
Abstract
Abstract
Background:
Weight loss by means of an intragastric balloon is an advantageous procedure, as usage of such a balloon is minimally invasive and of minimal operational risk. Nevertheless, despite the encouraging results referred in to large population studies, its success rate as a treatment option is still questionable. The aim of this study was to classify and analyze all parameters recorded in a database of a treatment protocol concerning obese individuals handled by an intragastric balloon, in an attempt to delineate the comparable profile of those who succeeded to lose weight and those who failed.
Subjects and Methods:
Retrospective data collection, including demographic and anthropometric data, social and psychological factors, educational status, and attendance at sessions and the exercise program, was conducted. Using as a criterion for grouping the percentage of excess weight loss (%EWL), the successful (%EWL ≥50%) and the poor (%EWL ≤20%) responders were identified.
Results:
In total, 583 patients were assessed. Initial and ideal body weight (BW), initial body mass index (BMI), and excess weight were significantly lower in the %EWL ≥50% group (P<.001). Upon balloon removal, both groups exhibited a significant difference regarding BW, BW lost, BMI, and %EWL (P<.001). Advanced age (odds ratio [OR]=1.06; P<.001), female gender (OR=3.31; P<.001), basic educational level (OR=3.12; P<.001), and single or divorced marital status (OR=6.00; P<.001) were identified as the most powerful determinants of %EWL ≥50%. Moreover, attendance at more than four monthly interviews and strict exercise program commitment contributed significantly to a favorable outcome.
Conclusions:
Our findings could serve as an initial step for further research into factors possibly contributing to the early identification of those individuals who will notably benefit from usage of an intragastric balloon regarding BW loss.
Introduction
A
The most recognized technique of this category, with a 15-year history of efficient use, is that of the Bioenterics intragastric balloon (BIB®; Allergan®, Marlow International, Marlow, UK). Published data from two meta-analyses2,3 and from the Italian Collaborative Study Group for Lap-Band and BIB 4 underline the safety and effectiveness of the method, reporting an approximate mean body mass index (BMI) reduction of 5.5 kg/m2, a range of weight loss from 15 to 18 kg, and a percentage of excess weight loss (% EWL) ranging between 32% and 34%. In accordance with the previous results, a recent study from our institution showed even more improved outcomes, with a mean BMI reduction of 7.4 kg/m2 and a %EWL of 38.1%. 5 However, an in-depth analysis of the characteristics of our cohort revealed that 17% of the total subjects enrolled had an unsatisfactory weight loss (meaning less than the widely accepted cutoff of 20% in %EWL). 3 In cases in which the accepted cutoff limit of %EWL is more than 25%, the reported incidence of insufficient weight loss reaches even higher levels (up to 40%). 3 Another striking finding derived from the analysis of the rate of weight loss during the 6-month treatment period is that 65% of individuals lost 80% of the total weight loss during the first 3 months, and these individuals were found to have much better results in the maintenance of the weight lost over the 5-year follow-up. 5
Nevertheless, weight loss success depends both on the technical characteristics of the balloon occupying most of the stomach volume and on patient motivation and ability to make enduring changes in behaviors, such as eating behavior and physical activity. Moreover, individual personality characteristics are assumed to relate directly to individual factors, such as personal goals and self-efficacy beliefs, and to affect and be affected by environmental factors, such as social support and reinforcement.6,7 For these reasons, weight change for a particular individual cannot be predicted with accuracy; however, the early identification of those least likely to succeed in losing weight by a given treatment regimen could prove valuable to the treating physician.
We therefore attempted to classify and analyze all parameters recorded in a database of a treatment protocol concerning obese individuals handled by an intragastric balloon, in an attempt to delineate the comparable profile of those who succeeded to lose weight and those who failed.
