1 minutes, respectively; SIL-AJ and O-J showed similar operative times, which were significantly shorter than the operative times in the MIL-J group (P<.001). There was one conversion to laparotomy in the MIL-J group, and there were no conversions in the SIL-AJ group. The proportions of patients who began feeding within 24 hours in the SIL-AJ, MIL-J, and O-J groups were 100%, 70%, and 37%, respectively; the SIL-AJ group showed a higher feeding rate at 24 hours than the two other groups (P=.001). The postoperative opioid requirements in the SIL-AJ, MIL-J, and O-J groups were 15.8±11.2, 35.0±27.7, and 49.4±20.2 mg within 72 hours after the operation, respectively; the requirement in the SIL-AJ group was significantly lower than that in the other two groups (P<.001). The SIL-AJ and MIL-J groups had fewer postoperative complications than the O-J group (P=.011).
ASA, American Society of Anesthesiologists; BMI, body mass index; MIL-J, multiple-incision laparoscopic jejunostomy; O-J, open jejunostomy; SD, standard deviation; SIL-AJ, single-incision laparoscopic-assisted jejunostomy.
Discussion
In recent years, single-incision laparoscopic surgery has emerged as a safe and effective minimally invasive approach for several abdominal procedures.18–20 Studies have shown that single-incision surgery is associated with reduced postoperative pain, acceptable incisions, shorter hospital stays, and quicker recovery.12,13,15 However, to our knowledge, few reports in the literature have addressed single-incision laparoscopic-assisted surgery to place feeding jejunostomy tubes, 17 which suggests that the safety and feasibility of SIL-AJ require evaluation. In this preliminary study, we have described 14 consecutive patients who underwent SIL-AJ with acceptable results.
Evidence for the safety of a new technique must be provided before its implementation in routine clinical practice. The present results indicate that SIL-AJ is a safe and feasible procedure. There were no intraoperative complications, such as bowel injury or uncontrollable bleeding, associated with the procedure, and none of the patients required additional surgery. There was no mortality among the patients included in the study. The median time for surgery was 52.5 minutes (interquartile range, 45–61 minutes). The median follow-up time was 6.5 months (interquartile range, 4–14 months). No wound infections, herniation, or intestinal obstructions were observed in the present series.
For patients who require an alternative enteral feeding route, the ability to commence feeding immediately is important. Less peritoneal trauma and bowel manipulation results in rapid recovery of bowel movement and smoother feeding. 21 With SIL-AJ, patients can begin jejunostomy feeding within 24 hours (many can begin immediately), and in the present study, none of the patients showed prolonged ileus after the operation. Compared with the O-J group, the SIL-AJ group had less peritoneal trauma and less irritation to the bowel, which resulted in better recovery of bowel movement. In addition, SIL-AJ resulted in a higher feeding rate within 24 hours than MIL-J and O-J, which may be related to the shorter operative time and reduced manipulation of the bowel.
In this study, the dosage of opioids for postoperative pain control was significantly reduced in the SIL-AJ group. In agreement with the findings of previous studies, a decreased number and size of the incision resulted in reduced postoperative pain and earlier patient ambulation.12,14,15 Because the advantages of laparoscopic-aided procedures include direct visualization and placement of the tube as well as avoidance of tube kinking in the bowel loop,9,22 there were no blockages in the SIL-AJ and MIL-J groups; however, 2 subjects in the O-J group showed failure of the jejunostomy arising from tube blockade. In the present study, SIL-AJ enabled the setting of the tube through a transumbilical incision, with limited extension of the wound. The use of a wound retractor prevented the development of infections, and none of the patients in our series had an infected wound. In the SIL-AJ group, a decreased wound infection rate was identified in this study, which is consistent with the decreased incidence of wound infection that has been previously associated with single-incision laparoscopic surgery. 23 Most patients who needed jejunostomy placement were malnourished and not active. All of the causes include risk factors for poor wound healing. Decreasing the size and number of the incisions was another consideration for decreased wound dehiscence. In the SIL-AJ and MIL-J groups, no patients had wound dehiscence, which was superior to the rate observed in the O-J group (dehiscence rate, 12.5%). 23 In addition, because postoperative adhesion makes further surgery difficult, the advantages of SIL-AJ are obvious. Several studies have reported that decreasing the size and number of incisions results in a lower incidence of adhesions.24,25 Compared with MIL-AJ and O-J, SIL-AJ is associated with fewer incisions and limited parietal trauma; therefore, the SIL-AJ procedure should theoretically decrease postoperative adhesion formation. However, the follow-up time was short, so we could not draw a definitive conclusion.
