
Abstract
Abstract
Background:
Large common bile duct (CBD) stones remain a major challenge for endoscopists. The capture of large CBD stones is a limiting factor for successful removal. The aim of the study is to evaluate the efficacy and safety of stretching the basket out at the bottom of the stones to capture large CBD stones.
Patients and Methods:
Sixty-five patients with large stones (>20 mm in diameter) were selected and randomly divided into Group A (33 cases) and Group B (34 cases). After appropriate sphincterotomy with balloon dilation, two different methods were used to capture stones. For Method A, the basket was inserted above a large stone and opened to capture it. For Method B, the basket was stretched out at the bottom of the large stone and opened slowly to capture it.
Results:
The success rate of capturing stones was 33.3% in Group A and 94.1% in Group B (P<.05). There was no statistically significant difference in complication rate between the two groups (P>.05).
Conclusions:
The success rate for capturing large CBD stones can be increased by stretching the basket out at the bottom of the stones to capture the stone.
Introduction
E
Patients and Methods
Patients
Between August 2008 and October 2012, 67 patients with large CBD stones managed by endoscopic sphincterotomy combined with balloon dilation by one physician were evaluated. This physician was experienced in the technique of endoscopic retrograde cholangiopancreatography (ERCP). Demographic and clinical characteristics of the study patients are presented in Table 1. A large stone was defined as one in which the diameter is >20 mm (referring to the maximum diameter measured by magnetic resonance cholangiopancreatography [MRCP]). All patients with a large stone at least ≥20 mm in diameter were enrolled in the study.
Data are number (range) or number as indicated.
F, female; M, male.
The exclusion criteria for this study were as follows: (1) bleeding tendency with an international normalized ratio of >1.5; (2) platelet count <50,000/mL; (3) stone size ≤20 mm; (4) acute cholecystitis; (5) intrahepatic duct stones; (6) pancreatobiliary malignancy; or (7) surgical history that can alter the papillary location.
Methods
ERCP was performed in 531 patients with CBD stones shown by MRCP; 67 of these patients had a maximum stone diameter of ≥20 mm. The study was designed as a prospective, randomized with crossover, observational clinical trial. Patients were randomized to undergo either Method A (Group A) or Method B (Group B), using a table of random numbers. A resident doctor assigned a number from the table to each patient entering the study. Patients given an odd number received Method A, and patients given an even number received Method B. For Method A (33 cases), the basket was inserted above the large stones, opened, and moved up and down. 20 For Method B (34 cases), the basket was stretched out from the bottom of the stones and opened slowly, upward from below. Patients who failed to have the common duct cleared of stones with Method A were reassigned to treatment with Method B. The study was approved by our institutional ethical review. All patients provided written informed consent before entering the study.
We made an incision to the midportion of the papilla with a pull-type sphincterotome and then inserted a balloon (20 mm in diameter; Wilson-Cook Medical, Winston-Salem, NC) over a guide wire. Balloon dilation was performed using wire-guided hydrostatic balloon catheters placed across the papilla (Fig. 1A and B). Using Method B, for single stones, the basket was stretched out from the bottom and pushed up to trap the stone. For multiple stones and permeated stones, insertion of the basket into the proximal CBD was avoided. As shown in Figure 2, the basket was stretched out from the distal CBD and opened slowly. During this process, the endoscope should be rotated counterclockwise repeatedly in order to push the opened basket to trap the stones. After the stones were trapped in the basket, they were extracted from the biliary tract (Fig. 1C). In cases where the stone could not be extracted from the biliary tract, the Teflon® (Dupont, Wilmington, DE) sheath of the basket was replaced with a metal sheath, and mechanical lithotripsy (Endo-Flex®, Voerde, Germany) was performed to fragment the stones. After the fragmented stones in the distal CBD were removed (Fig. 1D), the stones remaining in the proximal CBD were captured and crushed using Method B again. When the stones in the proximal CBD were captured, mechanical lithotripsy was carried out, and the lithotripsy basket was withdrawn. If the bile duct stones were retrievable, their composition was analyzed by sonography or computed tomography of the abdomen using a method described by Tsai et al. 21 The stones were classified as cholesterol or bilirubinate stones according to the predominant composition. The success rate of the first method used was recorded for this trial.
