
Abstract
Abstract
Background:
This study retrospectively reviewed 48 cases of gastric submucosal tumors (SMTs) treated by endolumenal endoscopic full-thickness resection (EFR) microsurgery in our gastrointestinal endoscopy center.
Patients and Methods:
From November 2009 to October 2012, 48 cases underwent endolumenal EFR for resection of muscularis propria–originating gastric SMTs. Characteristics of the 48 patients, clinical efficacy, safety of EFR, and post-EFR pathological diagnoses were evaluated retrospectively.
Results:
EFR was successfully performed in 48 cases with 52 lesions. The median operation time was 59.72 minutes (range, 30–270 minutes; standard deviation, 39.72 minutes). The mean tumor size was 1.59 cm (range, 0.50–4.80 cm; standard deviation, 1.01 cm). During the EFR process, dual-channel gastroscopy was applied in 20 cases of SMTs, and paracentesis during the EFR process was applied in 9 cases. EFR for larger SMTs and gastric corpus–originating SMTs had longer operative times. Pathological diagnosis included 43 gastrointestinal stromal tumors, 4 leiomyomas, and 1 schwannoma. A larger tumor size was associated with higher risk of malignancy. No severe postoperative complications were observed. No tumor recurrences were confirmed in follow-up gastroscopy.
Conclusions:
The endolumenal EFR technique proved to be feasible and minimally invasive, even for the resection of large gastric tumors originating from the muscularis propria. However, more data on EFR must be obtained and analyzed.
Introduction
T
From November 2009 to October 2012, 48 cases of gastric SMTs were endoscopically treated by endolumenal EFR in our endoscopy center. This article retrospectively reviews our experience and outcomes of endoscopic resection of gastric SMTs originating from the muscularis propria or close to the serosa.
Patients and Methods
From November 2009 to October 2012, 42,345 patients with abdominal pain, abdominal distention, and dyspepsia symptoms received a gastroscope examination at our outpatient department. When gastric SMTs were diagnosed, endoscopic ultrasonography (model UM-2000; Olympus, Tokyo, Japan) examination was introduced. After endoscopic ultrasonography examination, patients with lesions larger than 2 cm received an epigast computed tomography scan. Patients with gastric SMTs originating from the muscularis propria or close to the serosa were included for endolumenal EFR therapy. Exclusion criteria were as follows: (1) gastric SMTs larger than 5 cm; (2) patients with coagulopathy (international normalized ratio >1.5), platelet count <50,000/mL, and anticoagulation therapy; and (3) patients not suitable for general anesthesia with tracheal intubation.
Forty-eight patients with gastric SMTs received endolumenal EFR in our single tertiary-care center. The clinical characteristics of the 48 patients are shown in detail in Table 1. To evaluate healing of the incision and residual or recurrence of lesions after the endolumenal EFR operation, patients were recommended to receive gastroscope examinations 2 months after EFR. Then follow-up gastroscopy was performed at 6 months, 12 months, and 24 months. The present study was approved by the Internal Review Board of our hospital.
EFR, endoscopic full-thickness resection; GIST, gastrointestinal stromal tumor.
Equipment and endolumenal EFR procedure
A single-channel gastric endoscope (model GIF-Q260J; Olympus) or a dual-channel therapeutic gastroscope (model GIF-2T-240; Olympus), a high-frequency generator (ICC200; ERBE Elektromedizin GmbH, Tübingen, Germany), and an argon plasma coagulator (model APC300; ERBE) were applied for endolumenal EFR operations. Other accessory equipment included injection needles (model NM-200L-0423), transparent caps (model D201-11804), snares (model SD-5L-1), hot biopsy forceps (model FD-410LR), IT knife (model KD-610-L), hook knife (model KD-620LR), and titanium clips (HX-610-090 or HX-610-090-L) (all from Olympus).
Patients were adequately informed about the planned procedure and were kept nothing perorally for 6 hours before the endolumenal EFR microsurgery. The entire EFR procedure was carried out in the operating room. After receiving general anesthesia and tracheal intubation, patients were placed in a lateral recumbent position. The EFR procedure was performed under continuous pulse oximetry, electrocardiogram assessment, and intermittent blood pressure monitoring.