Subjects and Methods
This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving human subjects/patients were approved by the Scientific Council of AHEPA University Hospital. After written informed consent was obtained from all participants, the prospectively collected data of all obese patients subjected to and having completed the 6-month intragastric balloon treatment, over the past 9-year period, were retrospectively reviewed. Criteria for inclusion in the treatment protocol were individuals as follows: with a BMI of <35 kg/m2, associated with obesity-related comorbidities; with a BMI of >35 kg/m2, resistant to weight loss with regimens of diet, physical activity, and behavior therapy for at least 6 months; or with a BMI of >50 kg/m2, mostly as a preparation for bariatric surgery to reduce operation-related morbidity and mortality. 5 In brief, all participants in our study had either consulted for weight reduction but declined surgery of any kind or, although obese, failed to meet the International Federation for the Surgery of Obesity & Metabolic Disorders standards for surgery. All procedures were performed by the same two fully trained endoscopists, whereas data collection and patient consultations were undertaken by one endoscopist and two experienced dietitians.
According to the treatment protocol, all participants underwent a preliminary interview to ascertain demographic data, marital status, education level, medical history, previous attempts to lose weight, comorbidities, and the social and psychological impact of obesity on their lives. Additionally, they were asked for a brief statement of their motivation to lose weight, for instance, to alleviate physical symptoms, such as sleep apnea, diabetes, hypertension, or joint problems, to become more attractive (marriageable), and to increase their likelihood of becoming pregnant. Upon balloon (BIB) insertion, the patients were prescribed a 3-day liquid diet, after which they were initially put on a semiliquid diet, replaced gradually by a normal balanced diet of 800–1000 kcal for the remainder of the 6 months. Finally, all were scheduled for monthly interviews, during which the new dietary regimen was reviewed, and efforts were made to re-educate in relation to eating habits and exercise, with each individual being given as much responsibility for selecting preferred behaviors as possible. Body weight (BW) loss and bioelectric impedance measurements were also taken, and advice was given regarding dieting and an exercise program. Exercise prescription was directed at progressively increasing physical activity during leisure time to reach a minimum energy expenditure of about 200 kcal/day at the end of the treatment period.
For the purpose of the present study, these prospectively collected data were initially assessed with respect to %EWL at the time of balloon removal and classified accordingly. A lower limit cutoff of ≤20% and a upper limit cutoff of ≥50% were then used, to discriminate between a poor and a successful response; the cutoff points were decided to be approximately equal to ±1 standard deviation (SD) of the mean value of %EWL, as used by others.8,9
Thus two groups were identified: poor responders (PR) and successful responders (SR). The remaining population was not used for further analysis.
Statistical analysis
All obesity-related data were expressed in terms of mean±SD values for numeric variables and as counts and percentages for categorical variables. Normality of data was assessed by the Kolmogorov–Smirnov test. Bivariate analysis was undertaken using Student's t test for comparison of means of continuous variables and normally distributed data, whereas a nonparametric rank test, the Mann–Whitney test, was used to compare means in the case of non-normally and non-continuously distributed data. Subgroup comparisons of categorical variables were assessed by a chi-squared (with Yates's correction when applicable) or Fisher's exact test when the expected value of a cell was less than 5. In order to quantify cross-sectional relationships among categorical variables of interest, the chi-squared test was applied. Odds ratios (ORs) with 95% confidence intervals (CIs) were computed using a multivariate stepwise logistic regression model with hospital %EWL as the response variable and age, gender, marital status, education level, and motivation to lose weight as independent variables. For all statistical procedures, a P value of <.05 was considered significant. The Statistical Package for Social Sciences (SPSS version 19.0 software; SPSS Inc., Chicago, IL) was used for all calculations.
