
Abstract
Abstract
Background:
Single-port laparoscopic surgery (SPLS) has been introduced for totally extraperitoneal (TEP) inguinal hernia repair. The aim of this study was to report our initial experience with SPLS TEP inguinal hernia repair in 100 patients by a single-port laparoscopic surgeon who had no prior experience of conventional TEP hernia repair.
Patients and Methods:
Between October 2012 and December 2013, 100 patients underwent SPLS TEP inguinal hernia repair by a single surgeon. The procedures that were performed in the preperitoneal space did not differ from those in conventional TEP repair. Patient demographics, type of hernia, and operative and postoperative outcomes were analyzed. Also, we compared the results of current series with the data of the other studies for single-port TEP inguinal hernia repair.
Results:
Among the 100 patients, SPLS TEP inguinal hernia repair was successful in 99 patients; 1 patient required additional incisions for inserting the trocar. The mean operative time and postoperative length of stay were 97.8 minutes (range, 55–185 minutes) and 1.3 days (range, 1–4 days), respectively. In the current series, the operation time was longer than those in the other studies for SPLS TEP repair. Recurrent hernia, history of lower abdominal surgery, and peritoneal tear during the operation were significantly associated with prolonged operation time. The other data, including perioperative complications, were similar.
Conclusions:
In our experience, the transition from standard hernioplasty to SPLS TEP inguinal hernia repair by an experienced SPLS surgeon was feasible. However, a learning curve is necessary.
Introduction
I
In the clinic, SPLS was initially used to treat appendicitis and cholecystitis, but it is now widely accepted in many other areas of surgery.3–5 Inguinal hernia repair was not an exception to this trend, and clinical reports on totally extraperitoneal (TEP) hernia repair and transabdominal preperitoneal hernia repair by SPLS have been presented occasionally. Of these techniques, TEP hernia repair is preferred because of the low risk of intraperitoneal injury and the disease entity of inguinal hernia as an extraperitoneal disease. In almost all cases, this novel technique was safe and feasible, and some authors concluded that the shift in technique for training a laparoscopic surgeon is minimal. 6
Herein, we hypothesized that an experienced SPLS surgeon could perform a single-port TEP surgery for inguinal hernia repair with appropriate preparation for starting SPLS TEP hernia repair. The aim of this study was to assess the safety and feasibility and to report our initial experience of SPLS TEP inguinal hernia repair performed by an experienced SPLS surgeon who was inexperienced in conventional TEP hernia repair.
Patients and Methods
Procedures
Between October 2011 and December 2012, 135 patients with inguinal hernias underwent surgical treatment at Daejeon St. Mary's Hospital, which is affiliated with The Catholic University of Korea. SPLS TEP repair was performed in 100 consecutive patients, and the current study retrospectively analyzed the collected data. Patients were informed about the differences between conventional laparoscopic surgery and SPLS. In cases where the patients and family members agreed upon SPLS and gave written informed consent, we performed SPLS TEP inguinal hernia repair. The study was approved by the ethics committee of Daejeon St. Mary's Hospital of The Catholic University of Korea (Institutional Review Board code DC13RISI0033). All patients over the age of 20 years who were eligible for conventional laparoscopic TEP hernia repair met the inclusion criteria. Most of the patients with a history of abdominal surgery were included as per our criteria. The exclusion criteria were patients with a large amount of ascites, an irreducible hernia, or previous major surgery in the lower abdomen indicated by scars over the surgical field.
All surgeries were performed by a single surgeon (B.J.C.) who had no prior experience of laparoscopic TEP inguinal hernia repair. He is a member of the minimally invasive surgery center at our institution and has performed more than 400 SPLS procedures for treating various diseases, including benign and malignant colorectal disease, appendicitis, cholecystitis, small bowel obstruction, etc. He has also performed more than 100 open tension-free mesh hernioplasties. Before initiating this study, he participated in conventional laparoscopic TEP hernia repair surgeries in 30 cases as a laparoscopic assistant and viewed more than 20 hours of SPLS TEP inguinal hernia repair videos. After this, he performed SPLS TEP inguinal hernia repairs. Characteristics of the patients and those of hernia, postoperative outcomes including postoperative pain at Day 1 and at Week 1, time for return to activities of daily life (ADL), and perioperative complications were assessed. Time for return to ADL was assessed 1 and 4 weeks postoperatively, using a questionnaire (questions were asked about walking, dressing, and bathing). The number of days taken to return to ADL was defined as the absence of any problem in walking quickly, changing clothing, and bathing independently. The pain was measured on a visual analog scale (VAS), ranging from no pain (0) to maximal unbearable pain (10).
