
Abstract
Abstract
Background:
For small renal masses (SRMs), open partial nephrectomy represents the therapeutic standard of care, and laparoscopic partial nephrectomy (LPN) has provided encouraging outcomes. Laparoscopic renal cryoablation (LRC) could be regarded as an alternative to surgical excision in selected patients, if perioperative complication rates and oncologic results are comparable. However, the short- and long-term outcomes of LRC versus LPN have not been adequately assessed. This study evaluated the safety and efficacy of LRC compared with LPN in the treatment of SRMs.
Materials and Methods:
A systematic search of the Medline, Scopus, and CNKI databases and the Cochrane Library was performed up to October 1, 2013. Outcomes of interest assessing the two techniques included demographic and clinical baseline characteristics, surgical and oncological variables, renal function, and complications.
Results:
Nine eligible trials (555 cases and 642 controls) assessing LRC versus LPN were identified, including two prospective and seven retrospective studies. Patients undergoing LRC were significantly older (weighted mean difference [WMD], 6.48 years; 95% confidence interval [CI], 3.12–9.83; P<.001) and had a higher solitary kidney rate (odds ratio [OR]=3.76; 95% CI, 2.05–6.92; P<.001). Although LRC was associated with shorter operative time (WMD, −54.28 minutes; 95% CI, −83.79 to −24.78; P<.001), less blood loss (WMD, −111.75 mL; 95% CI, −147.96 to −75.53; P<.001), lower risk of conversion (OR=0.17; 95% CI, 0.05–0.60; P=.005), and fewer overall complications (OR=0.53; 95% CI, 0.29–0.98; P=.04), especially the rate of intraoperative complications (OR=0.20; 95% CI, 0.07–0.58; P=.003) and major complications (OR=0.45; 95% CI, 0.25–0.81; P=.008), patients having LPN might still benefit from a significantly lower local recurrence rate (OR=13.03; 95% CI, 4.20–40.39; P<.001) and lower distant metastasis rate (OR=9.05; 95% CI, 2.31–35.51; P=.002).
Conclusions:
Compared with LPN, LRC was associated with reliable perioperative safety, comparable renal function, and fewer complications; however, LRC may still result in a higher risk of tumor progression. Therefore, our meta-analysis suggested that LRC was associated with worse oncological outcomes than LPN but that LRC may be indicated in selected patients with significant comorbidity. Because of the inherent limitations of the included studies, further large sample, prospective, multicenter, and long-term follow-up studies are awaited to corroborate these findings.
Introduction
T
Materials and Methods
Literature search and study selection
A systematic review of the literature was performed to identify articles published up to September 1, 2013 on the management of SRMs. We conducted a systematic search of the electronic databases, including Medline, Scopus, CNKI and The Cochrane Library, using the terms “laparoscopic renal cryoablation,” “laparoscopic partial nephrectomy,” and “small renal mass.” Only English language studies were included. No temporal, regional, or publication status restrictions were set. In addition, a full manual search of the references in each relevant article was also conducted.
Inclusion criteria and exclusion criteria
To be included in the analysis, studies were required (1) to compare LRC and LPN, (2) to report on at least one outcome of interest mentioned below, and (3) to clearly document indications for resection of the renal tumor. Studies were excluded in the meta-analysis if (1) the inclusion criteria were not met or (2) no outcomes of interest (specified later) were reported or were impossible to calculate or extrapolate the necessary data for either LRC or LPN from the published results.
Data extraction and outcomes of interest
Two reviewers (K.T. and W.Y) extracted independently the following data: first author, year of publication, study design, number of patients who underwent LRC and LPN, characteristics of the study population, and outcomes of interest. All disagreements about eligibility were resolved by a third reviewer (Z.Y.) by discussion until a consensus was reached. The following data were the outcomes of interest that extracted from each eligible study: operating time, estimated blood loss, length of hospital stay, blood transfusion rate, conversions rate, postoperative serum creatinine (SCr) increase, postoperative glomerular filtration rate (GFR) decrease, catheterization time, local recurrence, distant metastasis, and the overall complications, including both intraoperative and postoperative minor and major complications.
Study quality and level of evidence
The level of evidence of included studies was rated according to criteria by the Centre for Evidence-Based Medicine in Oxford, United Kingdom. 15 Two reviewers (K.T. and W.Y.) independently assessed the quality of the studies, and disagreement was resolved by consensus.