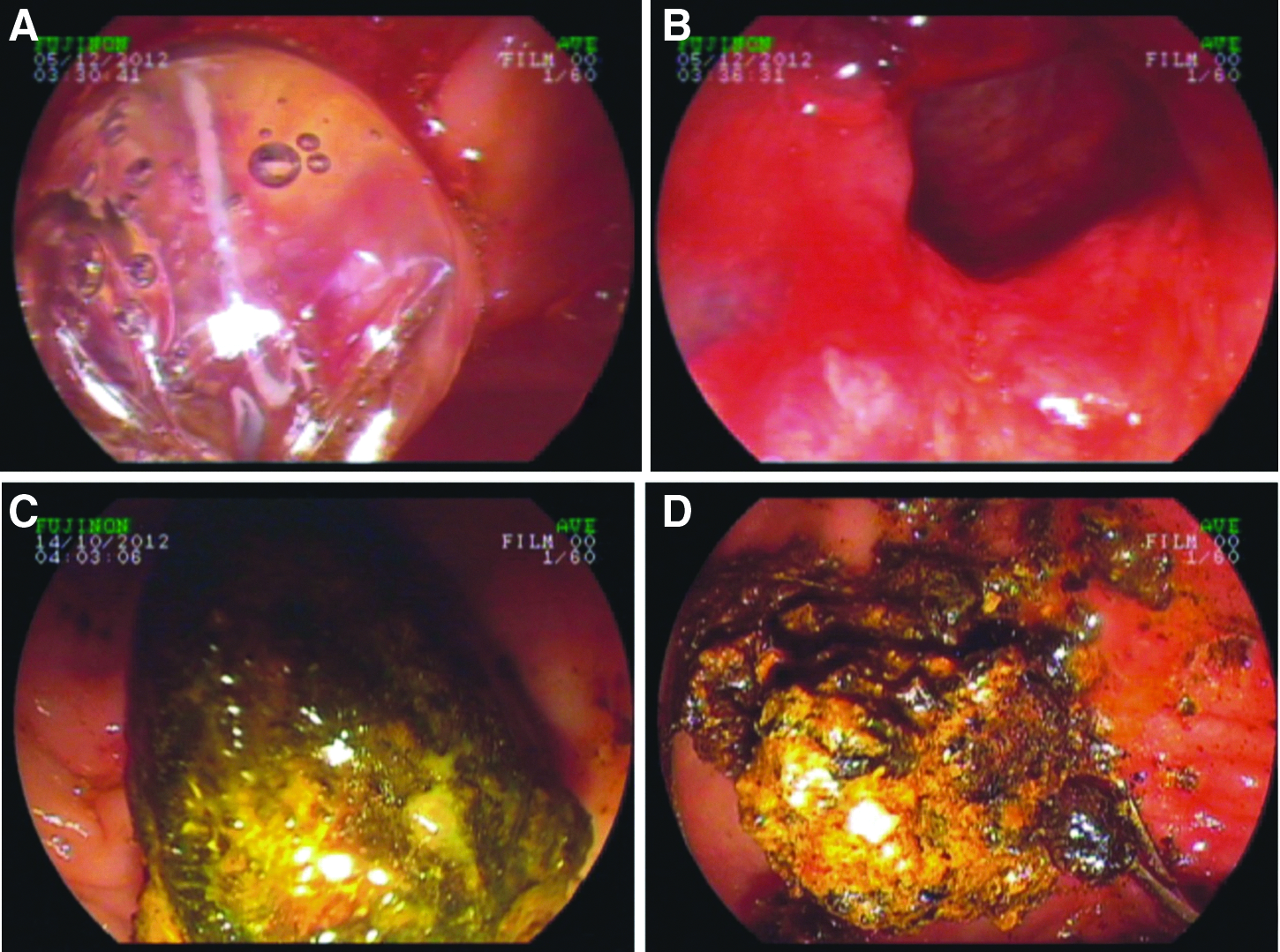
Endoscopic view.