Results
In total, 583 obese individuals were recorded to have completed the 6-month period of BIB treatment, over the past 9 years. The mean age of this cohort was 39.5 (SD, 11.2) years with a male-to-female ratio of 1:2.7 (157 males to 426 females). Upon referral to the clinic for weight loss, subjects had a mean BMI of 43.9 (SD, 8.4) kg/m2, a BW of 126.6 (SD, 27.9) kg, and a weight excess of 61.8 (SD, 25.3) kg. At the time of intragastric balloon removal their mean BMI was 36.3 (SD, 8.1) kg/m2, and their BW was 104.8 (SD, 26.6) kg, which corresponds to a BMI reduction of 7.6 (SD, 3.4) kg/m2 and a weight loss of 21.8 (SD, 9.9) kg, with a mean %EWL of 38.9% (SD, 20.1).
From the initial study population of 583 individuals, 162 and 105 subjects were allocated to the SR and PR groups, respectively. Table 1 presents the demographic data and those related to BMI and BW before and after treatment with the intragastric balloon.
Data are mean±standard deviation values or number of patients (%) as indicated.
%EWL, percentage of excess weight loss; BMI, body mass index; PR, poor responders; SR, successful responders.
With respect to age, the SR group was found to be statistically significantly older than the PR group (P<.001). Although there was no statistical difference in age between men and women (mean of 38.4 [SD, 13.8] and 42.3 [SD, 9.9] years, respectively; P=.087) within the SR group, a trend toward the males being younger was identified. However, of those who failed to lose weight (PR group), the females were younger compared with the males (mean of 33.8 [SD, 9.9] and 38.2 [SD, 10.9] years, respectively; P=.038). Female gender predominated in both groups, with the difference being more pronounced in the SR group compared with the PR group (82.8% versus 58.5%; P<.001).
Subjects belonging to the SR group were found to be statistically significantly taller in relation to those in the PR group (1.71 [SD, 0.09] and 1.68 [SD, 0.08] cm, respectively; P=.001), but no further difference was observed between males and females within the same group.
Regarding initial BW, initial BMI, and initial excess weight, these parameters were significantly lower in the SR group in relation to the PR group (P<.001), whether the groups were considered as a total population or analyzed as females and males. As expected, at the time of balloon removal the two groups also exhibited a highly statistically significant difference regarding BW, weight lost, BMI, and, of course, %EWL (P<.001).
When marital status was investigated, 84 (51.8%) subjects in the SR group were single, 60 (37%) were married, and 18 (11.1%) were divorced/separated. Correspondingly, in the PR group, 25 (23.8%) were single, and 80 (76.2%) were married; no divorced/separated patient was recorded in this group. No sex differences within both groups were identified. These findings demonstrate a significant difference in favor of the single/divorced patient losing weight (chi-squared=42.56, P<.001). It is of interest to mention that there were four couples in the PR group.
When participants were questioned about their education level, a significant difference between the two groups occurred. In the SR group, 92 (56.8%) individuals had a basic education, and 70 (43.2%) had a higher education level (university), whereas in the PR group, 32 (30.5%) participants had a basic education, and 73 (69.5%) had a higher educational level (chi-squared=17.73, P<.001). It is notable that subjects with a university and postdoctoral educational level spent much of their monthly interview asking questions, but the reduction in BW was insignificant.
An appreciable number of individuals in both groups (80.2% [n=130] in the SR group and 81.9% [n=86] in the PR group) had a long history of previous attempts to lose weight by various kinds of diet. The remaining patients came at their physician's specific recommendation in order to treat comorbidities. No individual in either group had a history of previous balloon insertion.
The most common comorbidities recorded were knee osteoarthritis, followed by sleep apnea. There were 22 cases (13.6%) of joint disease in the SR group and 24 (22.8%) in the PR group. Similarly, 37 cases (22.9%) of sleep apnea were recorded in the SR group and 20 (19.1%) in the PR group (chi-squared=3.92, P=.141).
