
Abstract
Abstract
Background:
Transareola single-site endoscopic thyroidectomy has been successfully established as a surgical approach. This study investigated the feasibility and safety of transareola single-site endoscopic thyroidectomy for bilateral thyroid disease.
Patients and Methods:
Twelve patients who underwent bilateral thyroidectomy were enrolled in this study. The surgical outcomes were analyzed, including operation time, intraoperative bleeding volume, postoperative pain score, and cosmetic satisfaction score.
Results:
All patients underwent successful transareola single-site endoscopic bilateral thyroidectomy, and no patient was semiconverted to three-port endoscopic surgery or open surgery. Seven patients underwent bilateral partial thyroidectomy, and 5 patients underwent subtotal thyroidectomy plus contralateral partial thyroidectomy. The mean operation time was 165±23.8 minutes (range, 142–185 minutes). The mean intraoperative bleeding volume was 27.3±12.3 mL (range, 20–45 mL). The mean postoperative wound drainage was 121±45.8 mL (range, 85–137 mL). The drainage tube was removed 3–4 days after surgery. The mean visual analog scale score was 3.3±2.5 (range, 1–5) at 24 hours postoperatively. The patients were followed up for 2 month with no complaint of chest wall wound pain and numbness. The mean cosmetic satisfaction score was 9.55±0.8 (range, 8–10).
Conclusions:
Transareola single-site endoscopic bilateral thyroidectomy is feasible and safe and has the advantages of high cosmetic satisfaction.
Introduction
L
In this study, we present 12 cases in patients who underwent transareola single-site endoscopic bilateral thyroidectomy in Fengxian Central Hospital (Shanghai, China) from January 2011 to April 2013. All patients achieved good clinical outcomes, and none was converted to the three-port endoscopic or an open surgical approach.
Subjects and Methods
Subjects
This study included 12 consecutive patients (11 female and 1 male) with bilateral benign thyroid diseases undergoing transareola single-site endoscopic thyroidectomy. Their average age was 26.7±4.8 years (range, 19–48 years). Preoperative ultrasonography was performed in all patients to precisely define the dimensions, location, and number of the thyroid nodules and the lymph node involvement and to determine whether partial or subtotal thyroidectomy should be performed. The boundary of the thyroid nodule was regular, with no abnormal blood flow signal and microcalcification. The diameter of the larger thyroid nodule ranged from 1.2 to 4.0 cm (mean diameter, 2.3±0.4 cm), and that of the smaller one ranged from 0.5 to 2.0 cm on the contralateral thyroid gland (mean diameter, 1.3±0.2 cm). Presurgical computed tomography revealed bilateral thyroid nodules with no signs of malignancy such as fine sand-like calcification (Fig. 1). Fine-needle aspiration cytology was performed in 8 cases and detected no malignant cells. All patients had normal thyroid function.
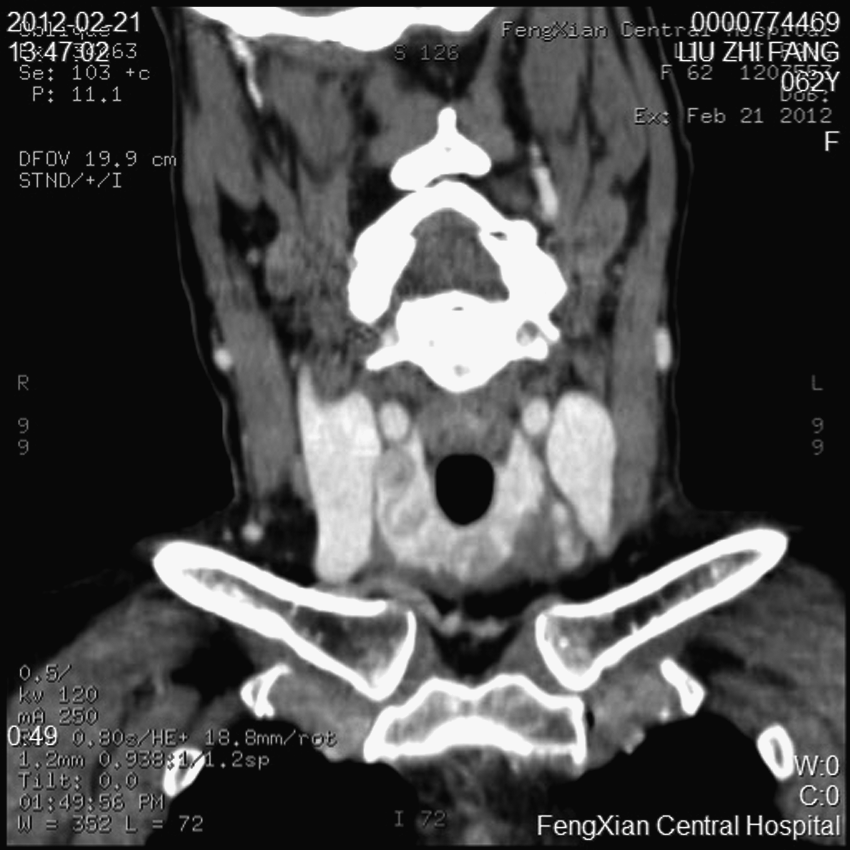
Computed tomography revealed bilateral thyroid nodules.