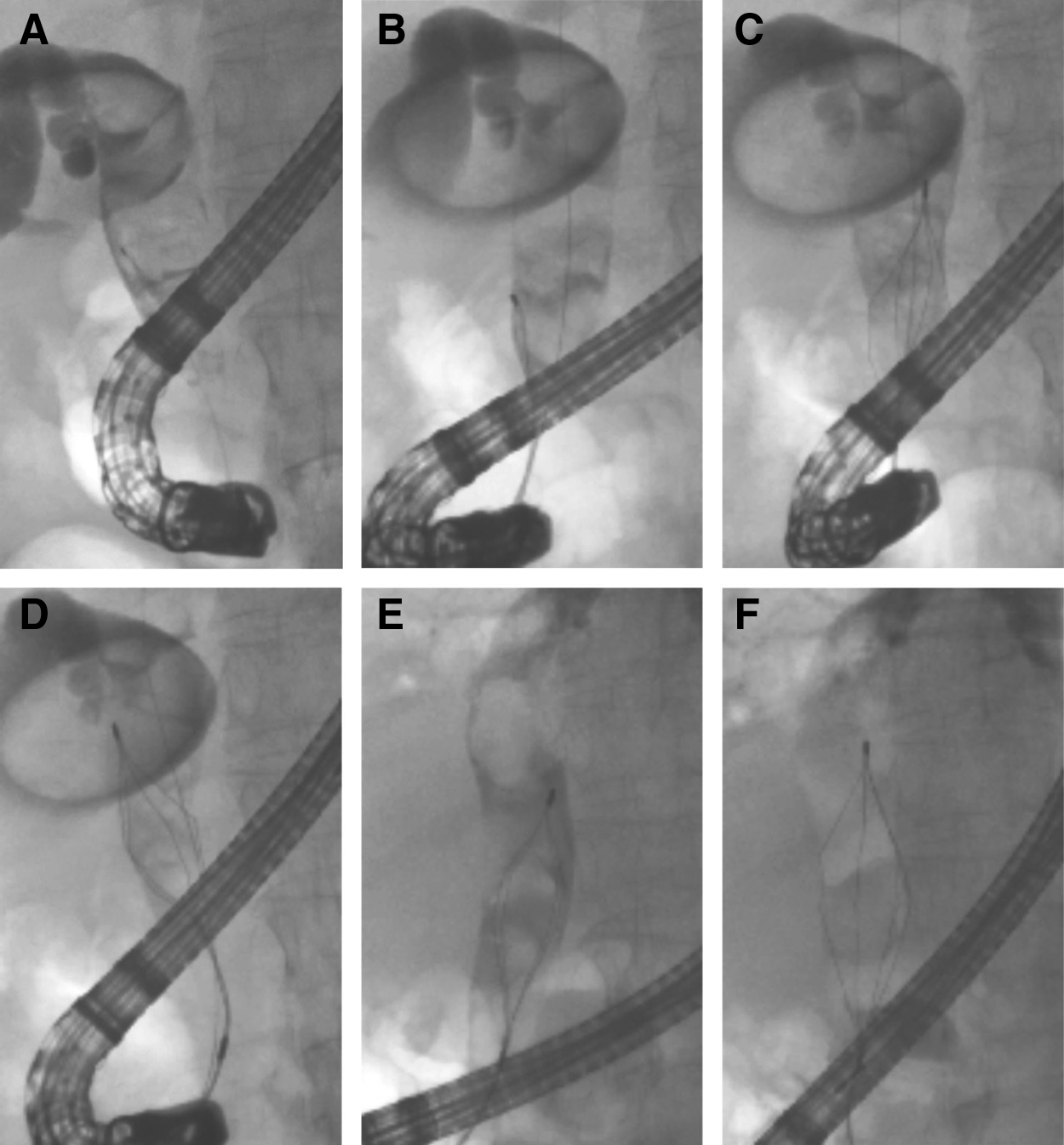
Fluoroscopic images of Method B.
Statistical analysis
Statistical analysis was performed using SPSS version 11.0 software (SPSS, Inc., Chicago, IL). All continuous variables were compared using multivariate analysis. The discrete variables were compared using the chi-squared test. A value of P<.05 was regarded as indicating a statistically significant difference.
Results
Of the 531 patients with CBD stonesindicated by MRCP, 466 patients were excluded, and 67 patients were included. In Group A, 11 cases were captured successfully with Method A, and the success rate was 33.3%. In Group B, 32 cases were captured successfully with Method B. Thus the success rate of Method B in Group B was 94.1%. Based on this success rate, Method B again was adopted to treat failed cases in Group A, and 21 cases were captured successfully. There was one failure cannulation in each group, respectively. The overall of Method B in the two groups was 96.4%. There was a significant difference in the success rate of capturing stones between the two groups (P<.05). The 7 cases with impacted large stones in the two groups were successfully captured using Method B. All stones successfully captured were directly removed (25 cases) (Fig. 1C) or removed after mechanical lithotripsy (38 cases) (Fig. 1D). A second procedure to achieve complete clearance was used in 12 patients in Group A and 13 patients in Group B. After ERCP, 7 patients had mild pancreatitis, and 2 patients had mild bleeding, returning to normal after conservative treatment. There was no significant difference between the two groups for major complications, such as pancreatitis, perforations, or hemorrhages (P>.05). The success rate, composition of the stones, and complications are presented in Table 2.
Data are number of cases (percentage) or number of cases as indicated.