Within the cohorts taken together, the most common motive to lose weight was to improve body image (55.1%; n=147), either for self-esteem or in order to become more attractive (marriageable); this was followed by the need/prompted necessity to alleviate comorbidities (32.6%; n=87) and, less commonly, to increase the probability of becoming pregnant (12.3%; n=33). The allocation of motivations into the two subgroups of patients was statistically significant (chi-squared=75.79, P<.001) and is shown in Figure 1. The most successful motivation in the SR group was the necessity to alleviate comorbidities, followed by the need to improve body image and, third, to become pregnant. In the PR group, however, the most successful motivation was the desire to improve body image/self-esteem, followed by the wish to become pregnant and then the necessity to alleviate comorbidities.
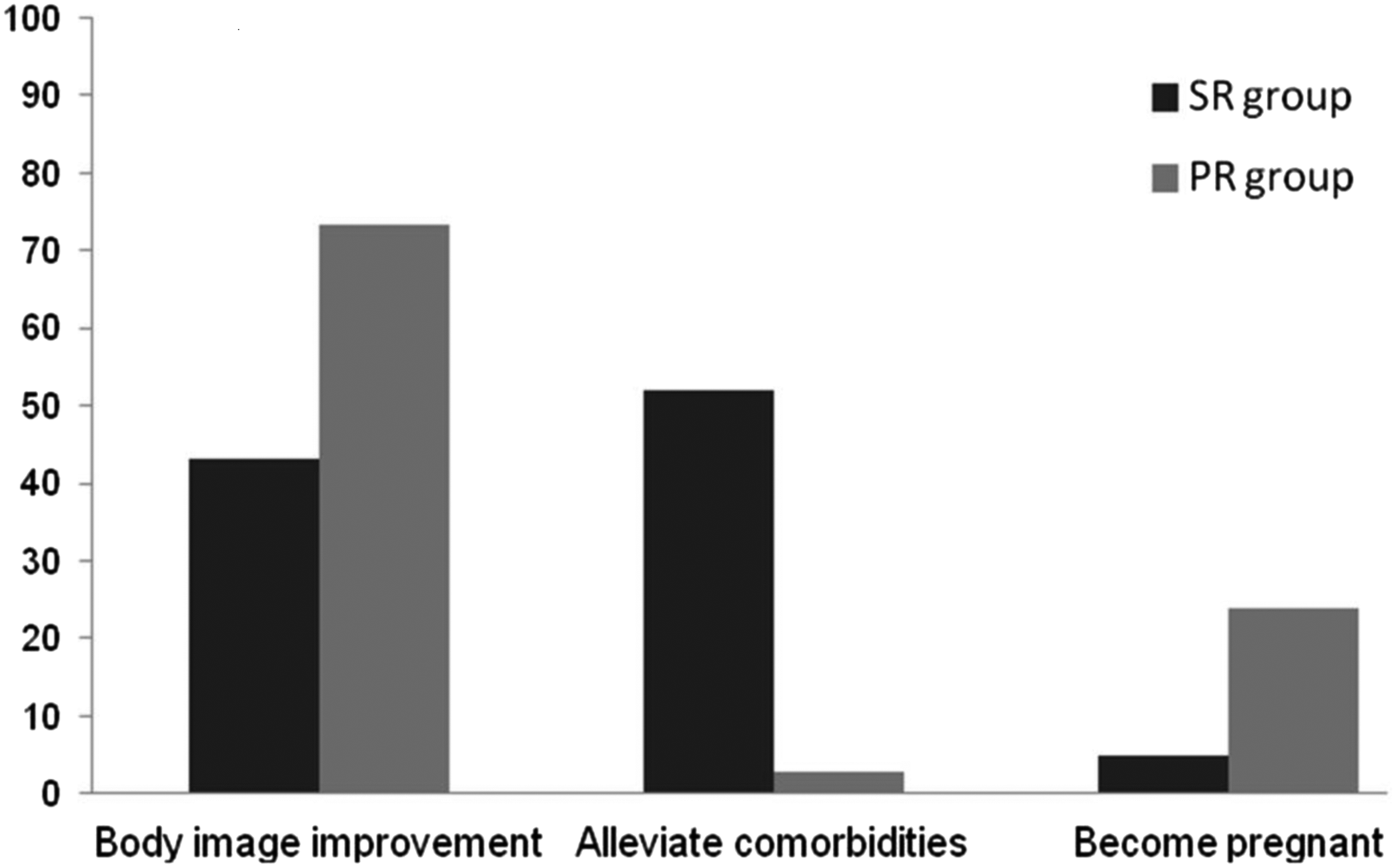
Distribution of all recruited patients by motivation type stratified by the percentage of excess weight loss. Data are expressed as percentages. PR, poor responders; SR, successful responders.