With a transparent cap attached to its tip, a single-channel gastroscope was introduced into the stomach. After dots were marked around the lesion, submucosal injection of a normal saline solution with 1% indigo carmine and epinephrine was performed. Incision of superficial layers overlying the SMT was performed with a hook knife and an IT knife. Mucosal and submucosal layers of the gastric wall were removed by a snare. Then a circumferential dissection around the border of the SMT was performed with a hook knife and an IT knife. To observe the lesion more clearly, the abovementioned solution was injected along the low border of the SMT as necessary. When the muscularis propria layer was reached and the root of the tumor was revealed, gastric fluid was extracted as much as possible. Active perforation was performed with a hook knife, and a further full-thickness incision was made with an IT knife. When the tumor was isolated, it was en bloc removed with a snare.
For treatment of tumors with a broad basement, a dual-channel gastroscope was applied, providing two snares passing through the accessory channels into the gastric cavity. With one snare grasping the tumor body, the tumor along with the attached serosal layer was en bloc enucleated with another snare and retrieved from the mouth. The defect of the gastric wall was closed by several titanium clips. If signs of pneumoperitoneum were found during the procedure, paracentesis using a 20-gauge needle was performed. The entire procedure of endolumenal EFR is shown in Figure 1.
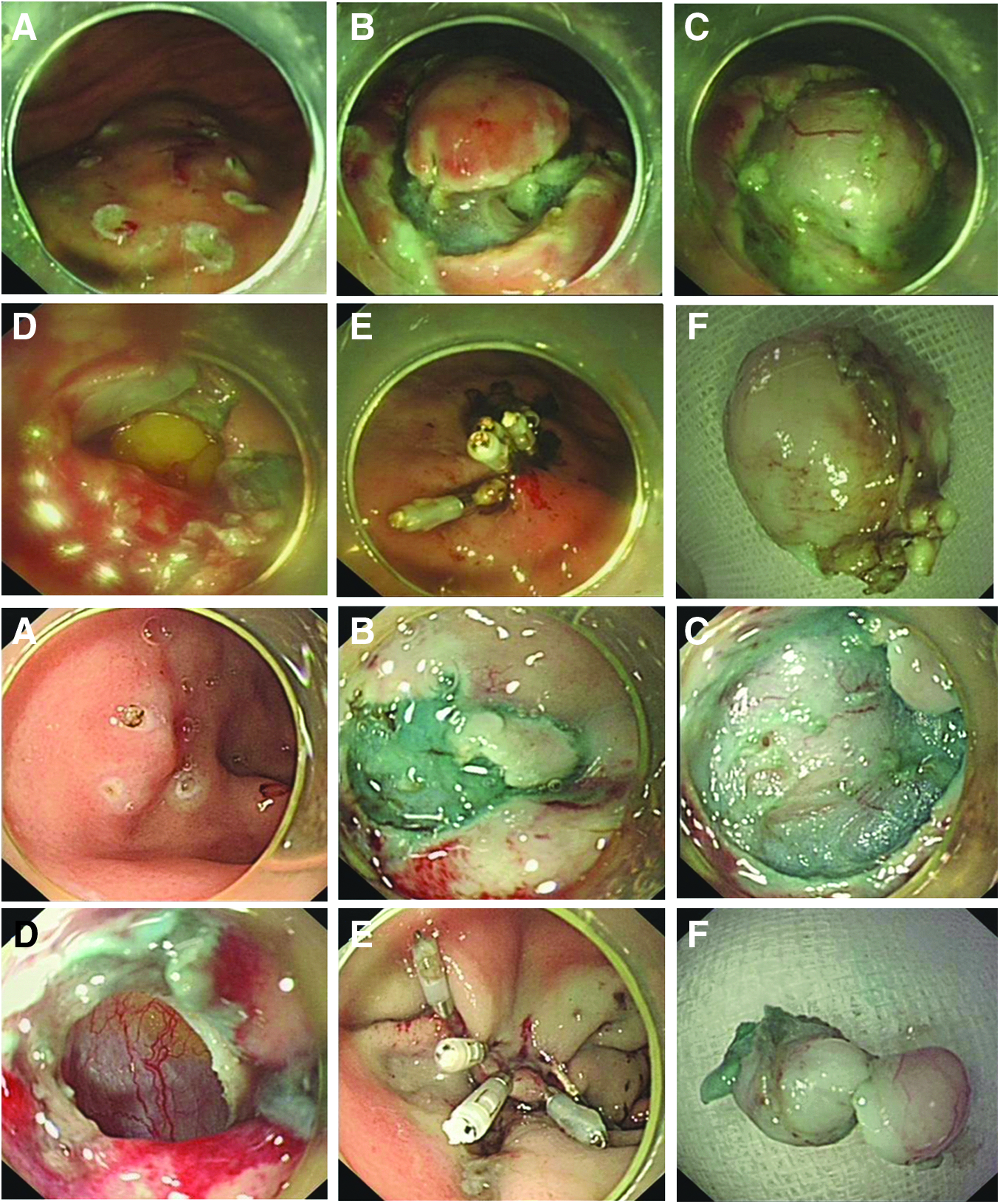
Procedures of endoscopic full-thickness resection for 2 cases of muscularis propria originating from gastric fundus submucosal tumors.
After the EFR surgery, a gastrointestinal decompression drainage tube was placed. Postoperative medication included nothing perorally, gastrointestinal decompression drainage for 24 hours, and drug therapy, such as a proton pump inhibitor and broad-spectrum antibiotic intravenous administration, for 3 days. Patients were discharged with proton pump inhibitor therapy for 2 months. A video of EFR performed with a gastroscope and a dual-channel gastroscope is supplied as a supplement.
