
Abstract
Abstract
Background:
Laparoscopic surgery has been associated with a perioperative decrease in renal function. As a result, an open approach may be preferred in patients with impaired renal function when prolonged laparoscopic procedures are anticipated. The aim of this study was to examine changes in renal function following colorectal operations and compare between the open and the laparoscopic approaches, in patients with preoperative impaired renal function.
Patients and Methods:
This is a single-center retrospective study. Records of all patients with impaired renal function (estimated glomerular filtration rate [eGFR] <60 mL/minute) who underwent elective colorectal resection between 2007 and 2011 were reviewed. The changes in eGFR were examined and compared between open and laparoscopic procedures.
Results:
Ninety consecutive patients with impaired renal function who underwent elective colorectal surgery from 2007 to 2011 were identified. Forty-seven patients underwent laparoscopic surgery, and 43 had an open surgery; 23.2% of the patients who had open surgery and 21.7% of the patients who underwent a laparoscopic procedure demonstrated a decrease in eGFR at the time of discharge (P=not significant). The mean decrease in eGFR did not differ between the two groups (6.3±6.8 mL/minute versus 4.04±4.01 mL/minute; P=.34). None of the patients required dialysis. Postoperative complications were found to be a risk factor for a significant decrease in renal function.
Conclusions:
Renal function may deteriorate in patients with chronic kidney disease who undergo elective colorectal surgery. No difference was noted in the incidence or severity of such deterioration between open and laparoscopic approaches. Postoperative complications are associated with deterioration in renal function regardless of the operative approach.
Introduction
D
Although studies have failed to demonstrate any adverse renal complications after laparoscopy in patients with normal preoperative renal function, 7 pneumoperitoneum may lead to clinically significant deterioration in renal function in patients with chronic kidney disease (CKD) or in patients with risk factors such as diabetes or hypertension.3,4 Decreased renal function was found to correlate with the level of pneumoperitoneal pressure and the length of the operation.1,5–7
The deterioration of renal function is mainly transient and resolves during the early postoperative period,8,9 without permanent damage to the tubular cells secondary to ischemia.5,9–11
Chronic renal failure is not a contraindication to laparoscopy, but the possibility of acute or chronic renal failure in this setting could affect the choice of approach for colorectal surgery in these patients.1,2
We set out to examine changes in enhanced glomerular filtration rate (eGFR) following colorectal surgery in patients with CKD comparing the open versus the laparoscopic approach.
Patients and Methods
This is an Institutional Review Board–approved retrospective analysis of all patients with impaired renal function who underwent elective colorectal resection for any indication at the Sourasky Medical Center (Tel Aviv, Israel) from 2007 to 2011.
The surgical approach (open versus laparoscopy) was dictated by surgeon preference. During this time interval, our center had two surgical services that differed in their approach: one service offered mainly an open approach to patients with previously impaired renal function, whereas the other offered mainly laparoscopy for similar patients.
Patients undergoing right-sided resections had no bowel preparation, whereas patients undergoing left-sided resections underwent bowel preparation with polyethylene glycol.
Our cutoff for CKD was based on a calculated eGFR of <60 mL/minute, according to the 4-variables equation from the Modification of Diet in Renal Disease. 12 Normal renal function patients and patients with end-stage renal failure who were on dialysis were excluded, as were any nonelective cases.
The preoperative calculated eGFR was based on laboratory tests that were completed in the range of a few days prior to surgery, whereas the postoperative eGFR was measured 1–2 days prior to discharge.
Clinical data were retrieved from computerized and archived patient medical records.
Data were collected for age, gender, indications for and type of surgery, Charlson Comorbidity Index, 13 operative time, length of hospital stay, eGFR prior to surgery, and eGFR before discharge. Patients who had an open procedure were compared with those who underwent laparoscopy.
Average baseline eGFR prior to surgery was compared with the average postoperative eGFR prior to discharge. The change in postoperative eGFR compared with the preoperative one was also calculated for each patient, and these values were compared between the open and laparoscopic groups.
Statistical analysis
Statistical analysis was performed using the chi-squared, t, and the Mann–Whitney nonparametric tests. P values of <.05 were considered statistically significant.
Results
Of the 996 patients who underwent colorectal resections in this time period in both services, in total, 90 patients met our inclusion criteria for CKD and elective surgery. Forty-seven underwent laparoscopic resection, whereas 43 underwent an open procedure. The open approach group included more males and more cancer patients (Table 1). One patient from the open group died following the operation. She developed sepsis a few days following the operation with no obvious septic source. She was treated supportively in the intensive care unit; however, she has developed multi-organ failure and died 3 weeks after surgery.
CCI, Charlson Comorbidity Index.
Complications were graded as minor (Grades 1 and 2) and major (Grades 3–5) based on the Clavien–Dindo classification 14 and were compared between the two groups. The rates of major complications were similar in both groups. Minor complications were more prevalent in the open group. This and other perioperative parameters are presented in Table 1.