Surgical technique
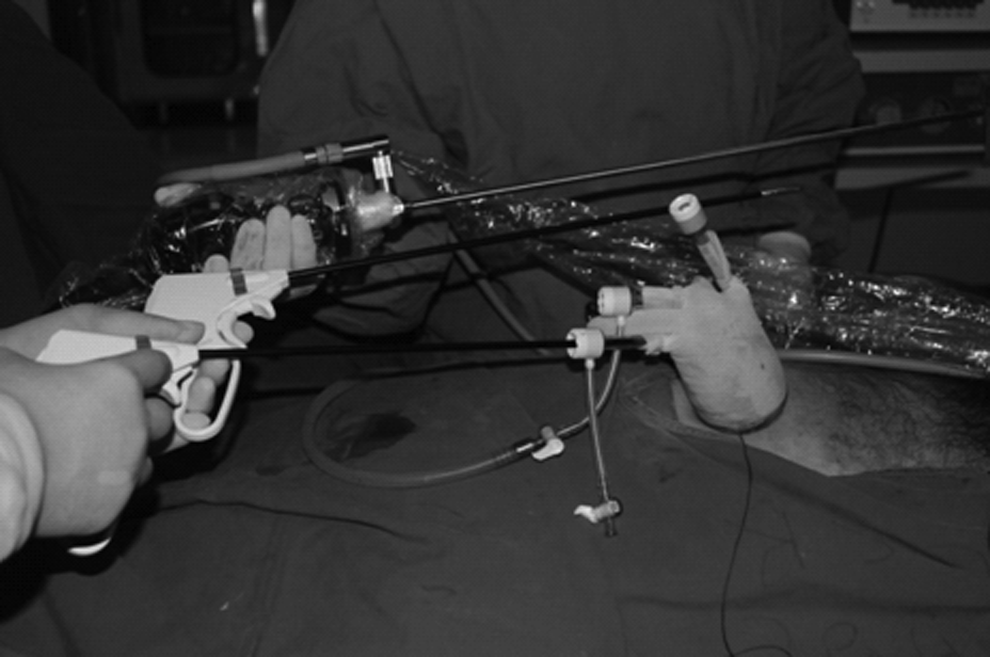
The patient was placed in the supine position with the arm opposite to the side of the hernia in adduction during general anesthesia. The operator stood on the side opposite to the hernia, and the laparoscopic assistant stood on the side of the hernia. A vertical incision, 1.5–2.0 cm in length, was made over the umbilicus, beginning from the deepest part of the umbilicus. After dissection of the subcutaneous tissue to expose the anterior rectus sheath on the side of the hernia, a transverse incision was made on the anterior rectus sheath. Then the space between the rectus muscle and the posterior rectus sheath was accessed by retracting the rectus muscle laterally. We attempted to insert the port device, which was a single port comprising a wound retractor (Xsmall; Applied Medical, Rancho Santa Margarita, CA) and a surgical glove. Three trocars were inserted in advance into the glove fingers. An 11-mm trocar was put into the middle finger, and two 5-mm trocars were put into the index and little finger of the glove, respectively (Fig. 1). Pneumoperitoneum was produced with a pressure of 8 mm Hg. A rigid 30° 5-mm laparoscope was inserted through the 11-mm trocar. We used the conventional straight and rigid type of laparoscopic instruments. The surgical procedure was performed after the patient was placed in the Trendelenburg position with the side of the hernia tilted up. The preperitoneal dissection was performed using a laparoscope and two instruments, usually a grasper and a suction device with hook tip (Surgiwand™; Covidien, Mansfield, MA). Positioning of the patient, the operative team's position, and pressure of the pneumoperitoneum were the same as those in conventional laparoscopic TEP inguinal hernia repair at our hospital. Procedures performed in the preperitoneal space were also the same. The overall operative techniques were similar to those described by Kim et al., 7 including the type of mesh and the method of mesh fixation.