The inclusion criteria were as follows: (1) the maximum diameter of the larger thyroid nodule on one lobe was less than 4 cm and that of the smaller on the other lobe was less than 2 cm; (2) a high possibility of a benign nodule was considered during preoperative examinations; (3) intraoperative frozen pathological section detected no malignant cells in 12 patients; (4) none had a history of neck operation and radiotherapy and medical history of severe coagulation disorders and organic diseases of important organs like the heart, lung, and kidney; and (5) all the patients had a strong desire for cervical cosmesis.
Postoperative pain was assessed by a visual analog scale (VAS), which consisted of words with “no pain” on the left side at 0 and “worst pain imaginable” on the right side at 5. 10 The cosmetic result was evaluated by the patient using a numerical scale ranging between 0 (worst) and 10 (best).
We evaluated the surgical outcomes of the thyroidectomy, including operation time, intraoperative bleeding volume, postoperative pain score, and cosmetic satisfaction score.
Surgical techniques
Under general anesthesia, the patient was placed in a supine position with the neck mildly hyperextended. With the two legs of the patient separated, the operator stood between them, a television screen was placed at the head of the patient, and the two assistants stood on both sides of the patient. The operating path was marked from the areola on the surface of the large thyroid nodule side to the neck (Fig. 2). A 20-mm incision delineated along the ipsilateral areola margin. A narrow subcutaneous tunnel was bluntly dissected in the anterior surface of the pectoralis major muscle and clavicle. A 10-mm trocar was inserted to pump CO2 into the cavity, with pressure maintained at 6–8 mm Hg, and a 30° 10-mm rigid laparoscope (Stryker Endoscopy, San Jose, CA) was implanted. A 5-mm trocar was inserted adjacent to the laparoscope hole, and an ultrasonic scalpel (model GEN300; Ethicon, a Johnson & Johnson Company, Somerville, NJ) was implanted upward to the thyroid cartilage for separation of surgical space. The linea alba cervicalis was incised using an electric coagulation hook, and the strap muscles were separated. The thyroid gland was exposed using the neck suture suspension technique (one or two sutures) (Fig. 3), and the middle thyroid vein was cut with an ultrasonic scalpel. The thyroid lobe with the larger nodule was suspended with one or two sutures, penetrated through the external skin of the neck, and pulled inward. The back tissues of the thyroid gland were separated and coagulated with an ultrasonic scalpel. After disarticulation of the upper or lower vessels of the thyroid gland, the thyroid nodule was cut by the ultrasonic scalpel, and the residual normal gland was not sutured. The contralateral lobectomy was similarly performed. The posterior capsule of the thyroid was dissected integrated throughout the surgery. The linea alba cervicalis was intermittently sutured with two absorbable sutures.

A 120-mm2 incision delineated along the upper ipsilateral areola border on the same side of the large thyroid nodule.