Statistical analysis
The present meta-analysis was performed according to the recommendations of the Cochrane Collaboration and the Quality of Reporting of Meta-analyses (QUORUM) guidelines. 16 The weighted mean differences (WMDs) and the odds ratios (ORs) were used to compare continuous and dichotomous variables, respectively. All outcomes were reported with 95% confidence intervals (CIs). For continuous variables, we calculated the difference in mean values and the 95% CI. This method requires that the study report the standard errors of the mean, the standard deviations, or the CIs. However, some studies that did not report any of these parameters but presented continuous data as medians and ranges; under this circumstance we made an approximate transformation using the technique described by Hozo et al. 17 For dichotomous variables derived from contingency tables, the ORs and 95% CI were computed. An OR significantly <1 favored LRC, whereas an OR significantly >1 favored LPN. All P values are two-tailed with a significant level at .05.
A fixed-effects meta-analysis was performed, and the quantity of heterogeneity was assessed using chi-squared and I 2 statistics, with significance set at P<.05 providing evidence of significant heterogeneity. For outcomes detected with higher values of I2 and the chi-squared statistic signified increasing levels of inconsistency between studies and significant interstudy heterogeneity, then a random-effects meta-analysis model was adopted. Data analysis was performed with Review Manager software (RevMan version 5.1; Cochrane Collaboration, Oxford).
Results
Characteristics of eligible studies and level of evidence
Nine studies4,7–14 assessing LRC versus LPN were considered suitable for meta-analysis, including two prospective4,10 and seven retrospective studies7–9,11–14 (Fig. 1). Unfortunately, no RCT comparing the two techniques was eligible. We used the U.S. Preventive Services Task grading system 15 to assess the quality of every study included in our meta-analysis. Among the two prospective and seven retrospective studies, four studies4,8,10,13 scored 3b, and five studies7,9,11,12,14 scored 4. Also, country, study interval, number of patients, positive margin, and follow-up times were extracted individually from each study and are listed in Table 1.
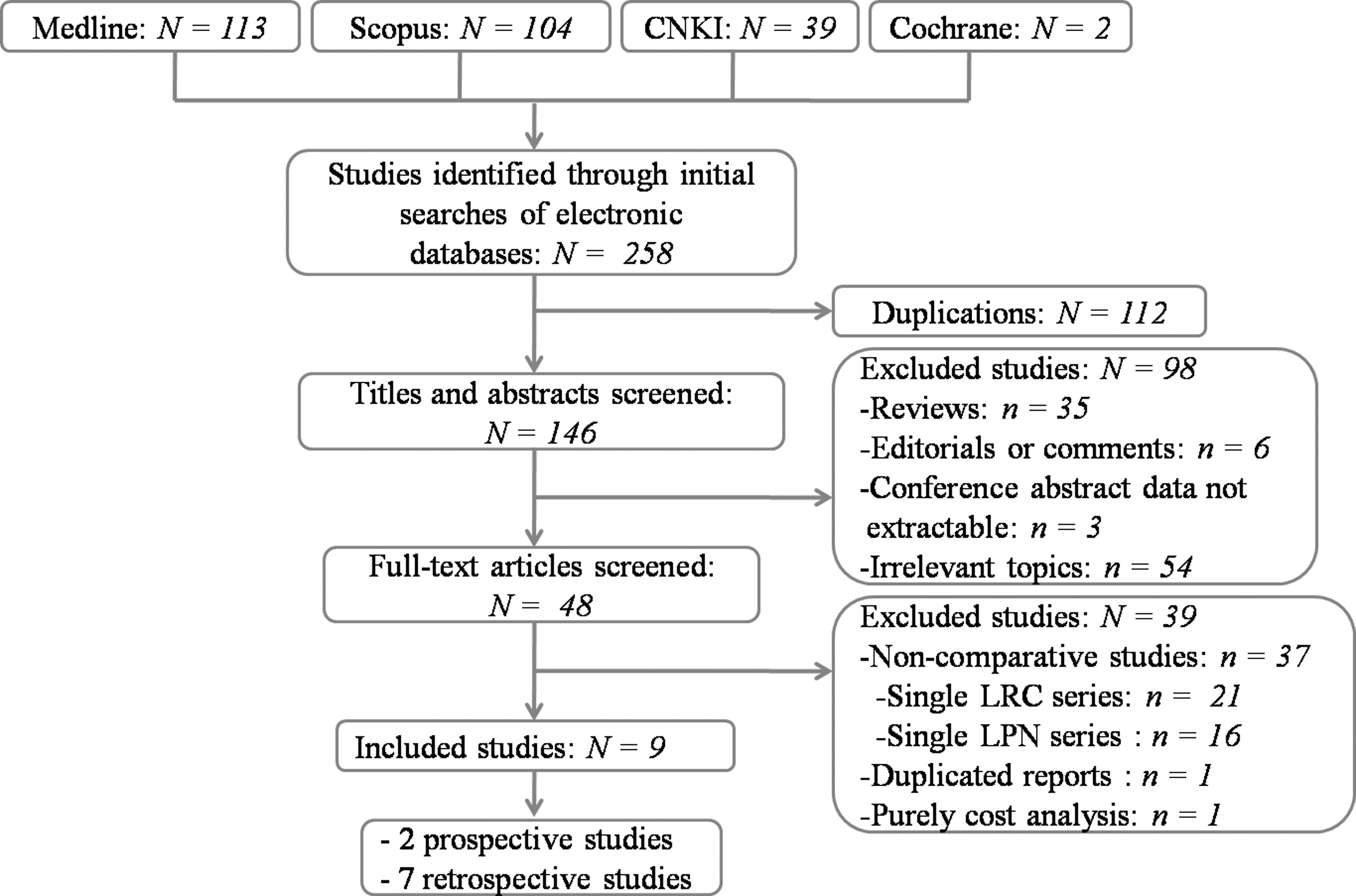
