
Abstract
Abstract
Objective:
Palmar hyperhidrosis is a common disease that causes intense significant embarassment for patients. Bilateral single-port thoracoscopic sympathectomy is an effective surgical treatment with high success rates and improvement in quality of life. In order to reduce surgical invasion and to seek better cosmetic results, we describe a novel protocol for thoracic sympathectomy in the treatment of palmar hyperhidrosis.
Materials and Methods:
Between January 2012 and September 2012, bilateral thoracic sympathectomy was performed through the anterior mediastinal pleura using the pleural videoscope with a single unilateral skin incision in 10 men and 6 women.
Results:
In total, 16 patients were cured, and the skin temperature increased by a mean of 2.7±0.6°C. The average operation time was 67.9±15.8 minutes, with a postoperative hospital stay of 1.9±0.6 days and operative bleeding of less than 20 mL. All operations were successful, with no severe complications or perioperative mortality. Follow-up of 9.8±2.3 months (range, 7–14 months) showed that palmar sweating improved in all patients, and the effective rate was 100%.
Conclusions:
A single unilateral incision for two-sided thoracic sympathectomy through the anterior mediastinal pleura is an effective, feasible, safe, and minimally invasive procedure with excellent cosmetic results.
Introduction
I
In this article, based on the work of Hidehiro Yamamoto, we presented a feasible and effective approach of bilateral thoracic sympathectomy with a single unilateral skin incision using the semirigid pleural videoscope through the anterior mediastinal pleura.
Materials and Methods
The novel protocol
From January 2012 to September 2012, there are 10 men and 6 women (mean age, 22.4±3.9 years) with primary palmar hyperhidrosis who underwent bilateral thoracic sympathectomy using the LTF-240 pleural videoscope (Olympus, Tokyo, Japan) (external diameter, 7 mm). All patients had routine preoperative evaluation, such as chest X-ray, chest computed tomography, electrocardiogram, and adrenal and thyroid function examination, with all consents obtained.
The patients were given general anesthesia through a double-lumen endotracheal tube and placed in a supine position, with 90° abduction of the right upper limb and the armpit exposed. The electrocardiogram monitor, blood pressure, arterial oxygen saturation, and skin temperature were monitored using a multichannel thermometer (Bat 12; Physitemp Instruments, Clifton, NJ) with probes taped to the palm. Mechanical ventilation was set to the one-lung (left) ventilation mode. A small transverse incision 7 mm in length was made in the right fourth intercostal space at the anterior axillary line, which was used as the camera port. The right sympathetic trunk and T4 sympathetic ganglion were identified accurately (Fig. 1A). A coagulation wire was inserted through the working channel of the pleural videoscope, and the right lateral mediastinal pleura was opened by electric coagulation (Fig. 1B). The scope was then advanced gradually through the anterior mediastinal pleura by electric coagulation under direct visualization; meanwhile, the mechanical ventilation was switched to the one-lung (right) ventilation mode.