Post-EFR pathological diagnosis was made by focusing on cell types. If spindle cells were present, immunohistochemical tests for CD34, CD117, Dog1, SMA, S-100, and Ki-67 were performed to differentiate a gastrointestinal stromal tumor (GIST) from a leiomyoma. Mitotic counts per 50 high-power fields were evaluated in GISTs.
Statistical analysis
All data were expressed as mean±standard deviation (SD) values. A Student's t test, chi-squared test, and analysis of variance (one-way) were applied using SPSS version 16.0 software (SPSS Inc., Chicago, IL). A P value of <.05 was considered to be statistically significant.
Results
Patient characteristics and outcomes of EFR are summarized in Table 1. Forty-eight patients (25 males and 23 females), with a mean age of 56.85 years (range, 27–75 years; SD, 11.23 years), were included in the study. Forty-four patients had a single tumor, and 2 patients had two lesions. In total, 52 SMTs were found. Among all enrolled patients, 40 tumors were located in the gastric fundus with 4 cases of two SMTs, 7 were in the gastric corpus, and 1 was in the gastric antrum. All lesions were confirmed as originating from the muscularis propria or close to the serosa by endoscopic ultrasonography examination or computed tomography scan.
The EFR success rate was 100%. The median operation time was 59.72 minutes (range, 30–270 minutes; SD, 39.72 minutes). In 1 case of SMT with a tumor of about 4.8 cm with a 70% nonintracavity tumor body, the entire EFR process took 270 minutes. The mean tumor size was 1.59 cm (range, 0.50–4.80 cm; SD, 1.01 cm). During the EFR process, the dual-channel gastroscope was used in 20 cases of SMTs, and paracentesis during the EFR process was applied in 9 cases. Pathological diagnosis showed 43 GISTs, 4 leiomyomas, and 1 schwannoma. Among the 43 GISTs, 29 cases were benign, 8 cases were very low risk of malignancy, and 6 were at low risk of malignancy. All specimens were border-free.