Flowchart showing the selection of studies for meta-analysis. LPN, laparoscopic partial nephrectomy; LRC, laparoscopic renal cryoablation.
Level of evidence (LOE) based on the U.S. Preventive Services Task Force grading system.
Data are mean±SD or median (range) values as indicated.
LPN, laparoscopic partial nephrectomy; LRC, laparoscopic renal cryoablation; NA, data not available.
Outcomes of demographic and clinical characteristics
Patients undergoing LRC were significantly older (WMD, 6.48 years; 95% CI, 3.12–9.83; P<.001) (Table 2) and had a higher solitary kidney rate (OR=3.76; 95% CI, 2.05–6.92; P<.001) (Table 2). There were no significant differences with respect to body mass index, American Society of Anesthesiologists score, preoperative SCr, preoperative GFR, tumor size, right-side tumor rate, and malignant tumor rate (Table 2) (all P>.05).
Statistically significant results.
Odds ratio (OR) values.
ASA, American Society of Anesthesiologists; BMI, body mass index; CI, confidence interval; GFR, glomerular filtration rate; LPN, laparoscopic partial nephrectomy; LRC, laparoscopic renal cryoablation; SCr, serum creatinine; WMD, weighted mean difference.
Outcomes of perioperative variables
Operating time and conversions rate
Pooled data from nine studies4,7–14 that reported operating time and six studies7–9,11,12,14 that reported conversion rate between LRC and LPN were examined. LRC was associated with shorter operative time (WMD, −54.28 minutes; 95% CI, −83.79 to −24.78; P<.001) (Table 3 and Supplementary Fig. S1 [Supplementary Data are available online at www.liebertonline.com/lap]) and lower conversion rate (OR=0.17; 95% CI, 0.05–0.60; P=.005) (Table 3 and Supplementary Fig. S2).
Statistically significant results.
Odds ratio (OR) values.
CI, confidence interval; EBL, estimated blood loss; GFR, glomerular filtration rate; LOS, length of hospital stay; LPN, laparoscopic partial nephrectomy; LRC, laparoscopic renal cryoablation; SCr, serum creatinine; WMD, weighted mean difference.
Estimated blood loss and blood transfusion rate
We extracted estimated blood loss from nine studies4,7–14 and blood transfusion rate from six studies.9–14 There was statistically significant less blood loss (WMD, −111.75 mL; 95% CI, −147.96 to −75.53; P<.001) (Table 3 and Supplementary Fig. S3) but similar blood transfusion rate (OR=0.56; 95% CI, 0.26–1.21; P=.14) (Table 3 and Supplementary Fig. S4) in the LRC group compared with the LPN group.