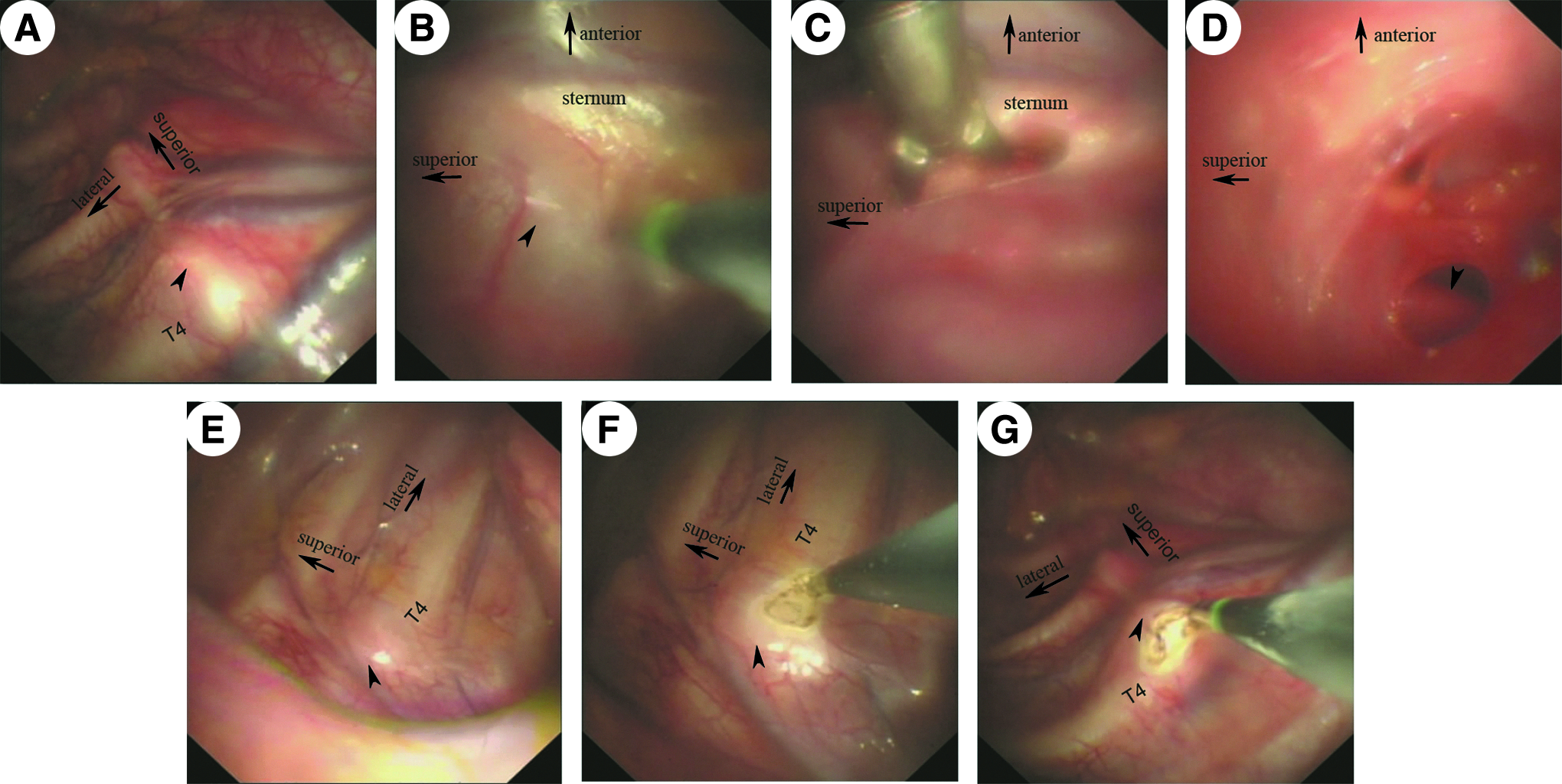
Demonstration of the novel approach of bilateral thoracic sympathectomy by the Olympus LTF-240 pleura videoscope with a single skin incision through the anterior mediastinal pleura.
In cases in which it is difficult to achieve access to the left thoracic cavity through the anterior mediastinal pleura by the videoscope alone, considering the potential risk of the injury of nearby vital structures by electric coagulation without satisfactory field exposure, extension of the skin incision may be necessary for the insertion of a separating forceps (external diameter, 5 mm) besides the pleural videoscope, which means the length of the skin incision extended to 12 mm.
The tunnel through the anterior mediastinal pleura was performed by electric coagulation and blunt dissection by the separating forceps (Fig. 1C) until the left thoracic cavity was exposed (Fig. 1D). When the videoscope entered the left pleural space, the left sympathetic chain and T4 sympathetic ganglion were identified (Fig. 1E). Subsequently, the sympathetic chain was transected by electric coagulation at the level of the fourth rib (Fig. 1F). Palm skin temperature rose about 1–3°C since the ablation, which indicated a correct target.
The mechanical ventilation was switched to the one-lung (left) ventilation mode. After the left lung had been fully expanded and the air of the left pleural space was drained by the videoscope, the videoscope was pulled back to the right thoracic cavity. The right sympathetic chain was transected in the same way as on the left side at the same level (Fig. 1G). Then, the mechanical ventilation was switched to the two-lung ventilation mode. After the bilateral lung had been fully expanded, the videoscope was removed. The incision was then closed with a subcutaneous suture.
