
Abstract

Oral Abstracts
Clinical & Basic Science
THE IMPACT OF LAPAROTOMY VERSUS LAPAROSCOPY ON INTRACELLULAR NITRIC OXIDE (NO) FORMATION AND BACTERIAL CLEARANCE
Background: Surgical intervention-related trauma contributes largely to the development of postoperative immunosuppression, with reduced resistance to secondary bacterial infection. This study compared the impact of laparotomy versus laparoscopy on intracellular nitric oxide (NO) formation and bacterial clearance.
Materials and Methods: Balb/c mice were randomized into control, laparotomy, and laparoscopy groups. Serum TNF-α and IL-6 were measured by cytometric bead array. Intracellular nitric oxide (NO) formation in peritoneal macrophages was detected by using the fluorescent probe 4-amino-5-methylamino-2’,7’-difluorescein (DAFFM) diacetate (Molecular Probes) as described previously. Bacterial clearance was assessed after mice were challenged with live E. coli and S. aureus.
Results: In contrast to laparoscopy, laparotomy led to a strong increase in serum TNF-α and IL-6. Intracellular NO formation in response to gram-negative E. coli or gram-positive S. aureus was dramatically reduced in macrophages from mice that underwent laparotomy when compared with macrophages from the control mice (p<0.05), whereas macrophages from mice that underwent laparoscopy showed significantly higher intracellular NO formation than that observed not only in macrophages from mice that underwent laparotomy, but also in macrophages from the control mice. Mice that underwent laparotomy displayed substantially higher bacterial counts in the blood and visceral organs following bacterial infection, whereas mice subjected to laparoscopy did not show any defects in their bacterial clearance.
Conclusion: In response to bacterial challenges macrophages from mice subjected to laparoscopy produced significantly more NO than macrophages from the control mice did. Laparotomy has an adverse effect on bacterial clearance. By contrast, laparoscopy appears to preserve, thus alleviating the development of postoperative immunosuppression.
THORACOSCOPIC DELIVERY OF RAAV GENE THERAPY TO THE DIAPHRAGM IN POMPE DISEASE
Background: Pompe disease is a metabolic myopathy that is based in lack of the enzyme responsible for glycogen degradation in tissues and affects primarily cardiac and skeletal muscle. With the advent of enzyme replacement therapy, cardiac function is improved, but progressive loss of diaphragmatic function continues with respiratory failure eventually requiring mechanical ventilation. We report our initial experience in thoracoscopic delivery of the gene vector to the diaphragm in an experimental rabbit model followed by a human trial.
Materials and Methods: After appropriate IRB and IACUC approval, 5 juvenile New Zealand white rabbits were injected with rAAV-gaa under thoracoscopic view using a 4 mm 30 degree scope through a 5 mm port. Insufflation was used in all cases with CO2. The right diaphragm was injected and all animals survived surgery. The rabbits were euthanized at day 10, and the diaphragms and multiple organs were harvested for evaluation.
Human thoracoscopic injections are being carried out as part of a Phase I/II trial and are being performed bilaterally in children from 3–14 years with ventilator dependant Pompe disease. Similar to the rabbit studies, three injections with 0.75 ml each were performed in each hemidiaphragm via transcutaneous needle placement, and diaphragmatic EMG was recorded as a baseline. Prior to the procedure, diaphragmatic thickness and function was analyzed using MRI and ventilation studies.
Results: All 5 rabbits survived the surgical procedure, and recovered. Examination of the diaphragm indicated detectable copies of the vector throughout the diaphragm with highest concentration around the injection sites. There was no systemic delivery of the vector noted in any organs. The gene was noted to be travelling in the phrenic nerve fibers retrograde.
Currently, we have injected the vector in 5 children with Pompe disease. All were ventilator dependant and on enzyme replacement therapy with stable cardiac function. Average age was 9.5 years. All were Caucasian, with 4 male and 1 female. Average case time was 68 minutes. All were discharged home according to protocol on day 5. Initial blood PCR analysis revealed no systemic administration of the vector. There were no wound complications, and two patients required chest tubes for 2 days each. We have noted significant improvement in diaphragmatic function in three of the early cases, with improved peak pressure generated, and one patient has been able to come off the ventilator for 3 hour periods.
Conclusions: This is an initial report detailing our experience with a novel delivery mechanism of gene vector to the diaphragm in Pompe disease. Thoracoscopy allows easy visualization and injection of the vector. This therapy holds promise for improving respiratory function in Pompe patients.
EVALUATION OF A VIDEO TELESCOPIC OPERATING MICROSCOPE (VITOM) FOR PEDIATRIC SURGERY AND UROLOGY: A PRELIMINARY REPORT
Introduction: Pediatric surgery and urology involve numerous complex procedures. Traditional magnification methods include loupes and the standard operating microscope. Drawbacks include, but are not limited to, neck strain of the operating surgeon, frequent need to refocus images and an inability to share the magnified visual field with assisting surgeons and trainees. Recent advances have led to the development of a novel compact video microscope (VITOM) that displays high-definition magnified images on a video monitor.
Objective: To evaluate VITOM as a potential substitute for loupes or the standard operating room microscope in complex pediatric procedures, and explore VITOM as an effective intraoperative teaching tool for open surgery.
Methods: Three surgeons (P.K.F., A.L.F., B.P.D.) utilized the VITOM in 20 operations (14 hypospadias, 1 ureteral reimplant, 1 infant inguinal hernia repair, 1 infant cut-down central venous catheter insertion, 1 sacrococcygeal teratoma resection, 1 recurrent tracheoesophageal fistula repair, 1 bilateral inguinal hernia repair). The VITOM II and the images were viewed on a 26-inch flat screen monitor. Each surgeon made subjective evaluations of neck strain and fatigue, and image quality. Two mid-level trainees assessed the potential for improved teaching value compared with traditional method.
Results: The VITOM was deemed easy to use, with each surgeon requiring approximately two procedures to “feel comfortable” utilizing the VITOM. The combined overall experience of the surgeons using the VITOM demonstrated improved comfort with less neck strain and fatigue compared with traditional magnification. In addition, each surgeon felt that the image quality was excellent and did not require additional time spent on focus adjustments. Trainees felt that intraoperative visualization was greatly enhanced through the use of a large HD flat screen, and was beneficial for teaching.
Conclusion: Based on our preliminary evaluation, we show that the VITOM is well suited for pediatric surgical cases requiring magnification. Our early findings also suggest that VITOM provides very workable magnification of small anatomic structures while reducing surgeon fatigability and neck strain. Furthermore, it facilitated effective intraoperative teaching for residents and may serve as means to archive operations for future pre-operative planning.

AUGMENTED REALITY NAVIGATION SYSTEM FOR LAPAROSCOPIC SURGERY FOR PEDIATRIC MALIGNANT TUMOR ON PREOPERATIVE CT IMAGE
Department of Pediatric Surgery, Faculty of Medical Sciences, Kyushu University
Background: In pediatric endoscopic surgery, limited views and lack of tactile sensation restrict the surgeon's abilities. Therefore, an intra-operative navigation system is very useful for pediatric endoscopic surgery. We developed an augmented reality (AR) navigation system based on preoperative CT imaging for pediatric endoscopic surgery. We report our experiences with an AR real-time surgical navigation system for laparoscopic surgery to detect and resect a tiny and less-visible recurrent mass of pediatric malignancies.
Case 1: 4-year-old girl was diagnosed with Wilms tumor. The tumor extirpation was performed and she was administered postoperative chemotherapy. After 6 months from postoperative chemothrapy, the local recurrence and the lung metastasis was detected by CT. After additional chemotherapy and radiotherapy, the size of the local recurrence decreased and the lung metastasis disappeared. The size of local recurrence was small (1 cm) and the adhesion was expected. Therefore, we applied the AR navigation system based on preoperative CT imaging for detection of the tumor. We used an optical tracking system for registration between reconstructed three-dimensional (3D) CT image and body surface markers. The AR visualization was superimposed preoperative three-dimensional 3D CT images onto captured laparoscopic live images and the tumor was resected successfully without surgical complications.
Case 2: 5-year-old girl was diagnosed with alveolar rhabdomyosarcoma in soft plate. When she was 6 years old, tumor recurrence was recognized at the left chest wall (about 13 mm). It was resected using thoracoscopy. When she was 8 years old, a tiny recurrent mass was recognized at the left chest wall again in CT scan. It was considered to be difficult to identify and resect the tumor because the tumor size was small (8 mm) and the pleural adhesion was expected. Therefore, we applied the AR navigation system based on preoperative CT imaging for detection of the tumor. The tumor was not recognized by laparoscopic image only during operation. However, we used the same method as case 1 and the tumor was resected successfully.
Conclusion: This navigation system is very useful for the small and less-visible tumor with pediatric malignancies.
Background: The pathogenesis of intestinal dysmotility in gastroschisis patients is not completely understood. Peel formation and dysorganisation of intestinal cajal cells have been proposed in humans. The aim of this study was to evaluate the impact of prenatal coverage of gastroschisis on gut inflammation and expression of intestinal cajal cells (ICC) in a fetal lamb model.
Methods: On mid-gestation (day 77) an abdominal wall defect was fetoscopically created within 8 German blackhead sheep. A second fetoscopic procedure was performed 21 days later, with the attempt to cover the created defect. The fetus was retrieved by cesarean section on day 132 of 145 days gestation and evaluated. For control 3 German blackhead sheep naturally born around day 147 of gestation were used. In all sheep tissue samples from stomach, small and large intestine as well as liver and spleen were collected. The samples were colored with triclor. For ICC anti-CD117 was used.
Results: In all samples with exposure to amnion fluid peel formation and decreased ICC was found. Successful coverage reduced peel formation and dysorganisation of ICC compared to long exposure.
Conclusions: Peel formation and ICC dysformation are vastly reduced by prenatal coverage of the abdominal wall defect, thus validating the concept of fetal therapy in subjects with gastroschisis. Moreover, the animal model used, mimics bowel changes as seen in human gastroschisis patients. The model may therefore be used for further research.
Urology & Hernia
LAPAROSCOPIC PERCUTANEOUS EXTRAPERITONEAL CLOSURE FOR INGUINAL HERNIAS IN CHILDREN: A SINGLE-INSTITUTE SERIES OF 277 CONSECUTIVE PATIENTS
Purpose: The indications for laparoscopic inguinal hernia repair in infants and children remain controversial. There are many techniques available for laparoscopic inguinal hernia repair in children. The aim of this study was to evaluate the efficacy and safety of laparoscopic percutaneous extraperitoneal closure (LPEC) in comparison with conventional open hernia repair (Potts).
Methods: In our institute, LPEC has been performed in girls since 2008, following which the indications were gradually extended. Currently, LPEC is indicated for all patients in the pediatric population regardless of sex. A retrospective analysis was performed using the surgical charts of consecutive patients who underwent LPEC or Potts during the last four years. The outcomes of LPEC were compared with those of Potts. During LPEC, a 5-mm laparoscope is placed through an umbilical incision, and then a 2-mm grasping forcep is inserted on the right or left side of the umbilicus. The hernia sac orifice is closed extraperitoneally using circuit suturing around the internal inguinal ring with an LPEC needle and non-absorbable suture materials percutaneously inserted at the midpoint of the inguinal line.
Results: A total of 277 infants and children (100 males and 177 females, mean age: 56.5±37.3 months) underwent LPEC and 158 infants and children (137 males and 21 females, mean age: 37.2±38.8 months) underwent Potts. All surgeries were successfully performed without any serious complications. During LPEC, a contralateral patent processus vaginalis was found and subsequently repaired in 136 of the 250 unilateral hernia cases (54.4%). The mean operative time for bilateral hernia repair was shorter using LPEC than that observed with Potts (LPEC: 45.6±12.9; Potts: 83.6±34.3 min, p<0.001). There were no differences in the mean operative time for unilateral hernia repair between the two procedures (LPEC: 37.3±8.0; Potts: 35.9±12.0 min). There were no differences in the recurrence rates (LPEC: 1.1%; Potts: 0%, p=0.557). There was a significant reduction in the risk of developing a contralateral metachronous inguinal hernia in the LPEC cases compared with that observed in the Potts cases (LPEC: 0/277; Potts: 13/158, p<0.001). Neither hydroceles nor testicular atrophy occurred after surgery with either operation method. The completion rate of day surgery was the same between the two methods (LPEC: 97%, Potts: 97%).
Conclusions: LPEC can provide shorter operative times for bilateral hernia repair and lower rates of metachronic contralateral hernias compared to Potts. The recurrence rate of LPEC is comparable to that of Potts with superior cosmetic results, and the completion rate of day surgery is comparable between the two procedures. These data indicate that LPEC can be used as a standard procedure for inguinal hernia repair in the pediatric population with some advantages over conventional open inguinal hernia repair.
SHOULD THE INGUINAL HERNIA IN CHILDREN BE TREATED BY LAPAROSCOPIC SURGERY?
Dept of Pediatric Surgery, The Affiliated Provincial Hospital of Anhui Medical University, Hefei, China
Objective: To evaluate whether laparoscopic surgery for inguinal hernia in children is better than traditional surgical treatment.
Methods: From January 2010 to October 2012, 3716 children with inguinal hernia were treated in two hospitals; 2616 of them were operated by laparoscopic surgery, and 1100 of them by traditional surgery. The operative time, length of hospital stay, postoperative hernia recurrence, and the treatment of contralateral occult hernia between the two groups were compared.
Results: The 3716 patients (3336 male, 380 female) had an average age of 3.5 years (14 days to 13 years). Laparoscopic surgery group, the mean operation time was 12 minutes, the average length of hospital stay for three days, and recurrence in 24 patients (0.9%), contralateral occult hernia were probed in 487 cases and treated at the same time. Traditional operation group, the mean operation time is twenty minutes, the average hospitalization time is 4 days. In this group, there are 11 patients (1%) of hernia recurrence, hospitalization for again on the other side of the hernia surgery treatment of 133 cases. The number of operative mode choosed by childrens'guardian, Laparoscopic operation increased 1.25 times than traditional operation, but no increase in traditional surgical surgery.
Conclusion: Although the choice for laparoscopic surgery for inguinal hernia in children is in the currently controversial circumstances, laparoscopic surgery with small trauma and cosmetic effect etc, has been generally accepted. Our data show that the laparoscopic treatment for inguinal hernia in children is safe, reliable and lower recurrence rate, and the operative time and hospitalization days is shortened compared with traditional surgery. It is especially suitable to children with bilateral inguinal hernia or contralateral occult hernia. For the good cosmetic effect, laparoscopic surgery is chosen by more and more children's guardians, thus good social and economic benefits are acquired in our hospitals for increased patients. To carry out laparoscopic treatment for children with inguinal hernia, surgeons should have a wealth of clinical experience about laparoscopy and familiarity with the hernia anatomy.
Key words: Inguinal hernia; Laparoscopic surgery; Children
ABSTRACT WITHDRAWN
RETROPERITONEOSCOPIC PYELOPLASTY IN CHILDREN - LESSONS LEARNT
Aim: Retroperitoneoscopic pyeloplasty was performed in 116 patients since January 2005 to November 2012. The aim of the study was to analyze difficulties faced during surgery and the options utilized to overcome them.
Methods: All patients who underwent retroperitoneoscopic pyelopasty since January 2005 were enrolled in the study. Data were collected prospectively and results were analyzed.
Results: 116 patients (Age 4 weeks–18 years) (right side 52, left side 66) underwent 118 retroperitoneoscopc Anderson Hynes pyeloplasty since January 2005 to November 2012. Mean operative time was 128 minutes. A balloon was used to open retroperitonea space in 87 procedures and open insertion of trocar with CO2 insufflation was used to open the retroperitoneal space in 31 procedures (oprative time to open the space was 27 min vs 10 min). Movement of kidney and pelvis during ventillation added to the difficulty in suturing in 81 procedures. Addition of trans-abdominal suture on pelvis in 37 procedures reduced the movements and mean operative time decreased significantly (96 minutes vs 158 minutes). 12 patients had UTI preoperatively and 4 patients had preoperative insertion of DJ stent. In 14 patients cystoscopy, retrograde pyelography and insertion of stent or guide wire was performed just before pyeloplasty. Mean operative time was 168 minutes at retroperitoneoscopic pyeloplasty. Antegrade stenting was performed in 68 patients and pelvi-ureteric stent was kept in 32 infants below 6 months of age. Pyeloplasty sutures were inturrupted in initial 16 procedures and continuous in 102 procedures. Mean operative time reduced significantly (189 min vs 112 min).
Conclusion: Open insertion of trocar and CO2 insufflation opens the retroperitoneal space easily in children. Operative time was reduced significantly by transabdominal stay suture, antegrade stenting and continous suturing in retroperitoneoscopic Anderson Hynes pyeloplasty in children.
URETEROPELVIC JUNCTION OBSTRUCTION (UPJO) DUE TO ABERRANT POLAR VESSELS: LAPAROSCOPIC VASCULAR HITCH
ABSTRACT WITHDRAWN
DOUBLE-J OR TRANSRENAL URETERAL STENT IN LAPAROSCOPIC PYELOPLASTY IN INFANTS AND CHILDREN: A COMPARISON AND NEW TECHNIQUE
Aim: Laparoscopic transabdominal pyeloplasty is today's standard treatment of choice for ureteropelvic junction obstruction in children and adolescents. Transureteral stenting of the anastomosis is a crucial technical detail and several methods have been described, such as laparoscopic placement of a double-J catheter or transrenal puncture using a cannula. We compared our experience with intra-and extracorporal stenting and presented a novel technique to solve the problem.
Methods: All 86 patients who underwent laparoscopic transabdominal pyeloplasty in our institution from 12/2003 to 11/2012 were included. We retrospectively compared patients with anastomosic stenting by laparoscopic placement of double-j catheter (n=48) versus patients with transrenal stent (n=38). Double-J catheters were routinely removed by cystoscopy with general anesthesia. The transrenal stents were introduced via a cannula from the flank (n=33) or from inside out by transrenal puncture using a specially constructed spear (n=5). The primary endpoint of the analysis were stent related complications that required surgical interventions or increased hospital stay.
Results: 62 boys, 24 girls with a mean age of 5.6 years (78 days-6.9 years) and mean weight of 22.1 kg (5.5–71 kg) underwent laparoscopic transabdominal pyeloplasty. In patients that underwent laparoscopic placement of the doube-J, there were two stent dislocations, requiring surgical intervention, two patients developed a urinary tract infection and in 9 cases it was impossible to place the stent correctly. These patients were left without stent and one of them developed a urinary leakage requiring revision and one a urinary obstruction requiring a temporary nephrostomy. In patients with transrenal stent introduced by puncture with the canula from the flank generally a minor intraoperative bleeing occurred, but there was no intervention or transfusion necessary. There was no bleeding in patients where the transrenal stent was placed from inside out. There were no stent dislocation and no revisions. Overall complications were 6/48 (12,5%) in the intra- and 0/38 (0%) in the extracorporal stent group (p<0.05).
Conclusion: The placement of a transureteral stent in laparoscopic transperitoneal pyeloplasty in children and infants can be challenging. Based on our experience we recommend transrenal stents to avoid complications such as stent dislocation and to facilitate stent removal without general anesthesia. The initial experience with our simple device for transrenal puncture and stent placement is promising.
VIDEO-ASSISTED EXTRACORPOREAL VERSUS OPEN PYELOPLASTY IN INFANTS: A COMPARATIVE STUDY
Background: Pediatric surgeons and urologists are aware of the fact that laparoscopic pyeloplasty in children younger than 2 years is too delicate, risky and controversial. The functional results and surgical morbidity, as well as the use of robotics, compared to traditional mini-lumbotomy pyeloplasty, have shown little or no clear advantage.
Objectives: The authors present the techniques of an intermediate approach, the video-assisted extracorporeal pyeloplasty (VEP) in infants, and a comparative analysis with a series of open surgery.
Patients and Methods: From January 2004 to January 2012, 36 children under 18 months of age underwent VEP to treat pyeloureteral junction (PUJ) obstruction (group A, mean age 6.8 months, 21 male, 15 female, 2 bilateral=38 pyeloplasties). From March 1999 to January 2012, 31 children were treated through mini-lumbotomy by the same authors in institutions where video was not available (group B, mean age 7.3 months, 17 male, 14 female, 1 bilateral=32 pyeloplasties). Patients for re-do procedures were not included. VEP was performed using 3 sites (ports or stab wounds). Viewing through a transperitoneal umbilical 4-mm scope, the PUJ was identified using an epigastric 2.5-mm grasper, and then a 5-mm port site was made right upon it, to help dissect and exteriorize the pelvis and ureter. In children from group B, the approach was a 2.5-cm long posterior lumbotomy. In all patients, a complete extracorporeal pyeloplasty was accomplished (dismembered: 35 in group A, 31 in group B; non-dismembered in the others). A double J catheter was necessary in 30 children from group A and 26 from B. When it did not pass from above (3 in each group), it was introduced retrogradely through a cystoscopy or a percutaneous stent-nephrostomy was done (n=2, group B). All patients after VEP had a perirenal Penrose drain at the lumbar site, and 25 from group B had a drain. Postoperative evolution was evaluated by periodical ultrasound, scintigraphy or radiographs.
Results: All VEP were performed without conversion or operative complications. There was no difference in the mean operative time, hospitalization, pain medication, and frequencies of leakage, stenosis and reoperation in both groups. The DJ catheter stayed for 3–6 months in both groups. Children from group B had keloids (n=2), late nephrectomy (n=2), larger time-consuming reoperations and 3 had lumbar bulging due to persistent neuropraxis.
Conclusions: VEP showed to have functional results similar to open pyeloplasty in infants, with the advantages of less late complications and better cosmesis. It is ideal for surgeons with a short learning curve in intracorporeal pyeloplasty.
ONE-TROCAR-ASSISTED PYELOPLASTY
Purpose: To present the technique and early outcomes of one-trocar-assisted pyeloplasty (OTAP).
Methods: The patient was placed in a lateral decubitus position. A skin incision of 11 mm width was made above the upper iliac crest. The fascia was opened longitudinally. The dissection was carried out through the muscle to Gerota's fascia which was then opened to the peri-renal space. A blunt tip trocar (auto suture) was inserted. The trocar was connected with CO2 and the retroperitoneal space was developed with an insufflation pressure maintained at 12 mmHg. The 10 mm operating laparoscope 0 degree (Stema, Germany) was inserted through the trocar. A retroperitoneal space was created and the pelvic-ureteral junction (PUJ) was identified, dissected from the surrounding tissue and brought up through the trocar site. The pyeloplasty was performed extracorporeally.
Results: From January 2010 to October 2012, 80 patients (66 males and 14 females) with UPJ obstruction underwent operation. The age of these patients ranged from 1 month to 60 months. Five patients required a conversion to open surgery. The mean operative time was 77 minutes and the mean hospital stay was 4.9 days.
Conclusion: OATP is feasible and safe for PUJ in children.
Gastrointestinal & Hepatobiliary I
LAPAROSCOPIC HEPATICOJEJUNOSTOMY FOR CHOLEDOCHAL CYST IN CHILDREN: A MULTICENTER ANALYSIS
Aims: To evaluate the outcomes of laparoscopic hepaticojejunostomy for choledochal cyst in a large multicenter series.
Materials and Methods: Medical records of 956 consecutive patients who underwent Laparoscopic hepaticojejunostomy for choledochal cyst at 7 academic institutions from Sept 2001 to July 2012 were retrospectively analyzed. Patient demographics, perioperative, and early outcomes were analyzed.
Results: A total of 956 patients with choledochal cyst treated laparoscopically were identified and included in the analysis; of these, 12 (1.3%) needed blood transfusion intra-or postoperation; 14 (1.5%) patients developed bile leakage after surgery, but only 5 cases needed surgical intervensions; 8 (0.8%) patient had Roux loop obstuction after the operation; 6 (0.6%) cases suffered anastomotic stenosis and needed re-anastomosis; and 1 case developed intrahepatic stone formation; 2 mortalities occurred, one died of hyperkalemia and the other one died of postoperative bleeding. No other complication occurred during the mean follow-up of 5.7 years (ranged from 4 months to 11 years).
Conclusions: We report a multi-institutional series of laparoscopic hepaticojejunostomy in children with choledochal cyst. Our findings suggest that laparoscopic hepaticojejunostomy represents a feasible treatment option for choledochal cyst by offering reliable middle and long term ourcome, low surgical morbidity.
MANAGEMENT OF THE PEDIATRIC PATIENT WITH CHOLEDOCHOLITHIASIS IN AN ERA OF ADVANCED MINIMALLY INVASIVE TECHNIQUES
Background: The treatment algorithm for children with suspected choledocholithiasis is not well established since the breadth of minimally invasive surgery and endoscopic techniques and equipment continues to evolve. We aimed to review our experience with common bile duct explorations (CBDE) over the past decade in order to detail the techniques used and describe the rate of complications of laparoscopic CBDE in children.
Methods: As a part of an IRB approved study, medical records were reviewed for all patients, ages 1 month to 18 years, undergoing a cholecystectomy at a large tertiary care children's hospital over an 11 year period. Those undergoing an intraoperative cholangiogram (IOC) were documented and operative reports and postoperative records were examined. The decision to perform a cholangiogram or a CBDE was based on the clinical judgement of the surgeon.
Results: Between January 2000 and December 2011, 464 cholecytectomies were performed at our institution. Based on surgeon preference, an IOC was attempted on 174 patients at the time of cholecystectomy with a 97% success rate (n=168). Indications for IOC at the time of surgery included gallstone pancreatitis (n=33), acute cholecystitis (n=12), chronic cholecystitis (n=12), choledocholithiasis (n=49), symptomatic cholelithiasis (n=60), and acalculus cholecystitis (n=8). The average age for patients undergoing an IOC was 12.8 years with a range of 3 months to 17.9 years and an average body mass index (BMI) of 23 (SD 9.2). A history of sickle cell disease was identified in 35% of the patients (n=61) who underwent IOC.
Of the patients who underwent a cholangiogram, 29% (n=51) had an obstructing stone. Laparoscopic CBDE was attempted in 49 out of 51 patients and successfully completed in 46, with a conversion rate of 6.1%. Two patients were treated with an open common bile duct exploration. CBDE was performed with wires, balloon catheters and ureteral baskets with and without the aid of a choledochoscope. The mean age of patients with obstruction of the common bile duct was 12.9 (SD 4.2) and the average BMI was 22.5 (SD 9.5). One third of the patients requiring CBDE had a history of sickle cell disease. Postoperatively, one patient underwent ERCP and sphincterotomy for a retained stone that was impacted and could not be cleared at the time of laparotomy. Two additional patients underwent ERCP for persistent hyperbilirubinemia; however no pathology was identified at the time of endoscopy. The overall rate of choledocholethiasis is 11%.
Conclusions: Biliary stone obstruction occurs with some frequency in our pediatric population. CBDE is a safe and successful approach to choledocholethiasis the majority of the time. The authors suggest that laparoscopic CBDE should be the first step in the management of obstructive choledocholethiasis in centers where the expertise exists to perform the procedure.
LAPAROSCOPIC VERSUS OPEN TREATMENT OF CONGENITAL DUODENAL OBSTRUCTION: MULTI-CENTER OUTCOMES ANALYSIS
Background: Laparoscopic repair of congenital duodenal obstruction has become popularized over the past decade. Comparative data on outcomes, however, are lacking. We hypothesized that laparoscopic repair of congenital duodenal obstruction can be performed with similar outcomes to that of the traditional open repair.
Methods: IRB-approved retrospective review of medical records for all cases of congenital duodenal obstruction (annular pancreas, duodenal web, and duodenal atresia) at three academic teaching hospitals were reviewed from 2005–2011. Patients (n=29) were excluded from the analysis if they had confounding surgical diseases (tracheoesophageal fistula, imperforate anus, gastroschisis, CDH, or complex cardiac disease requiring early repair), did not have duodenoduodenostomy during the first hospital admission or repair was performed prior to transfer from a referring hospital, or were less than 1.7 kg at the time of surgery. Baseline characteristics and outcome measures as well as post-operative complications were recorded. Analysis was performed as intention to treat, with laparoscopic converted to open cases included in the laparoscopic group. Two patients in the laparoscopic group required subsequent open revision: one for persistent obstruction due to a web (3 weeks later) and one for anastomotic stricture (1 year later).
Results: Ninety-eight cases were reviewed and 64 cases were included in the analysis (44 Open, 20 Laparoscopic). Seven laparoscopic cases required conversion to an open procedure (35%), most commonly for difficulty exposing the decompressed distal duodenum. Baseline characteristics were similar with the exception of a longer median time to repair in the open group (Table 1). Laparoscopic repair did take significantly longer, but clinical outcomes were similar (Table 2). Complications were rare (1 line infection, 1 surgical site infection, and 2 incisional hernias), and were similar between methods of repair.
Baseline Characteristics
Data expressed as Median (Range). † Mann-Whitney U.
Data expressed as Median (Range). †Mann-Whitney U.
Conclusions: Laparoscopic duodenoduodenostomy for congenital duodenal obstruction is a technically challenging procedure with a steep learning curve. Despite a relatively high conversion rate, clinical outcomes remain similar to the traditional open repair in selected patients.
Background: We speculated that Roux-en-Y cholecystocolonic anostomosis was as effective for treating children with progressive familial intrahepatic cholestasis (PFIC) as partial biliary diversion. The feasibility of the novel approach in bypassing bile was investigated in rabbits.
Methods: 24 rabbits were randomly divided into three groups: sham operated group (Group 1), 30 cm limb group (Group 2), and 10 cm limb group (Group 3). Group 2 or 3 underwent a Roux-en-Y cholecystocolonic anastomose with a 30- or 10-cm-long Roux limb. 99 mTcEHIDA dynamic biligraphy was used to detect alterations of bile flow among the three groups at 1 year postoperatively. TBA levels and histological changes were also evaluated.