Lengths of hospital stay
Nine studies4,7–14 including 1197 patients reported on lengths of hospital stay. The pooled data showed no significant difference with regard to length of hospital stay (WMD, −0.20 days; 95% CI, −0.63 to 0.23; P=.36) (Table 3 and Supplementary Fig. S5).
Renal function
No significantly difference was observed in LRC compared with LPN regarding postoperative SCr (WMD, 0.09 mg/dL; 95% CI, −0.04 to 0.22; P=.16) (Table 3 and Supplementary Fig. S6) and SCr percentage increase (WMD, −6.77; 95% CI, −13.79 to 0.24; P=.06) (Table 3 and Supplementary Fig. S7) during the postoperative follow-up. There were no significant differences in postoperative GFR (WMD, 0.15 mL/minute/1.73 m2; 95% CI, −28.24 to 28.55; P=.99) (Table 3 and Supplementary Fig. S8) and GFR percentage decrease (WMD, −1.83; 95% CI, −7.61 to 3.96; P=.54) (Table 3 and Supplementary Fig. S9).
Outcomes of complications
Pooled data from nine studies4,7–14 including 1197 patients reported on complications. There was a statistically significant reduction in the overall complications rate in the LRC group compared with the LPN group (OR=0.53; 95% CI, 0.29–0.98; P=.04) (Table 3 and Fig. 2), and it was especially reflected in intraoperative complications (OR=0.20; 95% CI, 0.07–0.58; P=.003) (Table 3 and Fig. 3), although the postoperative complications were not significant (Supplementary Fig. S10). Figure 2 shows a forest plot for overall complications. Grouping into major and minor complications was possible for nine studies. In this subanalysis, major complications more frequently occurred following LPN (OR=0.45; 95% CI, 0.25–0.81; P=0.008) (Table 3 and Fig. 4), whereas the rate of minor complications was similar (Supplementary Fig. S11). Heterogeneity between studies was effectively decreased after this subgroup analysis of all complications compared with the overall complications.
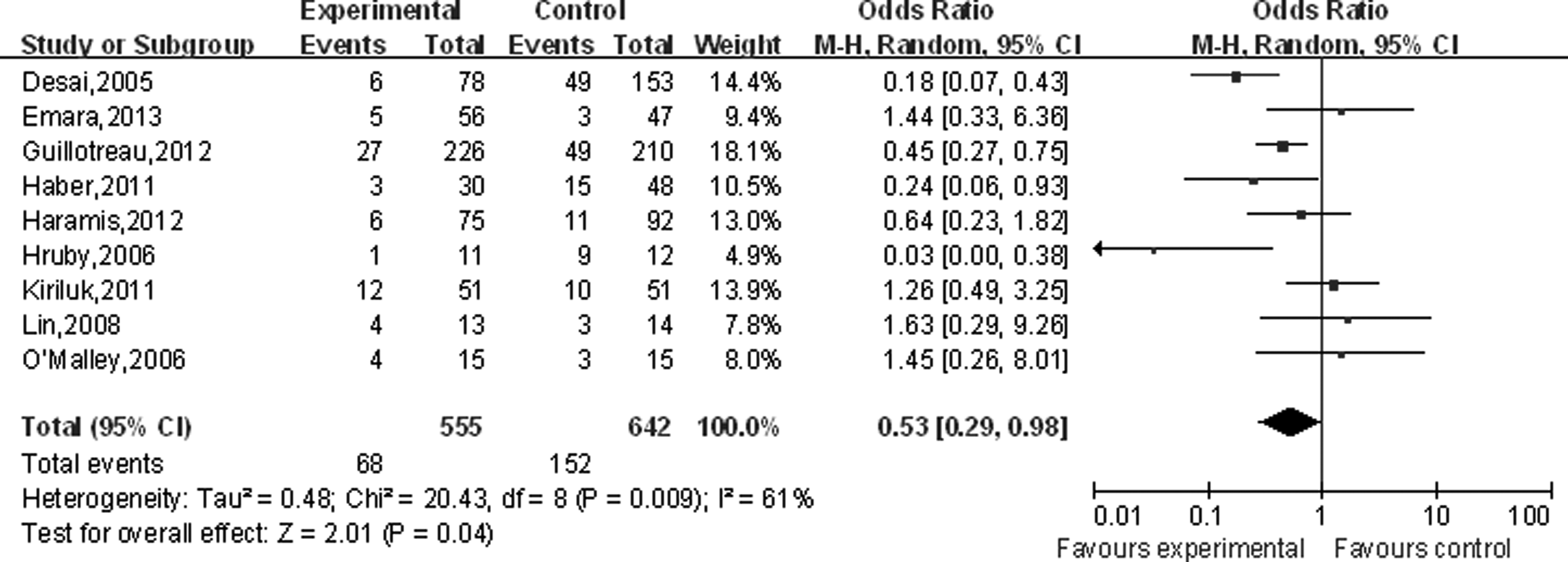
Forest plot and meta-analysis of overall complications comparing laparoscopic renal cryoablation (experimental) and laparoscopic partial nephrectomy (control). CI, confidence interval; M-H, Mantel–Haenszel test.