The average preoperative eGFR was similar in both groups (46.77±9.83 mL/minute in the open and 44.7±9.8 mL/minute in the laparoscopic group; P=not significant). An increase in eGFR following surgery (prior to discharge) occurred in 76.8% of patients in the open group and 78.3% in the laparoscopic group (P=not significant), whereas 23.2% and 21.7%, respectively, experienced a decrease in eGFR (P=not significant) (Fig. 1).
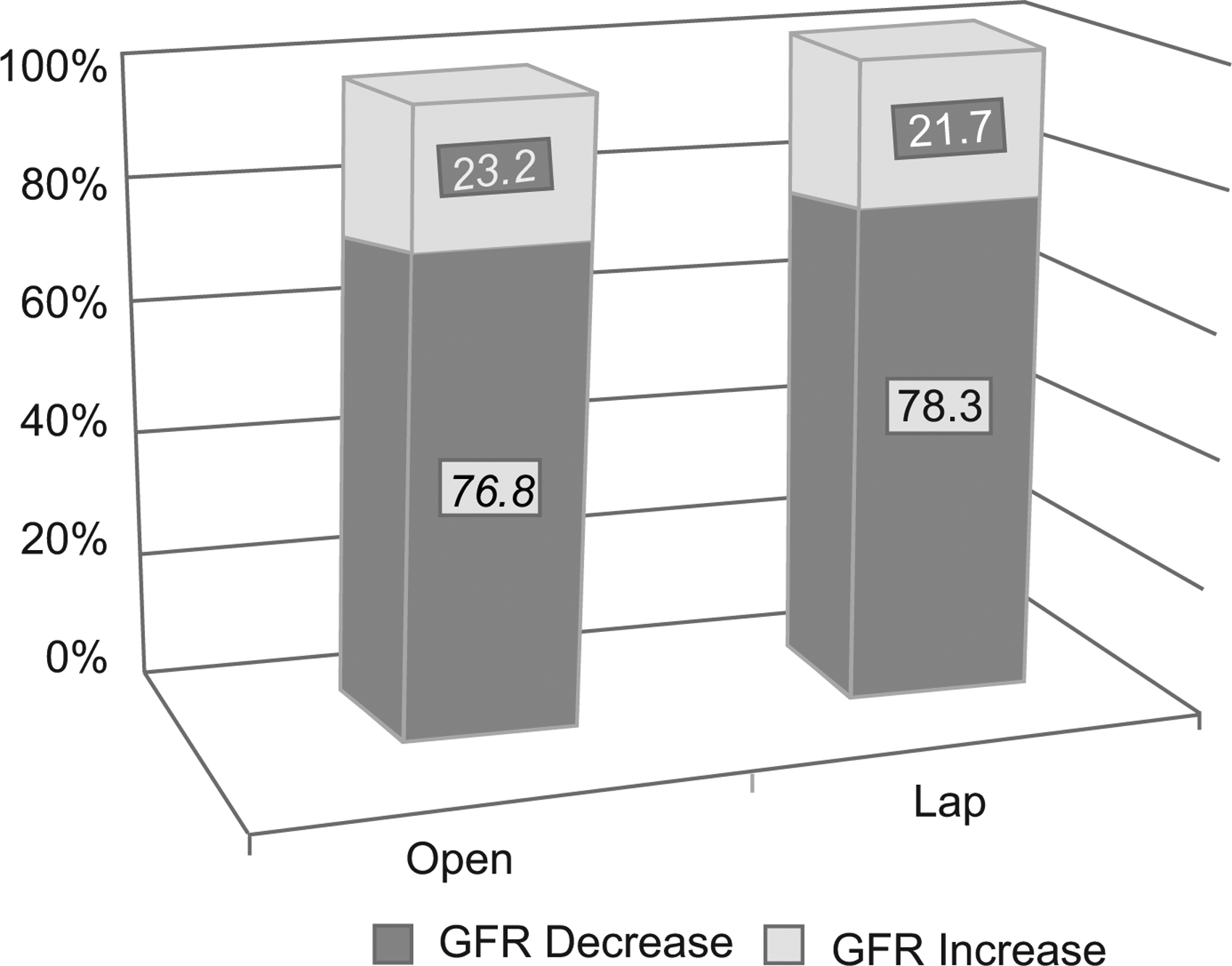
A comparison of the change (increase/decrease) of enhanced glomerular filtration rate (GFR) prior to patients' discharge between the two groups. Lap, laparoscopic.
The levels of changes in eGFR (increase and decrease) were similar between the two groups (Table 2). None of the patients required any form of postoperative dialysis.
eGFR, enhanced glomerular filtration rate.