Results: All animals survived and developed normally without clinical symptoms during 1 year follow-up. Bile was diverted into colon directly after cholecystocolonic anastomosis. In group 3, E20 and E35 values were (77.27±6.15)% and (90.39±1.49)% respectively. Gallbladder emptying was accelerated in 10 cm short limb group than in 30 cm long limb group. The ratio of bile shunt was (0.547±0.182), which was also more than that in group 2 (p<0.05). The activity-time curve for the gallbladder area in group 2 looks like a wave. A significant reduction in TBA level was observed in group 2 and 3 (p<0.05).
Conclusions: Roux-en-Y cholecystocolonic bypass was safe, feasibility, and affected by the length of Roux loop. Cholecystocolonic bypass led to a significant loss of bile acids in healthy rabbits and might be considered for bile diversion in pediatric patients with selected cholestatic diseases.
LAPAROSCOPIC KASAI PORTOENTEROSTOMY ACHIEVES 100% JAUNDICE CLEARANCE. A SECOND PROGRESS REPORT
Purpose: Almost 10 years have passed since Esteves et al reported the first laparoscopic Kasai portoenterostomy (Lap-KP) for uncorrectable biliary atresia (BA). Subsequent reports suggested that outcomes did not compare with the results of open portoenterostomy. It lost favor with the International Pediatric Endosurgery Group in 2007, and lost official recommendation as a treatment for BA when a prospective study in Europe proved that survival with the native liver was worse after Lap-KP. However, having faith in the sound surgical techniques that Kasai devised, we began performing Lap-KP in 2009, adapting the principles of Kasai's original portoenterostomy. Because we have persevered with Lap-KP even after it lost official recommendation in Europe, we feel a strong commitment to inform our peers of our experience to justify performing Lap-KP.
Methods: To date, we have treated 11 uncorrectable type BA patients with Lap-KP. Our last case is still recovering from surgery with decreasing total bilirubin and was excluded. All our cases were non-syndromic with no evidence of cytomegalovirus infection, in other words “isolated” BA. In our Lap-KP, transection of the biliary remnant is shallow, and suturing of the portoenterostomy at the 2 and 10 o'clock positions where the original right and left bile ducts were, is shallow to the connective tissues, as in Kasai's original portoenterostomy, and at other positions we suture to the liver parenchyma around the transected biliary remnant. All data were collected prospectively.
Results: Data for cases 1 to 10 were: age at surgery was 59, 119, 72, 70, 54, 64, 29, 75, 57 and 65 (mean=66.4) days, respectively; weight at surgery was 4.3, 4.5, 5.0, 4.6, 4.0, 3.6, 3.3, 4.6, 4.5 and 3.6 (mean=4.2) kg, respectively. All 10 patients (100%) achieved jaundice clearance (total bilirubin < 1.2 mg/dL) over 42, 53, 36, 53, 49, 61, 84, 26, 57 and 29 (mean=51.7) days, respectively, requiring 31.5, 66.5, 31.5, 0, 98, 98, 126, 52.5, 110 and 61.5 (mean 67.6) mg/kg of steroid, respectively. Micro bile ducts were 200, 400, 100, 50, 50, 0, 30, 250, 250 and 50 (mean 138.0) micro millimeters in diameter, respectively. Currently, 8 patients (80%) remain jaundice-free with the native liver and 2 required liver transplantation because of liver cirrhosis/portal hypertension although one was jaundice-free and the other had total bilirubin of 1.6 mg/dL. Duration of follow-up in the 8 patients with native livers is: 3.7, 3.7, 3.5, 2.7, 2.2, 1.5, 0.2 and 0.1 (mean=2.2) years, respectively. Postoperative complications to date include 6 patients with cholangitis and 2 patients with esophageal varices diagnosed endoscopically.
Conclusion: Our data suggests that Lap-KP should be considered for reinstation as a first line treatment for BA, provided that the procedure follows our revival of Kasai's original techniques.
NOVEL HYBRID (MAGNET PLUS CURVE DISSECTOR) TECHNIQUE DURING TRANSUMBILICAL CHOLECYSTECTOMY: INITIAL EXPERIENCE OF A PROMISING APPROACH
Objetives: The use of two magnets in transumbilical cholecystectomy (TUC) improves triangulation and achieves optimal critical view. Nonetheless, the tendency of the magnets to collide hinders the process. In order to simplify the surgical technique, we have developed a hybrid model with a single magnet and a curved grasper.
Materials and Methods: Retrospective review of all TUC performed with a hybrid strategy in our pediatric population between September 2009 and July 2012. From 260 surgical procedures in which at least one magnet was used, 87 were TUC. From those, 62 were performed with the hybrid strategy, 33 in adults and 29 in pediatric patients. The technique combines the use of a magnet and a curved grasper. Through transumbilical incision, a 12 mm trocar and another flexible 5 mm are placed. Laparoscope with working channel uses the 12 mm trocar. The magnet is introduced to the abdominal cavity using the working channel to provide cephalad retraction of gallbladder fundus. Curved grasper is run by the assistant to mobilize the infundibulum across flexible trocar. The surgeon operates through the working channel of the laparoscope.
Results: Mean age was 14 years (4–17) and weight 50 kg (18–90). 65% were girls. The mean operative time was 62 minutes (50–70) and the critical view of safety was achieved in 100% cases. Instrumental collision or hands crossing were not seen. There were no intraoperative or postoperative complications. The hospital stay was 1.4±0.6 days and the median follow-up 201 days (42–429).
Conclusions: The hybrid technique, combining a single magnet and a curved grasper, simplifies transumbilical surgery. It seems feasible and safe for TUC, and potentially reproducible.
A PROSPECTIVE COMPARISON STUDY OF LAPAROSCOPIC VERSUS CONVENTIONAL KASAI PORTOENTEROSTOMY FOR CHILDREN WITH BILIARY ATRESIA
Objective: The outcome of laparoscopic Kasai operation treatment for children with biliary atresia is not clear, and lack large cases of prospective study. To evaluate the outcome of laparoscopic Kasai portoenterostomy for children with biliary atresia, we designed a prospective comparative clinical study.
Methods: Ninety-five patients with biliary atresia were operated in the Capital Pediatric Institution between September 2009 to August 2011. They were randomized into 2 groups preoperatively: laparoscopic group (LP group, n=48) and open group (OP group, n=47). In LP group, 4 patients transferred to open operation, the remaining 44 cases in LP group and 47 cases in OP group entered the study. The gender and age at operative of the LP group did not differ from that of OP groups (LP group F/M 21/23, age at operative was 64.5±20.41 days, OP group F/M 24/23, age at operative was 68.34±17.59 days, P=0.75&0.28). Intraoperative blood loss, operation time, postoperative hospital stay, normal food resumption, changes of liver function before and after operation, jaundice clearance rate, incidence of cholangitis rate, other complication and the mortality rate were analyzed.
Results: The operation time is significantly longer in the LP group than OP group (172.32±29 min vs 149.66±27.91 min, P<0.01) operation. Intraoperative blood loss is significantly less in the OP group (8.07±3.09 ml/17.55±3.59 ml, P<0.01), And normal food resumption is significantly faster in the OP group (2.80±1.36 days vs 3.47±0.65 days, P=0.02). But there was no statistical differences between the postoperative hospital stay of two groups (LP group 12.55±3.92 days, OP group 13.57±3.03 days, P=0.16). The median follow-up period was 16 months in the LP group and 17 months in the OP group. There are no significant differences in the postoperation jaundice clearance rate (LP group 43.18%, OP group 51.06%, P=0.45), incidence of cholangitis (LP group 59.09%, OP group 59.57%, P=0.96), native liver survival (after 6 months 81.82% in LP group, 85.11% in OP group, P=0.67; after 1 year 78.12% in LP group, 72.22% in OP group, P=0.58), and changes of liver function before and after operation between 2 groups.
Conclusion: The postoperative recovery of liver function, jaundice clearance rate, incidence of cholangitis rates and native liver survival rates in the LP group were not superior to the OP group. Patients with poor postoperative outcome still need liver transplantation, the advantage of minimally invasive operation cannot be reflected. Therefore, laparoscopic Kasai operation for biliary atresia requires careful selection.
LAPAROSCOPIC CHOLANGIOJEJUNOSTOMY FOR CHOLEDOCHAL CYSTS IN CHILDREN USING DOUBLE-HEMICIRCUMFERENTIAL RUNNING SINGLE-LAYER SUTURE
Background: The purpose of this study was to evaluate the feasibility and effectiveness of implementing a validated double-hemicircumferential running suture in laparoscopic cholangiojejunostomy for choledochal cysts (CDC) in children.
Methods: From October 2001 to October 2009, we performed laparoscopic “double-hemicircumferential” anastomosis for 218 patients with congenital choledochal Cyst. Early postoperative and follow-up results were analyzed.
Results: A total of 218 patients had reconstruction with this type of single-layer running suture (median age: 4.16 years, F/M: 162/56). The mean operative time was 2.95±0.91 hour, and average bleeding amount was 9.08±6.13 ml. The average postoperative hospital stay time was 7.41±2.39 days. The median follow-up period was 38 months. During follow-up, no biliary stenosis and cholangitis occurred, except two patients developed bile leak which stopped spontaneously after 10 days of drainage.
Conclusion: The double-hemicircumferential running suture technique has the advantages of easy to operate in laparoscopy, saving time and less complications, thus it is an effective improvement of cholangiojejunostomy.
LAPAROSCOPIC SURGERY IN INFANTS WITH OBSTRUCTIVE JAUNDICE
Objective: To summarize the experience of laparoscopy in infants (less than 5 months old) with obstructive jaundice since October 2010.
Methods: The clinical data of 96 cases of infants with obstructive jaundice were analyzed retrospectively. 11 cases which had been diagnosed with congenital biliary dilatation were performed with the laparoscopic choledochal cyst excision and Roux-en-Y hepaticojejunostomy. Other 85 cases, which with obstructive jaundice but without cholangiectasis, were performed with laparoscopic exploration and treatment.
Result: 11 cases with congenital biliary dilatation underwent the laparoscopic surgery successfully. All 11 cases were cured without long-term complications, even though 1 of them had suffered reoperation due to intestinal internal hernia which occured within three months after first surgery. Among other 85 cases, 13 of them had been diagnosed with intrahepatic cholestasis and then gradually restored after intra-operative gall duct irrigating. 72 cases had been diagnosed with biliary atresia, 20 of them were performed Kasai portoenterostomy with laparoscope, 5 cases were converted to laparotomy and also performed Kasai portoenterostomy, while 47 of them given up the surgery. Among 25 infants who underwent Kasai portoenterostomy, 22(88%) cases had bile-like defecation after surgery. A long-term follow-up of them showed that the jaundice of 17(68%) cases faded away while 8 of them didn't. Moreover, 1 infant was dead while 2 had liver transplant. All cases were performed laparoscopic surgery successfully, no serious operative or postoperative complication occurred.
Conclusion: It is a safe, available and minutely wounding method to diagnose and treat obstructive jaundice in infants.
LAPAROSCOPIC REDO HEPATICOJEJUNOSTOMY FOR POSTOPERATIVE ANASTOMOTIC STENOSIS IN CHILDREN WITH CHOLEDOCHAL CYSTS
Background: Laparoscopic hepaticojejunostomy has been widely utilized in children with choledochal cysts (CDC). However, there is no report on laparoscopic redo hepaticojejunostomy for CDC children with postoperative anastomotic stenoses. The current study is the first series to evaluate the feasibility and efficacy of laparoscopic redo hepaticojejunostomy for CDC children who have postoperative anastomotic stenoses.
Methods: Between January 2006 and November 2012, 20 CDC children (mean age: 6.15 years, range: 8 months-14 years, F/M: 12/8) who suffered from anastomotic stenoses after primary hepaticojejunostomies were referred to our hospital. The laparoscopic ductoplasties and redo hepaticojejunostomies were conducted for all children. The stenotic segments were split vertically to the most dilated portion of proximal hepatic duct along the midline of anterior hepatic duct wall. The widen hepatic duct and Roux jejunal loop were sutured transversely. The diameter of redo anastomnotic stoma was same to the diameter of the most dilated portion of proximal hepatic duct. The operative time, postoperative hospital stay, time to resume full feeding and perioperative laboratory results were evaluated.
Results: All patients suffered recurrent jaundice, abdominal pain and fever at postoperative 1 month to 6 years (mean: 1.77 years). The first clinical symptoms presented as jaundice in 9 patients (45%), abdominal pain in 9 patients (45%), and combined jaundice with abdominal pain in 2 patients (10%). The mean diameter of stenotic anastomotic stoma was 0.16 cm (0.1–0.3 cm). The mean maximal diameter of dilated proximal hepatic duct was 2.45 cm (2–3.5 cm). Intrahepatic duct stone formations were detected by ultrasonographic studies, CT scans and intraoperative intrahepatic duct investigations using telescope in 12 patients (60%). All patients showed significantly elevated serum bilirubin with aberrant liver functions (mean serum bilirubin: 117.8 umol/L, ALT: 142.5 U/L, AST: 143.5 U/L, ALP: 522.0 U/L, and GGT: 494.6 U/L). All patients successfully underwent laparoscopic redo hepaticojejunostomies without conversions to open procedures. The mean diameter of redo anastomotic stoma was 2.45 cm (2–3.5 cm). The mean operative time was 1.93 hours (1.75–2 hours). Intraoperative blood loss was minimal. No blood transfusion was required. The average postoperative hospital stay, resumption of feed, and duration of drainage were 5.95, 2.2 and 2.9 days respectively. Median follow-up period was 40 months (1–82 months). No mortality or morbidities of recurrent anastomotic stenosis, bile leak or cholangitis was observed. Liver function parameters reversed to normal levels after surgery (p<0.001).
Conclusions: Laparoscopic redo hepaticojejunostomies for CDC children who had anastomotic stenoses after primary hepaticojejunostomies is feasible and safe. It minimizes the surgical trauma in redo surgery and obtains good mid-term outcomes.
LAPAROSCOPIC NEAR-TOTAL PANCREATECTOMY FOR PERSISTENT HYPERINSULINEMIC HYPOGLYCEMIA OF INFANCY
Aim: To present the technique and outcomes of laparoscopic near-total pancreatectomy for persistent hyperinsulinemic hypoglycemia (PHH).
Methods: The operation was performed using three ports. Fixation sutures of the stomach to the abdominal wall for stomach traction were used. The pancreas was dissected free from the spleen and splenic vessels and was mobilized beyond the right side of the superior mesenteric vein. The head of the pancreas was transected by using the Harmonic Scalpel (Tokyo, Japan), leaving only 1 cm of the pancreas along the duodenal C-loop.
Results: From October 2007 to July 2012, 9 patients underwent laparoscopic near-total pancreatectomy for PHH.
Mean age was 41.3 days±23, mean weight was 4200 g±597. Mean operative time was 155±43 minutes. Blood lost was not significant. Mean postoperative time was 15 days±5.
Plasma glucose level returned to normal range in 8 patients. In one patient, plasma glucose level was 0.1 mmol/l before operation and increased to 3.2 mmol/l after operation. This patient was lost for follow-up after 6 months.
Conclusion: Laparoscopic near-total pancreatectomy can be a safe, effective procedure for small infants with PHH.
TWO DECADES OF LAPAROSCOPIC NISSEN IN INFANTS AND CHILDREN; A CRITICAL ANALYSIS AND REVIEW
Laparoscopic Fundoplication for gastroesophageal reflux disease has become a common procedure performed in infants and children over the last 20 years. This report analyses a 20 year experience with nearly 2000 consecutive laparoscopic Nissen fundoplications.
Methods: From 1992 to 2011 data was kept prospectively on all patients undergoing laparoscopic fundoplication. Ages ranged from 5 days to 18 years and weight from 1.2 to 120 kg. 1928 fundoplications were performed by or under the direct supervision of a single surgeon. Pts were divided into groups based on age (Table). Data on indications, demographics, post-operative course, and long-term follow-up were kept prospectively on each patient.
Results: Average operative time decreased from 109 for the first 30 cases compared to 35 minutes for the last 30. 283 procedures were redos, 85 had previous open and 198 laparoscopic. Intra-operative and post-operative complications were 0.13% and 4.0% respectively in the primary group but was 2.2% and 4.2% in the redo group. Average time to discharge for the primary group was 1.1 days. Wrap failure rate for primary fundoplications was 4.6 percent and was highest in < 6 month age group. The failure rate in the redo group was 6.8%. The most common causes of wrap failure were hiatal hernia 46% and slipped Nissen 34%.
This study shows in a large operative experience over 20 years that laparoscopic fundoplication is safe and effective in the pediatric population. Technical considerations are paramount to improved outcomes. Clinical results are favorable to the traditional open fundoplication but with a significant decrease in morbidity and hospitalization. Laparoscopic Nissen fundoplication should be considered the gold standard for anti-reflux procedures.
LAPAROSCOPIC VERSUS OPEN FUNDOPLICATION IN INFANTS: A NATIONWIDE EVALUATION OF 6,398 PEDIATRIC OPERATIONS
Background: Over the past decade, laparoscopic fundoplication (LF) has gained momentum as an alternative technique for treatment of antireflux in infants versus open fundoplication (OF). Our aim was to compare the two techniques using a large nationwide database.
Methods: The Nationwide Inpatient Sample, which captures approximately 20% of all United States inpatient admissions, was queried from 2004–2010 for pediatric patients under 2 years of age who underwent LF or OF using ICD-9-CM coding. Demographics and outcomes were compared using Chi-square, Fisher's exact test and Wilcoxon rank sums.
Results: In total, 6,398 infants met inclusion; 2,102(33%) underwent LF and 4,296(67%) underwent OF. From 2004–2006, 3,115 fundoplications were performed, 703(23%) underwent LF and 2412(77%) underwent OF. From 2008–2010, 2,499 fundoplications were performed, 1091 (44%) underwent LF and 1408(56%) underwent OF. Overall, the mean age was older for infants undergoing LF than OF (80±152 days old v. 57±133 days old; p<0.0001); there was no difference in gender or race. Seventy percent of infants also underwent gastrostomy tube placement, which did not differ between those undergoing LF or OF. A higher proportion of infants undergoing LF had neurologic disorders than OF (17.2% v. 13.3%; p<0.0001). Postoperative pulmonary complications were lower in those undergoing LF than OF (4.0% v. 5.3%; p=0.0222), as well as decreased postoperative wound, soft tissue, and intrabdominal infections (1.7% v. 3.2%; p=0.0003), and postoperative gastrointestinal complications such as ileus and obstruction (1.6% v. 3.6%; p<0.0001). Procedural bleeding was lower in those undergoing LF compared to OF (1.1% v. 2.4%; p=0.0004). Those undergoing LF had a lower overall postoperative complication rate (8.8% v. 14.7%; p<0.0001) and in hospital mortality (1.1% v. 3.2%; p<0.0001) than those undergoing OF. Days to fundoplication from admission was shorter for LF versus OF (24±37 v. 31±43; p<0.0001) and length of stay was significantly shorter in those undergoing LF versus OF (37±48 days v. 50±58 days; p<0.0001). Total mean hospital charges were lower in those undergoing LF versus OF ($205, 027±289, 080 v. $228,485±273,948; p<0.0001). Both operations were performed predominately in urban hospitals; however a higher proportion of LF (90%) were performed at teaching hospitals than OF (84%) (p<0.0001). LF was also performed more often in areas of high median household income based on zip code than OF (40% v. 32%; p<0.0001).
Conclusions: With the largest evaluation of anti-reflux surgery in infants to date, the outcomes of LF in infants mimic those in adults with decreased individual and overall postoperative complications in comparison to OF. However, LF has not become the predominate technique despite its outcomes and increase in incidence over the last 7 years. Although LF appears to lead to decreased cost and length of stay, strong conclusions cannot be made due to the complicated long preoperative hospitalizations of the patients in the national sample.
OPERATIVE INTERVENTION FOR INTUSSUSCEPTION VARIES BY AGE AND LACKS A MINIMALLY INVASIVE APPROACH - A NATIONWIDE EVALUATION
Background: Intussusception is the most common cause of intestinal obstruction in children under 3 and often requires an emergency surgery. A laparoscopic approach for surgical treatment of intussusception has been proposed but it has yet to become mainstream practice or studied on a nationwide level. Our goal was to utilize a national database to evaluate operative intervention for intussusception including a laparoscopic approach.
Methods: The Nationwide Inpatient Sample, which captures approximately 20% of all US inpatient admissions, was queried from 1998–2010 for patients under 18 years with a diagnosis of intussusception using ICD-9-CM coding. Age associated with operative intervention and utilization of laparoscopy was used for unweighted statistical analysis.
Results: A total of 8,138 patients met inclusion with intussusception, 4938 (61%) treated non-operatively (NON) and 3200 (39%) required operative intervention (OI). OI incidence varied by age (Figure 1). Population was stratified by age into those < 1 yr old (Infant; n=3461), 1–3 yr old (Toddler; n=3203), and ≧4 yr old (School-age; n=1474). Of the patients who required OI, 108 (3.4%) utilized laparoscopy, which was significantly higher in School-age (6.7%) versus Toddler (3.9%) and Infants (1.6%) (p<0.0001). Overall, OI was lower in Toddler compared to Infant (29% v. 46%; p<0.0001) and School-age (29% v. 47%; p<0.0001). When patients with pathologic lead points such as Meckels or neoplasm were removed from the inclusion, OI remained lower in Toddler compared to Infant (27% v. 44%; p<0.001) and School-age (27% v. 38%; p<0.0001), but became lower in School-age compared to Infant (38% v. 44%; p=0.0007). In children undergoing OI, 1849 (58%) underwent reduction of intussusception with bowel manipulation without resection (MAN), 1089 (34%) underwent bowel resection (RSN), and 262(8%) did not specify beyond exploratory laparotomy. Of those undergoing MAN, only 42(2.3%) utilized laparoscopy, with a higher proportion in School-age (4.8%) than Toddler (2.6%) or Infant (1.5%) (p=0.0074). Of those undergoing RSN, only 25(2.3%) utilized laparoscopy, with a higher proportion in School-age (4.5%) than Toddler (2.3%) or Infant (0.6%) (p=0.0007). RSN was lower in Toddler compared to Infant (26% v. 33%; p=0.0004) and School-age (26% v. 62%; p<0.0001), and lower in Infant compared to School-age (33% v. 62%; p<0.0001). When patients with pathologic lead points were removed, RSN remained lower in Toddler compared to Infant (23% v. 31%; p<0.0001) and School-age (23% v. 59%; p<0.0001), but became lower in Infant compared to School-age (31% v. 59%; p<0.0001).
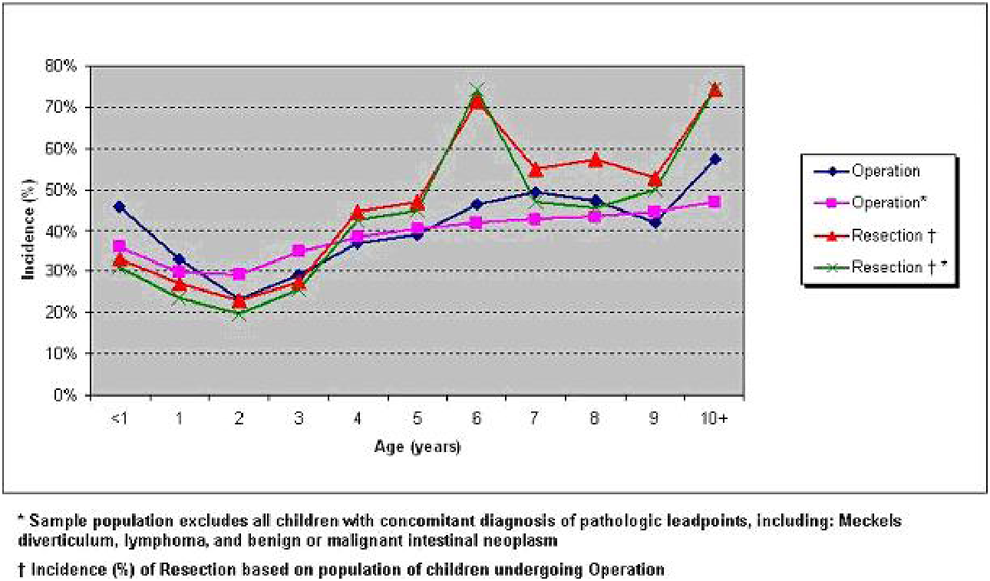
Operative intervention for intussusceptions by age.
Conclusions: The overwhelming majority of patients undergoing operative intervention for intussusception have an open operation; however the use of laparoscopy increases with age. Operative intervention and subsequent bowel resection for intussusception has a bimodal distribution with peaks in children under 1 and those 4 and older, which remains significant even without pathologic lead points.
Urogenital MIS
Background: Surgery for neurogeinc bladder patients usually include complicated reconstructive procedures, such as bladder augmentation, ureteral reimplantation and mitrofanoff procedures. Laparoscopic attempts are not regularly applied in this condition. With increased experience in reconstructive surgery, we started laparoscopic ileal cystoplasty, ureteral reimplantation and appendicovesicostomy in selected patients. The initial results are quite satisfactory.
Methods: From Feburary 2011 to Feburary 2012, there are 5 neurogenic bladder patients, 4 girls and 1 boy with a mean age of 10.3 years, who underwent laparoscopic ileal cystoplasty, ureteral reimplantation (4 bilateral, 1 left ureteral reimplantation), and appendicovesicostomy. One case (bilateral ureteral reimplantation) was converted to open. In the other 4 patients which were successfully completed laparoscopicaly, intestinal reanastomosis and ileal patch detubularization and anastomosis was performed by exteriorizing the bowel loop outside the abdomen through the umbilical port site. Creation of a large cystotomy, the circumferential enterovesical anastomosis, ureteral reimplantation and appendicovesicostomy were all performed intracorporeally. Double J were inserted in the ureters and removed 6–8 weeks postoperatively. The mitrofanoff openings were fashioned in the right lower abdomen.
Results: For the 4 successful laparoscopic cases, the operative times were 14, 13, 11, and 10 hours respectively. The recovery were uneventful and CIC were started 3 weeks after the operation.
Conclusions: Complicated laparoscopic reconstruction for neurogenic bladder patient is feasible and safe. In its initial stage, the operative time is relatively long. And more cases are needed to fully access its benefits in this condition.
RETROPERITONEOSCOPIC NEPHRECTOMY AND HEMINEPHRECTOMY IN CHILDREN PLANNED, PERFORMED, AND MANAGED BY SENIOR PEDIATRIC SURGICAL TRAINEES
Introduction: We compared a series of retroperitoneoscopic nephrectomies and heminephrectomies (Rneph) planned, performed, and managed by senior pediatric surgical trainees with conventional open nephrectomies and heminephrectomies (Oneph) performed by board certified pediatric surgeons with respect to perioperative morbidity, safety, and learning curves.
Methods: From 2004 through 2008, all Oneph were performed by 4 board certified pediatric surgeons through a conventional flank incision (n=20). In 2009, 4 trocar Rneph was introduced with all preoperative surgical planning, surgery, and management performed by 5 senior pediatric surgical trainees under the supervision of a board certified pediatric surgeon (n=11). In this study, senior pediatric surgical trainees were aged 33 to 37 all with 5 to 8 years experience of hands on pediatric surgery, having assisted or performed at least 30 cases of major laparoscopic/thoracoscopic surgery, and having performed experimental surgery including at least 20 cases of major laparoscopic/thoracoscopic surgery at our animal laboratory.
Results: In Oneph, there were 14 nephrectomies and 6 upper pole nephrectomies for multicystic dysplastic kidney (MCDK) n=6, duplex kidney (n=6), ectopic ureter (n=4), and hydronephrosis (n=4). In Rneph, there were 9 total nephrectomies and 2 upper pole nephrectomies for MCDK (n=3), duplex kidney (n=3), ectopic ureter (n=3), and hydronephrosis (n=2). At surgery, mean age was 41 (range: 4–109) months in Oneph, and 52 (range: 23–123) months in Rneph; mean body weight was 14 (range: 9–27) kg in Oneph and 18 (range: 13–32) kg in Rneph. One Rneph case required conversion to Oneph. Overall mean operating time was 137 (range: 85–290) mins in Oneph and 197 (range: 116–341) mins in Rneph (although mean duration dropped from 249 mins for the first 5 cases to 153 mins for the latter 6). Mean blood loss was 17 (range: 1–55) mL in Oneph and 10.3 (range: 2–40) mL in Rneph; no transfusions were required. No intraoperative complications arose in either group. Two patients (one Oneph and one Rneph) who underwent partial heminephrectomy developed transient urinomas postoperatively that resolved conservatively. Duration of postoperative bed rest was 1.0 day in Oneph, and 0.6 days in Rneph. Differences in mean analgesic requirement were statistically significant. In Oneph, 21.5 (range: 10–40) μg/kg of Fentanyl was used versus 4.1 (range: 0–20) μg/kg in Rneph (p<.05), and duration of postoperative non-steroidal anti-inflammatory suppository usage was 2.3 (range: 0–5) days in Oneph, and 0.9 (range: 0–2) days in Rneph (p<.05). Full oral feeding was possible after a mean of 1.6 (range: 1–2) days in Oneph and 1.2 (range: 1–2) days in Rneph.
Conclusions: There would appear to be no major disadvantages associated with retroperitoneoscopic nephrectomy/heminephrectomy being planned, performed, and managed by senior pediatric surgical trainees. Thus Rneph may prove to be a valuable practical procedure that senior trainees can master. Patients would benefit from significantly less physical discomfort as indicated by requirement for analgesia, and more efficient management.