The novel approach is illustrated in Figures 1A, B, and D–G and 2 for routine cases and in Figure 1 in its entirety for patients with wide and thick anterior mediastinal pleura.
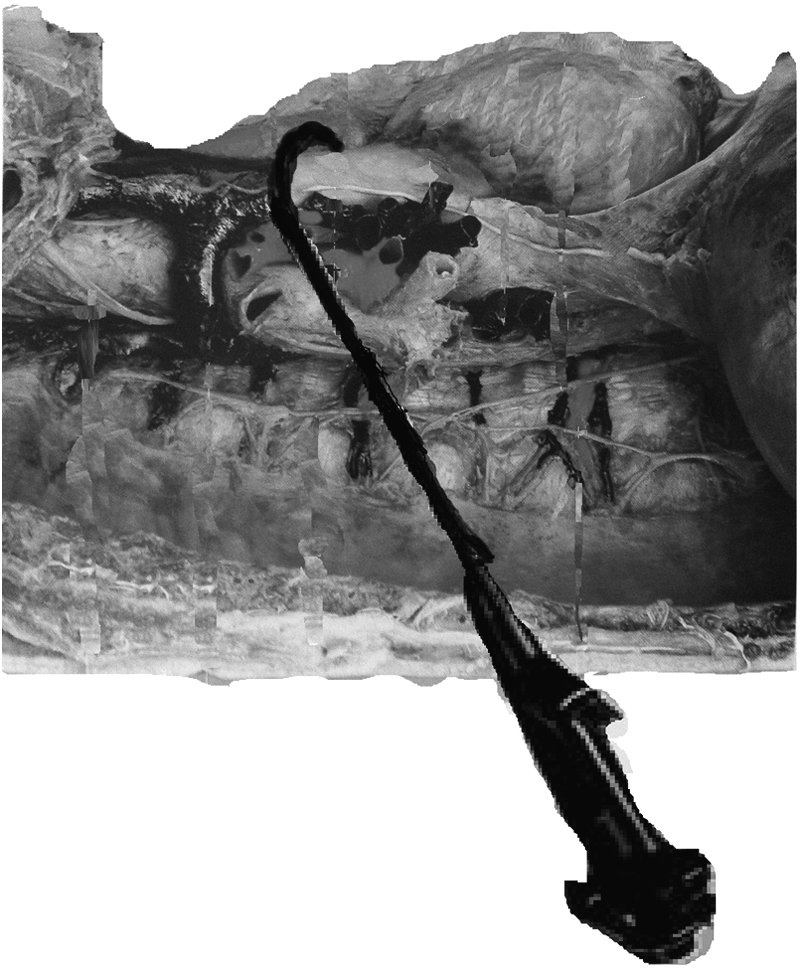
A demonstration of this technique was performed using a cadaver.
The typical bilateral two-port protocol
From January 2012 to September 2012, there were six men and five women (mean age, 23.4±5.4 years) with primary palmar hyperhidrosis who underwent a standard surgical procedure. The patients were given general anesthesia through a double-lumen endotracheal tube and placed in a supine position, with 90° abduction of both the upper limbs and the armpits exposed. After initiation of single-lung (left) ventilation, a thoracoport (10 mm) was placed in the right fifth intercostal space at the midaxillary line, and a assistant incision (5 mm) was placed in the right third intercostal space at the anterior axillary line for insertion of the electrocoagulation hook. After general inspection and identification of the right thoracic sympathetic trunk, the sympathetic chain was transected by electric coagulation at the level of the fourth rib. Extensive cauterization was carried out over the rib nearly 2 cm laterally in order to divide the accessory pathways. The air was drained, and the incision was then closed with a subcutaneous suture. Sympathectomy on the other side was completed in the same way.
Statistical analysis
Outcomes studied included patient characteristics, operative details, patients' satisfaction (yes/no) with their procedure, complications, including compensatory hyperhidrosis, using a descriptive scale (Table 1), and outcomes of follow-up, and analyses were performed with the statistical software SPSS version 20.0 for Windows (SPSS, Inc., Chicago, IL). Categorical values were compared with analysis of variance and the chi-squared test. A value of P<.05 was considered significant.