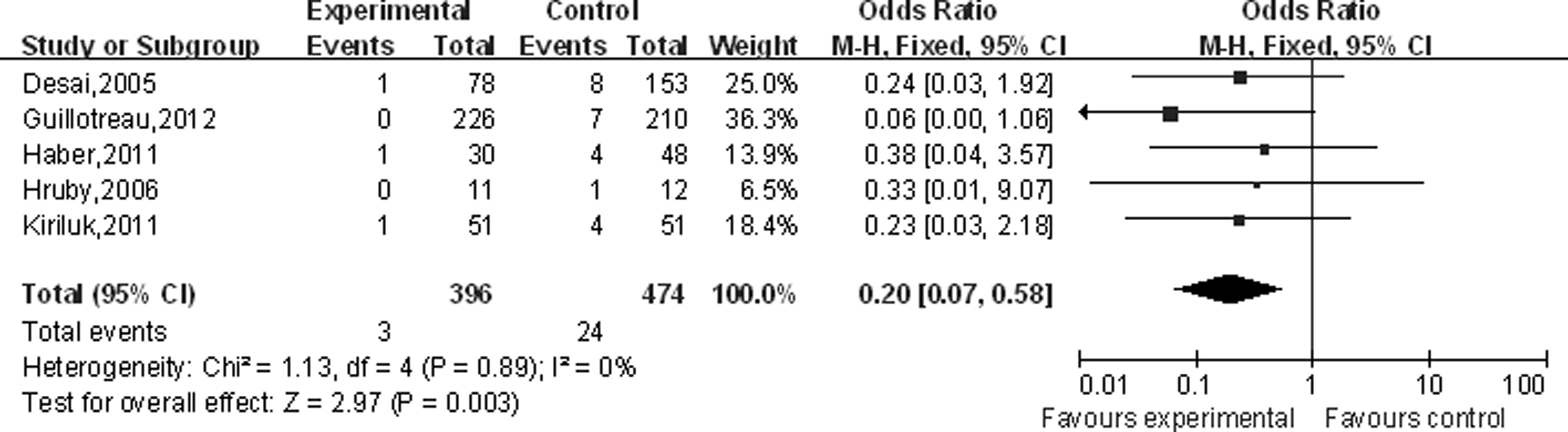
Forest plot and meta-analysis of intraoperative complications comparing laparoscopic renal cryoablation (experimental) and laparoscopic partial nephrectomy (control). CI, confidence interval; M-H, Mantel–Haenszel test.