VIDEO-ASSISTED TREATMENT OF WILMS TUMOR AND RENAL CARCINOMA IN CHILDREN: AN 8-YEAR EXPERIENCE
Background: Laparoscopic procedures for the treatment of adult urological tumors have been reported since the past decade, with good outcomes following careful indications. Only after 2003, pioneer Brazilian surgeons (Duarte & DÉnes) started managing pediatric nephroblastoma laparoscopically, after SIOP's chemotherapy protocols, with functional results similar to conventional surgery results in stage I.
Objectives: The purpose of this study is to present our experience of video-assisted nephrectomy using 3 ports for suspected Wilms tumors, clinical stages I and II.
Patients and Methods: This prospective controlled study included 21 children with non-metastatic renal tumors preoperatively treated with vincristine and actinomycin D (SIOP's) from April 2004 to February 2012, in whom the tumor diameters declined to 8 cm or less. Using a transperitoneal approach, 3 trocars, 3- or 5-mm instruments, special transparietal stitches and probes for exposure, and harmonic or bipolar devices, we performed a radical nephroureterectomy including perirenal lipectomy, selective lymphadenectomy, adrenalectomy if necessary, and clipping the margins of the dissected area. Very large renal veins were ligated. The tumors were extracted intact inside plastic bags through a limited Pfannenstiel incision.
Results: The tumors and lymph nodes were removed without intraoperative complications, ruptures or significant bleeding. The pseudocapsule involving the tumor after chemotherapy helped the dissection. Three children needed a 4th trocar, introduced where the suprapubic incision would be made. In the 2 cases that had adrenalectomy and in other 2 children, the pathological study confirmed tumor outside the renal capsule or invading small hilar veins (stage II). In one boy, the pathology confirmed a clear cell carcinoma. One girl had compromised lymph nodes, upstaging her to stage III. All other children were stage I Wilms tumors. The postoperative course was uneventful, and all the patients went home by the 3rd day. All patients remained on chemotherapy or radiotherapy according to their staging status. No recurrences, port implants or long-term complications have been registered after 10 months to 8 years of follow-up.
Conclusions: We conclude that video-assisted radical nephrectomy for renal tumors is feasible and safe in selected children after chemotherapy, including stages I, II and III and even renal carcinoma. All the oncological techniques of the classic open approach can be done, with all the advantages of the minimally invasive surgery and improvement in the quality of life. Other studies are needed to evaluate the role of MIS in preoperatively suspected stage III tumors.
UPPER POLE HEMINEPHROURETERECTOMY IN CHILDREN - LAPAROSCOPY VERSUS OPEN SURGERY
Aim: To evaluate the safety and feasibility of laparoscopic upper-pole heminephroureterectomy (HNU) in pediatric patients with duplex kidneys in comparison to open surgery.
Patients and Methods: From 2007 to 2011, 27 patients underwent HNU. By DMSA isotope scan hypofunctioning of ipsilateral moieties was detected in all cases. The patients were divided in laparoscopic (LHNU) and open surgery (OHNU) groups. Laparoscopic heminephroureterectomy was performed by transperitoneal approach in 10 girls and 5 boys with a mean age of 33 months (range 9–108). All procedures were performed using three port technique. Open surgery was performed in 10 girls and 2 boys with mean age of 29 months (range 7–174) by retroperitoneal approach in all cases. Renal ultrasound was done at 3 months postoperatively and repeated after 6 months together with renal scintigraphy.
Results: Mean operative time in the LHNU and OHNU groups was 148 minutes (range 100–220, CI 95% 129–167) and 124 minutes (range 100–150, CI 95% 115–133) respectively. In the LHNU and OHNU groups, mean analgesic requirement in the LHNU and OHNU groups was 2.8 days (range 2–4, CI 95% 2.4–3.2) and 3.7 days (range 3–5, CI 95% 3.3–4.1), mean hospital stay was 4.0 days (range 2–8, CI 95% 3.2–4.8) and 5.1 days (range 3–8, CI 95% 4.3–5.9) respectively. No intraoperative or major postoperative complications occurred. No conversion to open surgery was necessary in the LHNU group. Statistical analysis showed no statistical significant difference (p>0.05) in operating time between groups, while mean hospital stay (p=0.048) and analgesic requirement (p=0.005) were significant. The function of the remnant pole was preserved in all patients. Follow-up ultrasound showed asymptomatic cystic structures in one patient.
Conclusion: The laparoscopic upper-pole heminephroureterectomy is a safe and feasible procedure, even in infants. It is associated with minimal morbidity, reduces analgesic requirement and hospital stay and provides excellent cosmetic results. Operative time is acceptable. In our opinion it should be the preferred option for heminephroureterectomy in children.
TRANSPERITONEAL LAPAROSCOPIC ANDERSON-HYNES PYELOPLASTY IN INFANT AND CHILDREN
Objective: To evaluate the safety and outcome of transperitoneal laparoscopic pyeloplasty with a direct approach to the ureteropelvic junction obstruction (UPJO) through the mesenterocolic space.
Methods: 131 male and 42 female children were diagnosed with UPJO. Their ages ranged from 2 months to 16 years (mean, 5.5 years). Thirty six UPJO were found on the 173 patients, including 129 left unilateral PUJO, 36 right unilateral UPJO and 8 bilateral UPJO. All of them were treated with Anderson-Hynes transperitoneal laparoscopic dismembered pyeloplasty.
Results: 170 patients underwent laparoscopic operations except 3 patients were transferred opening operations. The duration of operations ranged from 44 min to 128 min. Blood lose during operation was 15 to 40 ml. Obstruction of double J catheter was noted on 5 patients (2.8%). Complications occurred in 2 cases (1.16%). Transient anastomotic stoma obstruction was observed in 6 cases (3.47%). The patients were followed up for 6 to 96 months. There is no case of secondly operation.
Conclusions: Transperitoneal AndersonHynes laparoscopic pyeloplasty is safe and effective for the treatment of UPJO in infant and children.
THE USE OF DIFFERENT PELVIS URINE DRAINAGES FOR LAPAROSCOPIC PYELOPLASTY
Objective: To evaluate the benefits, drawbacks and indication of different pelvis urine drainages after laparoscopic pyeloplasty.
Methods: A total of 90 patients (97 sides) who had undergone laparoscopic pyeloplasty between January 2010 and February 2012 were divided into nephrostomy external drainage group (61 sides), long-term double J catheter internal drainage group (23 sides) and short-term double J catheter internal drainage group (13 sides). To compare the difference of postoperative complications and successful rate with three groups.
Results: The incidence of postoperative gross hematuria in nephrostomy external drainage group was lower than long-term double J catheter internal drainage group (P<0.01) and short-term double J catheter internal drainage group (P<0.05). The total incidence of postoperative complications in nephrostomy external drainage group was lower than long-term double J catheter internal drainage group and short-term double J catheter internal drainage group (P<0.01). The incidence of urinary infection in nephrostomy external drainage group was lower than long-term double J catheter internal drainage group (P<0.05). The incidence of drainage tube blockage and omentum prolapsus in nephrostomy external drainage group was lower than short-term double J catheter internal drainage group (P<0.05). And there was no significant difference of anastomosis obstruction incidence and postoperative successful rate in three groups (P>0.05).
Conclusions: Nephrostomy external drainage was associated with lowest rates of postoperative complications after laparoscopic pyeloplasty. However, three urine drainages have their own indication. The most suitable urine drainages could be selected by actual situation.
INTRAVESICAL LAPAROSCOPY FOR COHEN URETERAL REIMPLANTATION UNDER PNEUMOVESICUM
Aims: To report our experience of intravesical laparoscopy Cohen ureteral reimplantation under carbon dioxide insufflation of the bladder (pneumovesicum).
Methods: 26 boys and 17 girls with ureteral and bladder malformation, ages ranged from 4 months to 9 years (mean 3.7 years). Among them, 25 patients were single side vesicoureteral junction obstruction, 18 primarily vesicoureteral reflux (VUR). Tile laparoscopic procedure was preceded by distention of the bladder with saline and insertion of a 5 mm portover the bladder dome under cystoscopie guidance. The bladder was then insufflated with CO2. The laparoscopic operation procedures were similar as open technique. Bladder drainage by a urethral catheter was maintained for five to seven days postoperatively.
Results: 42 patients were accomplished except one transferred opening. The duration of operations ranged from 57 min to 260 min. Six patients suffered from slightly hematuria, which spontaneous cured within two days postoperatively, except one administered haemostatic. All patients were followed up from 3 to 26 months. 28 ureters return to normal, 12 are better than preoperative, 2 are no significant change. No one occurred VUR.
Conclusions: Intravesical laparoscopy for Cohen urethral reimplantation can be performed safely, effectively and learned easily with routine laparoscopic surgical techniques under pneumovesicum, achieving a high success rate similar as the open technique but with minimal invasiveness and much faster recovery. However, it is very important to choose the adaptation cases.
A NEW SURGICAL TREATMENT METHOD OF STAG-HORN UROLITHIASIS IN CHILDREN
Children constitue approximately 1–3% of all patients suffering from urolithiasis. It is estimated that only 20% of this group require surgical intervention. There are 3 basic treatment methods of urolithiasis: ESWL, PCNL, and URSL. Only in case of massive stag-horn lithiasis a traditional open surgery is justified.
Objective: Analysis of treatment results of patients with stag-horn urolithiasis treated with an innovative method combining traditional pyelolithotomy and endoscopic technique.
Materials and Methods: The retrospective analysis was conducted on age, symptoms, diagnostics, surgery and treatment results.
In 2009–2012 120 children suffering from urolithiasis underwent medical treatment. 8,3% of patients age 3–15 were diagnosed with stag-horn lithiasis: 8 with unilateral and 2 with bilateral. All patients suffered from recurrent urinary system infection and pain from lumbar region. All of them underwent abdominal ultrasound examination, plain abdominal X-ray and urography. In all cases calculi filled at renal pelvis and at least two calyces. All children with stag-horn lithiasis required surgical treatment. 9 underwent elective surgery, and one required urgent surgery because of urosepsis and complete blockage of urine outflow by stag-horn calculus. All patients had received preoperative antibiotics. The surgical procedure included pyelotomy removal of calculi from pelvis by forceps under direct vision and endoscopy of the whole pelvis and each calyx by nephroscope. The presence of calculi required lithotripsy by ultrasound waves. Minor calculi were simultaneously removed by suction pump. After removing all stones DJ catheter was left. Renal pelvis was stitched in a typical way. In 3 cases Hynes Anderson pyeloplasty was conducted.
Results: 8(66,6%) out of 12 treated patients were completely stone free. Ultrasound examination showed that residual fragments (app. 6–8 mm in diameter) in calyces remained in 4 (33.3%) patients. 3 of them were treated with ESWL and one expelled stones without medical intervention. After the surgery one patient required transfusion of one unit of PRBCs. One patient was diagnosed with symptoms of urosepsis on the third day after the surgery.
Conclusion: Treatment of stag-horn lithiasis in children still remains a great challenge for pediatric surgeons. The presented method is a good alternative to the traditional pyelocalycotomy as well as minimally invasive PCNL. Both require multiple incisions of renal parenchyma. They are also risky because of possible bleeding and formation of parenchymal scars. The presented method enables to remove all calculi from pyelocalycal system very precisely without the necessity of renal parenchyma incision. The combination of traditional open surgery with endoscopy of calyces and lithotripsy is a good alternative to stag-horn calculi treatment in children.
LAPAROSCOPIC VAGINOPLASTY WITH A SIGMOID GRAFT THROUGH UMBILICAL SINGLE-INCISION HYBRID TRANSPERINEAL APPROACH - OUR INITIAL EXPERIENCE
Background: For better cosmetic appereance, the attempting to reduce abdominal incisions of laparoscopic surgery has been thought recently. Therefore, investigators have begun to carry out the procedures through a single incision or natural orifices endoscopic surgery instead of using the conventional laparoscopic surgery. The authors describe transumbilical single-incision hybrid transperineal laparoscopic surgery as a novel approch for vaginal reconstruction with a sigmoid segment.
Methods: From August 2010 to October 2011, 15 adolescents with Mayer–Rokitansky–Kuster–Hauser (MRKH) syndrome underwent laparoscopic sigmoid vaginosplasty using a combined transumbilical single-incision and transperineal approach. A multiport system (TriPort) was placed through the umbilicus single incision for the main laparoscopic procedures. Another 12 mm trocar as the assisted working port was inserted into pelvic cavity transvaginal dimple between the urethra, bladder and rectum. After mobilizing the descending colon and sigmoid, the sigmoid and rectum were dissected with an endoscopic linear cutter (endo-GIA). A segment of sigmoid approximately 12–15 cm in length with its vascular pedicle still intact was removed extracorporally through umbilicus incision. The distal oral was temporarily sealed, while the proximal oral was inserted the anvil of a curved intraluminal stapling device (CDH29). Under the laparoscope, the segment of sigmoid was reversed and pulled through the vaginal vestibule incision to create a neovagina. The rectosigmoid anastomosis was performed using a CDH29 through the anus and rectum.
Results: All the procedures were successfully performed without any intraoperative morbidity. The average operative time and hospital stay were 151.5±34.2 minutes and 7.4±3.2 days. The only postoperative complications were one case with stress ulcer and one case with umbilical infection. This operation had excellent cosmetic outcome, including good lubrication, adequate length and breadth, and appearance and physical functions similar to natural vagina.
Conclusions: Transumbilical single-incision hybrid transperineal laparoscopic sigmoid vaginoplasty offers a feasible scarless approach for women with MRKH syndrome. The favorable cosmetic results would be used as an alternative to conventional laparoscpy.
Gastrointestinal & Hepatobiliary II
MINIMALLY INVASIVE GASTRIC TRANSPOSITION IS A SAFE AND EFFECTIVE ALTERNATIVE TO OPEN SURGERY IN CHILDREN
Gastric transposition is established as a method of esophageal replacement when salvage of the native esophagus has failed. The open procedure includes laparotomy and (often) thoracotomy incisions, which are associated with significant morbidity. We have moved to performing this operation laparoscopically with a view to avoiding the trauma of open access. The aim of the present study was to review our experience of laparoscopic-assisted gastric transposition at Great Ormond Street Hospital (London, UK), and assess outcomes in children that have undergone the procedure.
We have performed laparoscopic-assisted gastric transposition in 19 patients over the last 10 years (January 2003 to date). There were 12 male and 7 female patients with mean age of 3.5 years (range: 0.6 to 15.2). Indications for surgery were long-gap esophageal atresia (n=11; 57.9%), caustic esophageal stricture (n=5; 26.3%), esophageal stricture following repair of atresia (n=2; 10.5%), and dysmotile/atonic esophagus (n=1; 5.3%). Associated congenital anomalies were present in 9 patients (47.4%).
All operations were performed individually or jointly by 6 consultant surgeons. A pneumoperitoneum of 10 mmHg was established via a 10 mm umbilical port, and the stomach was mobilized laparoscopically using 5 mm instruments. Following pyloromyotomy (n=10; 52.6%) or pyloroplasty (n=9; 47.4%), a tunnel was developed in the posterior mediastinum to allow the gastric fundus to be drawn to the neck and sutured to the cervical esophagus. Nine patients (47.4%) had thoracoscopy to facilitate the reconstruction. The mean anesthetic time was 354 minutes (range: 240 to 565), and 3 laparoscopic procedures (15.8%) had to be converted to open gastric transpositions. Post-operatively, patients were electively paralyzed and ventilated in the intensive care unit (mean duration of ventilation: 5 days; range: 2 to 9), and then transferred to the surgical ward (mean length of hospital stay: 19 days; range: 8 to 36).
Follow-up data (mean duration: 34 months; range: 1 to 85) was obtained in 12 patients (63.2%). From these patients, 75% (n=9) were on oral feeds and thriving without feeding tubes at last follow-up. Long-term feeding outcomes were classified as “excellent” (normal eating habits) or “good” (occasional dysphagia; small/frequent meals) in 58.3% (n=7) of patients available to follow-up. Complications included anastomotic leak (n=1; 8.3%), anastomotic stricture (n=2; 16.6%), hiatus hernia (n=2; 16.6%), and delayed gastric emptying (n=2; 16.6%). There were no deaths.
The present retrospective study suggests that laparoscopic gastric transposition is a safe and effective alternative to open surgery in pediatric patients. The minimally invasive procedure has similar outcomes to open gastric transposition while minimizing the significant trauma associated with the open procedure.
EXTRACTION OF ESOPHAGEAL FOREIGN BODIES: RIGID VS. FLEXIBLE ENDOSCOPY
Introduction: Foreign body (FB) ingestion is a common and potentially serious problem in children. Both rigid (RE) and flexible (FE) endoscopic techniques are used for removal of esophageal FBs; however, there is no consensus amongst pediatric surgeons regarding the best method. This study reviewed our experience managing esophageal FBs using both techniques.
Methods: After IRB approval, a 12-year retrospective review of children admitted with a diagnosis of esophageal FB between January 1999 and March 2012 was undertaken. Clinical data, management techniques, and complications were abstracted. Differences between these two groups were compared with standard statistical methods.
Results: 657 children were treated for esophageal FB ingestion, of which 366 (56%) were treated with flexible endoscopy (FE). The most frequently ingested item was a coin (84%), a penny being the most common coin (59%). More than one coin was found in 5% of children. FBs were lodged in the upper third of the esophagus in 78%, the middle third in 9%, and distal third in 13%. Underlying esophageal abnormalities such as congenital esophageal stricture, vascular rings, esophagitis, and achalasia were found in 3.3%. Food was the most common FB in this group. Either RE or FE were performed based upon surgeon preference. There were no significant differences between RE and FE in any of the variables examined (Table 1). Failure to remove the FB with one technique led to utilization of the other, seen in 17 children, resulting in an overall initial 97% success rate. There was no procedure related mortality.
Comparison of Intraoperative, Postoperative Events and Complications Between RE vs. FE
Conclusions: Based on our data, esophageal foreign bodies may be successfully removed with either RE or FE. Since treatment failures were managed with conversion to the other technique, both procedures should be included in the training curriculum.
Background and Aim: Percutaneous endoscopic gastrostomy (PEG) represents the gold standard procedure when a gastrostomy is required in pediatric patients. However, displacement of stomach for scoliosis or thorax deformities leads to technical difficulties of PEG. Laparoscopic assisted percutaneous endoscopic gastrostomy (LAPEG) has emerged as a viable alternative procedure to the open gastrostomy for these patients. This study aimed to establish the safety and the complications of LAPEG in a single center experience.
Materials/Methods: Data regarding operative techniques, intra- and post-operative complications, device replacement, outpatients clinic follow-up (1, 6, and 12 months) of patients who made gastrostomy in our institution between September 2000 to November 2011 have been prospectively collected. These patients were divided in two groups: PEG group and LAPEG group. The indication of the procedures was mainly determined by the preoperative upper gastrointestinal contrast studies. PEG procedures was carried out by introducer method using the Funada-type appliance, and in LAPEG the stomach was laparoscopically sutured to the abdominal wall and then the gastric tube was inserted by puncture under endoscope observation.
Results: We intended for 265 patients performed PEG or LAPEG except 46 open gastrostomy cases in the study period, whose average age was 4.2 years old at the operation. 87 patients underwent PEG and 178 patients did LAPG. 92 patients performed simultaneously the anti-reflux surgery at the gastrostomy. Three intraoperative complications had mesenteric vessel injury in PEG group, transverse colonic injury in PEG group, difficulty to make gastrostomy for far-off distance between stomach and abdominal wall in LAPEG group. Postoperative complications had tube dislodgement for insufficient formation of the fistula happened in 3 cases at the first time of the exchange. No significant differences between two groups were found in local complications at the follow-up (e.g., infection, hypergranulation tissue, hemorrhage, tube dislodgement and leak of gastric contents). Four patients underwent surgical revision (2 PEG, 2 LAPEG) for uncontrollable leak of gastric contents.
Conclusions: PEG and LAPEG represent safe alternatives for pediatric patients requiring gastrostomy. In our experience no significant differences occurred between two techniques in terms of local complications at the follow-up. The incidence of tube dislodgement was low but it is necessary to attend the tube dislodgement in the exchange. We believe that these two procedures are complementary and should be both currently handled in a pediatric surgery center.
LAPAROSCOPIC PYLOROMYOTOMY: A RESTORED SURGICAL TRAINING OPPORTUNITY
Background & Aims: Laparoscopic pyloromyotomy (LP) is established as a treatment for pyloric stenosis, with recent metanalyses reporting outcomes comparable with open pyloromyotomy (OP). Critics of LP contend improved outcomes have only been achieved by consultant-led operating at the expense of registrar training. This study's primary aim was to assess the impact of LP on operative training, since its introduction in our centre in 1999. In addition, outcome of LP and OP were measured.
Methods: A single-centre retrospective review was performed of all primary LPs and OPs between Jan 1999 and Nov 2012. Data collected included surgical approach, surgeon grade, postoperative stay, and complications. Parametric data were compared using Fisher's exact tests and non-parametric data using Wilcoxon rank-sum tests; P<0.05 considered significant.
Results: 421 primary pyloromyotomies were performed: 133 open and 288 laparoscopic. Overall M:F ratio was 4: 1, and gender distribution did not differ significant between LP and OP groups (LP: M 233 and F 55 vs. OP: M 115 and F 18; P=0.17). Similarly, median age at surgery was not statistically different (LP: 35 days vs. OP: 37 days; Wilcoxon rank-sum, P=0.11).
Percentage of primary pyloromyotomies performed laparoscopically trended up over the 14 years, from 21% in 1999 to 100% in 2012. Percentage of LPs performed by registrars also trended up, from 0% in 1999 to 95% in 2012. Overall, registrars performed 175/288 (61%) LPs, but performed only 31% of the “1st 100” LPs vs. 81% of the “most recent” 100 LPs (see figure).
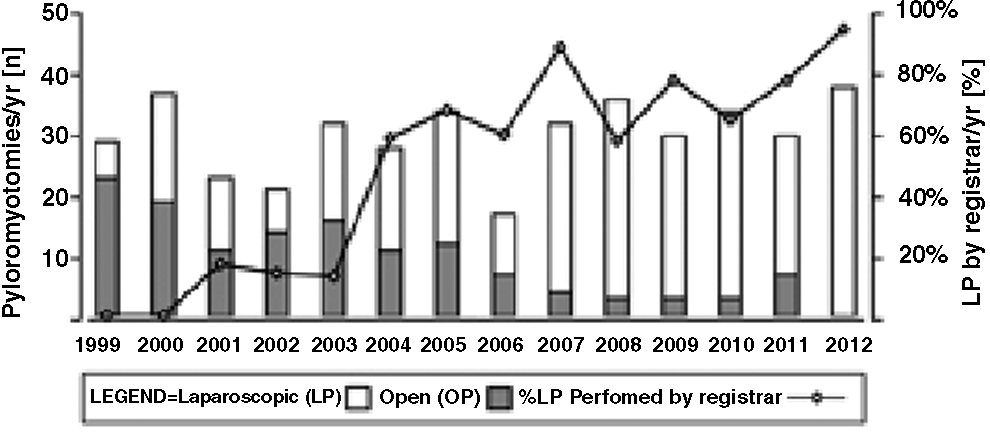
With the exception of shorter length of stay post LP (Wilcoxon rank-sum, P<0.001), no outcome measures differed significantly between LP and OP groups. Mucosal perforation occurred in 8 patients (LP 3/283 vs. OP 5/133; P=0.12). 2/288 LP patients incurred duodenal perforation unrelated to myotomy splitting, rather as a result of the left handed grasper. 13/14 patients requiring re-operation underwent LP, but this result did not reach significance (LP: 13/288 vs. OP: 1/133; P=0.07). Indications for reoperation post-LP were: inadequate pyloromyotomy (7/288), herniated omentum (5/288), and incisional hernia (1/288). The incidence of complications did not differ between consultant vs. registrar performed cases (mucosal perforation, P=0.56; reoperation, P=1.00).
The data were assessed for evidence of a learning curve. Comparison of the “most recent 100” LPs and OPs showed no significant difference in rates of mucosal perforation (LP 1/100 vs. OP 5/100; P=0.21) or reoperation (LP 5/100 vs. OP 1/100; P=0.21). Similarly, the incidence of complications did not differ between the “1st 100” LPs (majority consultant performed) and “most recent” 100 LPs (majority registrar performed; P=1.00).
Conclusions: These data suggest our institution established its expertise in LP through a consultant led service. However, it has become the norm for LPs to be performed by registrars. Importantly, increased registrar operating has not compromised outcome. Rather, procedural efficacy and patient safety are sustained by an “institutional learning curve” afforded by consultant training and/or supervision. Finally, experience gained during LP provides valuable preparation for future more complex endoscopic neonatal procedures. Thus, the surgical training opportunity of LP has been restored.
LAPAROSCOPIC PYLOROMYOTOMY IN 457 CASES: A RETROSPECTIVE ANALYSIS IN SINGLE-CENTER EXPERIENCE
Background: Laparoscopic pyloromyotomy (LP) for the treatment of hypertrophic pyloric stenosis (HPS) is one of popular laparoscopic procedures in pediatric surgery, and this procedure is used for resident training in many centers. This study was undertaken to investigate the influence of experience with LP on operative time, complication rate, learning curve and postoperative hospital stay for a large number of patients.
Methods: Between January 1999 and October 2012, 457 children underwent LP for HPS. These procedures involved 13 surgeons, 5 consultants, and 8 trainees. The outcome of all infants was retrospectively analyzed.
Results: Laparoscopic pyloromyotomy was successfully completed in 452 patients (98.9%). Intraoperative complication occurred in 10 (2.2%) patients (mucosal perforation, 6; serosal injury to the duodenum, 3; bladder perforation, 1). All were immediately recognized during operation and uneventfully repaired. Six patients (1.3%) required revision pyloromyotomy because of insufficient pyloromyotomy. Wound complications occurred in 6 (1.2%) patients (wound infection, 2; omental henia, 2; wound bleeding, 2). The median hospital stay after surgery was 4 days. Five patients transfered to open procedure during the first 12 cases due to technique insufficient or instruments problem. Intraoperative complication and insufficient pyloromyotomy always occurred in the initial series in each trainee and rarely occurred in the later cases. After about 15 LPs, the operative time was approximately 20∼30 min. The length of postoperative hospital stay also dropped with increasing experience.
Conclusions: Laparoscopic pyloromyotomy has an excellent success rate with low morbidity. This procedure seems to be well teachable. After about 15 LPs, the number of complications decreased significantly and the operative time was approximately 20∼30 min stably.
LAPAROSCOPIC PARTIAL SPLENECTOMY: A DECREASED BLEEDING BY PREOPERATIVE EVALUATION WITH COMPUTED TOMOGRAPHY ANGIOGRAPHY WHILE MAINTAINING SPLENIC FUNCTION
Background: A partial splenectomy is a good way to prevent postsplenectomy infections by preservation of the immune role of the spleen for children patients. Although a laparoscopic total splenectomy is a safe and feasible treatment modality, the laparoscopic approach has not been generally adopted for a partial splenectomy because of technical difficulties in controlling intraoperative parenchymal bleeding during splenic transection. We report herein our experience.
Methods: From May 2010 to July 2012, we successfully performed 8 consecutive laparoscopic partial splenectomies (LPS) at our institution and achieved meticulous hemostasis using harmonic scalpel or silk ligature according to the instruction of preoperative anatomic evaluation with computed tomography angiography (CTA). All data were prospectively collected and reviewed retrospectively. The indications were: portal hypertension and hypersplenism (n=3), hereditary spherocytosis (n=4) and torsion and infarction of migrative spleen (n=1). The surgical technique consisted of seven steps: preoperative individual evaluation of splenic anatomy by CTA, patient positioning and trocar placement, mobilization of the spleen, vascular dissection, parenchymal resection, hemostasis of the transected edge, and removal of the specimen. Follow-up was from 0.5 to 2.5 years. Data included preoperative and postoperative hemoglobin, erythrocyte count, splenic size, operative time, blood loss, complications, and length of stay.
Results: Eight patients with a median age of 6.9 years (6.9±3.8 years) successfully underwent laparoscopic partial splenectomy with a preoperative CTA determined upper-pole remnant of 10% to 30% and preservation of the blood supply through the upper short gastric arteries. The mean preoperative spleen length was 15.9 cm (15.9±2.1 cm). Mean operative time was 118 min (118±38 min). Median blood loss was 107 ml (range 40–300 ml). Comparison of haematological indexes between preoperation and postoperation was shown in Table 1. There was no intraoperative complication and conversions. No postoperative mortality occurred. Median hospital stay was 7.5 days (7.5±1.8 days). Approximately one-fourth of the spleen left on the basis of the short gastric arterial supply in all operations. Subtotal splenectomy appears to control hemolysis while maintaining splenic function.
Comparison of Haematological Indexes Between Preoperation and Postoperation
*P>0.05; **P<0.05.
Conclusions: On the basis of our experience, better understanding of the splenic segmental anatomy by preoperative CTA evaluation, need of splenic conservation, and advances in laparoscopic skills has made laparoscopic partial splenectomy a preferred treatment for hypersplenism or haematological diseases in children, with a decreased bleeding and risk of postsplenectomy infections, short hospital stay, and superior cosmesis.
Background: With the advent of preoperative chemotherapy (CTX) for neuroblastomas, we have observed great or complete reduction of the tumors and metastasis, and the development of a pseudocapsule that favors an easier and safer surgical dissection. These factors would allow the use of videosurgery in the treatment of neuroblastomas, applying safe oncological principles, as shown by our experience and by a few authors in the recent literature.
