
Abstract
Abstract
Background:
Near-infrared fluorescence laparoscopy after intravenous indocyanine green (ICG) administration has been proposed as a promising surgical imaging technique for real-time visualization of the extrahepatic bile ducts and arteries in clinical laparoscopic cholecystectomies. However, optimization of this new technique with respect to the imaging system combined with the fluorophore is desirable. The performance of a preclinical near-infrared dye, CW800-CA, was compared with that of ICG for near-infrared fluorescence laparoscopy of the cystic duct and artery in pigs.
Materials and Methods:
Laparoscopic cholecystectomy was performed in six pigs (average weight, 35 kg) using a commercially available laparoscopic fluorescence imaging system. The fluorophores CW800-CA and ICG (both 800 nm fluorescent dyes) were administered by intravenous injection in four and two pigs, respectively. CW800-CA was administered in three different doses (consecutively 0.25, 1, and 3 mg); ICG was intravenously injected (2.5 mg) for comparison. Intraoperative recognition of the biliary structures was recorded at set time points. The target-to-background ratio was determined to quantify the fluorescence signal of the designated tissues.
Results:
A clinically proven dose of 2.5 mg of ICG resulted in a successful fluorescence delineation of both the cystic duct and artery. In the CW800-CA-injected pigs a clear visualization of the cystic duct and artery was obtained after administration of 3 mg of CW800-CA. Time from injection until fluorescence identification of the cystic duct was reduced when CW800-CA was used compared with ICG (11.5 minutes versus 21.5 minutes, respectively). CW800-CA provided clearer illumination of the cystic artery, in terms of target-to-background ratio.
Conclusions:
As well as ICG, CW800-CA can be applied for fluorescence identification of the cystic artery and duct using a commercially available laparoscopic fluorescence imaging system. Fluorescence cholangiography of the cystic duct can be obtained earlier after intravenous injection of CW800-CA, compared with ICG. These findings increase the possibilities of use and of optimization of this imaging technique.
Introduction
I
Near-infrared fluorescence imaging after intravenous indocyanine green (ICG) administration is an innovative and promising laparoscopic imaging method for intraoperative visualization of crucial anatomical structures. 4 Several clinical pilot studies have demonstrated its usefulness and feasibility for real-time intraoperative identification of extrahepatic bile ducts and arteries to assist in safe and time-efficient gallbladder removal. However, this new technique needs optimization with respect to imaging systems and injected fluorophores.
CW800-CA is a relatively new fluorophore, which like ICG also has 800 nm fluorescent capabilities. It has not yet been cleared by the U.S. Food and Drug Administration for clinical use but has a low risk of toxicity equal to that of ICG and incorporates favorable characteristics for fluorescence imaging of vital anatomy.5,6 The most advantageous characteristic of CW800-CA is its increased hydrophilicity, resulting in improved secretion into bile and earlier fluorescence illumination of the bile ducts.5,6
This study was conducted to assess the performance of CW800-CA versus the clinically already available ICG for near-infrared fluorescence laparoscopy of the cystic duct and cystic artery in pigs using a commercially available laparoscopic fluorescence imaging system.
Materials and Methods
This study was conducted at the central animal facilities of Maastricht University (Maastricht, The Netherlands). Animals were used in compliance with the regulations of the Dutch legislation for animal research, and the study protocol was approved by the Animal Ethics Committee of Maastricht University (project number 2012-098). A pig model was chosen because of its similarity with human anatomy. Six female Dutch Landrace pigs, weighing an average of 35 kg, were used for the current study.
Laparoscopic fluorescence imaging system
A commercially available laparoscopic fluorescence imaging system (Karl Storz GmbH & Co. KG, Tuttlingen, Germany) was used. The system includes a plasma light guide and 30° 10-mm laparoscope applicable for both white light and near-infrared fluorescence imaging. A foot pedal allows the surgeon to easily switch back and forth from conventional imaging to fluorescence imaging. Procedures were digitally recorded.
Preparation of near-infrared fluorophore
In these animal experiments, the system, which was primarily developed for ICG imaging, was now also tested for its feasibility for real-time intraoperative fluorescence visualization of biliary anatomy (cystic duct and cystic artery) after intravenous administration of the preclinical fluorescent dye CW800-CA (a carboxylate of the near-infrared fluorophore IRDye® 800CW [LI-COR Biosciences, Lincoln, NE]). CW800-CA was diluted in a sterile phosphate-buffered saline (PBS) solution.