Results
Bilateral thoracic sympathectomy was performed successfully in a total of 16 patients by the LTF-240 pleura videoscope (as shown in Table 2), without leading to hemorrhage, arrhythmia, cardiac arrest, Horner's syndrome, or other severe complications. No conversion to the open technique was necessary. The procedure in 1 of 16 patients was performed by the bilateral single-port approach (two ports in total) because of the flat chest and the blockage of the superior vena cava, making dissection of the anterior mediastinal pleura by electrocoagulation highly risky. The procedure was performed in the other 15 patients with one single skin incision method (2 of 16 by the left lateral approach, 13 of 16 by the right lateral approach). After the surgery, all patients showed warm and dry palms without hyperhidrosis, and the palm temperature increased by a mean of 2.7±0.6°C. The mean time for the bilateral operation was 67.9±15.8 minutes. The mean postoperative hospital stay was 1.9±0.6 days, and operative bleeding was less than 20 mL.
P<.01.
SD, standard deviation.
All operations were successful with no severe complications or perioperative mortality. Minor pneumothorax (<15%) was observed in 5 of 16 patients on the first postoperative day, which could be resolved on its own; none need placement of a chest tube. Follow-up of 9.8±2.3 months (range, 7–14 months) showed that palmar sweating improved in all patients, and the patients' satisfaction with their procedure effective rate was 100% (the success rate is evaluated by dry hands). Mild and moderate compensatory sweating, which could be tolerable, occurred in 43.8% of patients. Other complications, including Horner's syndrome, severe compensatory hyperhidrosis, recurrence of palmar hyperhidrosis, postoperative costal neuralgia, etc., were not observed.
During the interval from January 2012 to September 2012, six men and five women (mean age, 23.4±5.4 years) with primary palmar hyperhidrosis underwent bilateral thoracic sympathectomy using a video-assisted thoracoscope by the typical two-port approach (one 10-mm port for the thoracoscope and the other 5-mm port for the electric coagulation hook) in our center (as shown in Table 2). The two groups were comparable in gender distribution, mean age, postoperative elevation of temperature, operation time, postoperative hospital stay, effective rate, complications, etc. The incision was significantly smaller in the novel protocol group (7.8 mm versus 30 mm, P<.01), with better cosmetic results.
Discussion
Primary hyperhidrosis is a pathological disorder, characterized by excessive secretion of the exocrine sweat glands, the etiology of which is unknown. Palmar involvement is naturally termed as palmar hyperhidrosis. There are two main types of palmar hyperhidrosis: primary and secondary. The exact cause of primary palmar hyperhidrosis is unknown, whereas the secondary type is considered to be related with obesity, diabetes, hyperthyroidism, side effects of drugs, etc. For many patients, it is debilitating and impairs social interactions. In the 1990s, studies concluded that ETS is currently the surgical gold standard treatment for hyperhidrosis, and ETS is recommended for those with moderate to severe hyperhidrosis who have not responded to any of the other treatments.
Typically, depending on the preference of the surgeon, one- to three-port thoracoscopic sympathectomy for each side was commonly applied, which, however, resulted in a relative large wound scarring. Hidehiro Yamamoto developed a new technique of bilateral ETS with only one single skin incision. The key of this approach is that puncture of the right mediastinal pleura using a unique curved scope guide and the flexible bronchoscope could be guided into the right pleural cavity through the retrosternal pulmonary junction. However, this technique has some limitations, including dependence on a unique scope guide, pneumopleural adhesions, thick width of the retrosternal pulmonary junction, anatomical abnormalities, and high risk of bleeding and injury of the vital structures during the puncture.