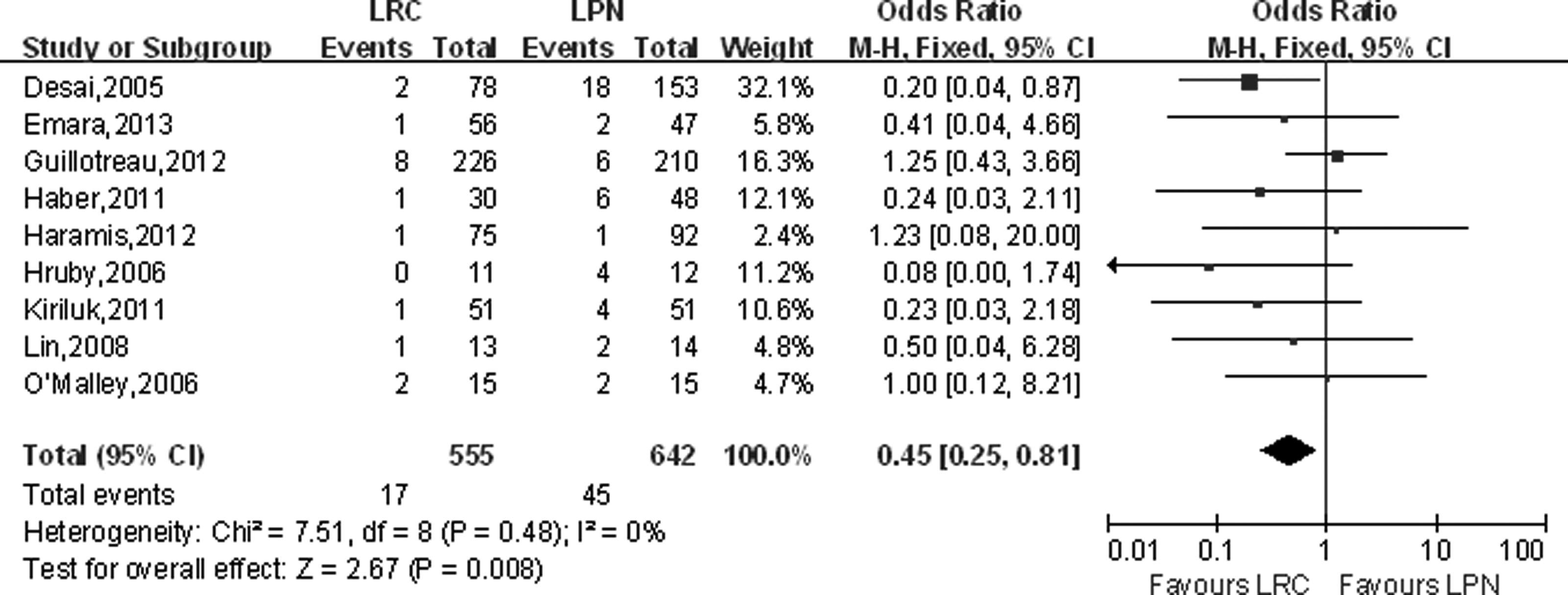
Forest plot and meta-analysis of major complications with laparoscopic renal cryoablation (LRC) and laparoscopic partial nephrectomy (LPN). CI, confidence interval; M-H, Mantel–Haenszel test.
Oncologic outcomes
Pooling data of five4,7–10 and three8,9,13 studies reported local recurrence and distant metastasis rate, respectively. LRC was associated with higher local recurrence (OR=13.03; 95% CI, 4.20–40.39; P<.001) (Table 3 and Fig. 5) and distant metastasis rate (OR=9.05; 95% CI, 2.31–35.51; P=.002) (Table 3 and Fig. 6).

Forest plot and meta-analysis of local recurrence comparing laparoscopic renal cryoablation (LRC) and laparoscopic partial nephrectomy (LPN). CI, confidence interval; M-H, Mantel–Haenszel test.

Forest plot and meta-analysis of distant metastasis rate comparing laparoscopic renal cryoablation (LRC) and laparoscopic partial nephrectomy (LPN). CI, confidence interval; M-H, Mantel–Haenszel test.
Discussion
Open partial nephrectomy is an effective method of treating SRMs and has been seen as the gold standard for decades. This meta-analysis shows that both LRC and LPN are viable options for the management of patients with SRMs. Compared with LPN, LRC results in a higher risk of local tumor progression but a lower risk of perioperative complications. Thus, patient morbidity, cancer control, and preservation of renal function should be balanced in treating SRMs.
Many surgeons who perform LPN tend to select patients who are generally fitter with a tolerable age and a good comorbidity profile. A significant selection bias occurs when comparing LRC and LPN with regard to age and solitary kidney rate. Pooled data showed that patients with older age and had a higher solitary kidney rate are more likely to undergo LRC. In addition, the longer follow-up experience available for LPN makes it a more suitable procedure for patients with longer life expectancy. 10 Both groups had a good postoperative renal function in management of patients with SRMs. We also recognized that the pre- and postoperative SCr and GFR outcomes of the two procedures of patients were comparable; also, the follow-up SCr percentage increase and GFR percentage decrease were similar.