Surgical technique
Premedication comprised intramuscular injection of azaperone (3 mg/kg), ketamine (10 mg/kg), and atropine (0.05 mg/kg). Anesthesia was induced with intravenous administration of thiopental (10–15 mg/kg), followed by intubation, and maintained with the animal under anesthesia with isoflurane (depending on effect) and oxygen (20–40 mL/kg/minute). Thereafter a laparoscopy was performed.
In each pig a laparoscopic cholecystectomy was performed, according to the Dutch Guidelines and best practice for laparoscopic cholecystectomy, 7 which is based on the Critical View of Safety technique.
One experiment per animal was conducted. In the first two pigs, 1 mL of ICG (2.5 mg/mL of Infracyanine®; SERB, Paris, France) was injected intravenously. This dose has proven sufficient for clinical use. 8 For the third experiment (pig number 3), 5 mg of CW800-CA was diluted in 20 mL of PBS solution (0.25 mg/mL). One millliliter of this solution (0.25 mg) was intravenously administered. For the subsequent three experiments, 5 mg of CW800-CA was diluted in 5 mL of PBS solution (1 mg/mL). Next, 1 mL (1.0 mg) of the solution was injected in pig number 4. Three milliliters (3.0 mg) of the solution was administered in pigs numbers 5 and 6.
Fluorescence imaging was obtained directly after dye injection and subsequently every 5–10 minutes. Intraoperatively the researcher systematically recorded on a form whether the localization of cystic duct or cystic artery could be identified at set time points, comparing the WL camera mode with the ICG mode. For agreement on the identification of the aforementioned structures, the attending surgeon was consulted. A structure was scored as “identified” if its localization was confirmed with great certainty by the experienced surgeon. An overview of the six experiments is presented in Table 1.
ICG, indocyanine green.
Quantitative fluorescence image analysis
For objective assessment of the degree of fluorescence illumination in the extrahepatic bile ducts and artery, OsiriX version 5.5.1 imaging (open source) software was used. The fluorescence images were analyzed by determining target-to-background ratio (TBR). TBR was defined as the mean fluorescence intensity (FI) (in arbitrary units) of three point regions of interest in the target (i.e., cystic duct or cystic artery) minus the mean FI of three background regions of interest in the liver hilum, divided by the mean FI of the three background regions of interest in the liver hilum, according to the following equation:
