
Abstract
Abstract
Introduction:
Spigelian hernia (SH) is rare and is traditionally repaired using an open technique. There has been an increasing popularity of laparoscopic methods, with transabdominal preperitoneal (TAPP) repair being one of the popular techniques. Currently, most surgeons using the TAPP technique close the fascial defect prior to mesh placement. Here we report our experience with a TAPP repair that deliberately excludes approximation of the fascial defect.
Subjects and Methods:
Prospective data were collected on consecutive patients undergoing elective SH repair under the care of a single surgeon between 2001 and 2012. Diagnosis was confirmed preoperatively using ultrasonography or computerized tomography. A laparoscopic TAPP repair was used without closing the defect. Following discharge all patients were followed up at 3 and 12 months. The clinical records were reviewed at the time this article was written. The technique, epidemiological characteristics, operative findings, hospital stay, morbidity, and follow-up are presented.
Results:
Twenty-six patients (16 males) with a median age of 63 years were operated on. The follow-up period ranged between 6 months and 11 years (median, 4 years). Hernia defect size ranged from 2 to 10 cm. Mean operating time for unilateral defects was 45 minutes; that for bilateral defects was 70 minutes. Twenty-two patients were discharged on the same day. There were no postoperative complications or recurrences.
Conclusions:
Laparoscopic TAPP repair of SH without closing the defect is safe, effective, and durable. There is no additional benefit from routine closure of the fascial defect. On the contrary, there may be potential advantages in leaving the defect unopposed.
Introduction
T
There have been various different reported presentations of an SH, varying from a palpable lump, abdominal pain, incarceration, strangulation, and as an incidental finding.8–13 Investigative methods for suspected SH include ultrasonography (US), computerized tomography (CT), or diagnostic laparoscopy. A recent retrospective study by Light et al. 14 confirmed a 100% positive predictive value with either US or CT.
SHs have traditionally been repaired by an open technique. Since Carter and Mizes 15 first described their laparoscopic technique in 1992, laparoscopic repair has become increasingly popular. Of the laparoscopic SH repairs reported in the literature, the most popular repair is the intraperitoneal onlay mesh method, followed by transabdominal preperitoneal (TAPP) repair.12,13,16–34
The majority of surgeons reporting use of the TAPP repair close the defect despite there being no evidence in the literature supporting this.16,19,31,34–36 Here we report the outcome of the largest series of patients undergoing laparoscopic TAPP repair of SH that deliberately omits approximation of the fascial defect.
Subjects and Methods
The details of consecutive patients who underwent TAPP repair of SH under the care of a single surgeon (A.S.A.) between 2001 and 2012 were reviewed. Data were collected prospectively, including patient demographics, comorbidities, side of hernia, operative findings, operative time, and complications including clinically apparent recurrence, seroma, hematoma, paresthesia, and pain.
Patients were followed up at 3 and 12 months and examined for evidence of recurrence and clinically apparent seromas or hematoma as well as being asked about pain and paresthesia. Patients were also asked as to whether they experienced any immediate postoperative complications in the preceding 3 months. Clinical notes were also reviewed in December 2012.
Surgical technique
After induction of general anesthesia and administration of prophylactic antibiotics, the patient is placed in a supine position with both arms adducted. Pneumoperitoneum is obtained using either Hassan's open technique or a Veress needle. A 12-mm port is inserted in the epigastric region at least 15 cm from the hernial defect. Diagnostic laparoscopy is then performed. Two further 5-mm ports are inserted: for unilateral defects, they are placed on the contralateral side of the defect; for bilateral defects, bilateral pararectal 5-mm ports are positioned.
Adhesions between the sac and its contents are released using sharp dissection. A peritoneal flap is then created with at least a 4-cm circumferential margin around the defect (Figs. 1 and 2). Care is taken to avoid injury to the inferior epigastric vessels. The defect is not opposed, and a standard polypropylene-based mesh is placed directly over the defect, ensuring a circumferential mesh–fascia overlap of at least 3 cm. Fixation of the mesh to the abdominal wall is achieved with two rows of tacks (Protack™, Autosuture; Covidien, Mansfield, MA) placing them 1–2 cm apart (Fig. 3). The peritoneal flap is then overlapped and fixed with tacks, ensuring complete mesh coverage (Fig. 4). Finally, the redundant sac is everted and fixed with tacks.

Left-sided Spigelian hernia after reduction of the sac contents.