The home-made glove port, which was composed of a wound retractor and surgical glove. An 11-mm trocar and two 5-mm trocars were utilized.
Statistical analysis
Numerical data were presented as mean and standard deviation values or as medians and ranges. We analyzed operative times using a moving average method. With this method, individual changes in operative time are removed, by shifting the mean values. As new data are added, by shifting the mean values, the changes in operative time are smoothed. Simple moving is a statistically process to compensate bias. Comparison between the operative times in patients with and without prior lower abdominal surgery, in patients with primary and recurrent hernia, and in patients with and without peritoneal tears was carried out using the unpaired sample t test. Results were considered statistically significant at values of P<.05.
Results
Among the 100 patients, SPLS TEP inguinal hernia repair was successful in 99 patients; 1 patient required additional incisions for inserting the trocar. The patients' characteristics are shown in Table 1.
The operative and postoperative outcomes are shown in Table 2. Patients with primary inguinal hernia had a significantly shorter mean operative time than patients with recurrent inguinal hernia (94.6 versus 117.5 minutes; P<.04). Patients who had not undergone previous lower abdominal surgery had a significantly shorter mean operative time of 93.3 versus 115.9 minutes (P<.04). We also analyzed operative times using a moving average method in 63 patients with primary unilateral hernia (Fig. 2). The mean operative time for each set of 10 patients decreased progressively. Analysis of the learning curve for operative time showed stabilization after 30 consecutive patients and a dramatic decrease after 50 patients. There were 23 intraoperative complications. Twenty-one patients had peritoneal tears, which were sutured intracorporeally in all cases. In these patients, the mean operative time was significantly longer than in the patients without intraoperative complications (88.7 versus 133.8 minutes; P<.04). In one of them, an additional trocar was required to secure suture closure for a very large peritoneal tear. One patient had continuous blood oozing from the dissection site of the spermatic cord structure. We inserted a drain via a stab incision on the suprapubic area, and the patient recovered well. There were no major postoperative complications. However, minor postoperative complications were noted in 11 patients and were well managed conservatively. The median follow-up period was 11.7 months (range, 5–19 months). During the follow-up period, there were no cases of recurrence.