Results
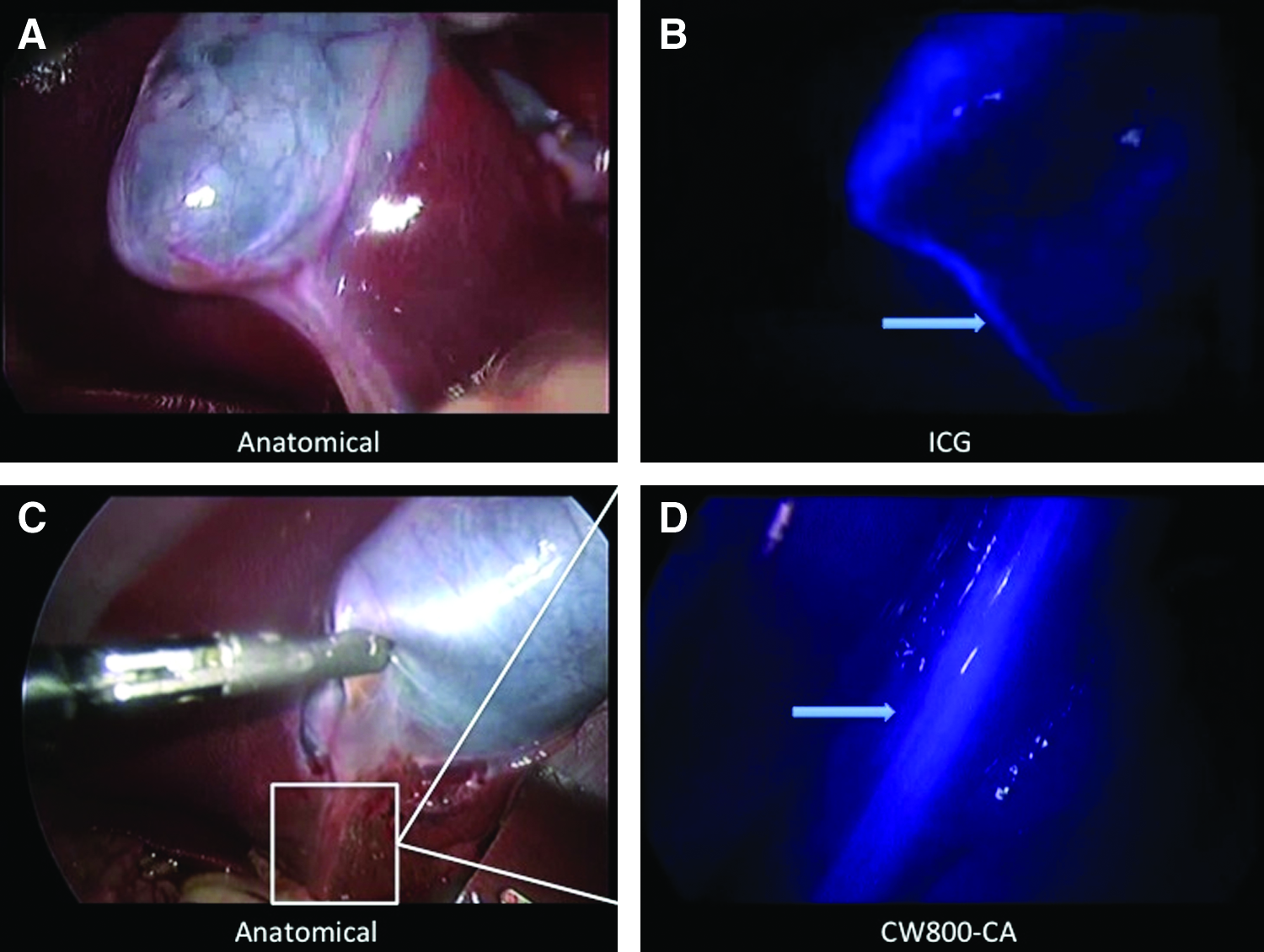
In the first two experiments ICG fluorescence laparoscopy for identification of the cystic artery (Fig. 1B) and cystic duct (Fig. 2B) was successfully conducted. The CW800-CA dosage in experiments 3 (0.25 mg) and 4 (1.0 mg) was insufficient to obtain fluorescence delineation of these structures. Using a dose of 3 mg of CW800-CA in the last two experiments led to clear visualization of the cystic artery (Fig. 1D) and cystic duct (Fig. 2D) in both pigs. Observations of the six experiments are summarized in Table 1.

Cystic artery imaging.
Cystic duct delineation.
TBR
The TBR values of the cystic artery versus gallbladder and the cystic artery versus liver parenchyma in the arterial phase after ICG injection were −0.6 and 0.5, respectively (pig 2,±30 seconds after dye administration [Fig. 1B]). These data confirm the inability of ICG-based imaging to identify the cystic artery when positioned directly on the liver parenchyma. After injection of CW800-CA, the TBR values of the cystic artery versus gallbladder and the cystic artery versus liver parenchyma were 1.1 and 1.7 (±30 seconds after dye administration [Fig. 1D]). This indicates a clear recognition of the cystic artery when positioned above liver parenchyma and the gallbladder if CW800-CA is used. The TBR values of the cystic duct versus liver parenchyma were 3.2 for ICG (Fig. 2B) and 2.3 for CW800-CA (Fig. 2D).
Complications
No peri- or postoperative complications regarding the extrahepatic bile ducts occurred. None of the pigs developed any adverse reactions to the injected ICG or CW800-CA. No interference with intraoperative monitoring of the saturation of peripheral oxygen was observed.
Discussion
In the present study the feasibility of fluorescence imaging of the cystic duct and artery using CW800-CA and a commercially available laparoscopic fluorescence imaging system was investigated. To assess the performance of this preclinical contrast agent, ICG was used for comparison. CW800-CA provided comparable visualization of the course of the cystic duct and better identification of the cystic artery.