Once per month, all participants were invited for personal interviews. These interviews included BW and bioelectric impedance measurement, dietary regimen revision, and re-education concerning eating habits, aiming to reduce total caloric intake, portion sizes, and the frequency of snacks, sweets, and dietary fat. Analysis of attendance at six programmed interviews revealed that in the SR group, 85.2% (n=138) of the subjects attended all six interviews, 8% (n=13) attended five, and the remaining 6.8% (n=11) attended four. Regarding the PR group, 16.2% (n=17) attended these interviews four times, 43.8% (n=46) three times, 33.3% (n=35) twice, and 6.7% (n=7) only once. Taking four interviews as the cutoff limit of adequate attendance, 93.2% (n=151) cases in the SR group attended more than four interviews, whereas all patients in the PR group attended four or fewer interviews (P=.001).
Patients were urged to walk or do static cycling daily for at least 2 km, to use stairs instead of elevators, and to take a gym program beginning from the third month. The vast majority of subjects in the SR group (85.8%; n=139) complied fully, whereas the remaining 14.2% (n=23) responded positively to only the walking or cycling suggestion. However, only 16.2% (n=17) of the individuals of the PR group who also adhered to the monthly interview program adopted the suggestion of walking/cycling, but gave no further details regarding the distance.
Variables that exhibited levels of statistical significance in the univariate analysis such as age, gender, marital status, education level, and motivation to lose weight were entered into a stepwise logistic regression model, highlighting relatively advanced age (OR=1.066; 95% CI, 1.036–1.097; P<.001), female gender (OR=3.316; 95% CI, 1.703–6.457; P<.001), basic educational level (OR=3.125; 95% CI, 1.697–5.756; P<.001), and single or divorced marital status (OR=6.003; 95% CI, 3.266–11.034; P<.001), as the most powerful determinants of %EWL >50%.
Discussion
Obesity is a well-recognized serious chronic condition, causing or exacerbating numerous diseases, which, in combination, reduce quality of life and life expectancy, all leading to spiraling health costs.
Insertion of an intragastric balloon for weight loss—for strictly medical reasons—is the most common endoscopic intervention for obesity. It is regarded as an effective, minimally invasive, and easy-to-perform nonsurgical procedure, which is advantageous in full reversibility and low rate of reported complications.1,3,5 However, there is pessimism about how successful the treatment can be because intragastric balloon patients lack the changed digestive tract anatomy that promotes weight loss in bariatric surgery. They have, instead, a continuous sensation of satiety leading to the ingestion of smaller portions of meals, but they may require the entire, multidisciplinary help offered to individuals who undergo dietary and lifestyle modification for weight loss without surgery. This would be one possible explanation of the various extreme results in weight loss referred to in the literature.1,3–5,10–12
In an attempt to identify the possible factors contributing to weight loss, several studies have focused on different aspects relating to various bariatric procedures, including demographics, anthropometrics, psychology, socioeconomics, and even race, in an effort to reliably predict individual success or failure.2,8,9,13–17 To the best of our knowledge there is no such study relating to intragastric balloon treatment, so it seemed of interest to attempt to identify predictors of better weight loss or to use our extensive database to profile individuals and demystify weight loss.