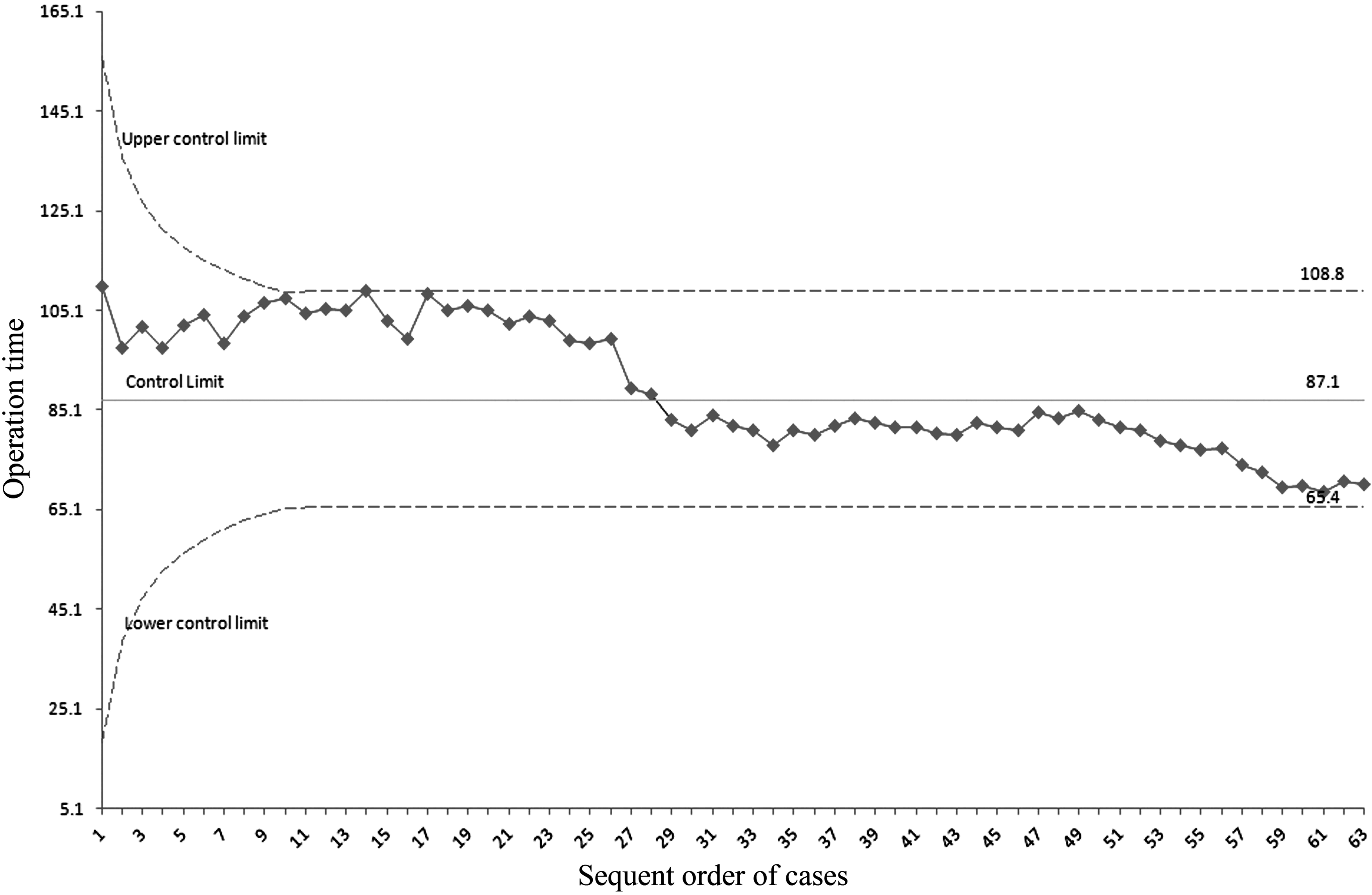
Learning curve analysis of single-port totally extraperitoneal inguinal hernia repair using a moving average method.
Data are mean (range) values unless indicated otherwise.
ADL, activities daily life; TEP, totally extraperitoneal; VAS, visual analog scale.
Discussion
Laparoscopic TEP hernia repair has been accepted as an efficacious surgical alternative to standard tension-free hernia repair for inguinal hernias. Compared with the transabdominal preperitoneal technique, the TEP technique has an advantage that it does not penetrate the peritoneum, and hence the risk of visceral injury, intestinal obstruction, and port-site hernia can be avoided. Therefore, most surgeons have started to prefer TEP hernia repair despite the steep learning curve.
Since SPLS, a minimally invasive technique to maximize the benefits of laparoscopic surgery, was introduced in 1992 for use in appendectomy surgeries, 3 it has been applied in a numerous areas of surgery. In inguinal hernia repair, in 2009, Jacob et al. 8 reported the first successful single-incision TEP inguinal hernia repair. Recently, several comparative studies using the conventional laparoscopic TEP hernia repair have been reported.9–12
Since April 2009, the St. Mary's Hospital in Daejeon has incorporated SPLS, starting with its application in appendectomies and subsequently widening its field of application as we became familiar with the technique. Nowadays, the SPLS technique is applied in almost all surgeries that can be performed with conventional laparoscopic surgery. However, for inguinal hernia, mainly open hernioplasty and conventional laparoscopic TEP repair were being performed. The authors of this report had performed only open hernioplasty for inguinal hernia. Hence we had planned a laparoscopic TEP repair for inguinal hernia in early 2011. However, after reviewing the literature for laparoscopic hernia repair, our views changed. If the most important factor responsible for the steep learning curve of TEP repair was the different and unfamiliar anatomical approach and a smaller surgical working space, we supposed that there may be a few differences in the difficulties during the initial experiences whether we used a multiport approach or a single-port approach. We postulated that a surgeon who has already mastered the SPLS technique as effectively as the multiport technique may be able to achieve similar surgical outcomes, even though the surgeon had started using the SPLS technique initially without having any experience of the conventional TEP operation. After the aforementioned preparation, the authors initiated the use of SPLS for TEP hernia repair.