Effects of tumor sizes and locations affecting the entire EFR process were then assessed by subgroup analysis (Tables 2 and 3). The operation time was associated with tumor sizes and locations. EFR for SMTs larger than 2 cm and for gastric corpus–located SMTs took longer times. Titanium clip numbers for gastric wall defects were higher in gastric corpus–located SMTs. Usage of a dual-channel gastroscope and paracentesis were not altered. Histologic diagnosis of GISTs differed with different tumor sizes.
GIST, gastrointestinal stromal tumor.
No post-EFR complication, such as bleeding and peritonitis, was observed. Five cases had moderate postoperative distention because of air filtration. Three cases were relieved by paracentesis, and the other 2 were resolved in 2 days. Hospital stay ranged from 4 to 7 days after EFR.
Follow-up gastroscopy examination was performed in all 48 patients. Gastroscopy after 2 months, 6 months, 12 months, and 24 months was performed in 48 patients, 40 patients, 24 patients, and 14 patients, respectively. No sign of tumor recurrence was found.
Discussion
Patients with gastric SMTs may have nonspecific symptoms. In our case series, all enrolled 48 patients were diagnosed by gastroscope and further endoscopic ultrasonography examinations as outpatients. Large gastric SMTs are routinely recommended for resection for potential risk of canceration. For treatment of gastric SMTs, laparoscopic and endoscopic cooperative surgery has been accepted as invasive surgery because of laparoscopic minimally sized wedge resection and liner stapler suturing.4,8,9 Sometimes in laparoscopic surgery, assistance of a gastroscope is essential to identify the resection area. On the other hand, some techniques in endoscopic submucosal dissection, such as tissue grasping, incision, and gastric wall defect closure by use of metal clips, make it possible for large gastric SMTs to be en bloc-incised by gastroscope full-thickness resection.10,11 Compared with laparoscopic and endoscopic cooperative surgery, EFR may be more feasible and advantageous, owing to less invasiveness through natural orifice lumina.
Perforation was once recognized as a complication in endoscopic resection. However, endoscopic closure techniques of gastrointestinal tract perforation12,13 do not make gastric perforation an obstacle to endoscopic resection of SMTs. With active perforation and endoscopic gastric wall defect seal techniques, EFR is now available. In the present study, we retrospectively reviewed those cases of gastric SMTs originating from the muscularis propria or close to the serosa layer treated by EFR therapy in our center. Our outcomes of EFR for gastric SMTs are encouraging, because of active perforation being performed and SMTs being successfully resected, as well as observing no severe post-EFR complications in all 48 patients.
In EFR for gastric SMTs, tumor size and location of the lesion must be evaluated before surgery, 14 considering the relationship with operation difficulty, operation time, and postoperative complications. In the present study, the EFR procedure for large or gastric corpus–located SMTs may be more time-consuming. According to our experience, a too small or too big SMT is not suitable for EFR. As for smaller SMTs (<0.5 cm in diameter), it is hard to find the tumor after submucosal injection or even after removing the overlying submucosal layers. On the other hand, some problems emerge during resection of large gastric SMTs. Incision of large lesions are associated with the potential high risk of suturing difficulty, long operative times, and complications during and after surgery. Most important is that a very large tumor body cannot be easily retrieved from the cardia. Preoperative computed tomography is very important, especially in patients with large lesions. If a lesion were confirmed to be a nonintracavity tumor, EFR would be difficult. In one patient with a partly nonintracavity SMT of 4.8 cm, EFR was successfully carried out in 270 minutes; however, the tumor body was retrieved in a piecemeal manner. Outcomes of our study demonstrated that GISTs are most common in gastric SMTs, which is similar to previous studies.15,16 Considering the pathological diagnosis of GISTs, 17 we argue that intracavity gastric muscularis propria–originating SMTs from 1 cm to 3 cm are most suitable for EFR therapy. Then location of an SMT should be considered. Consistent with the reports of Wang et al. 14 and Liu et al., 18 gastric muscularis propria-originating SMTs were mostly found at the gastric fundus. For gastric fundus–located SMTs, EFR procedures can be smoothly performed with an overturned gastroscope, even in the gastic fundus dome. In our series, gastric SMTs located near the gastric cardia, at the esophagus–gastric junction as well as at the upper less curve of the gastric corpus, were difficult to resection endoscopically. 14 This was because of little space being left for the surgeons to use the apparatus freely and to perform the endoclip gastric wall defect closure. On the other hand, EFRs for other located SMTs, such as at the lower less curve or greater curve of the gastric corpus and gastric antrum, are easier for a skilled endoscopist.