Another advantage of SIL-AJ is an improvement of the cosmetic results associated with the reduced number of trocars, as supported by experience.14,26 In most of our patients, the wound was not visible after surgery, and even in patients requiring extension of the incision, the final scar was acceptable.
One of the disadvantages of laparoscopic placement of feeding jejunostomy tubes is the difficulty of suturing in the limited space. Many techniques and innovative devices have been created for laparoscopic jejunal tube placement.9–11,27–29 However, such devices incur extra costs. For SIL-AJ, we used only conventional laparoscopic instruments with one wound retractor, which was cost-effective and as practically effective as other devices designed for jejunostomy placement.
Another limitation of laparoscopic surgery for jejunostomy feeding is related to the steep learning curve. 9 Complex suturing and peritoneal anchoring prevent the novice laparoscopic surgeon from performing this procedure regularly. SIL-AJ overcomes this disadvantage and can thus allow surgeons who are not familiar with laparoscopic surgery to effectively perform the procedure. The umbilicus provides a natural orifice to enter the peritoneal cavity with limited scarring. The use of a wound retractor enables the extension of a 1.5-cm umbilical incision to a 2–2.5-cm opening, which permits a surgeon inexperienced in intracorporeal suturing to perform purse-string sutures and anchor sutures transumbilically. In addition, the incision allows the surgeon's finger to pass through, allowing surgeons to tie peritoneal sutures with greater confidence. The operative time was decreased in the SIL-AJ group and was almost comparable with that in the O-J group, and it was much shorter than the operative time in the MIL-AJ group. A shorter the operative time allows surgeons to learn a procedure more easily. The combination of laparoscopic observation and direct inspection through the incision increases the safety and reproducibility of SIL-AJ. The ease of placement, ability to commence feeding immediately, and minimal morbidity have led us to favor SIL-AJ over MIL-AJ and O-J for tube placement.
The contraindications for SIL-AJ, which are similar to those for laparoscopic surgery, include hemodynamic instability, the inability to tolerate pneumoperitoneum, the presence of extensive intraabdominal soiling, and dense adhesions. Although our results confirmed the safety and feasibility of SIL-AJ, there were issues associated with the procedure that must be addressed. Suboptimal viewing angles, crowded instruments, and loss of triangulation may be encountered in SIL-AJ. A prolonged operative time was noted in the first few patients. Increased experience will certainly result in shorter operative times than those observed in our series. In most single-incision laparoscopic surgery cases, the operative technique itself is not very different from a laparoscopic approach, and there is minimal change in the equipment, with negligible differences in costs. The learning curves are reportedly favorable for surgeons who are already experienced in laparoscopic surgery.30,31 Finally, this was a retrospective nonrandomized study; therefore, selection bias cannot be completely excluded because of the study's design.
In conclusion, SIL-AJ is a feasible and safe procedure that can be performed in patients who require alternative enteral feeding. Reduced postoperative pain, acceptable incisions, and rapid feeding were seen in patients with SIL-AJ. Transumbilical SIL-AJ uses cost-effective instruments, and the procedure is a relatively simple technique to learn and in which to gain proficiency.
Footnotes
Disclosure Statement
No competing financial interests exist.