As expected, the biggest difficulties in the initial SPLS TEP hernia repairs were the peculiarity of the anatomy and the limited surgical working space, especially the limited extent of the vertical movement. As experience and familiarity with the technique increased, procedures in the limited surgical field were able to coordinate with the laparoscopic assistant and could be performed more easily. In particular, as other authors have found that a change in the dissection technique was important, an inward/downward movement was useful for retraction and dissection instead of limited upward/downward movement. 13 Also, in the middle of the study, there was a change in the equipment. In the latter 30 cases, we used the laparoscope with a long shaft (Stryker, San Jose, CA), a right-angle light cable connector (Stryker), and a 5-mm tree trocar (Fig. 3). These small changes were helpful to decrease friction among the laparoscope, instruments, and the trocar during the procedure. We used a home-made glove port and the conventional straight and rigid instrument in all of the patients because the home-made glove port has the advantage of freedom of movement through a single incision as the crossing point, and a flexible-tip laparoscope and roticular instruments have disadvantages due to their inadvertent movement and weak retraction strength, based on our experiences with SPLS. We did not use a balloon dissector, which resulted in cost reduction and avoidance of risk for balloon trocar injury. 14
The glove port used in the latter 30 cases. An extralong laparoscope, right angle adapter, and three 5-mm trocars were utilized.
In this study, we did not analyze the cost of single-port TEP compared with that of conventional TEP. However, when other conditions were the same (e.g., duration of hospital stay or amounts/types of medication), single-port TEP helped in saving as much as $110, which was the difference between the cost of a balloon dissector plus two 5-mm trocars (conventional TEP) and that of three 5-mm mini trocars plus a wound retractor (single-port TEP). Except for the difference in the cost-effectiveness, the materials and methods used are the same in both the techniques.
We reviewed the reports of prior studies on the initial experience of SPLS TEP inguinal hernia repair, which enrolled more than 30 patients, and a comparison of the results is given in Table 3. There was an increase in the surgical time with SPLS TEP hernia repair compared with that in the other prior reports.
ADL, activities of daily life; NA, not available; TAPP, transabdominal preperitoneal; TEP, totally extraperitoneal.
Although there has been a trend for a long operative time in bilateral inguinal hernia repair, we usually used the same skin and fascial incision to perform bilateral hernia repair. When we created a contralateral preperitoneal space through dissection with two instruments, after completing the inguinal hernia repair on one side, we found it a little difficult and time consuming to perform hernia repair on the other side. Hence, we used a balloon dissector for bilateral hernia repair in the latter 7 cases, and it was quite useful in reducing the effort of dissection and operation time. The incision length and the length of hospital stay were comparable with those in the other studies on SPLS TEP repair. We also examined the postoperative pain and time for return to normal activities as valuable assessments of postoperative outcomes. Among the studies that we reviewed in the literature, only one study assessed the VAS score for postoperative pain 13 : the VAS score was 2.26 (range, 0–4) on postoperative Day 1 and 0.83 (range, 0–2) on postoperative Day 7. Langeveld et al. 2 reported that the VAS score was 3–3.5 on postoperative Day 1 and 1–1.5 on postoperative Day 7 following conventional TEP repair. Our results demonstrated no increase in the VAS score compared with that in these results. Our study also demonstrated a good postoperative recovery and return to normal activities. Our series showed that 82.1% of the patients returned to normal activities within 7 days, and the mean time to return to ADL was 4.8 days. Similar to that in other SPLS studies, a vertical incision over the umbilicus showed excellent cosmetic benefits (Fig. 4).