Objectives: A retrospective cohort study to report the role and outcomes of minimally invasive surgery (MIS) in the treatment of neuroblastomas, after a 16-year experience, probably the largest series in South America.
Patients and Methods: From 1996 to 2011, 101 children aged 2 months to 12.4 years (76 boys, 45 girls) have been benefited by the use of MIS in their treatment for thoracic or abdominal neuroblastomas and ganglioneuroblastomas (n=13) in three institutions, by the same surgeon. After careful preoperative evaluation, tumors that were considered resectable through MIS had to be no larger than 6–8 cm in diameter, non-Stage 4, limited to abdomen or thorax alone. Thirty-two patients required more than one operation, resulting 133 procedures. They included pre-CTX biopsies (25) or staging (18), complete tumor extractions (43), video assisted extractions (12), second-look or re-do operations (22) and treatment of associated conditions (cholecystectomy-2, bowel occlusion by adhesions-1, oophoropexy-5, persistent chylothorax-1, ventriculo-peritoneal catheter management-2, gastrostomy-2).
Results: All patients except 3 could have the procedures accomplished thoracoscopically or laparoscopically without conversion. These children had intense adhesions to major vessels or liver hilum, not resectable through MIS. Complications related to videosurgery were minor, in the first cases: bleeding at trocar site (1), liver perforation by the assistant (1), incisional hernia (3). Local recurrences occurred only in stage 3 periaortic tumors (2/11) and were treated through laparotomy. Other complications were related to the diseases. Early postoperative CTX at 2nd PO day was started in 5 children (stage 2) without problems. Some resected masses showed no live tumor after CTX (n=17, 19.3%). After a follow-up period of 1–16 years, mortality depended on staging and pathology, ranging from 0% (ganglioneuroblastoma) to 21.8% (stage 3 neuroblastomas). No cases of port site implants.
Conclusions: MIS can be safely applied for diagnosis and treatment of selected cases of neuroblastomas post-chemotherapy and ganglioneuroblastomas, and for some associated conditions, avoiding morbidity of traditional laparotomies and improving quality of life. A larger series is needed to confirm the benefit of early postoperative CTX after MIS, in overall survival.
MAJOR COMPLICATIONS AFTER LAPAROSCOPIC-ASSISTED PULL-THROUGH FOR HIRSCHSPRUNG'S DISEASE
Purpose: To analyze the major complications after laparoscopic-assisted pull-through for Hirschsprung's disease.
Materials and Methods: We performed a retrospective study of 238 pediatric patients receiving laparoscopic-assisted pull-throughs for Hirschsprung's disease in our department from March 2008 to March 2012. Regular biological-feedback trainings and anal dilations were performed for 6 months.
Results: Our single institutional experience with laparoscopic-assisted pull-through for Hirschsprung's disease revealed major complications as follows: 1) Enterocolitis, occurred in 27 children (11.3%): 24 of them within 6 months after surgeries and 3 of them 1-year later; 8 patients experienced twice or more and 3 deaths occurred (1.3%). One child with enterocolitis was relieved by colostomy. 2) 17 children had mild to moderate post-operational soiling, 9 of which resolved within 6 months and 8 had gradually relieved symptoms after 18 months. 3) 19 mild anastomotic strictures occurred one month after surgery and experienced relief in 3 months after anal dilation. 4) Increased defecation rates were noted in 13 patients during the first month after surgery ranging from 3–4 times per day. 12 of them decreased to 1–3 times per day 6-month later. 5) Constipations occasionally occurred in the first month after pull-through procedures. Three children who had defecation intervals for 2–3 days had relieved symptoms after anal dilatation treatments. 6) One patient experienced infection of the rectal sheath which was recoverd 2 weeks after antibiotic therapy. 7) 5 children had rectal mucosa prolapse, 2 of which releived after conservative therapy and 3 of them received surgical therapies. 8) No adhesive intestinal obstructions, anastomotic leakages or wound infections happened in our group of patients.
Conclusion: As a minimal invasive surgical approach, laparoscopic-assisted pull-through brings less injury to patients with Hirschsprung's disease. But the higher rates of post-operational enterocolitis and soiling compared to conventional procedures (e.g. Duhamel procedure) should be concerns to pediatric surgeons. Regular follow-ups are crucial for at least 6 months.
Gastrointestinal & Hepatobiliary III
SINGLE-INCISION LAPAROSCOPIC DUCTOPLASTY FOR CHOLEDOCHAL CYSTS COMBINED WITH HEPATIC DUCT STRICTURES
Background: Single-incision laparoscopic hepaticojejunostomy has been utilized in children with choledochal cysts (CDC). The current study is the first series to evaluate the feasibility and efficacy of single-incision laparoscopic ductoplasty (SILD) for CDC children with hepatic duct strictures.
Methods: Fourteen CDC children with hepatic duct strictures who underwent SILD between April 2011 and November 2012. A vertical umbilical skin incision was made. An extra-long 5-mm 30° laparoscope was placed through the camera port which located at the midline fascial incision. Two 3-mm conventional straight laparoscopic instruments were inserted through working ports which were placed lateral to the camera port at the ends of the umbilical incision which was stretched transversely. With a series of transabdominnal suspension sutures, the cysts were dissected from proximal anterior wall to distal end and then to the posterior wall. The proximal cyst was dissected to the hepatic hilum. The intrahepatic ducts were routinely investigated using the telescope. The ductoplasty, i.e. splitting the hepatic duct vertically and suturing transversely, was performed. The protein plugs/calculi were evacuated by irrigation. Roux loop and wide hepaticojejunostomy were performed. Early postoperative and follow-up results were compared with the data in our historical report.
Results: All patients (F/M: 9/5) successfully underwent SILD without conversions. According to the Todani's classification, 8 of 14 patients were Type IV and 6 was Type I CDC. All patients were cystic dilatations. The minimal diameter of stenotic common hepatic duct was 0.1–0.3 cm. Protein plugs were detected in 6 patients. The mean age at operation in SILH group was 1.53 years (1.68 months-9.33 years). It was comparable to 6 months-12 years in our historical conventional laparoscopic ductoplasty (CLD) group.1 The mean operative time was 3.17 hours, significantly shorter than 4.3 hours in our previous CLD series 1 (p<0.001). Intraoperative blood loss was minimal. Postoperative hospital stay, time to resume full diet, duration of drainage in SILD were 5.42, 2.30 and 3.10 days respectively, which did not differ from those in CLD in our historical controls 1 (p=0.84, 0.08, 0.68 respectively). The diameter of anastomotic stoma was 1.0–1.5 cm. The median follow-up period was 8.5 months. No mortality or morbidities of anastomotic stenosis, bile leak, intrahepatic reflux, or cholangitis was observed. Liver function reversed to normal levels after operations (p<0.001).
Conclusions: In experienced hands, SILD is safe and effective to correct the hepatic duct strictures. Its short-term results are comparable to CLD.
Reference:
1. Li L, Liu SL, Hou WY et al. Laparoscopic correction of biliary duct stenosis in choledochal cyst. J Pediatr Surg 2008;43(4): 644–6.
LAPAROSCOPIC PYLOROMYOTOMY UNDER SPINAL ANESTHESIA: IS IT FEASIBLE?
Background: The use of general anesthesia (GA) in infants is receiving increasing attention due to the potential effects on brain development. Most agents used for GA are considered to be neurotoxins and affect developing brains in experimental models. Therefore, there has been a push to perform more procedures under spinal anesthesia to avoid the detrimental effects of GA. Pyloromyotomy is a common procedure performed in the neonatal or early infant period, and open operations have been done under a spinal anesthetic in the past (SA). However, most operations are now being performed laparoscopically. There are no reports of laparoscopic pyloromyotomy (LP) performed under SA. We present our experience with LP and SA and discuss feasibility.
Methods: A retrospective analysis was performed on a consecutive series of patients who underwent a LP at our institution. There was no pre selection of patients for the type of anesthesia used. An ‘intent to treat’ type analysis was utilized for grouping the patients, and GA was compared to SA. SA was administered using 0.75% bupivacaine and midazolam in all cases, using standard weight based calculations. Data regarding patient characteristics, operative intervention, complications, and post operative course were collected. Statistical analysis was performed with a student's t test.
Results: Twelve cases had attempted SA for the LP, 9 were successful. During the same time, 12 cases underwent LP under GA. The cohort was not different for age in weeks nor weight at time of surgery. We found no difference in the time for the surgery between the groups (29.25 minutes SA vs. 28 minutes GA), nor was the time to the first feed (PACU feeding for all cases), or the post operative LOS (1.083 vs. 1.25 days) different. The time to leave the OR after the procedure was over was significantly shorter for the SA group (14 min. vs. 28 min, p<0.001). There were no complications from the SA, however three cases had to be converted to GA as in two we could not obtain intrathecal access, and one did not tolerate the insufflation during the case.
Conclusions: It is feasible and safe to perform laparoscopic pyloromyotomy under spinal anesthesia. There was no increase in the operative time, and the post operative awakening was more rapid. Given the increasing concern over the use of GSA in infants, consideration may be given to use of SA for LP.
LAPAROSCOPIC OVARIAN TISSUE PRESERVATION IN GIRLS WITH RISK OF OVARIAN FAILURE FOLLOWING CHEMO/IRRADIATION FOR PRIMARY MALIGNANCY
Background: In young females considered to be long-term cancer survivors, aggressive chemotherapy and irradiation treatment may lead to gonadal failure and infertility. The putative aim of laparoscopic ovariectomy is to enable the process of fertility restoration either by transplantation of the frozen-thawed ovarian tissue or further into the future by in-vitro maturation of the frozen-thawed oocytes, followed by routine in vitro fertilization.
Patients and Methods: Retrospective date base review of Ethics Board approved procedure for ovarian tissue cryopreservation performed in female patients undergoing chemo/irradiation for diagnosed malignancy. Between 1998–2011, 52 females, median age 13.9 (5–18 y) underwent ovarian tissue preservation. Twenty-five patients had hematological malignancies, sixteen had bone tumors, nine had ovarian tumors and twelve intra-cranial lesions.
Results: Fifty-one underwent laparoscopic harvesting of ovarian tissue and in one patient the ovary was preserved during repair of inguinal hernia. Average OR time was 30 min, dissection was carried on avoiding use of devices that may induce collateral thermal injury. Adolescent females with larger volume of ovarian tissue underwent partial ovariectomy while pre-pubertal girs with small ovaries underwent complete ovariectomy. Ovarian evacuation require endo-bag, fresh tissue is sampled for pathological examination and bulk of ovarian tissue forward to laboratory in maximum 30 min. No complications were recorded. All patients had a benign postoperative course and were discharged at next day. In follow up (median 5.7 y), no wound infection or port-side hernias were detected and cosmetic results were superior.
Conclusions: Laparoscopy has gained acceptance as the ideal diagnostic and therapeutic method with high efficiency, low morbidity, quicker postoperative recovery and excellent cosmetic results. This especially important in young oncological patients, survivors and winners who need reaffirmation of their body image and self esteem. Since human ovarian tissue containing primordial follicles has been reported as successfully cryopreserved, we conclude that laparoscopy safely serve as important link in this new process that may enable hope for parenthood.
TECHNICAL IMPROVEMENTS IN THE LAPAROSCOPIC PORTOENTEROSTOMY FOR BILIARY ATRESIA
Background: Since the first description of the laparoscopic portoenterostomy (LPE) for biliary atresia (BA) in 2001, many centers have accomplished the operation with variable success. Most have reported short series of patients, including children operated along the learning curve, large anesthetic times, after late diagnosis, or not following adequate hints recommended at the first publication. Moreover, one of the most important objectives of the Kasai operation is to facilitate LTX, to benefit over 80% of the patients born with BA.
Objectives: The authors present new trends in the LPE, new tricks and hints to allow easy and fast operations and facilitate LTX, emphasizing a careful selection of the patients.
Methods: Since the year 2002, after the initial description of LPE, the authors have considered the importance of short operative times to reduce the influence of anesthetics and CO2 infusion to the small babies, and have developed new technical improvements aiming different purposes. All of them, at the end, would make the operation easy and fast: (1) to maximize exposure of the liver hilum: good preoperative management to keep the bowel empty, no use of nitrous oxide, fine needle aspiration of eventual colonic air, fixing the liver border or gallbladder remnant high under the diaphragm with a sliding knot, transparietal downward traction of the duodenum, a fine metallic epigastric 1.5 mm aspirator/retractor, cut off the pseudolobe that the liver sometimes develops in front of the porta hepatis (PH); (2) to avoid unnecessary adhesions and facilitate vascular dissection on LTX: preserve the gallbladder remnant in situ, no dissection of the liver pedicle proximally to the PH, where the dissection should be focused, perform the jejunal Roux-en-Y and mesenteric closure extracorporeally through the umbilical site, using running sutures or staplers, and marking the points carefully to avoid rotation; (3) to make hepato-enterostomy clean and faster: terminal anastomosis, 6–8 sliding extracorporeal sutures through the right trocar, with monofilament sutures, apnea during needle performances, no drains. Only children under 2 months of age were selected. Consent forms were available from all families.
Results: In the last 25 cases, the operations had a mean operative time (OT) of 100 minutes (85–150 min). During a follow-up period of 1–10 years, the 26 patients in whom the OT was no more than 2 hours, 36% are anicteric, 15(57%) of patients had LTX, all after one year of age and most of them because of portal hypertension. The overall biliary drainage rate is 82% (21/26). The LTX teams have been satisfied with the abdominal conditions of the patients, reported fewer transplantation complications and had preferred the LPE than the open Kasai patients.
Conclusions: Applying our surgical protocols, the functional results of LPE are similar or slightly better than the published data for open surgery, with lower morbidity and better cavity for LTX. Transplantation data is still missing to confirm the final influence of LPE in overall survival of children with BA.
A PROSECTIVE STUDY OF LAPAROSCOPIC TRANSANAL ENDORECTAL PULL-THROUGH FOR SUBTOTAL COLECTOMY IN HIRSCHSPRUNG'S DISEASE: ANASTOMOSIS USING LONG CUFF OR SHORT CUFF?
Objectives: Routine transanal endorectal pull-through is commonly practiced laparoscopically for treatment of longer segment aganglionosis. For this procedure, using long cuff or short cuff for anastomosis has not reach a consensus. We undertook a prospective randomized trial to assess if different cuff length might influence early and late outcomes of this procedure.
Methods: Between 2009 and 2012, 54 children preoperatively and postoperatively diagnosed with longer aganglionic segment above the proximal rectosigmoid colon were randomized into 2 groups before the laparoscopic endorectal pull-through: long cuff group (n=28) and short cuff group (n=26). Patients with total colonic aganglionosis or short/classic segment aganglionosis were excluded. Postoperative hospital stay, complications, and defecation function were analyzed.
Results: The mean age at surgery, mean operating time, mean postoperative hospital stay and mean intra-operative blood loss were not significantly different between the two groups. The median follow-up period was 22 months in the long cuff group and 24 months in short cuff group. Postoperative complications included perianal excoriation, anastomotic leak, constipation and anal stricture were comparable in the two groups. Soiling problems occurred only in two cases of short cuff group. Incidence of enterocolitis in long cuff group was 3.5% (1/28), which was significantly lower than that of short cuff group 15.4% (4/26). As for defecation frequency, no significance was observed in the first two months after surgery between the two groups. However, in the third months and sixth month, mean defecation frequency was significantly lower in long cuff group than that of short cuff group. In 12th and 18th follow up, though percentage of normal defecation in long cuff group is a bit higher than that of short group (82.1% vs 77.0% in 12th month and 85.7%vs 84.6% in 18th month), the difference is minimal.
Conclusions: Compared with short cuff anastomosis, laparoscopic transanal endorectal pull-through with a long cuff decrease incidence of enterocolitis and anastomotic leak but not the other complications. Long cuff anastomosis had a better defecation performance in the first 6 month of follow up. But in 12th and 18th month, defecation performance was similar in two groups.
Keywords: Hirschsprung's disease, transanal Soave, long cuff, short cuff, complications, defecation function.
ILEAL POUCH ANAL ANASTOMOSIS IN PEDIATRIC FAMILIAL ADENOMATOUS POLYPOSIS: A 24 YEAR REVIEW OF OPERATIVE TECHNIQUE AND PATIENT OUTCOMES
Purpose: Total proctocolectomy with ileal pouch anal anastomosis (IPAA) is the traditional operative procedure for pediatric patients with familial adenomatous polyposis (FAP). Over the years, IPAA has been performed with many technical variations (1 or 2 stage reconstruction, mucosectomy with hand sewn versus stapled anal anastomosis, laparoscopic or open). We reviewed the past 24 years of operative results and outcomes with IPAA in pediatric FAP patients in an attempt to determine whether these operative variations were significant.
Methods: All FAP patients, <20 years of age, presenting to our institution between 1987 and 2011 were retrospectively reviewed. 127 patients with FAP were treated surgically, 24 of which underwent resection other than IPAA. 7 patients underwent IPAA at an outside institution, resulting in 96 patients in the IPAA cohort. Primary outcomes included post-operative complications, long term bowel function, and polyp recurrence.
Results: Median age at IPAA was 16 years with median follow-up of 6 years. 29 patients had a 1-stage IPAA, 65 patients a two-stage procedure, and 1 patient underwent a 3-stage procedure. Patients with the 1-stage IPAA demonstrate better long term bowel control compared to the 2-stage IPAA (89% vs. 64% no incontinence, p=0.018). However, patients in the 1-stage group suffered increased short-term post-operative complications, such as anastomotic leak (17% vs. 0%, p=0.002) and re-operation for complications (21% vs. 5%, p=0.02). Polyp recurrence at the anal anastomosis occurred in 23% of 1-stage patients and 10% of 2-stage patients. When comparing open procedures to minimally invasive techniques, 67 patients had an open procedure, 26 underwent a laparoscopic approach, and more recently 3 patients have undergone single incision laparoscopic IPAA. Median length of stay was shorter for patients that had laparoscopic IPAA (7 vs. 9 days, p<0.001). 87% of the laparoscopic group reported no incontinence versus 67% of the open group (p=0.09). There were no statistically significant differences in short-term complications, polyp recurrence, or long-term continence. 85 patients had a mucosectomy with hand sewn anastomosis, while only 11 had a stapled anal anastomosis, precluding meaningful statistical comparison.
Conclusion: 1-stage IPAA in children with FAP is associated with better bowel control long term, but increased short term post-operative complications, re-operative rate, and polyp recurrence. The effect of short-term complications on long-term bowel function requires further investigation. In experienced hands, open versus laparoscopic IPAA is equivocal with regards to short-term complications, continence, and polyp recurrence. We reserve the use of 1-stage IPAA for a very select group of patients with the understanding that short-term complications are significantly increased compared to 2-stage procedures.
MID- TO LONG TERM OUTCOMES OF LAPAROSCOPY-ASSISTED ANORECTOPLASTY: A COMPARISON STUDY WITH POSTERIOR SAGITTAL ANORECTOPLASTY
Purpose: The aim of this study is to compare the mid- to long term outcomes between laparoscopic-assisted anorectoplasty (LAARP) and posterior sagittal anorectoplasty (PSARP) for children with high anorectal malformations (HARM).
Methods: Sixteen HARM children who underwent LAARP between September 2002 and October 2008 were reviewed. The outcomes were compared with those of 10 HARM children who underwent PSARP in the same period in our center. The sacral ratio (SR), age at operation, operative time, postoperative hospital stay and complications were evaluated. Bowel functions were assessed by the Krickenbeck score system.
Results: Mean operative time of the LAARP was significantly shorter than that of PSARP group (191.9±17.2 vs 254.0±55.7 mins). The postoperative hospital stay in LAARP group was significantly shorter than those in the PSARP group (13.4±4.1 vs 19.6±3.6 days). The incidence of postoperative infections was significantly higher (30% vs 0) in patients after PSARP. The overall morbidity rate was not significantly different between the two groups. Fourteen of 16 patients were followed up successfully in LAARP group while those were 9 patients in PSARP group. Median follow up period was 6.0 years (range 4–10) in LAARP patients and 7.5 years (range 4.3–9.6) in PSARP patients. Total continence was found in 3 (21.4%) of 14 patients after LAARP and one (11.1%) of 9 after PSARP. The rate of voluntary bowel movement, soiling (grade 1, 2 & 3) were similar in both groups. No patient suffered constipation after LAARP and one patient experienced grade 2 constipation after PSARP.
Conclusions: LAARP is an less invasive procedure when compared with PSARP for HARM. The mid- to long term functional outcome after LAARP was comparable to those after PSARP.
A COMPARISON OF THE EFFECTIVENESS OF THE LAPAROSCOPIC-ASSISTED SOAVE AND DUHAMEL PROCEDURES FOR CHILDREN WITH LONG AGANGLIONIC SEGMENT
Department of Pediatric Surgery Department, Wuhan Union Hospital, Huazhong University of Science and Technology, China
Purpose: Versatile pull-through techniques have been performed for long segment aganglionosis disease. However, no current consensus on a superior operative procedure exists. Our study evaluates the comparative effectiveness of the laparoscopic-assisted Soave and Duhamel procedure in the treatment of long segment aganglionosis.
Methods: Based on the preoperative radiographic diagnosis and operative biopsy findings, 84 patients were diagnosed as long segment aganglionosis between August 2007 and October 2012. Total colonic or total intestinal aganglionosis were excluded. Laparoscopic-assisted Duhamel procedure was performed in 34. 50 patients were treated with laparoscopic-assisted Soave procedure. In each group, the patients were subdivided into two small groups according to the extent of colectomy based on aganglionosis. Operation time, intraoperative blood loss, hospital stays, postoperative complications and a range of functional outcomes were analyzed to evaluate of the effectiveness of the laparoscopic-assisted Soave and Duhamel procedure.
Results: Long segment aganglionosis of Duhamel (group D) and Soave group (group S) were subdivided into laparoscopic left hemicolectomy subgroup (group D1 and group S1) and laparoscopic subtotal colectomy subgroup (group D2 and group S2) according to the affected segment of the aganglionosis. Left hemicolectomy groups included patients with aganglionic segment distal to the middle of descending colon, subtotal colectomy groups included patients with aganglionic segment in splenic flexure colon, transverse or ascendant colon. There were no difference between the four groups regards to bodyweight, operative age, sex, intraoperative blood loses and hospital stays. Mean operative time for Duhamel procedure (132 min) (group D) was significantly less than that of Soave procedure (176 min) (group S). As for postoperative complications, there was no anastomotic stricture or leak in group D but one anastomotic stricture and one leak occurred in group S. In the group D1, the incidence of enterocolitis (16.7%), recurrent constipation (5.6%), incontinence (5.6%) and fecaloma (5.6%) was not significantly different from those in group S1 (15.4 %, 7.7%, 7.7% and 3.8%, respectively). However, in group D2, the incidence of enterocolitis (12.5%) and recurrent constipation (6.3%) were significantly lower than those in group S2 (20.8% and 12.5%, respectively). Incidence of incontinence was similar in group D2 and S2 (6.3% vs 8.3%). At two weeks and four weeks follow-up, all patients had an increased frequency of defecation, and defecation frequency in Group S was significantly increasing than that in group D. 3 months after the operation, the percentage of normal defecation was significantly higher in Duhamel group than in Soave group (P<0.05). At half a year's follow-up the difference was still significant (P<0.05).
Conclusion: For patients with long segment aganglionosis, the performance of laparoscopic Duhamel procedure was similar to Soave procedure in aganglionic segment distal to the middle of descending colon. However, in aganglionic splenic flexure colon, transverse or ascendant colon, the laparoscopic Duhamel procedure had fewer postoperative enterocolitis and recurrent constipation. Better defecation outcome was observed in Duhamel procedure compared with those of Soave procedure.
ABSTRACT WITHDRAWN
Thorax
CURRENT PATTERNS OF PRACTICE AND TECHNIQUE IN THE REPAIR OF ESOPHAGEAL ATRESIA AND TRACHEOESOPHAGEAL FISTULA: AN IPEG SURVEY
Introduction: Optimal surgical treatment of infants with esophageal atresia (EA) and tracheoesophageal fistula (TEF) remains controversial. Practice patterns vary due to a lack of definitive studies identifying specific techniques or management styles that improve outcomes. In order to better understand the variability in management of EA/TEF patients, we surveyed the IPEG membership.
Methods: An online-based survey was conducted in 2012 and sent to all IPEG members. The survey gathered demographic, technical and management preferences.
Results: The survey was completed by 170 surgeons from 31 countries. A majority of respondents practiced in an academic/university setting (86%) and performed 1–3 EA/TEF repairs annually (67%). Those practicing for over 15 years comprised 39% of the study group, followed by those practicing 6–10 years (24%), 0–5 years (22%) and 11–15 years (15%).
The utilization of a thoracoscopic approach was reported by half of the respondents with a frequency of 1–3 (76%), 4–6 (17%), greater than 7 (7%) per year. Most (65%) learned the thoracoscopic technique after completing fellowship. Low birth weight, congenital heart disease, long gap length and compromised physiologic status were identified as the most common exclusion criteria for thoracoscopic repair. The thoracoscopic repair was almost uniformly performed via an intrapleural approach (96%), in contrast to the open repair, in which 89% perform the operation extrapleural. The use of tissue sealants to enforce the anastomosis, or synthetic material to interpose the esophageal and tracheal closures, was rarely utilized (12% and 5%, respectively).
Pre-operative bronchoscopy was routinely performed by 70%. Size 4–0 to 5–0 absorbable suture (PDS, Vicryl) were predominate choices of suture for EA repair (77% and 88% respectively). Post-operative chest tube/drain and trans-anastomotic tube placement was utilized by 83%. A normal esophagram was required by 85% to initiate oral feeding with 93% performing the esophagram on post-operative day 5–10. Sixty-six percent initiated trans-anastomotic feeds prior to obtaining an esophagram. Post-operative antibiotic use was common (76%) and varied from less than 1 day to greater than 14 days. Acid suppression medication was utilized by 76% with duration ranging from 7 days to lifelong. For long gap EA, spiral myotomies were rarely preformed (10%) and gastric transposition was the favored method for esophageal replacement (66%).
Anastomotic strictures were preferentially treated by balloon dilatation (74%) over Savory (13%) or Maloney (6%) techniques.
Conclusions: Considerable variability existed among the IPEG membership in the treatment of patients with EA/TEF. The identification of this variance is the first step in the creation of future studies to identify best practices.
COMPLICATIONS OF RECURRENT PECTUS EXCAVATUM REPAIR: WHICH PATIENTS ARE AT RISK?
Objective: To evaluate whether initial operation type affects complications for minimally invasive repair of recurrent pectus excavatum (PE), and to highlight complications that occur during repair of recurrent PE. Additionally, we evaluated whether complications were more frequent in patients with simple or complex recurrences.
Methods: An IRB-approved retrospective chart review was performed of patients who underwent minimally invasive repair for recurrent PE. Comparisons were made between those who previously underwent minimally invasive versus open procedures. Separate comparisons (irrespective of initial operation) were made between patients with simple (return of “cup” or “saucer” appearance) and complex recurrence (severe excavatum-carinatum, osteochondrodystrophy). Complications of redo repairs were stratified into intraoperative, early (within one month of operation) and late groups.
Results: Of 113 patients with recurrent PE from June 1987 to September 2012, 60 (53.1%) had one or more previous minimally invasive (closed) procedures; 53 had open procedures prior to recurrence. Patients who underwent an open procedure had complex recurrences significantly more often than those who initially underwent the closed procedure (77.4% vs 13.3%, χ2(1)=44.97, p<.001). Osteochondrodystrophy was seen in 77.4% of previous open patients versus 6.7% of previous closed patients (χ2(1)=58.68, p<.001). Complex adhesions occurred in 58.3% of previous closed cases compared to 39.6% of previous open cases (χ2(1)=3.94, p=.047). Estimated blood loss (EBL) was higher during redo operations than in primary repairs; mean EBL was 67 ml (range 10–500) in patients who initially underwent closed repair and 43 ml (range 10–300) for initial open repair, although initial operation type was not found to be a factor associated with greater than expected EBL (24.4% closed vs 14.6% open; χ2(1)=1.242, p=.265).
Complex recurrences were present in 49 patients (43.4%). There was no statistically significant difference between the simple and complex recurrence groups with respect to EBL (18.4% vs 21.2%; χ2(1)=.102, p=.750) or complex adhesions (53.1% vs 43.9%; χ2(1)=.751, p=.386).
Intraoperative complications included nonfatal cardiac arrest (1.8%), intercostal muscle tear (3.5%), air leak (1.8%), intercostal vessel bleeding (0.9%), pericardial tear (0.9%). Early complications included pneumothorax (3.5%), hemothorax (1.8%), pleural effusion (0.9%), pericarditis (0.9%), bar displacement (0.9%), and C. difficile colitis (0.9%). Late complications included persistent pain (2.7%), bar displacement (1.8%), arrhythmia (0.9%), chronic infection (0.9%), and carinatum requiring operative repair (0.9%). There was no significant difference in these complications when comparing primary repair type or simple versus complex groups.
Results for the redo operation were Excellent in 69.8%, Good in 27.4%, Fair in 1.9% and Poor in 0.9%.
Conclusion: Recurrent PE repairs are more challenging than primary repairs because of patient factors that develop as sequelae of the initial repair, irrespective of the type of initial repair. It is imperative to anticipate complications; in particular, it is important to be prepared for the presence of complex adhesions and the increased risk of muscle laceration, cardiac and pulmonary injury with osteochondrodystrophy. Additionally, the overall results are less optimal than for primary repair, which yields an excellent result in 85.3% of cases versus 69.8% for redo cases.