This study examined the %EWL associated with BIB placement in a cohort of obese individuals who had completed the 6-month treatment period. A mean %EWL of 38.9% (SD, 20.1%) was observed, so we decided a priori to use a successful response definition of ≥50% and a poor response of ≤20%, with the cutoff points being approximately equal to±1 SD of the mean value of %EWL. Moreover, the lower cutoff point was that used for exclusion of those who failed to lose weight in our previous study, 5 whereas the upper cutoff was similar to that used in assessment of results after bariatric surgery. 9
There is no consistency in the reported data regarding the role of gender in the final outcome following bariatric procedures.8,15,18–22 Our findings regarding gender are in accordance with previous studies showing male gender to be one failure predictor for bariatric surgery.23–26
When the age was assessed, the patients in the SR group were found to be older than those in the PR group. In the former, the females tended to be older than the males, whereas in the PR group the females were younger. It is interesting that Ortega et al. 15 and Snyder et al. 9 in similar bariatric population settings found a younger age, of either gender, to be associated with higher excess weight loss and lower risk of unsuccessful surgery. However, when patients are classified in terms of specific procedures, age does not tend to predict success.
Furthermore, subjects of the SR group were found to be significantly taller in relation to those in the PR group, with no difference between males and females within the same group. This finding is reliable, if one accepts that taller patients have a greater lean body mass. 9
In accordance with previous studies,8,9 initial BW, BMI, and excess weight were significantly lower in the SR group in relation to the PR group, whether the comparison was made between groups or between males and females within the same group. This finding is not surprising because much more time is required for the more obese to lose >50% %EWL and because more weight needs to be lost to have a significant metabolic response in terms of the resolution of their comorbidities.8,27 Furthermore, other independent variables such as the patient's self-esteem, body image, and activity level, as well as satisfaction with a lower weight loss, may be implicated.13,22,26,28 Additionally, a lower BW can also reflect better self-control. In the same manner, greater weight loss at the beginning of the treatment appears to lead to a better final result, relating directly to good compliance and good self-discipline.14,28
Marital status was also a significant predictor of successful outcome. The surrounding environment and the life events facing the person trying to lose weight can facilitate as well as hamper the outcome. Stress in life events, family relations, or social activities are not the ideal context for weight loss. 29 The majority of our patients in the SR group (62.9%) were single or divorced. This finding could be explained by the internal need of singles, and even more of divorced people, to improve their body image in order to begin a new life. This aspect is further supported by the observation that 76.2% of the individuals in the PR group were married, possibly suggesting either that there may be many unhealthy foods, such as snacks, in a family house, particularly if there are children, or that married people may have had little motivation to take care of their bodies, or, worse, live in an environment of tension and stress, to which eating is a reaction. In patients who underwent gastric bypass, singles achieved a higher percentage of %EWL than married people (89.8% and 77.7%, respectively), whereas married people were at more than 2.6 times the risk of failing compared with those who were unmarried; at the same time, singles had more time for regular physical activities. 8
Educational level status evolved as another factor affecting the success of weight loss in our study group, as tertiary education and postdoctoral subjects had greater difficulty in losing weight. Although this parameter has already been underlined as a negative predictor, 16 no study so far offers any explanation. This finding is probably related to the observation that they asked more questions during the monthly interviews, because of prior knowledge and interest, but in the final analysis, the complexity of their thought processes may detract from their ability to lose weight.
Both groups had similar and equally high percentages of members with a long history of previous attempts to lose weight. Patients with repeated dietary attempts related to weight cycling have been found to be more prone to regain weight. 30 Previous dieting and weight loss attempts have emerged as reliable negative predictors of weight loss.28,30,31 Despite the lack of association between the number of previous slimming attempts and weight loss,32,33 it is possible that some subjects regard this treatment option as one more in the long track of the previously failed attempts and thus are more prone to low self-confidence and impaired motivation. 28 The same also applies for those coming not from self-motivation but as a condition for treatment for comorbidities, and this accounted for approximately 20% of our participants, in both groups.