Discussion
The factors influencing the success rate of stone clearance have drawn considerable attention.10,22 Several reports indicate that large stones could also be successfully captured and crushed.5,8,9,19 However, very large stones often make mechanical lithotripsy cumbersome or even impossible. 23 There have also been numerous reports about the failure to capture large stones.4,8,10,12,24,25 Cipolletta et al. 22 reported that mechanical lithotripsy failed in 16.0% of patients with large stones, which was primarily due to inability to capture the stone within the basket. Kim et al. 2 also reported similar results. The primary reason reported for the failure is insufficient space in the CBD to properly open the basket to capture the stone despite the fact that the basket wires may slip around the stone.26–28 Unfortunately, these reports did not mention if the failure in the capture of large stones correlated with the capture method. We believe that failure to capture large stones is likely to be associated with the method used. In the present study, the success rate of capturing stones was compared between two methods. Our findings demonstrated that the success rate of Method B was significantly higher than with Method A. As described above for Method B, the basket was stretched out from the bottom of the distal CBD and pushed up to engage the stone, which was different from Method A, in which the basket is inserted above the stone and pulled down in order to capture it. The high success rate of this new method could be explained by the empty distal CBD when the stones in the distal CBD are moved up to facilitate opening the basket. Moreover, when the basket encounters resistance from the proximal CBD, it is more easily opened because of driving force from below. Ten patients with stones >3 cm (the largest was 4.8×3.1 cm) (Fig. 3) were successfully captured. In our study, the proportion of bilirubinate stones was 87.9% in Group A and 91.2% in Group B, which might have a small influence on the success rates of the two methods. However, the key factor for the successful removal of larger stones is the ability to capture the stones. Our findings indicate that Method B is more successful for the removal of these large stones.
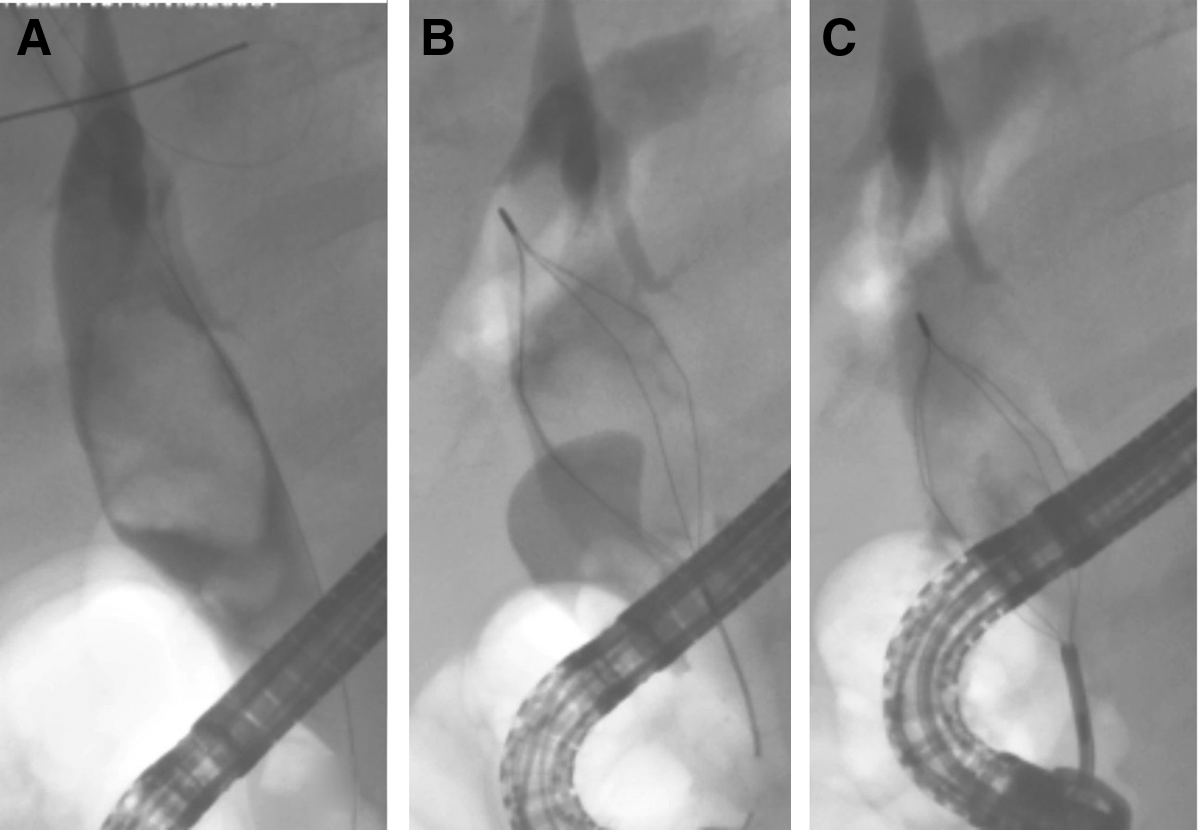
Fluoroscopic images of capturing and crushing a large stone (4.8×3.1 mm) with Method B.
Method B was used to relieve the stone blockage because after the injection of contrast media, pushing the basket can loosen impacted stones. This was different from previously reported methods.13,23,29 The impacted large stone in 7 cases in our study was successfully captured using this method.
When findings are taken together, Method B was clearly the method of choice for the management of large CBD stones. Future studies in a large cohort of patients should be performed to confirm our findings.
Footnotes
Disclosure Statement
No competing financial interests exist.