THE DEVELOPMENT AND EVALUATION OF A NOVEL THORACOSCOPIC DIAPHRAGMATIC HERNIA REPAIR SIMULATOR
Background: Several studies on thoracoscopic diaphragmatic hernia (DH) repair show a higher recurrence rate compared to an open repair. The etiology of the higher recurrence is unknown; however, it may be related to the learning curve for the newer technique. A simulation model that replicates the key portions of the procedure may improve specific minimally invasive skills, allowing improved technical performance in the operating room for novice surgeons. Therefore, we sought to create a size appropriate, anatomically correct thoracoscopic diaphragmatic hernia repair simulator. The purposes of this study were 1) proof of concept and 2) to determine the content validity of the simulator as an educational tool.
Methods: IRB exempt pilot study (#2012-15098). Literature review and plain film chest x-rays of neonates were used to create a to-scale neonatal rib cage, using 3D engineering software. The left side of the ribcage was then printed using a 3D rapid-prototype printer. Internal structure was completed with simulated diaphragm muscle and artificial intestine, replicating the classic bowel herniation through a posterior lateral hernia defect. Final assembly included a stabilizing base and synthetic skin. Thirty-four pediatric surgery fellows and six faculty members (n=40) performed the simulated thoracoscopic DH repair. Participants completed a self-reported, six-domain, 20-item instrument consisting of 5-point rating scales, ranging from 0 (Don't know) to 4 (Highly realistic, no changes needed). An additional 4-point item was used to identify participants' global opinion of the simulator. Content validity was evaluated by examining the ratings using the many-Facet Rasch model.
Results: Analyses indicated no differences when comparing faculty (Observed Average (OA)=3.3/out of 4.0) to fellow (OA=3.1) ratings, p=.29. In descending order, observed averages of the domains were 3.57 (Relevance), 3.54 (Value), 3.32 (Physical attributes), 3.00 (Realism of experience), 2.84 (Realism of materials), 3.24 (Ability to perform task). The highest observed averages were for Value as a Training Tool (OA=3.78), while the lowest ratings were Realism of Materials-Herniated Intestines, (OA=2.50), and Realism of Materials-Diaphragm (OA=2.83). The observed average of Global opinion ratings was 2.84, indicating the simulator can be considered for teaching thoracoscopic DH repair, but could be improved. Experienced surgeons (>8 DH repair, >4 thoracoscopic) had higher overall ratings than inexperienced surgeons (3.4 vs. 3.1, P=0.01).
Conclusions: We successfully created a thoracic space relevant to a thoracoscopic DH repair, and completed the model using inexpensive, readily accessible materials. After performing a simulated thoracoscopic DH repair, fellow and faculty ratings indicated the simulator was relevant to clinical practice and valuable as a learning tool, but still required minor tissue improvements. Surgeons with thoracoscopic DH repair experience had higher overall ratings than novice surgeons. Improvements and additional validation evidence (content, internal structure, response processes and relationship to other variables) are necessary prior to full implementation of this model as an educational tool.
IS A SHORTER BAR THE SOLUTION TO AVOID BAR DISLOCATION?
Purpose: Bar dislodgement is the most frequent reported complication of Nuss procedure, accounting for at least 5% of cases. To explain the mechanism of such dislodgement, forces and torques acting on the bar and the correspondent mechanical constraints should be understood. We designed a two steps' study: initially we generated a computer-assisted design (CAD) model in order to outline the mechanical forces acting on bars of different length after their placement (in Nuss technique), subsequently we applied these suggestions to clinical scenario.
Methods: From our CAD model, bar dislodgement is caused by the rotational torque, expressed as: τ=r×F, where F is the force exerted by the sternum on the implanted bar and r is the minimum distance between rotational axis and applied force. The rotational torque is normally balanced by a reaction torque, due to the overall physical constraints the bar is subjected to, such as those onto the costal plane and those applied to sutures between bar-stabilizer and chest wall. This can be expressed by means of the following formula: τR=α×τRC+τRS where τRc is reaction torque due to the costal plane; α=scale factor, depending by the orientation of the stabilizer respect to the costal plane; τRS=reaction torque due to the sutures. α factor varies in 0–1 range and decreases as the angle θ between stabilizer and costal plane increases, until reaching the orthogonality. As a rule of thumb, with longer bars, reaction torque relies more on stabilizer fixation with sutures than on reaction forces onto costal plane. Conversely in shorter bars, α is maximized as well as reaction forces onto costal plane. Transferring these data into clinical field, we used from January 2010 bar at least four inches shorter than the distance measured from one to the other mid-axillary line.
Data collected retrospectively from a first group of patients operated at our institution from March 2006 to December 2009 following Nuss teaching (NT) (bar ½ inch shorter than the distance measured from one to the other mid-axillary line) were compared with the second group treated from January 2010 to June 2012 applying our CAD model suggestion (MS).
Results: The NT group-(48 cases) had a mean age of 16.4 years with 84% of males. Mean operating time was 57’. We accounted 5 cases (10.4%) of bar dislodgement (2 mild, 1 moderate, 2 severe which required early removal). The MS group-(88 cases) had a mean age of 16.2 years, 87% were males. Mean operating time was 43’. There was only one bar dislodgement, thus reducing dislodgement incidence from 10,4%(NS) to 1, 1%(SB) Odds Ratio 0.0989 (C.I. 0.0112 to 0.8727) p=0.0373.

Conclusion: A shorter Nuss bar, as explained in a mechanical CAD model, focus the reaction forces prominently onto the costal plane. This mechanism eventually contributes to an enhanced bar stability, thus reducing its possibility to flip. Our clinical data confirm that the use of a shorter Nuss bar may significantly reduce the incidence of bar dislodgement.
PRELIMINARY RESULTS WITH DYNAMIC COMPRESSION SYSTEM IN PECTUS CARINATUM
Objective: This study sought to evaluate the efficacy of Dynamic Compression System (DCS) with pressure measuring of the deformity device in the treatment of Pectus Carinatum (PC) described by Martinez-Ferro, as an alternative to surgery.
Methods: Infants and adolescents presenting with PC between October 2011 and October 2012 were prospectively enrolled in this study. The management protocol included: the custom of DCS, strengthening exercises, and frequent clinical follow-up. The criteria's of inclusion were: patients with PC and pressure of initial correction (PIC) ≤9 PSI (pound square inch).
Results: A total of 45 patients with PC (41 males and 4 females) were treated by DCS in 42 cases and by minimal invasive surgery (Abramson technique) in 3 cases due to highly elevated PIC. These three patients were excluded of this study.
The patients treated by DCS were: Symmetric PC in 26 cases and Asymmetric PC in 16 cases. The mean age was 15 years-old (5–19). The mean PIC was 6.1 PSI (2.5–9). The mean utilization time was 18 hours daily for 8 months (3–12). None patients abandoned treatment. Esthetic results were evaluated by using a double blinded scale (1–10). In 12 cases the treatment was completed with excellent esthetic results. In the 30 cases remaining, the normal shape of the thorax has been obtained, with excellent esthetic results, but the patients still keep the brace during the weaning.
Conclusion: This preliminary study demonstrated that DCS with pressure measuring of the deformity device is effective and helpful for treatment of PC in patients where the anterior chest wall is still compliant. The control of different pressures' measurement could be used as the inclusion criteria as well as predictive factor for esthetic results and duration of the treatment.
THORACOSCOPIC TRACTION TECHNIQUES FOR ELONGATION IN LONG-GAP ESOPHAGEAL ATRESIA
Background: Since the description of the traction techniques for long-gap esophageal atresia (LGEA) by John Foker, using standard open thoracotomies, many colleagues have confirmed their efficacy, elongating and preserving the original esophagus, however presenting some problems due to the open approaches. After our first reports of successful thoracoscopic extracorporeal Foker procedures, we have also applied Foker's recent intrathoracic and transoperative traction techniques, with the advantages of the minimally invasive surgery (MIS), even after previous thoracotomies.
Objectives: To present a series of children with LGEA treated thoracoscopically by traction elongating techniques and primary anastomosis.
Patients and Methods: From May 2003 to July 2012, 29 children with LGEA (16 female/11 male, aging 2 days - 3.8 years) underwent thoracoscopic treatment by the same surgeon at 6 different centers. Twenty patients had type A pure esophageal atresia that did not grow enough spontaneously or had previous esophagostomy or failed anastomosis, 3 had type B, 4 had type C after failed anastomosis, and 2 type D (one re-do). With the patient in prone position, using 3 ports, primary anastomosis was attempted in all cases, after good freeing of the proximal and distal esophagus, however it was not possible, so elongation procedures were performed: continuous intra-operative traction by transparietal sutures (“Foker 3” one-step anastomosis, in 11 patients), intrathoracic traction sutures+postergated primary anastomosis (“Foker 2”, n=5), or transparietal extracorporeal sutures+clips at both ends+postergated anastomosis (“Foker 1”, n=13). In the latter, radiography was taken each 2 days to evaluate the approximation of the metallic clips. At reoperation after Foker 1 and 2, another thoracoscopy was performed except in 2 cases (thoracotomy, by other surgeons).
Results: All the elongating procedures could be accomplished thoracoscopically, including suture of fistulas and despite previous adhesions. Two patients had early rupture of the traction stitches (one Foker 1 at proximal esophagus, one Foker 2 at distal esophagus), but immediate re-intervention allowed primary anastomosis. Except for these cases, the mean interval after Foker 1 and 2 was 20 days (range 10–38). One premature girl with traction sutures developed mediastinitis that cured with upper pouch suction, drainage and antibiotics. All patients achieved esophageal primary anastomosis, without myotomies or transfusion. One patient (Down syndrome, congenital cardiopathy) died 12 days later due to heart failure. Gastroesophageal reflux was confirmed in 24/28 patients (85.7%), and laparoscopic fundoplication was required in 14 of them (58.3%). Variable degrees of stenosis occurred in only 12/28 patients (42.8%), proportional to the degree of reflux, all resolving with endoscopy.
Conclusion: Thoracoscopic Foker techniques are feasible and very efficient in preserving the original esophagus in several types of LGEA, with very low morbidity, featuring all the advantages of MIS.
THE VACUUM BELL FOR CONSERVATIVE TREATMENT OF PECTUS EXCAVATUM: AN ONGOING EXPERIENCE
Background: In 1910, the german orthopaedist Fritz Lange described for the first time the effect of vacuum to lift the funnel chest. Since the minimally invasive repair for pectus excavatum (MIRPE), established by Donald Nuss in 1998, has achieved considerable progress, the therapeutic use of the vacuum bell was not given special attention. We report about our experience using the vacuum bell since 2003 to correct pectus excavatum.
Methods: After institutional review board approval, the following parameters were analysed retrospectively: patients' age, gender, depth of pectus before and after the treatment, length of application, follow-up and side-effects. To lift the sternum and correct the funnel chest, a vacuum bell (Eckart Klobe, Mannheim, Germany) was used.
Results: A total of 140 patients (28 females/20%, 112 males/80%) aged from 3 to 60 years (medium 16.05 y) were included. 61 patients (43.6%) completed the therapy and 23 (16.4%) are still under treatment. Of 25 (17.8%) patients, 10 stopped the application because of lack of motivation and not satisfying result, and 15 (10.7%) decided for surgical repair. 31 patients (22, 1%) were excluded from this study because of lacking data. Before therapy, the depth of the funnel chest was 2.7 cm in average (range 1–6.3 cm). After cessation of the treatment, depth of pectus was 0.8 cm (range 0.3–3.5 cm). The duration of daily application was 88.1 min, and application was performed during 21.8 months in average. The medium follow-up was 27.6 months (range, 0–73 months). The most reported side effects were skin irritation (13.6%), pain in the sternum region (12.1%) and petechial bleeding (7.1%).
Conclusion: The vacuum bell has proved to be an alternative therapeutic tool in selected patients suffering from pectus excavatum. The results of the recent study are encouraging, but more differentiating, age dependent studies as well as long-term results are lacking so far.
THORACOSCOPIC RESECTION OF FOREGUT DUPLICATIONS
Aim: To present our experience with thoracoscopic resections of foregut duplications (FD) and highlight their presentation, surgery and outcome.
Methods: Retrospective cohort study assessing: antenatal diagnosis, symptoms, radiological features, surgical management and outcomes.
Results: 35 patients with FD (mean age 3.2 yrs, range 0.02–11.8) were managed from 1997–2012. The diagnosis was antenatal in 12 (5 symptomatic) and postnatal in 23 (22 symptomatic and 1 incidental). The cyst location was 3 cervical, 3 cervico-thoracic, 28 thoracic and 1 thoraco-abdominal. Presenting symptoms were varied and related to FD site and included: recurrent infections 12, stridor 5, respiratory distress 5, dysphagia 3, chronic cough 4, neck swelling 2 and failure to thrive 1.
Thoracoscopic excision was performed in 23 cases (7 antenatal, 15 non-infected postnatal and 1 incidental). Thoracoscopy failed in one due to adhesions from previously failed thoracotomy excision. Thoracotomy was performed in 4 antenatal and 8 late presenting cases because of symptoms and CT findings. A cervical approach was used in 3. Laparoscopy was required in 1 case for excision of an intra-abdominal component. In 1 case in addition to thoracoscopic excision of FD a cervical laminoplasty was performed to excise an intra-spinal neuroenteric component.
Histologically epithelium identified 20 bronchogenic, 8 oesophageal, 5 mixed, 1 gastric, 1 neuroenteric.
Surgical complications included: undiagnosed cervical cyst 1, chylothorax and oesophageal leak with stricture 1, failure to completely excise cyst at initial open operation performed elsewhere 1, phrenic nerve palsy requiring diaphragmatic plication 1, transient hoarse voice 1, neurological sequealae secondary to neurosurgical neuroenteric cyst management.
Conclusion: Antenatally diagnosed foregut duplications are amenable to thoracoscopic resection. Infected cases tend to require conversions or an open procedure. Presenting symptoms can be varied and dependent on the position of the duplication cyst.
THORACOSCOPIC AORTOPEXY FOR TRACHEOMALACIA
Introduction: Tracheomalacia concerns a weakness of the tracheal rings and is usually part of an esophageal atresia complex.
Symptoms consist of life-threatening events, recurrent infectious or cyanotic spells and apnea.
Aortopexy is the treatment of choice. Nowadays this can also be performed thoracoscopically.
Patients and Methods: Between 2002 and 2012 a total of 15 children underwent thoracoscopic aortopexy. There were 7 girls and 8 boys. Mean age at the time of surgery was 25 weeks. Thirteen children had a history of esophageal atresia. Follow-up varied from 6 months to 10 years.
Results: There were no intra- or early postoperative complications. All procedures could be completed thoracoscopically. The effect was checked in all patients by flexible tracheoscopy during the procedure. In 5 patients there was a recurrence of symptoms between 2 weeks and 6 months for which a redo-thoracoscopic aortopexy was carried out. One patient with extended malacia is still on a tracheostomy. All others have fully recovered and have had no more complaints.
Conclusion: Thoracoscopic aortopexy is a successful and safe minimal invasive procedure for tracheomalacia.
Bariatric & Miscellaneous
INITIAL WEIGHT LOSS IN ADOLESCENT LAP-BAND PATIENTS DOES NOT PREDICT LONG-TERM SUCCESS
Background: Adjustable gastric banding (lap band) is well established in bariatric surgery in the adult population, however the sustainability of the weight loss is debated. Lap banding is less well studied in the adolescent patient population. Specifically we sought to evaluate if initial successful weight management predicts long-term weight loss over five years in obese adolescents.
Methods: Since our first patient in March 2005, data have been collected prospectively on all the patients. This data included basic labs, weight, percent excess weight loss, body mass index (BMI), length of stay, operative complications, operative time, and narcotic requirement. Patients were seen post-operatively every three months during the first year, then every six months following. We followed the National Institutes of Health criteria to qualify patients for bariatric surgery (BMI greater than 35 with medical comorbidities or BMI>40 by itself). Patients were excluded either because they did not have surgery at our center (although they completed the preoperatively work-up), or they did not return for their one-year follow-up appointment.
Results: The average age of the patients at the time of surgery was 15.8-years old. Their average weight was 142.3 kilograms, and the average BMI was 49. Twenty males and 47 females met inclusion criteria, 16 patients were actively followed and still had their gastric band after five years. The mean percent weight loss in the first year after having the lap band placed was 14.6% or a mean BMI reduction of 7 kg/m2. Over the ensuing four years the mean percent weight loss and BMI reduction was 17.4% and 9 kg/m2 at two years, 13.9% and 7 kg/m2 at three years, 7% and 3 kg/m2 at four years, and 3.9% and 2 kg/m2 at five years. In the first year, sixty-three (94%) patients lost weight, while three gained weight. After two years 51 patients (90%) lost weight, 5 gained, and 1 patient was at their preoperative weight. After three years 33 patients (83%) lost weight, 7 gained. At four years 20 patients (67%) had lost weight, 10 gained. In the fifth year 7 patients (44%) continued to have weight below their preoperative weight, but 9 patients had regained and surpassed their preoperative weight.
Conclusion: The majority of patients did very well in the short-term following surgery. Unfortunately many experienced their weight not only plateau but increase during years three through five. Most of the patients after five years, even those whose weight fell below their preoperative weight, found their weight trending upwards. This lack of sustained long-term weight loss with the lap band is consistent with findings in the adult literature, and also exposes specific challenges encountered in the adolescent population. We have found adolescent patients, already developmentally susceptible to external pressure, require much more support for chronic disease management to achieve positive outcomes. Another cause is likely the nature of adolescence, in that it is a time of transition, and many patients during the course of the study underwent major changes in their lives and fell out of clinical follow-up.
LAPAROSCOPIC ADJUSTABLE GASTRIC BANDING IN MORBIDLY OBESE ADOLESCENTS - SHOULD IT BE DONE?
Introduction: Non-surgical interventions for morbid obesity have proved largely ineffective in producing sustained, significant weight loss in paediatric populations. Lack of reliable long term data and the risk of serious, irreversible complications have been major impediments towards more widespread use of bariatric surgery for adolescents in Australia. The surgical procedure of choice for adolescents also remains controversial. Laparoscopic adjustable gastric banding (LAGB) is the commonest bariatric procedure performed in Australia, and the only procedure recommended at present for adolescents.
The aim of this presentation is to discuss the current outcome data of a prospective trial commenced in 2009 to evaluate the safety and efficacy of LAGB in morbidly obese adolescents; and the measures being currently undertaken to further improve outcome.
Materials and Methods: 20 morbidly obese adolescents have undergone LAGB in South Australia as part of a prospective trial since 2009. Inclusion parameters were similar to the FDA trial commenced in 2005. Outcome measures included weight loss, change in co-morbidities and development of complications. All patients were invited to undergo high resolution impedence manometry, 24 hr pH impedence, solid gastric emptying breath test, blood sampling for gut hormone analysis as well as quality of life questionnaires (Paeds SQL) at three time points - baseline, immediate pre-operative, and 6 months post-op.
Results: Eight males and 12 females have undergone LAGB since 2009. Mean age at operation was 16.6 yrs (±1.06). Mean baseline BMI was 46.04 (±8.33). 18/20 patients have had minimum 6 month follow up so far. Mean percentage excess weight loss (%EWL) at 6 months (n=18) was 35.335 (±17.52); at 1 year (n=13) 47.5% (±28.94). At 2 years (n=7), the mean %EWL decreased to 41.4% (±29.67).
The mean overall quality of life scores showed significant improvement – as reported by both patients (p=.01) and parents (p=.002) but did not reach normal levels.
There was no significant change in the reflux index 6 months post surgery (n=11, p=.073). The dysphagia risk index as measured by high resolution impedence manometry decreased significantly (n=7, p=.01) from baseline after 4 weeks of very low calory diet just prior to surgery; but returned to baseline levels 6 months post LAGB.
No revisional surgery for band related complications has been required so far.
Conclusion: The average weight loss in our series following LAGB has not been as impressive as compared with previous studies. Nevertheless, our experience so far shows that LAGB can be considered as a safe, reversible surgical option in effecting significant weight loss over the medium term with few complications in adolescents.
EARLY RESULTS FOR LAPAROSCOPIC SLEEVE GASTRECTOMY FOR TREATING ADOLESCENT OBESITY
Background: Like most of the world, the United States faces a growing epidemic of morbid obesity in the pediatric population. At least eight states have obesity rates among adolescents approaching forty percent. In some areas over half the children are obese. Eighty percent of obese adolescents become obese adults and suffer all the associated morbidity and mortality of obesity. Surgery has proven to be the most effective method to sustain long-term weight loss. A relatively new bariatric procedure, the sleeve gastrectomy, is only now becoming popular in the adolescent age group. We present our early experience with eleven patients undergoing laparoscopic sleeve gastrectomy.
Methods: Since our first patient in November 2010, data have been collected prospectively on all the patients. This data included basic labs, weight, percent excess weight loss, body mass index (BMI), length of stay, operative complications, operative time, and narcotic requirement. Patients were seen post-operatively at two weeks, four weeks, then three month intervals for the first year, and six month intervals after the first year.
Results: Eleven patients have undergone laparosopic sleeve gastrectomy at our institution either as a primary or secondary bariatric procedure since November 2010. Seven were females, and four were males. The average age at the time of surgery was nineteen, and all were followed preoperatively in a multidisciplinary clinic an average of 35 months (range 15 to 50) and demonstrated adherence to modifications made in diet and exercise regimens. The average preoperative weight was 152 kg (range 108–201) with an average BMI of 54 kg/m2 (range 42–67). There were no intraoperative complications and no deaths. The average LOS was 3.2 days (range 2–4.8). One patient suffered gastroesophageal reflux severe enough to require medication, but this resolved within two months. Two patients became pregnant (10 and 15 months postoperatively) and had an increase in their weight curves while pregnant. The mean follow-up was 11.7 months (3–24 months). For patients reaching various time intervals, the percent excess weight loss was 7% (2 weeks), 13% (4 weeks), 15% (3 months), 23% (6 months), 22% (9 months), 23% (12 months), 25% (18 months), and 22% (24 months). By excluding the pregnant patients, the average percent excess weight loss became 28% (12 months) and 36% (18 months).
Conclusions: This study iterates the safety and feasibility of laparoscopic sleeve gastrectomy in the adolescent population. The weight loss experienced by these patients is greater than that of device-mediated weight loss strategies, however it remains to be seen if the results are durable beyond two years. Longer-term follow-up will be required to further evaluate these promising short-term findings.
REVERSAL OF MORBID OBESITY IN ADOLESCENTS COMBINING LAPAROSCOPIC SLEEVE GASTRECTOMY WITH A MULTIDISCIPLINARY TREATMENT PROGRAM
Background: Obesity has become one of the most important public health problems in children and adolescents. Standard treatment for obesity in adolescents repeatedly shows only modest weight lost and surgery has become the last option for many morbidly obese adolescents. Laparoscopic sleeve gastrectomy (LSG) is a bariatric surgery that has shown good results with a relatively low rate of complications in morbidly obese adults. Currently, data on the efficiency of this procedure in the pediatric age is still scarce. Further, we use a multidisciplinary team that include pediatric surgeon, pediatric endocrinologist, pediatric psychiatrist, sport medicine specialist, dietitian, psychologist, and social worker in the care of morbid obese adolescents referred to LSG, as required by the Israeli Ministry of Health in its guidelines on adolescent bariatric surgery. The aim of this study was to examine the ability of LSG backed by a multidisciplinary team in reversing morbid obesity in adolescents.
Methods: Data were prospectively collected prior to surgery and at 3, 6, and 12 month intervals from all adolescents undergoing LSG at our institution and included age, gender, height, weight, body fat percentage, comorbid conditions, postoperative length of stay, operative and postoperative complications. Severe obesity was defined as body mass index (BMI) above the 99th percentile of US CDC growth curves in adolescents, as defined by the American Academy of Pediatrics.
Results: From March 2011 until October 2012, 18 morbidly obese adolescents have undergone LSG at our institution, of these 12 were male and 6 were female. The mean age was 16.6±1.6 years (range 13.7–18.5 yrs), mean preoperative body mass index (BMI) was 47.5±7.4 kg/m2 (range 41.5–72.4) and mean body fat percentage was 47.3±5.3% (range 39.5–57.3%). Preoperative complications of obesity were non alcoholic fatty liver (55.5%), hypertension (38.8%), diabetes mellitus (22.2%), obstructive sleep apnea (27.7%), and pseudotumorcerebri (16.6%) as well as behavioral and emotional complications associated with the obese condition. There were no intraoperative complications. The mean postoperative length of stay was 4.3 (range 3–8) days. Postoperatively, three patients developed cholelithiasis, two of them underwent laparoscopic cholecystectomy and one was treated successfully with ursodeoxycholic acid. One patient developed multiple vitamin deficiencies with severe lower extremity weakness that slowly resolved over 3 months. In 8 patients with 12 month data post-surgery, mean BMI decreased by 40% to 32.5±6.2 kg/m2, body fat percentage decreased by 40% to 28.7±12.3 (range 17.7–45.6), lean body mass reduced from baseline values by only 10% and the percent excess weight lost was 82±22% (range 51–100%). After one year, 6 of the 8 patients were no longer considered morbidly obese and 4 of them were no longer obese. The patients who did not reverse their obesity status had additional psychological morbidity and were not complying with the diet and exercise prescriptions.
Conclusion: LSG is safe and effective operation for morbidly obese adolescents and the use of a multidisciplinary team which administers diet, exercise and emotional support, greatly enhances its success.
EFFECTS OF LAPAROSCOPIC GASTRIC MUCOSA DEVITALISATION ON GASTRIC HORMONES EXPRESSION, BODY WEIGHT AND GLUCOSE HOMEOSTASIS
Background: In the recent years bariatric surgery has shown to be a helpful instrument in the long term treatment of obesity. In patients there is still a lack of acceptance against bariatric surgery due to the irreversible changes of the gastrointestinal tract, the burden of surgical revisions and complications. We established a novel endosurgical organ-preserving method for gastric mucosa devitalisation in the rat model. The aim of our project was to investigate the effects of laparoscopic gastric mucosa devitalisation on gastric hormones expression of the gut brain axis, body weight and glucose homeostasis.
Methods: 30 rats were fasted with high fat diet over a period of 11 weeks. 10 rats each group age of 15 weeks were randomly divided into either Sham, Laparoscopic Sleeve gastrectomy (LSG) or endosurgical argon plasma coagulation (APC) of gastric mucosa. Following midline laparotomy the stomach is mobilized and a small orifice is made into the fundus to introduce a catheter for a stiff endoscope, a flexible APC-probe (outer diameter of 1.5 mm) and a flexible ERBE-Waterjet flushing probe (outer diameter 1.5 mm) into the stomach. To ablate under visual control the endoscope with an outer diameter of 4 mm is introduced via the catheter and visual information is transferred to a monitor. (Telepack, Storz). The ablation is carried out under visual control after introducing the flexible APC probe into the stomach to ablate the mucosa in the corpus and antrum with a power of 25 W and gas flow of 0,2 ml/min. The gas pressure in the stomach is controlled by another notch in the fundus catheter. Following the ablation the endoscope, probes and catheters are retracted from stomach and the incision is closed with thread sutures.
28 days following surgical intervention, based on intraperitoneal glucose tolerance test (2 h/ipGTT) serum level of the orexigenic gut hormones ghrelin, total as well as active GLP-1 and PYY was measured by ELISA. Multiple/Post Hoc Group Comparisons was performed by ANOVA after Bonferroni's adjustment.
Results: After 4 weeks surgical intervention, both LSG and APC showed significantly down regulation of body weight and improved glucose metabolism compared with sham. Furthermore, our data indicate that APC regulate ghrelin (30% decrease), GLP-1 (35% decrease) and PYY (20% up) secretion comparable to SG and more effective than Sham.
Conclusion: Our new approach of endosurgery organ-preserving gastric mucosa devitalisation could be translated into a useful clinical supplementation of established bariatric surgery methods.
SUCCESSFUL WEIGHT LOSS FOLLOWING CONVERSION OF ADJUSTABLE GASTRIC BANDING TO SLEEVE GASTRECTOMY IN ADOLESCENTS
Introduction: Laparoscopic adjustable gastric banding (LAGB) has experienced widespread use in obese adults worldwide. Less is known about the effectiveness of LAGB in adolescents. Surgeons have reported band removal for complications and for failure to lose weight in adults who have subsequently undergone other weight loss procedures; few patients who have undergone LAGB as teenagers have been identified.
Methods: 5 patients (range 15.1 to 17.6 yrs, mean 16.3) out of 137 who underwent LAGB as teenagers under an IRB and FDA-approved protocol underwent band system removal and conversion to sleeve gastrectomy (GSR) as a one-stage procedure. All 5 patients underwent conversion for failure to lose weight (average wt gain 26.0 lbs), and 1 patient also had developed intractable esophagitis. One patient underwent laparoscopic cholecystectomy at the time of conversion. The mean pre-conversion weight was 358.3+82.0 lbs and pre-conversion BMI was 56.7+12.9. A 40-Bougie was used in all cases and all staple lines were reinforced with bioabsorbable material. Operating time averaged 229 minutes (range 124–303).
Esophagogastroscopy was performed in all cases. Patients underwent contrast swallow on POD 1 then were started on clear fluids, discharged on POD 2, advanced to puree at 2 weeks, then to a regular diet at 5 weeks. Diet and exercise counseling was provided at each visit.
Results: There were no perioperative complications. No patient experienced significant vomiting, heartburn, or abdominal pain in follow-up of 6–29 months. Weight loss ranged from 52.0 lb at 6 months to 112.5 lb at 29 months post-op; BMI decreased 8.6 points at 3 months to 15.8 points at 29 months. Excess weight loss following conversion ranged from 29.6+3.1% at 6 months to 77.9% at 29 months. Patients converted to GSR were able to tolerate a regular diet (including foods that they could not tolerate following LAGB). Comorbidities improved with weight loss following GSR.