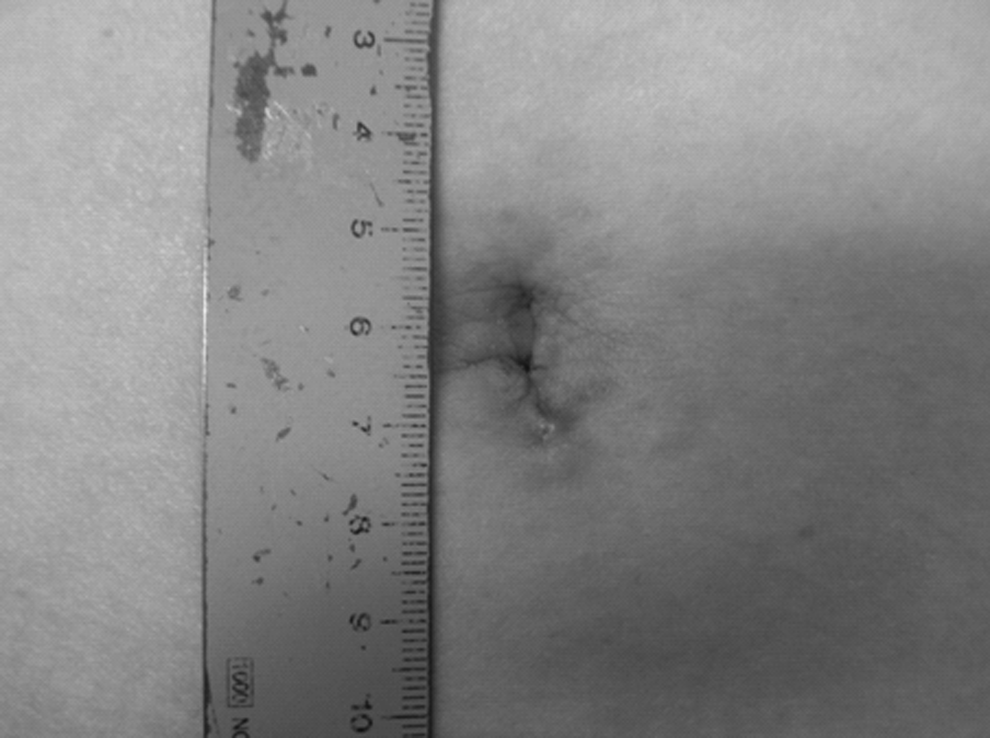
The postoperative scar 1 week after single-port totally extraperitoneal inguinal hernia repair.
In our current study, we focused on the results for the operation time and perioperative complications to evaluate the safety and feasibility of this technique. The SPLS TEP inguinal hernia repair was successful in all patients except in 1 patient, in whom an additional trocar was inserted in the suprapubic area because of a large peritoneal tear. There were no major postoperative complications. However, the intraoperative complication rate (including minor events) was relatively high (23%), and, as mentioned above, the operation time was longer. Based on this experience, we have some considerations. It would be better to exclude those patients with recurrent inguinal hernia and those with an operative scar in the surgical field until the operator is fully familiar with this technique. In addition, appropriate adjustment of the equipment can increase the feasibility of SPLS TEP repair by reducing collision. A shorter operative time in the latter 30 cases of our series might be related to the use of a laparoscope with a long shaft and angled light cable connector. For bilateral inguinal hernia repair, to create a large cavity, the utilization of a balloon dissector might be considered. Another important point is to pay attention while performing dissection in the preperitoneal space to avoid peritoneal tear. Peritoneal tear was reported as the most common reason for conversion following conventional TEP repair. 15
We acknowledge that this study has several limitations, including a lack of long-term and functional outcomes and a retrospective review of the prospectively collected data. Furthermore, the absence of a control arm and the proficiency of the SPLS operator could be the other limitations of this study.
In conclusion, in the hands of an experienced SPLS surgeon, the transition from standard hernioplasty to SPLS TEP inguinal hernia repair has been feasible. However, the safety is relative, and a learning curve is necessary. But with careful selection of cases and appropriate protocol and equipment preparation, we believe that the operation time can be shortened acceptably. The technique warrants further investigation, and there is a need to perform prospective comparative studies.
Footnotes
Disclosure Statement
No competing financial interests exist.