Although knee osteoarthritis emerged as the most common comorbidity, followed by sleep apnea, the small difference in the incidence between groups suggests that comorbidities did not constitute a serious motivation for weight loss.
Psychosocial personality could be regarded as an additional “comorbidity.” In many cases, obese individuals dislike their bodies, and a poor body image has been associated with binge eating and low self-esteem and may partially explain their level of psychological distress.34,35 Additionally, failure to reach a self-determined goal may negatively impact on an individual's self-belief in his or her ability to control his or her weight, which will by itself result in giving up. 36 Conversely, dissatisfaction with one's appearance and quality of life and suffering as a result of comorbidities might imply greater motivation for making changes. 37 A retrospective study has shown that a greater concern with weight, body shape, and appearance in women works positively, and pride in appearance has been rated among the top four factors facilitating weight maintenance. 38
A key difference between the SR and PR groups was the initial cause of motivation, which is one of the most obvious aspects in weight control, because higher pretreatment motivation is related to greater weight loss.28,37 In the present study, patients who succeed in losing weight were mostly found to have decided to improve BW in order to alleviate comorbidities and, second, to improve body image. Low self-esteem seemed to motivate those in the PR group simply to do something (anything), but the result tended to be failure. This is additionally verified by the difference in the rate of adherence to monthly interviews for dieting instructions and re-education relating to eating habits. Those who were determined to participate in the program and lose weight for specific positive reasons, and of their own volition, were thus more successful because autonomous motivation implies an internal locus of causality for behavior. According to the self-determination theory, the probability that a person will or will not persist with a behavior depends on the extent to which he or she believes that the idea for initiating and subsequently continuing to regulate said behavior comes from within him- or herself. 37 The vast majority of individuals in the SR group (85.2%) attended the maximum of six interviews, whereas a comparable percentage in the PR group (83.8%) attended fewer than four interviews per month. Because treatment interventions work by strengthening the self-confidence, leading to better outcomes, those who failed to attend support sessions were left to themselves, unsupported, and were thus prone to give up more easily.
Physical activity, besides facilitating weight loss through direct energy expenditure, can also improve well-being, which may in turn facilitate the other positive behaviors needed for weight loss. 35 Poor compliance in carrying out the exercise protocol, as seen in the PR group, is generally considered a serious cause of today's obesity epidemic and for discouraging results in weight loss efforts.32,39,40 This viewpoint is supported by the evidence of the 85.8% participation in physical activity by the SR group, who fully complied with the gym program. A stronger sense of autonomy in starting and maintaining participation throughout the program (as opposed to controlling motivations) was a predictor of better weight loss. 35 It seems that the strict dedication to the goal of appearance improvement, assessed by the attendance at monthly interviews and the compliance with an exercise program, constitutes a crucial factor in sustaining or even advancing the good results obtained by BIB insertion.
Taking together all the important pre-BIB insertion prognostic indicants in a multivariate model—advanced age (around 40 years), female gender, basic educational level, and single or divorced marital status—were identified as the most powerful determinants influencing weight loss, in a positive manner. It seems that these patients, after several previous attempts and having passed through a period of body image dissatisfaction and mood disorder, have decided to change their way of thinking, behavior, and life-style to include significant weight loss, a healthy diet, and physical activity and to become more confident and feel better about their bodies and themselves generally.
In conclusion, the profile of obese individuals who are likely to benefit from an intragastric balloon insertion is multifactorial in origin, involving demographic, anthropometric, educational, social, and psychological parameters. This could serve as an additional tool in the area not only of successful outcome prediction but, more importantly, of delineating contributors to possible failure, as well. Further studies are needed to verify our conclusions and to clarify how pre-education and psychological support could produce successful weight loss in greater numbers of patients.
Footnotes
Disclosure Statement
No competing financial interests exist.