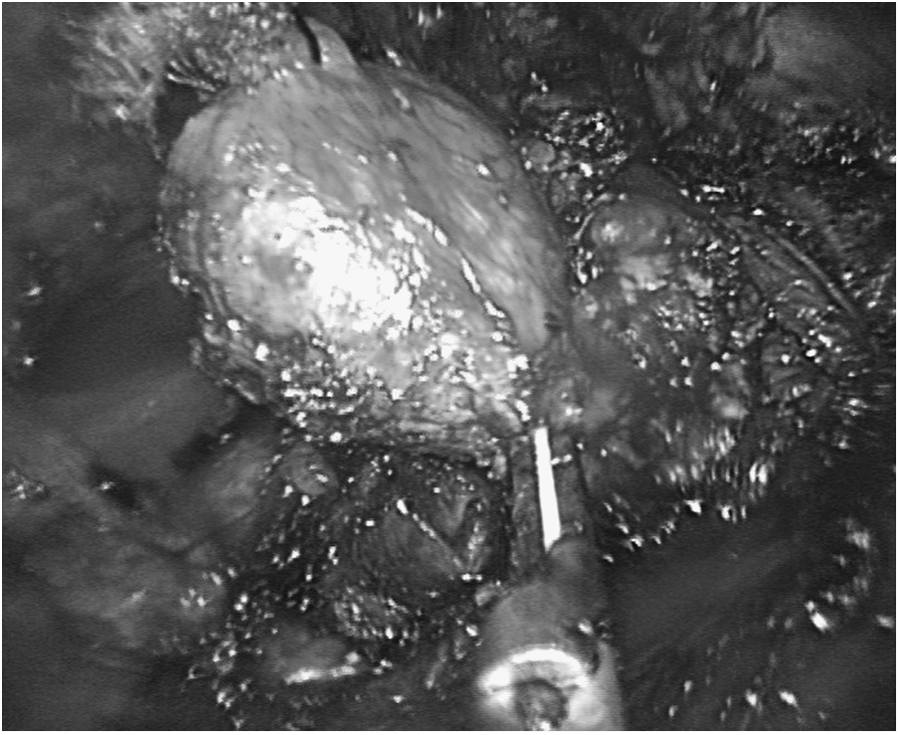
The thyroid gland was exposed using the neck suture suspension technique.
The resected specimen was placed into a specimen bag, extracted through that operative hole, and sent for frozen histologic examination. After the presence of bleeding on the wound side was checked, a negative pressure drainage tube was placed through the incision on the areola, the incised skin was sutured intradermally, and the wound side was compressed and bandaged.
Results
All 12 patients successfully underwent transareola single-site laparoendoscopic bilateral thyroidectomy, and none was converted to three-port endoscopic surgery or open surgery. Bilateral subtotal lobectomy was performed in 7 patients, versus subtotal plus contralateral partial thyroidectomy in 5 patients. The mean operation time was 165±23.8 minutes (range, 142–185 minutes). The average intraoperative bleeding volume was 27.3±12.3 mL (range, 20–45 mL). The total postoperative wound drainage was 121±45.8 mL (range, 85–137 mL). The drainage tube was removed 3–4 days after surgery, before the patient was discharged. The average soft tissue dissection area delineated along the operation path was 118±25 cm2 (Fig. 2). Postoperative pathological examination diagnosed bilateral thyroid adenoma in 4 cases, bilateral nodular goiter in 5 cases, and both thyroid adenoma and nodular goiter in 3 cases. No symptoms of cough after drinking water, hoarseness, or tetany were observed after surgery. All patients were asked to use the VAS to report their pain at 24 hours postoperatively. The mean VAS score was 3.3±2.5 (range, 1–5). Two patients received one-time analgesic therapy with bucinperazine after surgery, whereas no analgesic measures were performed in the other 10 patients. No patient complained of pain, hypesthesia, or paresthesia in the anterior chest wall at the 2-month postsurgical follow-up. All 12 patients were satisfied with the cosmetic results of the operation. The mean cosmetic satisfaction score was 9.55±0.8 (range, 8–10).
Discussion
Thyroid disease is prevalent in young women, and they desire reducing or even eliminating neck scarring. Conventional open thyroidectomy leaves a permanent 6–8-cm transverse incision exposing in the anterior neck. Such a scar results in cervical hypesthesia, paresthesia, or even harmful psychological effects in patients' complaints after surgery. Instead, endoscopic thyroidectomy leaves no operative scars in the neck and becomes more and more attractive for thyroid surgery. Gagner 11 reported a case of endoscopic parathyroidectomy in 1996, in which endoscopic procedures was applied in cervical surgery for the first time. Endoscopic neck surgery for the thyroid was developed by Hüscher et al. 12 in 1997. In 2000 Ikeda et al. 13 and Ohgami et al. 14 performed three-port endoscopic thyroidectomy via the axillary and breast approaches, respectively, and further improved the cosmetic result. 15 However, conventional endoscopic thyroidectomy requires the creation of three tunnels from skin incisions, which involves a much wider subcutaneous tissue dissection and results in even some hypertrophic scarring at the site of the middle incision. According to Miccoli, 16 total endoscopic thyroidectomy should not be considered minimally invasive, but rather a cosmetic operation, because of the extensive dissection and long operative time. Others 17 considered the total endoscopic procedure to be minimally invasive because the dissection level was located in loose connective tissue in the chest wall without injury to the mammary gland or duct, as well as under the platysma in the neck.