Compared with traditional endoscopic submucosal dissection, there are some key steps in the EFR operation, which are as follows. First, to provide a satisfactory visual field for operators, removing the overlying superficial mucosal and submucosal layers enclosing the tumor is essential. Good exposure of a tumor body following removal of the overlying tissues will make the next steps convenient. 11 Second, the stomach contents may flow into the abdominal cavity through the gastric wall defect created by active perforation and may cause peritonitis. To avoid post-EFR localized peritonitis, 11 it is crucial to extract intracavitary gastric fluid and control bleeding. No sign of severe infection or peritonitis was observed in all the enrolled patients. Third, possible tissue grasping techniques should be applied. During the tumor body incision process, the entire SMT should be prevented from falling into the abdominal cavity.5,19 Sometimes, for endoscopic treatment of large SMTs with a wide basement or partly nonintracavity SMTs, a dual-channel endoscope should always be applied. When an SMT was bulk-isolated, a dual-channel gastroscope and two snares were introduced to achieve tissue-grasping and tumor body incision. With one snare to lift tumor tissue into the gastric cavity by the grasping tumor body, another is applied to incise the SMTs with some serosa. Compared with a forceps grasping technique,11,19 it is more feasible to incise an SMT integrated with some serosa tissue and the least possible tumor cell sublation. Fourth, a gastric wall defect must be immediately closed when the SMT is removed. Metal clip sutures are efficacious for gastric wall defect closure.7,11,14 The gastric wall defect may be reduced by continuous suction and can be easily sealed by endoclip sutures. We used enlongated clips for closure of the gastric wall defect in all patients. Once the first two clips were properly placed, the gastric wall defect became smaller, and the subsequent procedure became easier. In our series, reliable endoclip sutures seem to be achieved at the gastric fundus rather than the gastric autrum, which may be because of the thinner full-thickness of the gastric wall. For closure of a larger gastric wall defect and gastric antrum wound, we chose sealing by suturing the full mucosa to some omenta tissues. 20 Fifth, operators must deal with the pneumoperitoneum in the EFR procedure. Because air filtration is the main cause of tension pneumoperitoneum following EFR, 21 carbon dioxide is recommended rather than air during the EFR procedure. When an SMT is isolated from the serosa, less air, continuous effective suction, and prompt gastric wall defect sutures are recommended. If severe abdominal distension emerges, prophylactic paracentesis must be carried out. We performed paracentesis at the outer margin of the right rectus abdominis in the midabdomen.
Our present work shows encouraging effects for EFR on muscularis propria–originating gastric SMTs. Compared with previous endoscopic enucleation for muscularis propria-originating gastric SMTs, 16 EFR seems to be better for postsurgery pathologic diagnosis because SMTs are completely resected with some serosa tissues. Some limitations also exist in this work. Our data are outcomes of a single center, and a large-scale multicenter evaluation on this issue is needed. Because of the biological characteristics of GISTs, the follow-up period was relatively shorter in our study. Long-term follow-up is essential to assess complete removal and recurrence of GISTs. Theoretically, EFR may be applied for esophageal SMTs, 1 although it also may cause severe complications such as pneumatothorax, mediastinal emphysema, and mediastinal infection. Therefore, indications of EFR for gastrointestinal SMTs may be further studied by involving more prospective multicenter data.
In conclusion, EFR for gastric muscularis propria–originating SMTs is an effective and safe technique. EFR may replace open surgery and may be feasible than laparoscopic and endoscopic cooperative surgery for deep originating gastric SMTs.
Footnotes
Disclosure Statement
No competing financial interests exist.