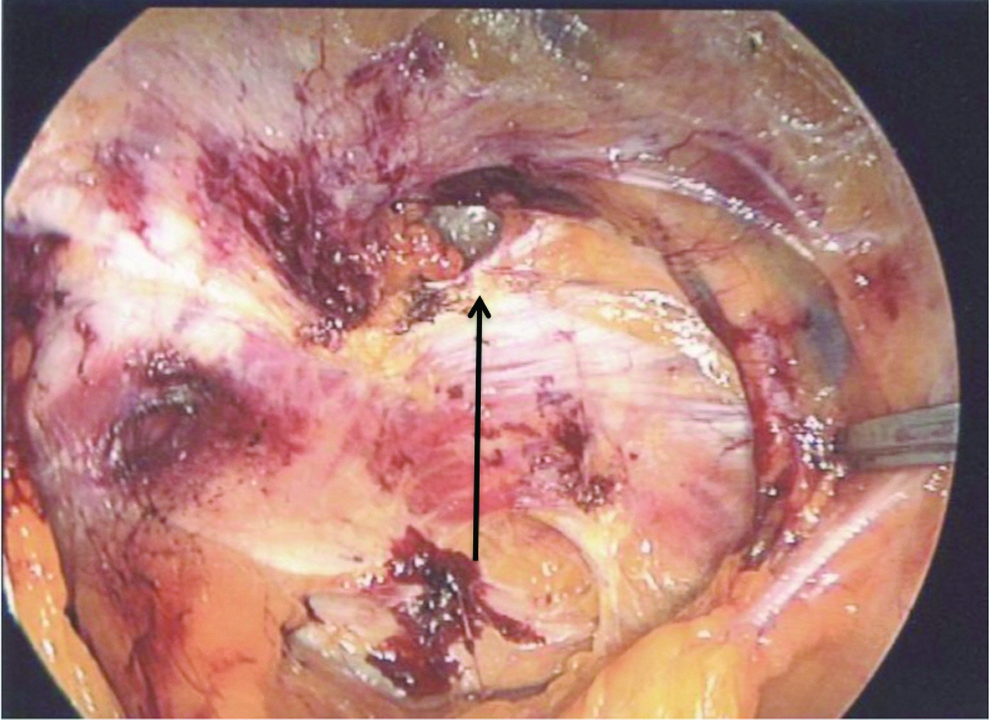
Complete dissection of the hernia sac sparing the epigastric vessels (arrow points to the defect).

A sub-underlay mesh repair with a minimum circumferential mesh–fascia overlap of 3 cm. The mesh was fixed to the posterior abdominal wall using tacks, again avoiding the inferior epigastric vessels (arrow).

The edges of the peritoneal flap are overlapped, ensuring complete mesh coverage, and the hernial sac is everted and fixed with tacks.
Patients were assessed postoperatively and discharged if they were clinically well, comfortable, tolerating diet, and mobilizing safely.
All the SHs encountered in this series were located in the “SH belt”—a transverse 6-cm-wide zone above the interspinous plane. The authors are aware that SHs below this zone have been reported but are extremely rare. 37 Such hernias should be differentiated from direct inguinal or supravesical hernias. Had we encountered a “lower” SH, we would still adopt the same technique described above, but we would recommend taking extra care when creating the peritoneal flap inferiorly to ensure that dissection and mesh fixation do not result in a nerve injury.
Results
In total, 26 consecutive patients undergoing repair of SH using the above-described technique were included in this study. Table 1 shows the patients' demographics and comorbidities. Six patients who had had previous abdominal surgery had no evidence of incisional hernia. All cases were scheduled as elective day-case procedures except for the patient with previous deep vein thrombosis and pulmonary embolus.
BMI, body mass index; DVT, deep vein thrombosis; F, female; M, male; PE, pulmonary embolus.
Diagnosis was confirmed preoperatively with either US or CT in 25 patients. The remaining patient was diagnosed incidentally during laparoscopic inguinal hernia repair. Table 2 shows the presenting features of these 26 patients and the side(s) of the defect(s).
Table 3 summarizes the intraoperative findings. Operative time ranged between 35 and 70 minutes (median, 45 minutes) and 70 and 95 minutes (median, 80 minutes) for unilateral and bilateral defect repair, respectively. In all cases, sac contents were reduced easily, and there were no intraoperative complications. No patients required conversion to open surgery.
Twenty-two patients were discharged on the same day of surgery, whereas 3 patients required overnight stay owing to an evening starting time of their procedure. The patient who had a history of deep vein thrombosis and pulmonary embolus stayed for 3 days to ensure adequate anticoagulation. There were no re-admissions related to SH repair.
At 3 months all patients attended their clinic review. Patients were asked if they had experienced any postoperative problems in the preceding period of time (including wound infection, paresthesia, or chronic pain) as well as being examined for any clinical evidence of seroma, hematoma, or recurrence. No patients in our series had reported having any problems in the 3-month postoperative period. The clinical examination was unremarkable in all patients.