Several possible risk factors for a significant eGFR decrease (a decrease of >4 mL/minute) were evaluated and are listed in Table 3. In a multivariate analysis, the presence of postoperative complications (any type or grade) was the only statistically significant risk factor for a significant decrease in eGFR.
Decrease of >4 mL/minute.
Indicates a significant difference.
CCI, Charlson Comorbidity Index; eGFR, enhanced glomerular filtration rate.
Discussion
Published reports do not provide a definitive answer as to whether a laparoscopic approach to colorectal surgery is safe for patients with impaired renal function, compared with an open approach. Clinical studies on the impact of laparoscopy on renal function are characterized by a small number of relatively young patients and exclusion of patients with significant comorbidities or with impaired renal function.6,9,10,15
In this study we evaluated and compared changes in renal function specifically in patients who had preoperative CKD and who underwent open or laparoscopic colorectal procedures. Our results demonstrated similar changes in renal function in patients who underwent open versus laparoscopic procedures. In most patients, eGFR increased after surgery. This may be attributed to a possible element of preoperative dehydration as a result of an underlying disease and to the intraoperative and postoperative fluid resuscitation.
Several studies have compared different aspects of renal function between a standard laparoscopic approach and low-pressure
9
or retractor-assisted6,9 laparoscopy, in otherwise healthy individuals. These studies have shown a temporary reduction in renal blood flow, intraoperative urine output, and glomerular filtration rate in patients undergoing laparoscopy. However, no long-term impact following the operation was noted. One study
6
has also shown that the level of N-acetyl-beta-
Nguyen et al. 17 randomally assigned 104 patients to undergo laparoscopic or open gastric bypass surgery and evaluated their intraoperative urine output; patients with chronic renal failure were excluded. Their results showed that prolonged pneumoperitoneum significantly reduced intraoperative urine output but, again, did not adversely alter postoperative renal function.
A retrospective evaluation of 1800 patients undergoing laparoscopic gastric bypass was analyzed by Sharma et al. 11 Of the 1800 patients, they detected 42 patients (2.3%) who developed postoperative acute renal failure. Dialysis was required in 6 patients, 2 of whom became dialysis dependent. Acute renal failure was completely resolved in the remaining patients. Patients with a body mass index of >50 kg/m2, previous chronic renal failure, and prolonged operative times and intraoperative hypotension were at the greatest risk of postoperative renal failure. However, no comparison with the open approach was performed, and thus the laparoscopic approach for itself could not be evaluated as a possible factor affecting renal function outcome.
A method for decreasing the negative intraoperative impact of prolonged pneumoperitoneum on renal function was suggested in several studies.18,19 These studies demonstrated that intraoperative infusion of low-dose dopamine to patients undergoing laparoscopic colorectal procedures prevents a decrease in urinary output and creatinine clearance, compared with a control group in otherwise healthy people.
A recent study demonstrated that laparoscopy was associated with a reduction in postoperative morbidity in patients undergoing major bowel resection; however, this study was specifically related to dialysis-depenedent patients. 20
Our study is unique and different from other reports as it was specifically designed to evaluate the potential postoperative effect of the laparoscopic approach compared with an open approach solely in patients with previously impaired renal function but not on dialysis. Additionally, we have focused on pre- and postoperative (prior to discharge) renal function, regardless of temprary changes that might have occurred during or in the immediate postoperative period.
It is important to note that regardless of the operative approach, a bowel preparation in and of itself may have an effect on renal function, Nevertheless, the polyethylene glycol that was used in our patients for left-sided resections is considered to be safer than other preparations in patients with preexisting renal disease. 21 Our study size did not allow for further stratification to examine this.
The limitations of our study are related to the fact that the two groups were not similar in all parameters, the retrospective nature of the study, and its small population size.
Regarding sample size, in order to detect a difference of a 10% decrease in eGFR between the two groups in a one-tailed statistical test, assuming an alpha level of 0.05, with a statistical power of 90%, 290 patients are required in each group. To detect smaller differences, the study population needs to be even larger.
Nevertheless, it is difficult to identify such a large number of patients with CKD undergoing laproscopic or open colectomy in a single center.
We believe that despite the mentioned limitations the importance of this study arises from the actual comparison between the two surgical approaches and the similiarity in renal function outcome in both groups. Additionally, a multivariate analysis of all parameters, including the surgical approach, has demonstrated that the only risk factor associated with a significant decrease in eGFR was the development of postoperative complications regardless of the complications' grade.
In conclusion, eGFR may decrease in some patients with chronic renal failure who undergo elective colorectal procedures. A significant decline in eGFR is associated with postoperative complications. No difference was found in the incidence and severity of this decline between open and laparoscopic procedures.
Laparoscopic colectomy can be safely offered to patients with preoperative CKD while ensuring adequate fluid balance and preventing of postoperative complications.
Disclosure Statement
No competing financial interests exist.