Conclusion: In this small group of patients conversion to GSR led to successful weight loss in patients who had not lost weight after LAGB.
Weight Loss Following Conversion of LAGB to GSR
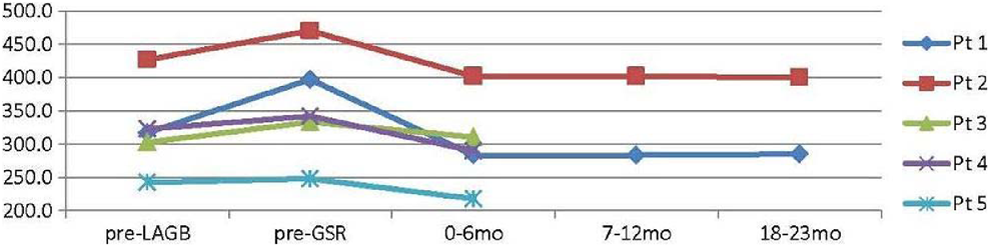
Background: We now face an epidemic of obesity among adolescents in the United States. In some states the rate of adolescent obesity nears forty percent. Eighty percent of obese adolescents become obese adults and suffer the same comorbidities as adults. Adolescent bariatric surgery is still a relatively recent endeavor, and the mainstay of therapy thus far has been the laparoscopically placed adjustable gastric band (lap band). Our institution has been placing lap bands in adolescents since March 2005 and many patients have lost considerable weight. Unfortunately we have a subset of patients mirroring the adult experience. In the adult bariatric population failure of the lap band system has been reported up to fifty percent. Regardless of meticulous dieting and exercise, they are unable to lose weight. We hypothesized for patients for whom the lap band does not allow successful weight loss, they will have better success with alternative surgical procedures.
Methods: Our choice for alternative surgical procedure was the laparoscopic sleeve gastrectomy (sleeve), because of the more favorable complication profile compared to other options. Since our first lap band conversion to sleeve gastrectomy in November 2010, we have collected data prospectively on all the patients. This data included basic labs, weight, percent excess weight loss, body mass index (BMI), length of stay, operative complications, operative time, and narcotic requirement. Patients were seen post-operatively at two weeks, four weeks, then three month intervals for the first year, and six month intervals after the first year.
Results: Six patients have undergone conversion to sleeve at our institution, 4 females and 2 males. The average age at the time of their lap band surgery was 16.7 years old, and the average age at time of sleeve was 19.7 years old. The average weight at the time of the lap band was 166 kg (133–206) with an average BMI of 60 kg/2 (range 51–71). On average patients were followed for 38 months (range 27–43) from band to conversion. Every patient requested conversion from band due to multiple episodes of pouch enlargement and failure to feel restriction with the lap band. All surgeries were performed laparoscopically in one stage, and there were neither intraoperative complications nor deaths. The average LOS was 3.3 days (range 2.3–4.8). Two patients became pregnant (10 and 15 months postoperatively) and had an increase in their weight curves while pregnant. The mean follow-up was 15 months (12–14 months). For patients reaching various time intervals, the percent excess weight loss was 5% (2 weeks), 13% (4 weeks), 14% (3 months), 18% (9 months), 22% (12 months), 18% (18 months), and 22% (24 months). By excluding the pregnant patients, the average percent excess weight loss became 27% (12 months) and 33% (18 months).
Conclusion: This study demonstrates the feasibility and safety of sleeve gastrectomy following previous placement of lap band. This offers a new hope to the unfortunate patients, who are unable to lose weight despite maximal effort. Longer follow-up will be needed to confirm the sustainability of the weight loss.
MONITORING THE METABOLIC CONSEQUENCES OF BARIATRIC SURGERY IN CHILDREN AND ADOLESCENTS: MULTIPLEXED MULTIPLE REACTION MONITORING (MRM) ASSAYS REVEAL DISTINCT DIFFERENCES BETWEEN RESTRICTIVE VERSUS MALABSORPTIVE PROCEDURES
Background: Clinical outcomes studies following laparoscopic metabolic surgery in children and adolescents are essential to investigate the course of associated comorbidities such as chronic inflammation, cardio-vascular disease or disturbed glucose homeostasis. Moreover the impact of restrictive versus malabsorptive procedures must be understood. However, essential biomarker assays have not been standardized yet. In the present study we developed and validated a serum based multiplexed MRM approach and compared the metabolic course based on a prospective cohort study of 3 different bariatric procedures.
Methods: Quantitative liquid chromatography with tandem mass spectrometry detection (LC-MS/MS) assays were established for tryptic peptides representing retinol binding protein 4 (RBP4), Adiponectin, C3 complement (C3) and Angiotensin III (AT3) in human plasma using a multiplexed MRM approach. 15 obese adolescents (age of 15±2) underwent either laparoscopic gastric banding (LGB; n=5), laparoscopic sleeve gastrectomy (LSG; n=5) or laparoscopic Roux-en-Y gastric bypass (RYGB; n=5). Their preoperative and 12 months follow-up serum samples were compared to 15 healthy non obese males (age 14±3) by multiplexed MRM assay.
Results: All target peptides produced reliable quantitative data in the MRM assays, demonstrated by a run coefficients of variation (CVs) of 2–15%. Cross-comparison with ELISA measurements (as the gold standard) revealed significant correlations. Clinically all patients demonstrated a significant weight loss following laparoscopic bariatric surgery. However the course of biomarkers differed significantly between the restrictive and malabsortive procedures: LSG and RYGB induced a significant decrease of RBP4, C3 and AT3 and an increase of adiponectin, while LGB revealed less changes of Adiponectin, C3 and RBP4.
Conclusion: Targeted multiplexed multiple reaction monitoring (MRM) assays reveal specific and sensitive insights into the pathophysiological changes following bariatric surgery in children. Standardized MRM monitoring of adipose biomarkers may help to understand the long-term consequences and the differences between the various techniques.
Robotics and Alternative Technologies
DEVELOPMENT OF A NEEDLE DRIVER WITH MULTIPLE DEGREES OF FREEDOM FOR NEONATAL LAPAROSCOPIC SURGERY
Aim: It is difficult to perform multi-directional suturing in laparoscopic surgery, because the motions of the needle driver are restricted by the trocar and the tip of a conventional needle driver has only one degree of freedom for grasping. In addition, in neonates an extremely small working space makes it more difficult to perform procedures. The aims of this study were to develop a thin needle driver with multiple degrees of freedom and to evaluate its efficacy in multi-directional suturing compared with a conventional needle driver.
Methods: A novel needle driver was developed in collaboration with the Department of Mechanical Engineering of our university. The tip of the novel needle driver has three degrees of freedom for grasping, rotation, and deflection and the length of the tip is 15 mm. The diameter of the driver is 3.5 mm. An intuitive user-friendly interface was designed and implemented for this instrument. To evaluate the usability of this device compared with the conventional needle driver, six pediatric surgeons (3 experienced surgeons, 3 trainees) were asked to perform two kinds of suturing tasks in a dry box. They were asked to make three stitches in continuous suturing that were vertical or horizontal to the insertion direction of the instrument. After the subject was given instructions and practiced manipulating the novel needle driver, the subjects was first asked to perform the tasks using the novel instrument, then using a conventional one, and finally using the novel one again. The accuracy of insertion and exit compared with the target points, and procedure time were measured. A questionnaire was administered after the experiments. Analysis was performed between the results of the conventional device and those of the second attempt of the novel device.
Results: Mean gaps from the insertion point to the target in vertical suturing were 0.5, 0.7 mm (conventional, novel, respectively), and those in horizontal suturing were 0.8, 0.6 mm. Mean gaps from the exit point to the target in vertical suturing were 0.6, 0.6 mm (conventional, novel, respectively), and those in horizontal suturing were 0.6, 0.8 mm. There were no significant differences in accuracy of suturing. Procedure time of vertical suturing was 33 and 64 sec (conventional, novel, respectively, p=0.02). Procedure time of horizontal suturing was 114 and 91 sec (conventional, novel, respectively), and there were no significant differences. All but one surgeon answered that the new instrument was easy to use in vertical suturing, and the remaining one said that the usability of the novel device and the conventional device were the same. Two of three experienced surgeons preferred to use the conventional device in horizontal suturing, but the other surgeons answered that the novel needle driver was superior to the conventional one.
Conclusions: Our novel needle driver did not affect the accuracy of suturing and may make it easier to perform horizontal suturing than the conventional one. Further studies on the trajectory of the needle or force acting on the object may show differences between them.
TOTALLY TRANSANAL LAPARO-ENDOSCOPIC SINGLE-SITE ILEAL J-POUCH (TLPC-J) - EXPERIMENTAL STUDY OF A NOVEL APPROACH FOR AVOIDING ABDOMINAL WALL INCISION FOR TOTAL COLECTOMY
Department of Pediatric Surgery, Shiraz University School of Medical Sciences, Iran
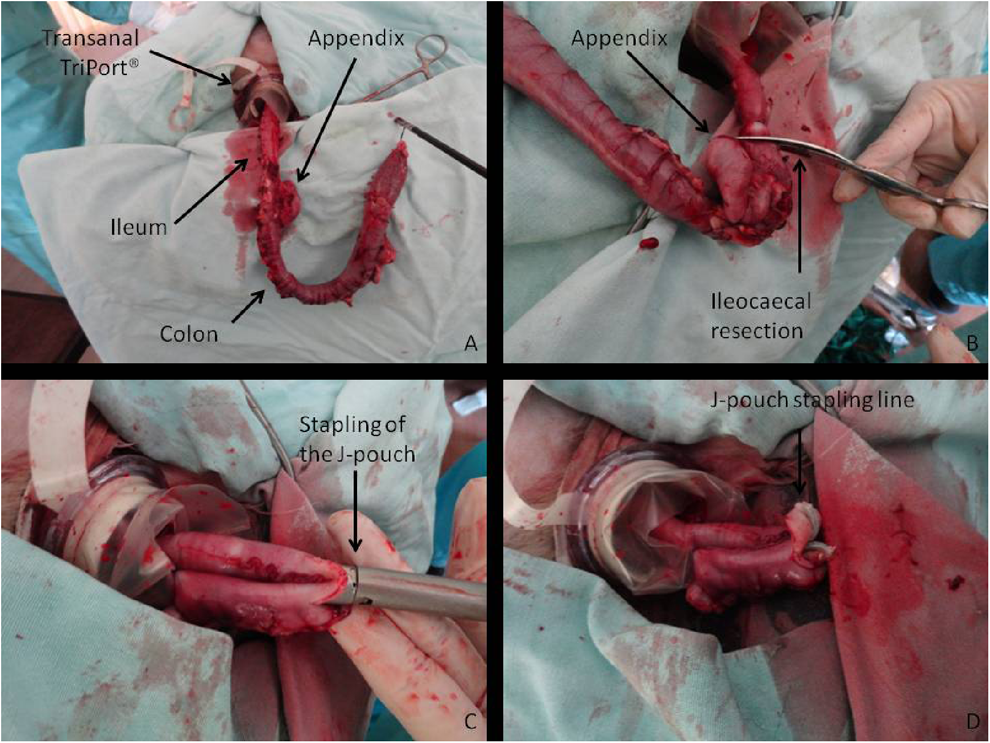
Introduction: Minimally invasive surgery in patients requiring total colectomy undergoes constant modifications with the aim to avoid abdominal wall incisions. This goal was reached by the combination of Laparo-endoscopic single-site (LESS) surgery and natural orifice transluminal endoscopic surgery (NOTES™) for totally transanal LESS pullthrough colectomy (TLPC).
We further developed TLPC and describe a novel technique for the creation of a totally transanal ileal J-pouch (TLPC-J).
Methods: TLPC-J was performed in four dogs. The TLPC-J procedure consisted of an endorectal technique with submucosal dissection starting 1 cm orally from the dentate line to above the peritoneal reflection, where the rectal muscle was divided circumferentially. After ligation of the rectal mucosa, the proximal bowel was replaced into the abdominal cavity and a TriPort® was introduced transanally. Mesenterial resection of the complete colon, mobilization of a distal ileal segment, and extra corporeal suture of an ileal J-loop were accomplished via the transanal approach. The mobilized ileum was reached and pulled down to the site of anastomosis. An incision in the J-loop was accomplished transanally. The J-pouch was created with an Endo-GIA®. After removal of the TriPort® the J-pouch was sutured to the rectal wall.
Results: All animals displayed regular bowel movements and were complication-free during the follow-up period of up to 6 months.
Conclusion: TLPC-J combines the minimally invasive LESS surgery with the scarless concept of NOTES™ and allows creation of an ileal J-pouch without abdominal incision. TLPC-J is a safe, effective, and feasible surgical procedure in total colectomy.
Background/Introduction: A broader adoption of complex minimally invasive surgery (MIS) in pediatric surgery remains challenged by the limitations of current technology. The advertised potentially enabling capacity of today's robotic technology based on master-slave paradigm faces even greater challenges, including equivocal clinical benefits and prohibitive costs. Our hypothesis is that a shared control between experienced surgeons and ‘smart’ robots will accomplish surgical tasks more proficiently than manual or tele-operated master-slave robots. We report here a clear demonstration of superior efficacy of the Smart Tissue Anastomosis Robot (STAR) as compared to today's MIS technologies.
Methods: We designed and built a novel robotic system based on the concept of shared control between surgeons and robots for minimally invasive anastomosis. STAR consists of three components: a robotic positioning platform, novel end effectors, and graphical user interface, enabling efficient tissue closure. We modified a commercially available manual suturing tool, Endo360°® (EndoEvolution, MA), as an end effector. A commercially available Kuka Light Weight Robot (KUKA, Germany) with force feedback was selected for robotic positioning platform. A graphical user interface was developed to map the desired positions of the stitches.
To test the hypothesis, we conducted a comparative study evaluating the performance of STAR (n=6) relative to that of standard 5 mm laparoscopic (n=4), laparoscopic with manual Endo360° (n=4), and robot-assisted suturing (n=4; DaVinci, Intuitive Surgical, CA). Surgical fellows and consultants with at least 5 years of clinical experience were asked to perform suturing procedures involving one knot followed by 9 stitches on 3D phantoms (3-DMed, OH). Midway into the procedure, the phantom was rotated 45 degrees to allow optical tracking of the pre-mapped suturing path by the robot. Speed, consistency, and quality of the stitches were measured based on procedure duration (minutes), suture spacing (mm), suture depth (mm), and suture displacement (mm) under 20 gram force. Statistical analysis was performed using Mann–Whitney–Wilcoxon Test (SigmaStat 3.5).
Results and Conclusions: Mean duration of the suturing task was 1.03±0.01 min (standard deviation) for STAR, 5.71±3.77 min for DaVinci (p=0.01, vs. STAR), 9.34±4.31 min for laparoscopic (p=0.01) and 4.79±1.29 min for laparoscopic Endo360° (p=0.01). Standard deviation of the suture spacing was 0.85 mm for STAR, 1.24 mm for DaVinci, and 1.55 mm for both laparoscopic and laparoscopic Endo360°. Standard deviation of suture depth was 0.70 mm for STAR, 1.10 mm for DaVinci, 1.09 mm for laparoscopic, and 1.38 mm for laparoscopic Endo360°. Mean suture displacement under 20 gram force was 0.42±1.09 mm for STAR, 1.08±1.26 mm for DaVinci (p<0.01, vs. STAR), 1.56±2.12 mm for laparoscopic (p<0.01), and 1.22±1.84 mm for laparoscopic Endo360 (p=0.02). In conclusion, we report the next generation concept for surgical robotics and clearly demonstrate the feasibility and superior efficacy of the Smart Tissue Anastomosis Robot (STAR) in phantoms as compared to today's MIS methods. A shared control between experienced surgeons and ‘smart’ robots may offer the higher standard of precision and versatility demanded in pediatric surgery.
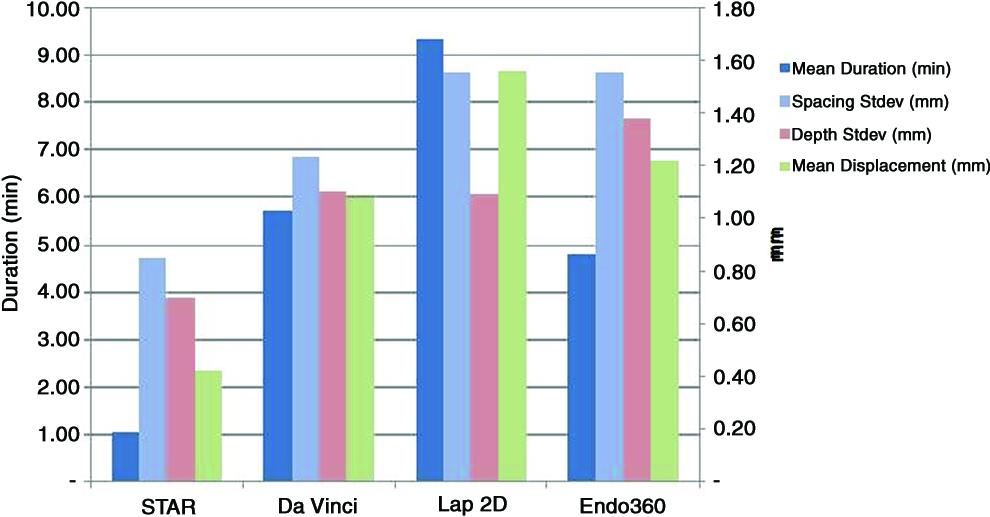
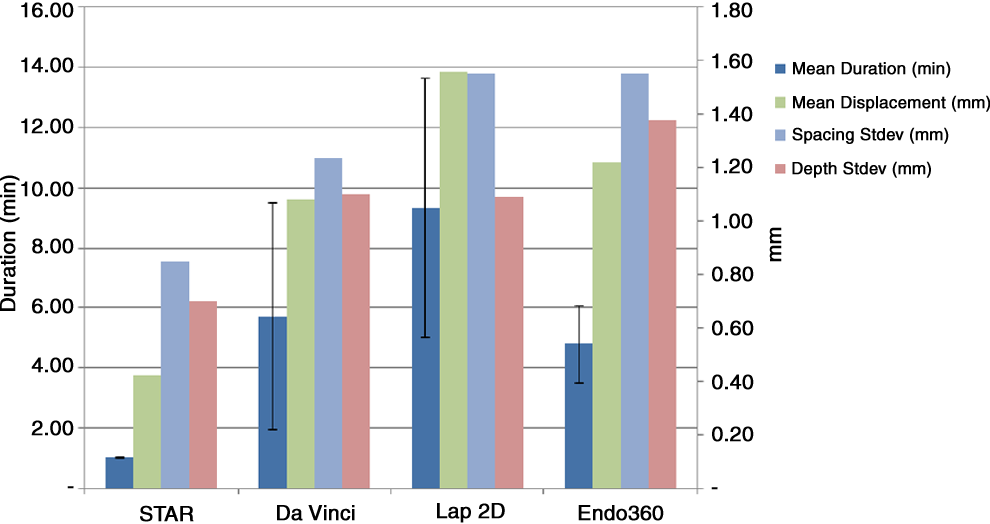
Acknowledgements: We would like to thank Craig Peters MD, Aaron Martin MD, Kelly Swords MD, and Amy Burns MD for their participation.
THE FIRST DECADE OF ROBOTIC SURGERY IN CHILDREN
Background: Robotic surgery offers technological solutions to current challenges of minimal access surgery, particularly for delicate and dexterous procedures within spatially constrained operative workspaces of children. The first robotic surgical procedure in a child was reported in April 2001. This review aims to examine the literature for global case volumes, trends, and quality of evidence for the first decade of robotic surgery in children.
Methods: A systematic literature search was performed for all reported cases of robotic surgery in children during the period of April 2001 to March 2012. The comprehensive search strategy included the following sources; 1) PubMed, 2) Ovid MEDLINE, 3) EMBASE, 4) PubMed related articles feature, 5) hand searching reference lists from retrieved publications, 6) individual search of a relevant but non-indexed journal, and 7) published abstracts from annual congresses of the International Pediatric Endosurgery Group.
Results: Following identification of 220 relevant publications, 137 publications were included that reported 2393 procedures in 1840 patients. The most prevalent gastrointestinal, genitourinary and thoracic procedures were fundoplication (n=424), pyeloplasty (n=672) and lobectomy (n=18) respectively. There was an overall progressive trend of increasing number of publications and case volumes over time. Subgroup analysis of case volumes by anatomical region revealed that genitourinary procedures most closely reflected the total reported case volume over time. The quality of evidence did not appear to improve over time, however the number of higher quality of evidence publications did increase proportionally to total number of publications. No randomized controlled trials were identified. During the 11-year review period, the published literature comprises 34% case reports, 52% case series, and 14% non-randomized comparative studies (n=220 publications). The study design was prospective in only 6% (2/32) of non-randomized comparative studies. Analysis of total published case volume by country of origin revealed that publications from the United States comprised a 79% majority. Publications were represented from 18 countries, across 52 institutions. The conversion rates for gastrointestinal, genitourinary and thoracic procedures were 3.9%, 1.3% and 10% respectively, with a net overall conversion rate of 2.5%. The rate of reported robot malfunctions or failures was 0.6%, with none of these events reported as causing harm to the patient other than operative delay or need for conversion.
Conclusions: Robotic surgery is an expanding and diffusing innovation in pediatric surgery. The rate of reported robot malfunctions or failures is low, providing reassuring evidence for the stability of robotic system software and hardware in the operative environment. The overall conversion rate was found to be comparable with conventional pediatric minimal access surgery. Technological advancements are forecast to deliver new flexible, smart robotic instruments that will have a smaller footprint and be better adapted for small operative workspaces in children. Future evolution and evaluation should occur simultaneously, such that wider and broader clinical uptake may be led by higher quality evidence.
PEDIATRIC ROBOTIC ASSISTED LAPAROSCOPIC AND LAPAROENDOSCOPIC SINGLE SITE (LESS) NEPHROURETERECTOMY
ABSTRACT WITHDRAWN
IS THE EVOLUTION FROM CONVENTIONAL LAPAROSCOPIC TO LAPARO-ENDOSCOPIC SINGLE-SITE APPENDECTOMY (LESS-A) IN CHILDREN ADVANTAGEOUS?
Introduction: Laparo-Endoscopic Single-Site appendectomy (LESS-A) through one transumbilical port minimizes visible scars. There is a paucity of data concerning the outcome of LESS-A. We evaluate the outcome of LESS-A vs. standard 3-port laparoscopic appendectomy (3-TA) in children.
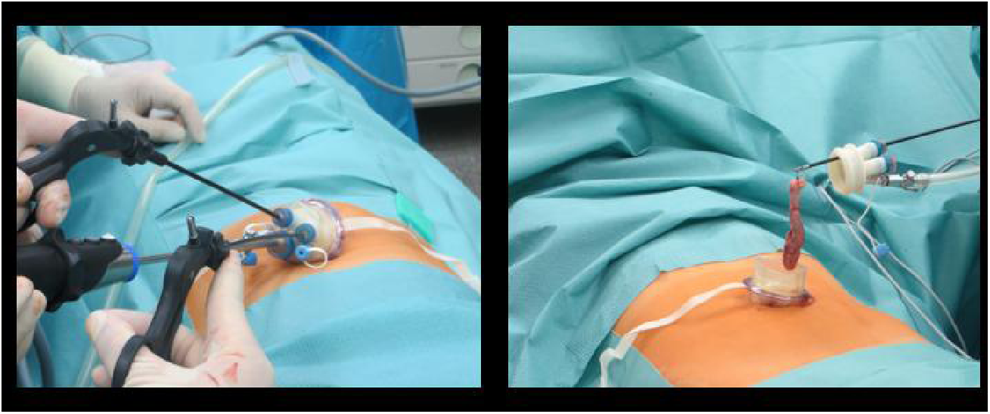
Methods: We reviewed the medical files of 309 children. The degree of appendiceal inflammation identified acute appendicitis catarrhalis (CA) in 149, phlegmonous (PLA) in 133, and perforated (PA) in 27 patients. 65 patients underwent LESS-A and 244 3-TA. We compared the duration of operation, re-admissions, re-operations, intra-abdominal abscesses, and wound infections.
Results: (Table 1)
Investigated Parameters in Laparoscopic Appendectomy
For all degrees of appendiceal inflammation LESS-A resulted in a shorter duration of operation than 3-TA (CA P=.014, PLA P=.006, PA P=.039). We found no significant differences between LESS-A and 3-TA with regard to complication rates concerning re-admissions (CA P=.512, PLA P=1.00, PA P=1.00), re-operations (CA P=.415, PLA P=1.00, PA P=1.00), intra-abdominal abscesses (CA P=1.00, PLA P=1.00, PA P=.37), and wound infections (CA P=.531, PLA P=1.00, PA P=.37).
Conclusions: We report that LESS-A is superior to 3-TA with regard to duration of operation and has similar complication rates.
Background: The single incision laparoscopic approach for cholecystectomy has been reported to be cosmetically superior in the traditional 4-port technique in several case series, however prospective comparative data are lacking. We conducted a 60 patient prospective, randomized trial comparing single incision laparoscopic cholecystectomy to standard 4-port cholecystectomy, including validated scar assessment evaluation around 6 weeks and 18 months after the operation in an effort to determine if a cosmetic advantage existed.
Methods: Patients over 12 years of age and parents of patents under 12 yrs of age enrolled in the trial were asked to complete the validated Patient Scar Assessment Questionnaire (PSAQ). The PSAQ consists of 4 subscales: Appearance, Consciousness, Satisfaction with Appearance, and Satisfaction with Symptoms. The Symptoms subscale is omitted from analysis per PSAQ instructions due to insufficient reliability. Each subscale is a set of items with 4-point categorical responses (1=most favorable, 4=least favorable). The sum of the questions quantifies each subscale. Data are expressed as mean±standard deviation.
Results: 18 single site patients and 8 4-port patients completed early questionnaires where there was no difference in overall scar assessment (P=0.17) (Table 1). Telephone follow-up was accomplished in 17 single site patients and 24 4-port patients and revealed that the overall scar assessment significantly favored the single site approach (p=0.04) (Table 2).
PSAQ Scores - Early
Conclusion: Patients or parents of patients do not identify an overall superior scar assessment at early follow up after single site laparoscopic versus 4-port cholecystectomy. However, they do perceive a superior scar assessement at long-term follow up suggesting that there is a cosmetic benefit favoring the single site approach.
Video Abstracts
Coolest Tricks, Extraordinary Procedures
Background: We have previously created a size appropriate, term neonatal chest cavity for use in a low fidelity thoracoscopic diaphragmatic hernia (DH) simulator. To increase the fidelity, or authenticity, of our DH model, real tissue would be required. The aim was to create a size appropriate real tissue thoracoscopic diaphragmatic hernia repair simulator.
Methods: The diaphragm was dissected from a second trimester fetal calf. The diaphragm was cut in half and rotated counterclockwise, to position the esophageal hiatus in a posterior lateral position, The diaphragm was then secured to a left-sided, anatomically correct, neonatal rib cage using eye hooks. Fetal bovine intestine was then herniated through the diaphragm, completing a classic left-side posterior lateral DH. The model was then covered with synthetic skin.
Results: A senior surgical resident performed the thoracoscopic DH repair. The posterior lateral defect is identified, with intestines protruding into the chest cavity. Blunt grasping instruments are used to safely reduce the herniated intestine back into the abdomen. Care is taken to ensure no inadvertent bowel injury. The abdominal domain for the simulator is limited, mimicking the limited abdominal domain of infants born with a DH. Once the intestine is fully reduced, the closure begins.
The first stitch is a lateral stitch. The lateral stitch technique shown here is an extra-corporeal suture placed through both sides of the diaphragm and around the lateral rib. The remainder of the closure is performed using interrupted sutures, with intra-corporeal knot tying techniques. After complete closure, the suture line is examined to ensure no injury to the underlying bowel. Additionally, it is examined for gaps and loose sutures.
Conclusions: We have created a size appropriate, anatomically correct, real tissue simulator that reproduces a thoracoscopic diaphragmatic hernia repair in an infant. The simulator allows for the same potential errors that may be encountered in a real operation. However, the simulator allows for a safe environment to facilitate skills acquisition, error avoidance and error correction. Validation data are necessary prior to full implementation of the simulator as an educational tool.
SUCCESSFUL LEFT THORACOSCOPIC ESOPHAGECTOMY FOR CONGENITAL ESOPHAGEAL STENOSIS WITH A USEFUL ADJUNCT OF PREOPERATIVE ENDOSCOPIC MARKING
Purpose: Minimally invasive surgery is an alternative to open surgery in esophageal resection. Many studies have described thoracoscopic esophagectomy for both benign and malignant esophageal lesions in adults. It is standard to conduct esophagectomy from the right thoracic cavity, so the aorta does not obstruct the procedure. So far, there have been no reports on left thoracoscopic esophagectomy in children.
In a case of congenital esophageal stenosis where the lesioned part was close to the esophagogastric junction, we show a successful left thoracoscopic esophagectomy with a useful adjunct of preoperative endoscopic marking.
Case report: A 3-year-old female with Down's syndrome consulted with the chief complaint of vomiting after eating solid food. In the esophagogram, stenosis was seen involving the entire circumference of the lower esophagus. The esophageal endoscope revealed a pinhole stenosis in the lower esophagus, diagnosed as congenital esophageal stenosis. On endoscopic ultrasonography, no cartilage was observed in the constricted part. Balloon dilation was performed twice; however, esophageal perforation occurred on the second dilation. The symptoms did not improve after this, and so we performed thoracoscopic esophagectomy.