At the 12-month review none of our patients had reported any problems relating to his or her SH repair. Furthermore, no patients had evidence of recurrence on clinical examination. No patient had sought medical advice regarding his or her SH repair from another clinician since the surgery.
Clinical records for all patients were reviewed in December 2012, equating to a follow-up period ranging between 6 months and 11 years (median, 4 years). Table 4 shows the follow-up periods for all patients. There was no documented evidence of any postoperative related attendances.
Discussion
SHs represent approximately 1% of all abdominal wall hernias.21,31,38 The absence of typical hernia symptoms, lack of persistent physical findings, and the partial nature of the defect can make early diagnosis difficult. Hence SH often remains unrecognized and is underreported.39,40 Given the high rate of incarceration and strangulation, a diagnosis of SH often necessitates repair.2,9,10,12
SHs were traditionally repaired using an open suture repair with or without mesh.12,13,41 The results of such repairs are widely reported with low recurrence rates.1,40,42–45 However, technically an open repair is more invasive. Moreover, identifying the actual defect may prove to be challenging, especially in obese patients and those who have had previous abdominal surgery. 46
Since Carter and Mizes 15 reported the first laparoscopic repair of SH in 1992, increasing numbers of patients have undergone laparoscopic repair owing to the well-documented advantages of minimally invasive surgery. There are several reported methods of laparoscopic repair. Laparoscopic primary suture repair has only been recommended for small defects in order to ensure a tension-free repair.5,47,48 There have been sporadic case reports using hybrid or laparoscopic-assisted techniques, which involve a diagnostic laparoscopy to confirm the diagnosis, localize the defect, and reduce the contents, followed by a formal open repair. Again, this method has only been recommended for SH with small defects.49,50
The most commonly reported (39%) laparoscopic method of SH repair is the intraperitoneal onlay mesh technique.12,13,16–34 This procedure involves reduction of the hernial contents and placement of a composite mesh directly on the abdominal wall. Although the technique is relatively simple, its major drawbacks are the possibility of interactions between peritoneal contents and the mesh potentially causing significant complications.51,52 In addition, when considering costs, composite mesh is more expensive than the standard mesh routinely used for TAPP or total extraperitoneal (TEP) repair.
TEP repair of SH has been reported, albeit in smaller numbers.21,53,54 Although this technique avoids entry into the peritoneal cavity, it is technically more demanding, requires a longer operating time, and does not enable the surgeon to address the possibility of bilateral defects. There is also the possibility of missing smaller SHs with this approach. 49 As with TEP repair for inguinal hernia, a proportion of patients undergoing intentional TEP repair will inevitably undergo TAPP repair.
TAPP repair is increasingly reported as one of the methods of choice for SH repairs. Table 5 summarizes the reported cases/series using the TAPP technique. This clearly demonstrates that there is a variation in practice when it comes to closing the defect. Prior to this study, the two largest series of patients undergoing TAPP repair for SH reported by Palanivelu et al. 34 and Patle et al. 31 had the primary defect closed. Both research groups reported no postoperative complications, with the longest follow-up being 3.4 years. 34 We performed a laparoscopic TAPP repair without closing the fascial defect, regardless of the defect size, in 26 consecutive patients with SH. We deliberately omitted the approximation of the hernia defect in all of our cases based on our belief that because of the anatomic nature of SH the abdominal wall is stable and provides reasonable support after the incorporation of a mesh.
In this study we reported the largest series of laparoscopically repaired SHs with probably the longest follow-up time. The technique we used, which deliberately omits closure of the fascial defect, has proven to be safe, feasible, and durable. We did not encounter any postoperative complications. In particular, there were no wound infections, clinically apparent seromas, hematomas, paresthesia, or chronic pain. To date, we are not aware of any recurrence. The majority of our patients were managed as day-cases.
In conclusion, TAPP repair without closure of the fascial defect for SH is safe, feasible, and durable. In addition, the potential benefits of omitting closure of the defect include reduced operating time and the possibility of less postoperative pain. It can be performed as a day-case procedure in the majority of cases.
Footnotes
Acknowledgments
The authors thank Mr. Barry Taylor, Mr. Phil Wake, Mr. Mark Tighe, Mr. John Lund, Mr. Graham Copeland, Mr. Degi Olujugba, Mr. Noman Sarfraz, and Mr. Ansar Farooq, who all are consultant surgeons at Warrington & Halton Hospitals NHS Foundation Trust, for referring their patients to us to undergo laparoscopic repair. We would also like to thank Dr. Karthik Gopal, Dr. John Whalley, and Dr. Rachel Magennis, consultant radiologists, for their support.
Disclosure Statement
No competing financial interests exist.