Transareola single-site endoscopic thyroidectomy involves significantly less tissue dissection, and thus less injury, to patients, improving the popularity of this technique. Many studies have reported unilateral thyroidectomy via transareola single-site endoscopic thyroidectomy.7,8 We successfully performed transareola single-site endoscopic unilateral thyroidectomy in patients and established promising modality. 9 With an increase in experience, we gradually expanded surgical indications and performed transareola single-site endoscopic bilateral thyroidectomy in selected cases. Transareola single-site endoscopic thyroidectomy is performed in a unidirectional view and a single channel. Thus, the limited surgical space leads to the characteristics of difficulty in operation, visceral pulling, and limitation of the operative field. When the subcutaneous operation space is separated, the anatomical plane should be fully understood, and the subcutaneous separation stick should be used under the superficial layer of deep fascia (loose tissues and a few vessels), so as to avoid damaging the subcutaneous small vessels or dermis, which would result in subcutaneous fat liquefaction, skin ecchymosis and inflammation, and secondary infections. Intraoperative CO2 pressure is very important. 18 High CO2 pressure may enabled hypercapnia respiratory acidosis, subcutaneous emphysema, and air embolisms, whereas low CO2 pressure may affect the surgeon being able to identify the contralateral thyroid lobe. Therefore, the CO2 pressure used with our approach was set at 6–8 mm Hg.
Cervical transcutaneous suture suspension and retraction also play an important role in our transareola single-site endoscopic thyroidectomy procedure, which pulled the thyroid gland and strap muscles to the medial and lateral sides and led to clearer exposure and safer operation of the single-site endoscopic surgery. In addition, the ultrasonic scalpel's power was very helpful in this procedure 19 in that it produced little smog and eschar, and the thermal injury was less than 1 mm, which resulted in precise anatomical separation and stypsis and achieved a good hemostatic effect. In the present study, thyroidectomy directly disarticulated the thyroid artery and vein, which simplified surgical procedures. Before disarticulation of the upper and lower vessels of the thyroid gland, the ultrasonic scalpel precoagulated the proximate end and the distal end, which enabled more exact vascular closure. When the posterior side of the thyroid gland is dissected, the head of the ultrasonic scalpel was placed upward, which made it closely contact with the thyroid membrane, and separated neighboring tissues, so as to avoid damage to the parathyroid and laryngeal recurrent nerve. After complete hemostasis, a closed suction drain was inserted, which was removed when the volume of operation wound exudates was less than 10 mL 3–4 days later.
The bilateral thyroidectomy was performed in selected cases with benign signs. According to the inclusion criteria for this approach, the maximum diameter of the larger thyroid nodule was less than 4 cm, and that of the contralateral smaller one was less than 2 cm. The incisions delineated along the upper ipsilateral areola border at the same side of the larger thyroid nodule. Dissection of the smaller thyroid nodules must cross the trachea, an obstacle to the surgery, which required a smaller nodule diameter.
The transareola single-site endoscopic thyroidectomy has a better cosmetic result, as the skin incision is located on the border of the areola, which conceals the surgical scar. In the present study, the separation area is about 120 cm2. The transareola single-site endoscopic thyroidectomy is less invasive because it involves less subcutaneous dissection compared with three-port endoscopic thyroidectomy. In the current study, the mean VAS score was 3.10 at 24 hours postoperatively. The 2-month postsurgical follow-up revealed that the mean cosmetic satisfaction score was 9.5. In conclusion, transareola single-site endoscopic thyroidectomy is safe and feasible for selected patients with benign thyroid nodules and has the advantages of a covert incision, less subcutaneous separation, and high cosmetic satisfaction.
Footnotes
Disclosure Statement
No competing financial interests exist.