In the early 1990s, the diagnostic flexible bronchoscope used as a rigid thoracoscope for the treatment of pneumothorax and undiagnosed pleural effusion was reported.4–6 It was found to be feasible, but the flexibility of the instrument made manipulation within the pleural space difficult. Consequently, the pleuroscope, a semirigid scope combining features of both instruments, having a solid body and a flexible terminal tip, was invented. 7 Subsequently, a videoscope with the same design as the pleuroscope was designed, called the pleura videoscope, which optimized the advantages of both rigid and flexible scopes. 8 The pleura videoscope was successfully applied to the diagnosis of pleural effusions, 9 assessment of vascular patterns of the pleura using a pleura videoscope with narrow band imaging for the selection of optimal biopsy sites, 10 etc.
Based on the above points, the present work was designed to test the feasibility and efficacy of the pleura videoscope applied to bilateral thoracic sympathectomy with a single skin incision through the anterior mediastinal pleura. Our experience demonstrated that bilateral thoracic sympathectomy with a single skin incision through the anterior mediastinal pleura using the pleura videoscope was a feasible and effective approach for the treatment of palmar hyperhidrosis, with highly satisfactory cosmetic results.
There are several essential differences between the present technique and that described by Yamamoto et al., 3 although we both focus on only one single skin incision for thoracic sympathectomy. First is the pleura videoscope applied in the present study. During the first decade of the 21st century, the innovative pleura videoscope was designed; the semirigid LTF-240 scope, having a solid body that just acts like the role of the metal scope guide used in the work of Yamamoto and a flexible terminal tip, makes manipulation within the pleural space quite simple and gives good field exposure, independent of the unique scope guide. Second is the improvement of safety. The essential part of the approach is the dissection of the anterior mediastinal pleura, making a tunnel to the contralateral thoracic cavity. The dissection by our approach could be gradually advanced and adjusted in time under direct visualization, which would decrease the risk of potential bleeding and injury of the vital structures. Third is the extension of the surgical indication. Relative contraindications, such as thick width of the retrosternal pulmonary junction and anatomical abnormalities, would be eliminated by the present technique. Considering the good qualities of this novel approach, we believe that this technique is highly recommended for the treatment of palmar hyperhidrosis and can be explored as a cue for the application of the traditional diagnostic endoscope to therapeutic procedures.
The following are some experiences in this study: (1) We suggest that the single skin incision should be made in the right fourth intercostal space of the anterior axillary line. The first 2 cases were performed perfectly in the left lateral way. However, we had to make a conversion to the bilateral one-port approach (two ports in total) because of the blockage of the superior vena cava during the third case, making the dissection of the anterior mediastinal pleura by electrocoagulation highly risky. The superior vena cava and other structures could be exposed more satisfactorily in the right lateral approach, which could minimize the risk of fatal bleeding. So, the procedure in the rest of the (13/16) patients was performed by the right lateral approach. (2) Regarding patients with a wide and thick anterior mediastinal pleura, we suggest making a lateral extension of the previous skin incision (one single skin incision, 7+5=12 mm in length) for the insertion of a separating forceps (external diameter, 5 mm), which could be used for the blunt dissection of the anterior mediastinal pleura and was very helpful to the field exposure for electric coagulation. (3) After the identification of the right sympathetic chain, do not transect the right chain at the T4 level directly; reach the left thoracic cavity through the anterior pleura, and identify the condition of the left sympathetic chain, to make sure that the bilateral thoracic sympathectomy could be performed at the same level.
Naturally, the approach has some limitations. First, compared with the previous studies, the procedure time we need for this bilateral procedure (on average, more than 1 hour) is relative longer. However, we consider that the procedure time needed for this novel approach will become increasingly shorter after it has been carried out on a larger number of cases. Second, the small sample size may affect the preciseness of the statistical result, and the novel protocol should be re-evaluated in large clinical trials in the future. Also, this method is also relatively contraindicated in cases of pneumopleural adhesions. In the future, we would continue to improve the approach, such as making the skin incision around the border of the areola for a better cosmetic result in male patients (on the lower border of the breast in female patients), evaluating the cosmetic result accompany with questionnaires, using single-lumen intubation for better protection of the trachea and bronchus, etc.
Conclusions
The present study has shown that the pleura videoscope applied to bilateral thoracic sympathectomy with a single skin incision through the anterior mediastinal pleura is feasible and reliable, which is an important advancement for thoracoscopic sympathectomy.
Footnotes
Disclosure Statement
No competing financial interests exist.