Just before the thoracoscopic surgery, esophageal stricture was marked by injecting crystal violet into the constricted part using an esophageal endoscope. After this, in a right lateral decubitus position, four 5-mm ports and 3-mm forceps were inserted into the left thoracic cavity in the seventh intercostal space, anterior-axillary line; seventh intercostal space, midaxillary line; fifth intercostal space, midaxillary line; and sixth intercostal space, posterior axillary line. A 5-mm, 30-degree telescope was used. After the incision of the mediastinal pleura, the constricted part could be easily found by the dye mark. Dissection from the central esophagus to before the esophageal hiatus was thoroughly performed. Vagus nerves were identified and preserved. A semicircle incision was made on the anal side of the stained part in the esophagus and extended to the oral side longitudinally to check the constricted part. The constricted part was slightly thick and stiff. The position of the stump on the oral side was decided as above the constricted part where the luminal diameter was sufficient. Anastomosis was performed with 6 stitches of 4-0 PDS knotted suture. A nasogastric tube was positioned through the anastomosis.
In the incised pathology specimen, ciliated epithelium and bronchial glands were observed, but no cartilaginous tissues, and the patient was diagnosed with esophageal stenosis due to tracheobronchial remnants.
A minor leakage was seen in the esophagogram 7 days after the operation; however, it healed with conservative treatment. Three months after the operation, the patient is eating baby food, and vomiting does not occur.
Conclusion: Left thoracoscopic views were excellent, and manipulations of the lower esophagus were easily handled. Injecting crystal violet into the mucous membrane of the constricted part with an esophageal endoscope before the operation made it easy to verify the constricted part with a thoracoscope.
ULTRASOUND GUIDED, LAPAROSCOPIC PARTIAL NEPHRECTOMY FOR A METANEPHRIC ADENOMA
Introduction: A metanephric adenoma is a rare, benign tumour of the kidney, with only 80 cases reported in the surgical literature. Surgical excision is curative and does not require removal of the entire kidney. However, it can be difficult to localize the tumour laparoscopically. We present a US guided, transperitoneal, nephron sparing approach to this lesion.
Case History: An otherwise fit and well 16 year old female presented to the emergency department with abdominal pain. The only medical history of note was a normal renal ultrasound performed at 18 months of age, following a urinary tract infection. An abdominal ultrasound revealed a 2.4 cm isoechoic mass in the interpolar region of the left kidney. A subsequent MRI confirmed a solid renal lesion with no associated lymphadenopathy. Urinary cytology was normal. Following discussion at the local tumour advisory meeting, it was decided to undertake nephron sparing surgery to obtain a histological diagnosis, as renal cell carcinoma could not be excluded.
Procedure: Using a transperitoneal approach the kidney was exposed. Intra operative ultrasound was used to delineate the lesion. The arterial and vascular supply to the tumour where then clipped and divided. Using the Enseal, the devascularised portion of the kidney containing the tumour was then removed. The cut surface was then oversown and sprayed with tissue sealant. The patient made an uneventful recovery and was discharged 2 days following the procedure. An ultrasound performed 1 month post operatively, has shown no urinoma or tumour recurrence.
Results: The tumour was successfully removed, with clear excision margins, without the need for total nephrectomy.
Discussion: The use of intra operative ultrasound allowed for accurate and confident identification of the small target lesion. By removing the minimum amount of renal tissue, only a small number of vessels required division. This avoided the need for renal vessel clamping and the associated risks of warm ischaemia time. The use of a bipolar sealing device allowed for rapid excision of the remaining tissue and excellent haemostasis. Combined with the US guidance, this allowed for the preservation of the adjacent renal collecting system, avoiding the need for total nephrectomy. Urinary leak from the cut kidney surface was effectively prevented by oversowing the area and using tissue sealant.
THORACOSCOPIC REPAIR OF H-TYPE TRACHEOESOPHAGEAL FISTULA IN AN INFANT
Introduction: Congenital H-type tracheoesophageal fistula (H-TEF) is a rare anomaly. It is often located in the low cervical or high thoracic region and rarely in the low thoracic region. We present the thoracoscopic repair of a 2-month-old boy with H-TEF of the tracheal bifurcation.
Methods: A 2-month-old boy weighing 3,800 g was referred to the pediatric surgery because of suspicion of the TEF. He was born weighing 2,870 g at 39 weeks' gestation, and transferred to the neonatal intensive care unit due to abdominal distension and vomiting on day 3. X-ray imaging revealed gaseous distention of the stomach and TEF was suspected. The esophagogram revealed H-type fistula, and flexible bronchoscope under general anesthesia showed the fistula just above the carina. He had no other congenital anomalies. He was treated using thoracoscopic approach. Under general anesthesia, a 4-Fr Fogarty catheter was inserted via a nostril into the trachea, and then tracheal intubation was performed with a 3.0-mm tracheal tube. A flexible bronchoscopy was performed, and the fistula was cannulated with the Fogarty catheter to block of the fistula. After blocking of the fistula, a tracheal tube was replaced in the left main bronchus and one-lung ventilation was carried out. The patient was then placed in semi-prone position with the right side elevated. A 5-mm trocar was inserted approximately 1 cm blow the angle of the scapula. The pleural space was insufflated at a pressure of 8 mm Hg, and the 5 mm thoracoscope was used. Three additional trocars (1 5-mm and 2 3-mm) were then placed for the insertion of a working instrument. First, the azygous vein was dissected, ligated proximally and divided by using ENSEAL. The esophagus and trachea were carefully dissected using bipolar bovies until the fistula was identified. TEF was circumferentially dissected from the tracheal bifurcation, and ligated with 4-0 Vicryl after removing of the Fogarty catheter. Transfixing Vicryl 5-0 sutures were laid on the both sides of the fistula, and the fistula was ligated close. The fistula was divided in between. The distal stump of the esophageal side was covered using the muscular layer by 4 sutures of 5-0 Vicryl. Finally, a polyglycolic acid (PGA) sheet with fibrin glue was interpositioned between the trachea and the esophagus to prevent a recurrent fistula. No drain was placed.
Results: The operating time was 150 minutes. The patient was successfully extubated on 1 POD. Swallow study on 3 POD revealed normal without evidence of leak and oral feeding was initiated. The patient was discharged home on 7 POD and did well at 7-month follow-up.
Conclusions: Thoracoscopic management is obviously less invasive, and provides excellent visualization and magnification for low type H-TEF. Blocking of TEF by a Fogarty catheter is useful for finding the fistula and preventing of gastric distension. In this case, PGA sheet with fibrin glue was interpositioned between the trachea and the esophagus to prevent a recurrent fistula.
THORACOSCOPIC LEFT UPPER PULMONARY LOBECTOMY IN A GIRL WITH CCAM AND FUSED MEDIASTINAL LINGULAR BRANCHES (A 4 + 5) OF THE LEFT PULMONARY ARTERY
We present a case of a 2-year-old girl, weighing 14 kg, who had thoracoscopic left upper lobectomy (TLUL) for the treatment of prenatally diagnosed left upper lobe congenital cystic adenomatoid malformation (CCAM). On preoperative 1 mm thin-section computed tomography, intralobular lingular branches of the left pulmonary artery appeared to be absent, suggestive of the presence of mediastinal lingular branches. Lingular branches, A4 and A5, are usually located in the intralobar part of the pulmonary artery and thus do not exist in the mediastinal part of the pulmonary artery in the majority of cases. However, although rare, they may be present in the mediastinal part of the pulmonary artery, and less commonly, the lingular branches may be totally absent in the intralobar part of the pulmonary artery, and may be present only in the mediastinal part of the pulmonary artery. Furthermore, mediastinal lingular arteries A4 and A5 may be fused as one vessel, A4 + 5, which has a short pedicle and is located just behind the left upper lobe pulmonary veins V1 to V5, and attached to the left upper lobe bronchus. Thus, surgeons should be mindful of mediastinal A4 and A5, and fused A4 + 5. When fused, the vessel is thick with a short pedicle from the main trunk of the pulmonary artery, and if bleeding occurs secondary to excessive traction, hemostasis is almost impossible. TLUL was performed in the lateral decubitus position with single lung ventilation using four 5 mm trocars. Firstly, the intralobar part of the left pulmonary artery was exposed after dividing the relatively thick incomplete fissure with an EnSeal tissue sealing device. Thus, we were able to confirm that our patient did not have intralobar lingular branches. Left upper lobe pulmonary veins V1 to V5 were then exposed, and dissected free using hook diathermy with great caution, since the lingular branches of the pulmonary artery were likely to be located just behind the left upper pulmonary veins in this patient. After the pulmonary veins were dissected, they were divided en bloc with an endoscopic stapler. After division of the left upper lobe pulmonary veins, anterior branch A3 and mediastinal lingular branches were exposed and at this stage, the lingular branches, A4 and A5, were found to be fused. The fused vessel (A4 + 5) was carefully dissected free from surrounding structures such as the left upper bronchus and A3, with great care taken not to tear the main pulmonary artery trunk during traction on A4 + 5. A4 + 5 was then clipped and divided. A3 also had a short pedicle and was carefully dissected free, clipped, and divided. The remaining apical artery A1 + 2 was divided, and the left upper bronchus exposed and divided with an endoscopic stapler to complete the left upper lobectomy. Operative time was 3 hours and intraoperative blood loss was 10 mL. A chest drain was removed on postoperative day 2. She remains well after follow-up of 24 months.
VIDEOSCOPIC LEFT CARDIAC SYMPATHETIC DENERVATION SURGERY FOR THE TREATMENT OF LONG QT SYNDROME
Background: Congenital long QT syndrome can result in malignant ventricular arrhythmia's stemming from channelopathies. Although beta blockers are the mainstay of management, some will require more aggressive prevention strategies such as implantable cardioverter defibrillators. However, given that ICDs carry significant comorbidities, left cardiac sympathetic denervation surgery has become a viable alternative.
Methods: We present here a 9 month-old female patient who was diagnosed in utero with type I long QT syndrome. She was found to have a homozygous mutation involving the KCNQ1 potassium channel. Our patient has a significant family history of long QT syndrome, including an older sister, who has received an implantable defibrillator, as well as two paternal aunts who tragically died in infancy. Pre-operative evaluation consisted of an electrocardiogram which demonstrated a prolonged QTc of 515 msec. She also underwent echocardiography which showed normal cardiac anatomy and function.
Results: After anesthetic induction, the right bronchus was selectively intubated and the left lung collapsed. The patient was placed in right lateral decubitus position and three 3-mm incisions were made, the first in the posterior axillary line in the fifth interspace, the second in the fourth interspace in the anterior axillary line, and the third in the second interspace in the midaxillary line. The sympathetic chain was visualized and then further exposed by dividing the overlying pleura using sharp dissection followed by cautery. 1% Lidocaine was then instilled over the field. The sympathetic chain was then divided beginning at the ganglion of T4. The ganglions were removed by dividing the major rami communicans and fully identifying the much smaller sympathetic nerve branches that travel toward the heart. The left stellate ganglion was then divided along the anatomic fusion between its upper and lower poles, just above the major lower branches. The completely dissected nerve trunk and ganglia were removed en bloc. The dissected materials were sent to pathology and read by frozen section to ensure that nerve and ganglions had been removed.
Conclusion: Our patient was able to leave the hospital on postoperative day number two and did not suffer any significant morbidity. Her surgery related pain was negligible. She had no eyelid droop. Her post-operative ECG showed a QTc of 512 msec; essentially back to her pre-operative state. Videoscopic denervation surgery offers a safe and effective treatment option for patients with a sudden-death-predisposing channelopathy such as long QT syndrome.
THORACOSCOPIC-ASSISTED PARTIAL RIB RESECTION
Background: Osteochondroma the most common benign bone tumor in children, however it is rarely the domain of the paediatric surgeon to manage.
Methods: We present a symptomatic, pedunculated osteochondroma of the left-6th rib extending into the thorax with no visible or palpable external landmarks.
Results: The thoracoscope was used to visualize the lesion within the chest and map out the resection margins prior to incision. This allowed optimal use of the incision and precise excision.
Conclusion: Thoracoscopic assistance during chest wall excision is a useful technique for benign and malignant lesions to optimize cosmesis and margins.
ULTRASOUND GUIDED THORACOSCOPIC DENTAL EXTRACTION
Backgound: Recurrent pneumonias in children may be a consequence of a previously unrecognized aspirated foreign body (AFB).
Method and Materials: We present a case of a 10-year-old neurologically impaired (NI) child with an aspirated tooth in the right lower lobe segmental bronchus as seen on chest CT scan. A retrospective analysis of his previous chest x-rays suggested the presence of an AFB four months prior. Although a severely inflamed bronchial tree and copious secretions were noted on flexible bronchoscopy, the AFB was not visualized directly due to its extremely distal location. After a week of pulmonary optimization and intravenous antibiotics, the patient was taken to the operating room for surgical excision.
During thoracoscopy, it was quickly evident that the AFB was not visible or palpable on the surface of the lung parenchyma. Intraoperative ultrasound was then used during thoracoscopy to identify the location of the foreign body.
Result: The foreign body was easily identified using intraoperative ultrasound. This consequently facilitated a wedge resection of the lung parenchyma containing the tooth. The extraction was thus completed thoracoscopically and a lobectomy was avoided.
Conclusion: A multimodal approach with ultrasound and thoracoscopy can be useful in managing AFB that cannot be extracted via rigid or flexible bronchoscopy. One may consider this technique during thoracoscopic wedge resection of calcified lesions in the lung that are deep in the parenchyma.
Unexpected Findings, Troubles, and Complications
THE STRING PUPPET TECHNIQUE: A USEFUL TOOL FOR TRANSUMBILICAL SURGERY
Transumbilical surgery (TS) has emerged to improve aesthetics results and enhance postoperative recovery. Nonetheless, TS entails a considerable learning curve, especially to avoid instrumental collision while in the quest for optimal organ retraction and triangulation. We describe the String Puppet Technique, a maneuver that allows organ retraction using an internal grasper that is controlled by external leashes. A straight needle with a 2.0 nylon suture is introduced at the epigastrium in a percutaneous fashion. The needle is then externalized through a 12-mm umbilical trocar using a 10-mm scope with a 6-mm working channel. The procedure is repeated on the right flank. Outside the abdominal cavity, both sutures are tied to a stainless steel alligator clamp (AC). For deployment into the abdominal cavity, the AC is placed into the operating channel at the tip of the laparoscope with its jaws open. Already in the abdomen, the AC is directed to the target area with a Thomas forceps. In this video, the infundibulum is grabbed with the AC and external traction is provided using both sutures. The AC allows for strong organ retraction and can be repositioned without difficulty. Finally, the AC is withdrawn along with both sutures through the umbilical port.
SUSPENSION STITCHES FOR COMPLEX NEONATAL ANASTOMOSES
Introduction: Complex neonatal congenital defects pose a challenge for surgical repair utilizing minimally invasive techniques. We demonstrate a technique using suspension stitches to facilitate the thoracoscopic repair of esophageal atresia and laparoscopic repair of duodenal atresia.
Methods: Esophageal atresia: a one day old 2900 gram baby boy presented with an aberrant right subclavian artery, a left-sided aortic arch, proximal esophageal atresia and distal tracheoesophageal fistula. A 10 French chest tube inserted into the proximal esophageal pouch with slight pressure demonstrated a short gap atresia on radiograph. In the OR, he was placed on high frequency oscillator ventilation and positioned in the exaggerated left lateral decubitus position (nearly prone). A thoracoscopic approach was used with 3 mm equipment, ligating and dividing the azygous vein and tracheoesophageal fistula in standard fashion. A 4-0 PDS suture was placed through the chest wall near the spine, through the proximal pouch, through the distal esophagus, and back out the chest wall to bring the two ends of the esophagus together. This suspension stitch facilitated completion of the anastomosis with good visualization and minimal manipulation of the tissues. An 8 French feeding tube was guided through the anastomosis and a 12 French chest tube placed into the right hemithorax.
Duodenal atresia: a two day old 2700 gram baby girl presented with trisomy 21, balanced AV canal, duodenal atresia and annular pancreas. A radiograph demonstrated a “double bubble” with no distal gas. In the OR, she was intubated and positioned supine. A laparoscopic approach was used with 3 mm equipment, first confirming normal rotation and identifying the proximal and distal ends of the duodenum with intervening annular pancreas. A 4-0 PDS suture was placed through the abdominal wall near the fundus of the gallbladder, through the proximal duodenum, through the distal duodenum, and back out the abdominal wall to bring the two ends of the duodenum together. This suspension stitch facilitated completion of the anastomosis with good visualization and minimal manipulation of the tissues.
Results: Operative time for thoracoscopic esophageal atresia repair was ninety minutes. Nasogastric feeds were initiated with return of bowel function. An esophagram on postoperative day five showed no leak. Oral feeds were started and the thoracostomy tube removed. Repeat esophagram at one year showed no stricture.
Operative time for laparoscopic duodenal atresia repair was one hundred and twenty minutes. Feeds were initiated on postoperative day seven, once orogastric tube output had decreased.
Conclusion: We demonstrate a use of suspension stitches to line up difficult anastomoses and minimize tissue manipulation. This facilitates the repair of complex neonatal congenital defects using minimally invasive techniques. Using this technique we are able to routinely repair these congenital defects in neonates weighing as little as 1.7 kilograms. Suspension stitches provide another innovative method to build reproducible success in dealing with these difficult congenital anomalies.
LAPAROSCOPIC LIVER RESECTION: RESECTION WITH A TUMOR HANGING FROM SUPERFICIAL HEPATIC LEFT LATERAL SEGMENT
We report a case of a child with a tumor hanging from superficial hepatic left lateral segment which was successfully resected laparoscopically. A 2 y/o female previously treated with surgical resection for dumbbell type malignant peripheral nerve sheath tumor (MPNST) in the first year of life, and post-operative surveillance imaging revealed a growing tumor hanging from left lobe of liver. Because of concern for malignancy, she underwent laparoscopic assisted resection including left lateral segment of liver with the use of the LigaSureTM (without the Pringle's maneuver). There was no bile leak, bleeding nor other complication of this procedure. In pediatric tumor lesions, localized in superficial hepatic segments could be a suitable indication for this technique.
LAPAROSCOPIC MEDIAN ARCUATE LIGAMENT RELEASE
Background: The patient is a 13 year-old female with a history of acute onset of food and exercise induced epigastric pain, beginning 18 months prior to presentation. She experienced early weight loss, which stabilized once she changes to multiple small meals per day. After an extensive workup that was negative for causative abdominal pain factors, she was referred for evaluation for median arcuate ligament syndrome (MALS).
Methods: A complete abdominal ultrasound (US) was negative for solid organ structural abnormalities. Doppler US of the mesenteric vessels was notable for focal narrowing of the celiac trunk at the takeoff from the aorta. Peak systolic velocities of the celiac artery were elevated at 373 cm/sec, with normal distal velocities in the hepatic and splenic arteries. The superior mesenteric artery also had somewhat elevated velocities without evidence of focal narrowing. Given the possible two-vessel disease, a magnetic resonance angiogram (MRA) was obtained to further evaluate the US findings. The MRA was notable for focal narrowing of the celiac artery only, with a normal superior mesenteric artery. The combination of symptoms, an exhaustive negative workup, elevated systolic velocities of the celiac artery and focal narrowing of the celiac artery are suggestive of MALS.
Results: The patient was positioned in stirrups and then placed in reverse Trendelenberg position. One 12 mm port, required for the laparoscopic US probe, was placed at the umbilicus. Four 5 mm ports were then placed in the usual configuration for a fundoplication. A liver retractor was placed to expose the gastrohepatic ligament.
The gastrohepatic ligament was taken down sharply. The left gastric artery was identified and anterior and posterior dissection was begun to further expose the vessel. A laparoscopic US probe was used to further delineate the anatomy and the precise position of the celiac artery. The intraoperative US images showed the focal narrowing of the celiac artery, with post-stenotic dilatation of the vessel. The aorta was exposed proximal to the celiac artery. The arcuate fibers of the diaphragm were exposed with blunt dissection, and transected with electrocautery. With full exposure of the adventitia of the aorta, US was used to confirm celiac artery location.
Staying in the anterior and posterior planes only, the gastric artery dissection was continued. Lateral dissection is cautioned against, to prevent inadvertent injury to the hepatic and splenic arteries. The gastric artery was traced to the celiac artery, where dense fibrotic tissue is encountered. The constricting fibrotic band was clearly visible. With the gastric artery visible in the foreground and the aorta in the background, the fibrotic tissue was carefully transected. With final release of the fibrotic band, the celiac artery came into view, with no residual compression.
Conclusion: In carefully selected patients with vascular Doppler US results suggestive of celiac artery compression, a median arcuate ligament release can be safely performed laparoscopically. Intra-operative US is critical to safely identify relevant anatomy and to minimize risk of major vascular injury.
LAPAROSCOPIC DISTAL PANCREATECTOMY WITH SPLENIC PRESERVATION FOR SOLID PSEUDOPAPILLARY PANCREATIC NEOPLASMS IN THE ADOLESCENT POPULATION
Introduction: Pancreatic masses in children and adolescents are predominately benign. Solid pseudopapillary neoplasms, or Frantz tumors, are exceedingly rare with an incidence of <1% of all pediatric pancreatic neoplasms. These tumors have low malignant potential and have been predominately reported in young women. Treatment of choice remains complete resection. This video demonstrates our techniques of laparoscopic distal pancreatectomy with splenic preservation in an adolescent female.
Video Objectives:
1. Overview of solid pseudopapillary pancreatic neoplasms. 2. Discuss the importance of splenic preservation in children in prevention of overwhelming post-splenectomy sepsis.
Operative Indication: The patient is a 14-year-old girl who presented with a chief complaint of right-sided abdominal pain. Subsequent evaluation revealed a 5 cm mass in the tail of the pancreas.
Operative Findings:
1. Complete preservation of splenic artery vein with minor devascularization of segmental branch vessel to spleen (over 90% perfused). 2. No violation of the mass throughout the operation.
Final Pathology:
A) Hilar lymph node, biopsy: Cauterized lymph node, negative for malignancy. B) Tail of pancreas, resection: Solid-pseudopapillary neoplasm, resected pancreatic margin negative for tumor.
Discuss operative challenges of this approach in the adolescent population.
Conclusion: Laparoscopic distal pancreatectomy with splenic preservation is technically feasible and adheres to oncologic principles in the pediatric population. Splenic preservation is important in this population to preserve immunity and prevent overwhelming post-splenectomy sepsis.
SURGICAL TREATMENT OF INSPISSATED BILE SYNDROME USING A 2-STAGE PURE LAPAROSCOPIC APPROACH
Introduction: Neonatal jaundice is common and requires rapid evaluation. Herein, inspissated bile syndrom (IBS) represents a rare condition. Treatment in general consists of interventional percutaneous transhepatic cholangiography with contempory therapeutic lavage of the biliary tree in those cases that do not respond to oral ursodeoxycholic acid. Because of technical impracticability of this interventional procedure due to the small size of intrahepatic bile ducts and in order to avoid laparotomy, minimally invasive techniques raise high interest.
Methods: We present a video of a 3-month-old infant suffering from extrahepatic cholestasis. Treatment consisted of cholecystotomy, insertion of an indwelling catheter for local ursodeoxycholic acid bile duct flushing and subsequent removal of cholecystotomy in a fully laparoscopic two-session approach. Indication consisted of a bilirubin increase (7.7 mg/dl) in combination with sludge-related dilatation of the extrahepatic bile ducts shown on MRCP and ultrasound.
Results: Under general anaesthesia a three-port technique in supine position was used. A 5 mm trocar was inserted at the umbilicus and two 3 mm working ports were positioned in the right and left middle abdomen. The gallbladder was fixed to the ventral abdominal wall using a 4.0 vicryl intracorporeal suture. A purse-string suture was placed at the fundus before punctiform cholecystotomy was performed using a monopolar instrument. A 6 French balloon catheter was inserted transabdominally, positioned in the gallbladder and blocked. Tight fixation of the gallbladder was realized using 3 additional intracorporeal sutures to the ventral abdominal wall in order to prevent leakage. Intraoperative cholangiography illustrated the choledochal duct filled with bile concretions, a severe hepatic influx and delayed drainage of contrast agent into the duodenum. Postoperatively, bile duct lavage using a 5 ml solution containing 10 mg ursodeoxycholic acid was performed 3 times a day for 13 consecutive days until control cholangiography showed free drainage into the bowel and reduction of the bilirubin value to 1.9 mg/dl. A second laparoscopy was perfomed using the same trocar setting for release of the cholecystotomy and closure of the gallbladder using two 4.0 vicryl Z-sutures preserving the organ. The postoperative course was uneventful. Follow up was 7 months after operation and showed normal bilirubin and transaminase levels. Ultrasound imaging showed a normal shape of the gallbladder, but also mild hepatosplenomegaly.
Conclusion: This minimally invasive approach for antegrade bile duct flushing for IBS might be recommended as the treatment of choice in cases without response to oral ursodeoxycholic acid. Using this fully laparoscopic technique we could preseve the gallbladder and avoided more invasive laparotomy with coexistent morbidities.
LAPAROSCOPIC DUODENAL ATRESIA REPAIR SIMULATOR
Background: The aim was to create a size appropriate real tissue laparoscopic duodenal atresia repair simulator. Bovine stomach anatomy is notable for having 4 separate compartments for initial digestion. We sought to determine if fetal bovine foregut anatomy would be usable for infant laparoscopy simulation modeling.
Methods: An abdominal block of liver, stomach and proximal intestine was dissected from a second trimester fetal calf. The fetal bovine stomach also has four separate compartments of the stomach, which ultimately connect to a decompressed duodenal segment of bowel. Notably, the third and fourth portions of the fetal stomach are similar in appearance to the double bubble of duodenal atresia. There is a narrowing between the third and fourth stomachs, replicating the appearance of a pylorus. The fourth stomach then connects to a duodenum with a marked difference in caliber. Thus, the fetal bovine stomach and duodenum have a very similar outward appearance of a duodenal stenosis or web.
To complete the simulator, the fetal bovine abdominal block was mounted into an infant abdominal cavity with a size appropriate abdominal domain for a full term infant. The model was then covered with a silicon synthetic skin.
Results: The laparoscopic repair begins with identification of the anatomy, a proximal dilated duodenum with a marked caliber change in the distal duodenum. The transverse duodenotomy is created in the proximal duodenum, with clear identification of the lumen of the bowel. A longitudinal duodenotomy is created in the distal duodenum, again, identifying the lumen of the bowel.
The operative repair will be a duodenoduodenostomy, in the classically described diamond-shaped configuration. The first suture is placed in the posterior wall, beginning the anastomosis. Intracorporeal suturing techniques are used for the entire anastomosis. Two additional back wall sutures are placed in similar fashion, ensuring that full-thickness bites are taken and that there are no gaps. After completing the posterior wall, the anterior wall is closed with continued interrupted sutures. The completed duodenoduodenostomy was then examined for patency and any gaps.
Conclusion: In summary, the segmental compartmentalization of the second trimester fetal bovine stomach has surprising similarity to an infant born with duodenal stenosis or web. Using this second trimester fetal bovine abdominal block, we have subsequently created a size appropriate real tissue laparoscopic duodenal atresia simulator. Validation data are necessary prior to the full implementation of this model as a teaching tool.
Urogenital MIS
MINI-PERCUTANEOUS NEPHROLITHOTOMY FOR UPPER URINARY TRACT CALCULI IN CHILDREN (REPORT OF 134 CASES)
ABSTRACT WITHDRAWN
Afternon Scientific Video Session
LAPAROSCOPIC GASTRIC PULL-UP IN LONG GAP ESOPHAGEAL ATRESIA
This is the case of a 2-year-old male preschooler, diagnosed with type III esophageal atresia. During the neonatal period, the patient had a right thoracotomy, ligation of a tracheo-esophageal fistula and and esophago-esophagostomy were carried out, but failed because there was a long gap atresia. The measured gap was of 4 vertebrae confirmed the diagnosis of long gap esophageal atresia; upon its evaluation by a multidisciplinary team, a laparoscopic gastric pull-up was carried out using 4 trocars: one 12 mm, two 5 mm and one 3 mm trocar. The 6-hour duration of surgery was due to a firm adhesion of esophago to the posterior mediastinum. The patient had a favorable outcome without major complications. He remained in PICU for 72 hours and was extubated 48 hours after surgery. This is the sixth case of this particular pediatric surgeon and although our follow-up is still underway, we believe that laparoscopic pediatric surgeons with a certain degree of experience would be able to reproduce this technique, which is an excellent therapeutic option for the management of long gap esophageal atresia with good postoperative results.
REVIVING KASAI'S ORIGINAL PORTOENTEROSTOMY FOR LAPAROSCOPIC APPLICATION ENABLES OUTCOME COMPARABLE TO OPEN PORTOENTEROSTOMY IN PATIENTS WITH BILIARY ATRESIA
Through modification, the current portoenterostomy procedure has come to vary from Kasai's brilliant original procedure for the surgical treatment of uncorrectable biliary atresia (BA). We revived the principles he devised and adapted them for laparoscopic use. To date, we have treated 10 BA patients using our laparoscopic Kasai portoenterostomy (lap-KP) achieving encouraging results with 100% jaundice clearance (10/10 BA patients) and 80% jaundice-free (Total bilirubin less than or equal to 1.2 mg/dL) survival with the native liver (8/10 after a mean follow-up to 2.2 years (range: 1 month–3.8 years). Although 2 patients required liver transplantation, one was jaundice-free and the other had total bilirubin of 1.6 mg/dL. We present our technique for lap-KP. An extra 5 mm trocar is placed in the epigastrium in addition to conventional trocar placement, and a Ligasure device is inserted to dissect the fibrotic biliary remnant and divide portal vein branches at the porta hepatis instead of hook diathermy, because Ligasure causes less lateral thermal injury than diathermy. The biliary remnant is then transected shallowly as per Kasai's original technique which we will show using an original video of Professor Kasai himself operating, rather than performing an extended dissection. Anastomotic sutures are placed shallowly to the liver parenchyma around the margin of the transected biliary remnant at porta hepatis, whilst sutures at the 2 and 10 o'clock positions where the original right and left bile ducts were are placed shallowly to the connective tissues, not the liver parenchyma nor the biliary remnant. An individualized Roux-limb is created extracorporeally through the umbilicus by bringing the distal end of the limb up to just above the xiphoid process. The jejunojejunostomy is also custom made to fit into the splenic flexure when it is returned to the abdominal cavity. The “short” Roux-limb is then approximated to the native jejunum for 8 cm cranially to prevent contents of the native jejunum from flowing into the Roux-limb. Thus, Roux-limb redundancy and reflux/stasis, associated with Roux-limbs of predetermined length are prevented. Lap-KP could prove to be a promising alternative to open portoenterostomy.