With respect to the fluorophores investigated in this study, it is important to address the following characteristics. ICG is a disulfonated heptamethine indocyanine that is Food and Drug Administration–approved for clinical use. After intravenous injection, it is rapidly cleared from the blood by the liver and transported into the bile. Consequently, intravenously injected ICG is applicable for cholangiography. CW800-CA is a carboxylate of IRDye 800CW, a tetrasulfonated heptamethine indocyanine. Emission of this dye is quite similar to that of ICG (also at 800 nm). However, after intravenous injection, it is rapidly cleared not only by the liver and excreted into bile, but also by the kidneys and excreted into the urine. As a result this dye is usable for imaging of the biliary anatomy and of the ureters. 9
Previously Tanaka et al. 5 tested ICG and CW800-CA for bile duct imaging in rats and pigs during open surgery. CW800-CA proved to be more selective, as ICG suffered from lack of efficient secretion into bile from the liver. In addition, CW800-CA was excreted into bile in a predominantly unmetabolized form, which increases the rapidity and signal intensity by which images can be obtained after administration.
In the present study, the CW800-CA dosage in the first experiment was based on the report by Tanaka et al. 5 A dose of 7.5 μg/kg of body weight appeared not sufficient for laparoscopic fluorescence detection of the cystic duct and artery. With a significantly higher dose (85 μg/kg) of the injected dye, clear visualization of the course of the cystic duct and artery was obtained in this study.
Furthermore, from this study it was noted that time from injection until fluorescence identification of the cystic duct was reduced when CW800-CA was used compared with ICG (11.5 minutes versus 21.5 minutes, respectively). Based on TBR values, this study demonstrates the ability of identifying the cystic duct after injection of both fluorophores. Regarding arterial fluorescence imaging, background signal (i.e., dye uptake by the liver parenchyma) was larger when ICG was used, compared with CW800-CA. Therefore recognition of the cystic artery might be easier with CW800-CA.
Besides laparoscopic cholecystectomy, fluorescence imaging of crucial biliary structures might be beneficial in other (laparoscopic) hepatopancreatobiliary surgical procedures as well. Possible applications of this technique during hepatopancreatobiliary surgery include tumor detection in liver and pancreas resections and real-time imaging of intra- and extrahepatic bile ducts (and branches) of hepatic, cystic, pancreatic, gastroduodenal, and pancreatoduodenal arteries.10–12
Moreover, fluorescence imaging could be performed to detect bile leakage during open and laparoscopic partial liver resections. This complication after hepatectomy occurs in approximately 8% of all patients undergoing partial liver resection and is associated with greater postoperative mortality and healthcare costs. 13 Prevention of bile leakage after hepatectomy therefore deserves attention. In a randomized clinical trial that evaluated the use of ICG fluorescence cholangiography to prevent postoperative bile leakage after hepatic resections, the ability to detect leaking bile duct stumps at the cut surface of the remnant liver, which were missed by conventional bile leak tests, was demonstrated. 14 Given its pharmacokinetics, CW800-CA might prove to be even more suitable for the detection of bile leakage.
Although this report only describes a small experimental animal study and a large difference in dosage of CW800-CA, the concept of fluorescence visualization of the cystic duct and artery using CW800-CA has successfully been demonstrated using a commercially available laparoscopic fluorescence imaging system. A clinical pilot study investigating the feasibility of near-infrared fluorescence imaging using CW800-CA in laparoscopic cholecystectomy is the next step. Such a pilot study should focus on dose-finding of the administered dye, as even a lower dose than 3 mg/mL (used in experiments 5 and 6) might be sufficient.
Conclusions
As well as ICG, CW800-CA can be applied for laparoscopic fluorescence identification of the cystic artery and duct using a commercially available imaging system. Laparoscopic fluorescence cholangiography of the cystic duct can be obtained earlier after intravenous injection of CW800-CA, compared with ICG. With the availability of two instead of one fluorophore, the possibilities increase to further optimize the imaging capabilities of the presently available fluorescence systems. A dose-finding and clinical feasibility study for CW800-CA is the next step.
Footnotes
Acknowledgments
The authors thank Karl Storz GmbH & Co. KG (Tuttlingen, Germany) for technical services and providing the laparoscopic fluorescence imaging system for animal experiments and the staff of the animal facilities of Maastricht University for their assistance in performing the animal experiments.
Disclosure Statement
No competing financial interests exist.