Our study indicates that LPN may convey a higher risk of perioperative complications than LRC. Most notable is that the risk for intraoperative and major complications appears to be increased. In particular, beyond the evident selection bias in terms of elder age and solitary kidney (in favor of LPN), the comparison of complications between LRC and LPN is still strongly significant. If one could account for this, the increased risk of complications for LPN may be higher than for LRC, especially the rate of intraoperative and major complications. One issue with this analysis is the grading of complications; however, this was not possible because details of managing the particular complication were not always reported. Thus, we divided the complications group into minor and major complications instead of the standard Clavien grading. Although the Clavien classification may be more detailed, this method appears to be appropriate for the purpose of this meta-analysis.
As for the oncologic outcomes, LRC achieved a poor prognosis compared with LPN in terms of local recurrence and distant metastasis. Only two studies reported the survival; thus, no meta-analysis was conducted. Haber et al. 9 found that overall survival was comparable between LPN and LRC at 3 (93% versus 93%) and 5 (93% versus 88%) years, respectively (P=.74), although the LPN group had superior cancer-specific survival and recurrence-free survival at 3 and 5 years compared with the LRC group. Lin et al. 13 demonstrated the overall and cancer-specific survival rates were 100% and 100% for the LPN group at 3 years and 92% and 89% for the LRC group at 2 years, respectively. Gill et al. 18 reported on 56 patients with 3 years of follow-up with a 75% reduction in the size of the cryolesion, and the 3-year cancer-specific survival was 98%. Hegarty et al. 19 reported on 66 patients who had over 5 years of follow-up; 3 patients (6%) developed tumor recurrence and required nephrectomy, the 5-year overall survival was 81%, and the cancer-specific survival was 98%. A significant selection bias occurs when comparing oncologic outcomes of LPN and LRC because patients with poorer prognostic features, for example, elder age and a greater risk of solitary kidney, are more likely to undergo LRC. In addition, the rate of metastatic tumor progression is strongly influenced by differences in follow-up duration between LRC and LPN. It is possible that the rate of local recurrence and distant metastases following LRC would be higher with longer follow-up. 20 Therefore, further well-designed, large, simple, long-term follow-up RCTs should take into consideration proving the finding of oncologic outcomes.
However, we should admit that there existing certain inherent limitations in the studies included in our meta-analysis that cannot be ignored when interpreting our data. In addition to the limitations already discussed (selection bias, nonstandard complications grading, and lack of standardized reporting of tumor progression and survival), several points merit discussion. We did not have original datasets from each series available. The major limitation of this study was the limited number of well-constructed prospective studies. Indeed, there was no RCT included in our analysis, and only two comparative prospective trials compared LPN with LRC. Second, the mean follow-up duration of LRC studies is shorter, which makes the results subject to follow-up bias. In addition, the small sample size of some studies, the marked heterogeneity for several continuous variables, an unmeasurable selection bias, and the potentially existing significant risk of publication bias may have had an influence on the confidence of the results more or less.
Nevertheless, our data analysis establishes the feasibility and advantages of performing LRC as being comparable to those of LPN. Our present meta-analysis comparing LRC and LPN was conducted at an appropriate time with enough data available for extraction. We applied a series of as many variables as available, including demographic and clinical baseline characteristics, perioperative and oncological variables, renal function, and complications, to compare LRC with LPN and strict criteria to evaluate the quality of the included studies. Here, we provide up-to-date information that may be worthy of reference on the role of LRC for the treatment of SMRs compared with LPN.
Conclusions
Nine eligible trials (555 cases and 642 controls) assessing LRC versus LPN were identified, including two prospective and seven retrospective studies. Patients undergoing LRC were significantly older and had a higher solitary kidney rate. Compared with LPN, although LRC was associated with superior perioperative safety, comparable renal function, and fewer complications, especially the rate of intraoperative complications and major complications, LRC may still result in a higher risk of tumor progression with higher local recurrence and distant metastasis rate. Therefore, our meta-analysis suggested that LRC is associated with worse oncological outcomes than LPN, but LRC may be indicated in selected patients with significant comorbidity. However, despite our rigorous methodological review, because of the inherent limitations of the included studies and the fact that the long-term oncologic results are not available, further large sample, prospective, multicenter, long-term follow-up studies and RCTs should be undertaken to confirm our findings.
Footnotes
Acknowledgments
This work was supported by the National Natural Science Foundation of China (grants 31072238, 31172441, 31372562, and 81170650) and the National Major Scientific and Technological Special Project for Significant New Drugs Development (grant 2012ZX09303018). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.