TIPS AND TRICKS: LAPAROSCOPIC MANAGEMENT AND RECONSTRUCTION OF PROXIMAL HEPATIC DUCT TRANSECTION DURING LAPAROSCOPIC CHOLEDOCHAL CYST EXCISION
Introduction: Laparoscopic management of hepatic duct transaction during choledochal cyst excision can be challenging. This video demonstrates the lesson learned in how to potentially avoid this situation and the technical aspects of how to manage it should it occur.
Method: A five year old girl underwent a standard laparoscopic choledochal cyst excision and Roux-en-Y hepaticojejunostomy reconstruction. For the ease of the distal dissection of the choledochal cyst, the common hepatic was transected above the cystic duct insertion. We quickly recognized that the hepatic ducts were transected above the bifurcation. Rather than individually implanting into the jejunal Roux limb, we reconstructed them into a common channel via a “fish mouth” method to facilitate a single larger hepaticojejunostomy anastomosis.
Results: The patient has uneventful postoperative course and at one year follow-up has normal liver function tests.
Conclusion: It is not uncommon that the cystic duct enters into the common hepatic duct high, and therefore, dividing the common hepatic duct above the junction with the cystic duct may lead to transaction of the left and right hepatic ducts. In the case of a high transaction, laparoscopic “fish mouth” reconstruction may provide a bigger common channel and potentially minimize the risk of stricture.
HYBRID SURGICAL REPAIR OF TOTAL TUBULAR COLONIC DUPLICATION ASSOCIATED WITH ANOVESIBULAR AND ANOCUTANEOUS FISTULAS
Introduction: Total tubular colonic duplication is a rare and complex anomaly. We present a new technique consisted on anterior sagittal anorectoplasty and fenestration of the duplicated colon using a Hybrid method, single incision laparoscope-assisted and endoscopic procedures, for a case of total tubular colonic duplication associated with anovesibular and anocutaneous fistulas.
Patient: A 3,030 gram female baby presented with an anocutaneous fistula and an anovestibular fistula through which fecal discharge was observed. Radiological and endoscopic evaluations revealed tubular duplication of the entire colon, dextrocardia with situs inversus and duplication of bladder, urethra and vagina without a vertebral anomaly.
Treatment: She underwent a surgical repair at 9 months of age. In the lithotomy position, anterior sagittal incision was placed from the vestibule of vagina to the center of anal complex, and the 1.5 cm-length both fistulae were excised. The duplicated rectum was dissected with preserving the puborectal muscle and reconstructed into a single lumen using EnSeaL tissue sealing system (TM, Ethicon, Japan). Single incision laparoscopic surgery revealed mesenterium commune associated with mobile of the total colon. The intestinal tract between the terminal ileum and sigmoid colon was exteriorized through the umbilical wound. A common wall of duplication from the cecum to the sigmoid colon was fenestrated using EnSeaL that was inserted through four small transverse colotomies. The 20 cm length remaining septum of the anorectosigmoid colonic duplication was dissected using a monopolar endoscopic device, SB knife Jr (TM, Sumitomo Bakelite, Japan), under colonoscopy, and anorectoplasty was performed. Postoperative course was uneventful. At the 1-year follow up, normal defecation and urination was observed.
Conclusion: Treatment of total tubular colonic duplication remains to be established. Fenestration using a linear stapling device may have adverse effect of normal growth of the colon. The present surgical technique is useful and minimum invasive.
RECTAL MUCOSAL DISSECTION COMMENCING DIRECTLY ON THE ANORECTAL LINE IN LAPAROSCOPY-ASSISTED TRANSANAL PULL-THROUGH FOR HIRSCHSPRUNG'S DISEASE
Rectal mucosal dissection is a critical step during laparoscopy-assisted transanal pull-through for Hirschsprung's disease and is conventionally commenced from a somewhat arbitrary level determined by the treating surgeon somewhere above the dentate line. This largely subjective decision making process has the potential to damage the surgical anal canal, defined as the distance between the dentate line and the anorectal line, if dissection of the rectal mucosa commences below the anorectal line, and the potential to leave an aganglionic remnant if dissection of the rectal mucosa commences above the anorectal line. At our institution, we commence dissection of the rectal mucosa directly on the anorectal line, giving surgeons a distinct landmark as an objective starting point. Briefly, our technique involves: insertion of a suction biopsy device into the colon through the anus under laparoscopic guidance until it is proximal to the area of caliber change; rectal suction biopsy until normoganglionic colon is identified; marking this level with a clip; laparoscopic dissection of the rectum/colon; transanal dissection commencing directly on the anorectal line identified by hooking the crypts on the dentate line to expose the anal canal with a Scott retractor (initially full-thickness for 2 cm then conversion to mucosectomy); insertion of a large bore silicon tube into the rectal lumen to facilitate transanal mucosal dissection. As mucosectomy progresses, the full-thickness colon proximal to the mucosectomized rectum/sigmoid colon invaginates into the rectal muscle cuff and once it reaches the anus, the rectal muscle cuff is divided circumferentially and the proximal colon is pulled-through until the level of the clip. Near total excision of the rectal muscle cuff is then performed carefully to prevent postoperative constipation secondary to rectal stenosis that can be caused by residual rectal muscle cuff. Anoplasty is completed by anastomozing the pulled-through colon to the anorectal line using interrupted absorbable sutures. Our technique eliminates all guesswork and preserves the surgical anal canal intact, ensuring that the anorectum has normal sensory and motor function. Finally, we use laparoscopy to check for torsion of the pulled-through colon, tension on feeding vessels, and confirm hemostasis.
NOTES FOR LONG-SEGMENT HIRSCHSPRUNG'S DISEASE: REPORT OF 3 CASES
Purpose: The aim of this study was to evaluate the feasibility of natural orifice translumenal endoscopic surgery (NOTES) for the management of long-segment Hirschsprung's disease.
Materials and Methods: Three children of Hirschsprung's disease who were diagnosed in our department were enrolled in this study. The extents of involved bowel were above splenic flexure in all three cases, which were too long to perform simple transanal pull-through. Our procedure was as follows: A rectal mucosectomy was performed starting 0.5 cm proximal to the dentate line and extending proximally to the level of intraperitoneal rectum. Three cannula were inserted through the muscular sleeve into the abdominal cavity. The laparoscope and operation instruments were placed in to dissect the mesocolon, lateral peritoneum and greater omentum to mobilize the colon. After the mobilization, the involved bowel segments were pull-through and resected. Finally the colon-anal anastomosis was made.
Results: All three operations were successfully performed without intraoperative complications. No additional ports or any conversions to an open procedure were required. The operative times were 242, 195 and 174 minutes respectively. All three children were discharged smoothly and followed-up for at least 1 year. The stool was 1–3 time a day. No fecal soiling or constipation was complained.
Conclusion: This NOTES procedure may be a safe and feasible option for long-segment Hirschsprung's disease, which leaves absolutely no scar on abdominal wall.
SINGLE-INCISION PEDIATRIC ENDOSURGICAL EPIGASTRIC HERNIA REPAIR
Purpose: Epigastric hernias represent about 4% of all abdominal hernias in children and require surgical repair. Traditionally, these hernias are repaired by an open surgical technique. More recently, laparoscopic epigastric hernia repairs have been described using two trocars in the upper abdomen. In this paper we describe a novel single-incision pediatric endosurgical (SIPES) technique.
Methods: Patients with symptomatic epigastric hernias that were deemed to be too far superior to be repaired with an open technique through an umbilical incision were selected for SIPES repair. Two trocars (5 mm and 3 mm) were introduced through a single umbilical incision and the hernia repair was performed using looped 4-0 polypropylene sutures introduced through a 17 gauge spinal needle in a lasso technique.
Results: Four girls (age 4.4 to 7.9, median 4.9 years) underwent single-incision endosurgical epigastric hernia repair. The mean operative time was 24±6 minutes, and there were no intraoperative complications. All patients were discharged home from the recovery room on the day of surgery. All patients were followed up 2 to 3 weeks after the operation, with no recurrence and excellent cosmetic results.
Conclusions: The described SIPES technique offers a virtually scarless, quick, and simple option for repair of symptomatic epigastric hernias that can be performed with standard laparoscopic equipment.
SINGLE INCISION PARA-AXILLARY SUBCUTANEOUS ENDOSCOPIC APPROACH IN TORTICOLLIS
Introduction: An obvious scar on the neck may appear following the open surgery for congenital muscular torticollis (CMT). The cosmetic result may displease the patient and the family. In this video, a minimally invasive technique, single incision para-axillary subcutaneous endoscopic approach (SIPASEA) in CMT was described.
Patients and Surgical Technique: Eleven children were operated for torticollis by para-axillary subcutaneous endoscopic approach. A single incision surgery in the last two patients was preferred; the rest had double para-axillary incision. The patients had torticollis with significant facial asymmetry and head and neck postural abnormality. Following an incision at the ipsilateral para-axillary region, a subcutaneous cavernous working space is formed by a balloon dilatation toward sternocleidomastoid (SCM) muscle. The muscle and fascia are cut by cautery. Both monopolor hook and bipolar cautery were used. Postoperative early and late results were satisfactory for the surgeon, the patients and the families.
Conclusions: The open surgery techniques of CMT causes visible lifelong incision scar on the neck. SIPASEA leaves a cosmetically hidden scar in the axillary region. A well-formed cavernous working space, external manual palpation, delegate dissection and cutting of SCM muscle with cautery are the important components of the procedure. SIPASEA could be considered as an excellent alternative to the open approach.
Poster Abstracts
EFFECTS OF CARBON DIOXIDE PNEUMOPERITONEUM ON INFLAMMATORY RESPONSE AND BACTERIAL TRANSLOCATION IN INTRA-ABDOMINAL INFECTION
ABSTRACT WITHDRAWN
LAPAROSCOPIC RESECTION OF THE PANCRES
ABSTRACT WITHDRAWN
INTRACORPOREAL KNOTTING SUPPORT - EXPERIMENTAL STUDY
One of the most challenging areas in the field of endoscopic surgery is knot tying. Especially sufficient first double knot (square or sliding). It needs more time, more skills and more patientce. Hence a few authors and firms have introduced pretentious and sophisticated helpers for knot tying.
Authors have suggested that more simple procedures can support intracorporeal knotting in the field of laparoscopy and thoracoscopy. The aim of this study is capacitate the suture material. It means to give him its own shape for required time. The shape from the needle to the end of the cord is: two loops and than the tail in pick up position. Authors use inert ways and means for retention of desired shape. They suggest that creation of the suturing material will simplify to arrange the first stitch (more safeness, less time).
LAPAROSCOPIC-ASSISTED PERCUTANEOUS CECOSTOMY FOR ANTEGRADE COLONIC ENEMA (LAPCACE)
Purpose: The antegrade continence enema (ACE) is an option in the management of fecal incontinence and chronic constipation. It may be administered via an appendicostomy or a tube cecostomy. Appendicostomy has a high rate of surgical revision for stenosis. We report excellent safety and low complication rates with a laparoscopic–assisted percutaneous tube cecostomy (LAPCACE).
Materials and Methods: Prospective data have been collected on 15 children (8 boys), who required ACE for fecal incontinence or chronic constipation. Success is defined as cessation of fecal soiling with no need for diapers.
Results: Mean age at cecostomy was 10 years (range 5–16 y). Mean follow up after cecostomy was 19 months (range 2–41 months). Diagnoses were myelomeningocele (1), Hirschsprung's disease (3), and intractable chronic constipation (11). Three had open surgery; 12 had laparoscopic tube cecostomy. Two had primary laparoscopic placement of a trapdoor device (Chait Trapdoor Cecostomy Catheter, Cook Medical, Bloomington, IN); 13 had placement of a long tube, with later placement of a skin level device: a Chait trapdoor or Mic-Key Low profile gastrostomy tube (Kimberley Clark, Roswell, GA) by Interventional Radiology (IR).
Initial results with primary placement of a trapdoor device were disappointing, because of patient discomfort. We now place a long Foley-type tube, which is replaced by a skin-level device after 6 weeks.
Because of ease of placement and security of fixation of the cecum to the abdominal wall, we have evolved a laparoscopic-assisted percutaneous technique, using fixation sutures on the cecum, and a dilator and peel-away sheath for introduction of the catheter. Of the 12 laparoscopic cecostomies, the first 7 had laparoscopic suturing of the cecum to the abdominal wall, and the last 5 have had T-fastener sutures (Gastrointestinal Anchor Set with Saf-T-Pexy, Kimberley Clark, Roswell, GA) placed percutaneously.
Complications occurred in 3 patients: 2 returned to the operating room, one for tube occlusion due to technical error, one for suture granuloma. One patient required intravenous antibiotics because of suspected peritonitis on the first postoperative day. These latter two complications occurred in patients who had primary placement of a Chait trapdoor device with laparoscopic fixation.
Three have had the tube removed for failure of therapy. Twelve patients are using their cecostomies. Seven patients have had a successful outcome. Four have improvement in symptoms, but still soil, and one has a poor outcome with repeated fecal impaction.
Conclusions: LAPCACE has an excellent safety profile and patient comfort. Eleven of fifteen patients have a good or improved outcome. The procedure utilizing T-fasteners is simple, secure, and with fewer technical complications than appendicostomy. Overall results in term of fecal continence are comparable to those reported with other techniques.
LAPAROSCOPIC MINIMALLY INVASIVE SURGICAL TREATMENT FOR INFANTS AND YOUNG CHILDREN WITH APPENDICEAL ABSCESS
Objective: To investigate the feasibility of laparoscopic operation in treatment of appendiceal abscess in children, and its advantages compared with traditional therapy.
Methods: The clinical data of 45 children with appendiceal abscess who underwent laparoscopic surgery from Jan. 2011 to Jul. 2011 were retrospectively analyzed. The children were 7 months to 5 years old, the time from symptoms appeared to visiting was 3–10 d.
Results: Time of laparoscopic appendectomy [75(35–130)min] and open appendectomy were similar (P>0.05). The complication rate after operation was less in laparoscopic appendectomy than in open appendectomy (P<0.05).
Conclusion: As long as the surgical and perioperative situations are properly disposed, laparoscopic treatment of appendiceal mass in infants is safe and feasible. Laparoscopic operation has obvious advantages in looking for appendix, treatment of abscess and abdominal focal irrigation.
SIMPLE APPENDIX SNARE ASSISTED TRANSUMBILICAL SINGLE INCISION LAPAROSCOPIC APPENDECTOMY
Background: Single-incision laparoscopy (SILS) has recently become popular in pediatric surgery. But this requires some special instrumentation and equipment, such as Triport, EndoEYE, Endo-Mini-shears and so on. We invented the simple appendix snare does not require special equipment to complete transumbilical single incision laparoscopic appendectomy.
Methods: We reviewed 42 children who underwent SILS between May and October 2012. 42 SILS appendectomies were performed in 28 boys and 14 girls. The mean age at operation was 8.2 years (range, 3–13 years), and the mean weight was 26 kg (range, 17–43 kg). Simple appendicitis 2 cases, seven cases of chronic appendectomy, 33 cases of complicated appendicitis. The mean operative time was 52 minutes (range, 38–75 minutes), and length of stay was 5.2 days (range, 2–7 days). Just before surgery make a simple appendix snare (the #9 syringe needle and 2-0 silk braided), the 2-0 silk braided through asyringe needle (Figure 1). Make a 1.5 cm incision in the umbilicus, through which a 12mm trocar and 5mm trocar are introduced into the abdominal cavity. In the right lower quadrant of the corresponding position of appendix, select the avascular zone, monitored in laparoscopic simple appendix snare puncture into the abdominal cavity, grasping forceps through the silk coil clamp living the appendix 's head end and pull it into the snare (Figure 2), adjust the set into the appendix length and orientation, and appendix will be fixed in the abdominal wall (Figure 3). After puncturing on the root between appendix and mesoappendix, give ligation to mesoappendix by Hem-o-lok. Then separate mesoappendix from tail to root by electrocautery, and give ligation to appendix by Hem-o-lok and remove it. Loosen the simple appendix snare, endoscopic retriever taking out the appendix from the 12mm trocar.
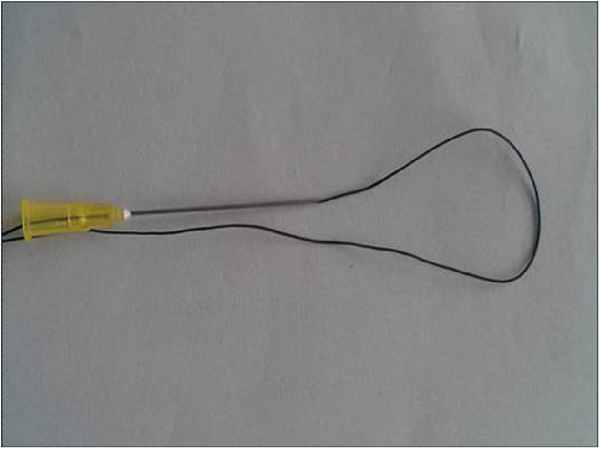
Results: In total, 1 operation (2%) required one additional 5-mm trocar to complete the operation, and none was converted to an open operation. There were no intraoperative complications, nor were there any wound infections.
Conclusion: Simple appendix snare assisted transumbilical single incision laparoscopic appendectomy is safe, feasible, more convenient, and has better cosmetic results.
THE ROLE OF LAPAROSCOPIC SURGERY IN THE TREATMENT OF INTUSSUSCEPTION
ABSTRACT WITHDRAWN
SINGLE TROCAR LAPAROSCOPIC ASSISTED COLOSTOMY IN NEWBORNS
ABSTRACT WITHDRAWN
COMBINED LAPAROSCOPIC AND MODIFIED POSTERIOR SAGITTAL APPROACH SAVING THE EXTERNAL SPHINCTER FOR RECTOURETHRAL FISTULA: AN EASIER AND MORE PHYSIOLOGIC APPROACH
Aim: To present surgical technique and results of combined laparoscopic and modified posterior sagittal approach (PSAP) saving the external sphincter in the management of rectourethral fistula.
Methods: The operation was started by a laparoscopic approach to dissect around the rectal pouch and separate the rectal pouch from the upper urethra. The modified sagittal approach was added to completely separate the rectal pouch from the urethra, and divide and close the fistula. The rectal pouch was then pulled through a tunnel created at the center of the external sphincter and an anoplasty was performed.
Results: During the study period, 19 patients were operated using the same technique. Mean age of patients was 4.0±1.8 months. Rectourethral fistula was located in the prostatic urethra in 15 patients and in the bulbar urethra in 4 patients. The mean operative time was 82±13 minutes. There were no intraoperative complications. Postoperative necrosis of the posterior wall of the rectum happened in one patient and required a second laparoscopic operation. Follow-up after closure of colostomy from 1 month–7 months revealed all patients were able to pass stool spontaneously. All patients could urinate easily. No urethral fistula nor diverticulum was detected on voiding cysto-urethography.
Conclusions: Combined laparoscopic and PSAP saving the external sphincter is the easier and more physiologic approach to manage rectourethral fistula with fewer complications.
MINIMAL ACCESS LAPAROSCOPIC SURGERY FOR TREATMENT OF ULCERATIVE COLITIS (UC) AND FAMILIAL ADENOMATOUS POLYPOSIS (FAP) COLI IN CHILDREN AND ADOLESCENTS
Background/Purpose: Total proctocolectomy is standard for treatment of symptomatic medically refractory disease, and prevention of colon cancer in patients with UC and FAP. Ileo-anal J pouch anastomosis (IPAA) is our preferred reconstructive option, performed in two or three stages. The laparoscopic approach decreases post-operative pain, and allows for quicker return to normal activity, in addition to achieving a better cosmetic outcome. In the era of single port access, minimally invasive surgeons attempt to minimize scarring by reducing the number of laparoscopic ports. The aim of this study is to review the authors' early experience with reduced port laparoscopic total colectomy and IPAA for UC and FAP and compare it to conventional laparoscopic assisted procedures using multiple ports with or without an additional small laparotomy.
Methods: Charts of children and adolescents undergoing total colectomy for UC or FAP between 2009 and 2012 at four institutions were retrospectively reviewed. Patients who had their operation performed through one or two multi-channel laparoscopic ports were assigned into the minimal access (MA) study group. Patients who had four or five single channel ports with or without an additional small laparotomy, were assigned into the control group.
Results: 22 patients were identified, 8 with FAP, 14 with UC. Ages at first operation were 2 to 18 years (median 13.5). Eleven abdominal colectomies with end ileostomy were performed, 7 MA and 4 controls. Nine completion proctectomies with IPAA and diverting loop ileostomy (DLI) were performed: 6 MA and 3 controls. Eleven proctocolectomies with IPAA and DLI, and one without diverting ileostomy were performed; 4 MA and 7 controls.
There were no conversions to laparotomy, and no mortality.
Operative Time (Op.t.) and Length of Stay (LOS)
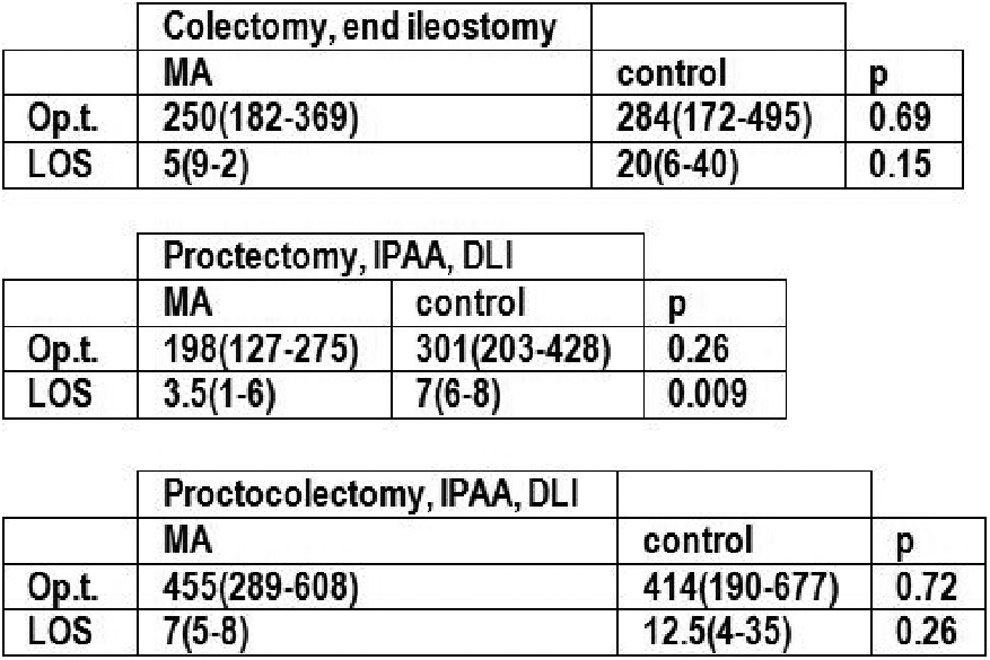
MA – Minimal Access
IPAA – Ileal Pouch Anal Anastomosis
LI – Diverting Loop Ileostomy
Op.t. in minutes: mean (range)
LOS in days: mean (range)
Complications requiring surgical correction occurred in five patients (42%) in MA group. Three required local revisions without making additional incisions (ileostomy malfunction, EEA staple line partial dehiscence, rectovaginal fistula), one required multi-port laparoscopy (retained rectum with persistent bleeding and pain), and one laparotomy (obstruction with perforation at DLI). In control group, two patients (20%) experienced major surgical complications, and required a laparotomy (both bowel obstructions requiring lysis of adhesions and revision of ileostomy).
Conclusion: Minimal access laparoscopic surgery for UC and FAP using one or two multichannel ports is safe and feasible. A slightly larger incision at the ostomy site facilitates extraction of specimen and extracorporeal construction of J-pouch. Operating times and hospital stay are comparable to multi-port laparoscopy. In our series, more surgery related complications occurred in minimal access group, but most of them were able to be corrected with minor procedures without long-term sequelae.
Objective: To evaluate the safety and feasibility of lapar-oscopic-assisted endorectal soave pull-through (LAEPT) for Hirschsprung's disease (HD) with stepwise and gradient cutting muscular cuff Methods.
Methods: We retrospectively analyzed 37 patients (31 males and 6 females, aged between 35 days to 5 years old, average age of 2.4 years old) with Hirschsprung's disease who were administrated with LAEPT in a stepwise and gradient cutting methods from December 2009 to October 2012. All the above patients were diagnosed with HD preoperatively by clinical manifestation, barium enema, anorectal manometry, endorectal mucosa and muscular layer biopsy. We improved operation methods on the basis of previous LAEPT approach, ring-shaped dissecting endorectal mucosa 0.5 cm above dentate line using aciculiform electrotome, dissecting circular and longitudinal muscles in a stepwise and gradient method, resecting rectal muscular sleeve upward to where the bottom of rectal mesentery dissected by laparoscope. Postoperative anal dilation was not routinely implemented.
Results: All patients were successfully administrated with one stage improved Soave operation without any conversion to open surgery, in which general types account for 29 cases, long segment 5 cases, HD allied disorder 3 cases, left colon resection 35 cases, subtotal colectomy 2 cases; the length of resected segment was 20∼40 cm, on an average of 32 cm. Blood loss was 5∼20 ml, mean operation time was about 150 min, with no complications happened, early defecation functions time after surgery was about 8∼24 h, mean value 16 h, postoperativehospital stays 6∼14 d, mean value 8 days. 10 cases perioperative perianal excoriation occurred (27.0%), without any anastomotic leakage or enterocolitis happening, all 37 patients were given 1∼29 months follow-up visits, mean visit periods were about 14 months, in which time 1 case constipation (2.7%), 1 case enterocolitis (2.7%), 2 case soiling (5.45%) occurred, with no anal stenosis. Excellent and good bowel function was achieved in 90% patients.
Conclusion: Improved LAEPT is probably safe and effective, patients can attain good defecating function postoperatively.
PRELIMINARY UMBILICAL DIVIDED COLOSTOMY AND TWO-STAGE LAPAROSCOPIC ANORECTOPLASTY FOR ANORECTAL MALFORMATIONS
Objectives: Majority of intermediate- and high-type anorectal malformations (ARMs) required protective colostomy, causing obvious scars to abdomen. The purposes of this study were to assess the feasibility and cosmetic results of preliminary umbilical loop colostomy and laparoscopic anorectoplasty by placing a laparoscopic port in the colostomy site in patients with ARMs.
Methods: 25 patients with intermediate- or high-type ARMs were chosen for this two-stage procedure. The skin, subcutaneous tissue, and fascia were cored out vertically. A loop colostomy was created in double-barreled fashion and the loop was divided at the same time. The two diverting ends both located in the umbilicus incision with the proximal end more than 2 cm and the distal end half closed more than 3 cm above the level of the skin. The interspace between adjacent wall of two ends were closed and the bowel wall was fixed to the peritoneum with interrupted 5-0 absorb-able sutures. 2–3 months later, the stoma was closed, and laparoscopic-assisted anorectoplasty was performed by placing a laparoscopic port in the colostomy site for laparoscopic rectum mobilization, fistula repair and anorectal anastomosis.
Result: Preliminary umbilical divided colostomy and laparoscopic anorectoplasty were successfully created in 25 patients (15 males and 10 females) aged 1 days to 5 months, 3 cases with rectourethral fistula, 7 with rectobladderneck fistula, 5 with rectovestibular fistulas and 10 without fistulas. Postoperative complications were carefully observed. One patient had mucosal prolapse in umbilicus. No wound infection, parastomal hernia, obstructive symptoms, skin problems, spontaneous umbilical ring narrowing was observed. Stoma care could easily be performed by attaching stoma bag. Healing of umbilical wounds after colostomy closure and laparoscopic procedures was excellent. Early functional stooling outcome were satisfactory.
Conclusions: The umbilicus may be an alternative stoma site for colostomy in neonates or infants with intermediate- and high-type anorectal malformations, who undergo laparoscopic anorectoplasty. This procedure provided good cosmetic and functional results; it proved to be feasible and safe in early outcomes.
MINIMALLY INVASIVE PULL-THROUGH (MIPT) IN HIRSCHSPRUNG'S DISEASE
Introduction: Hirschsprung's disease causes hyperplasia of upstream ganglion cells connected with increased excretion of acetylcholine while aganglionosis dominates the submucosal and myenteric plexus. Consequently, a permanent stimulation of the circular part of the muscles at least leads to functional anorectal stenosis.
Materials and Methods: Minimally invasive pull-through (MIPT) is feasible in children from a weight of 6 kg upwards. Umbilicus is the main access (12 mm trocar), two more trocars are placed laterally in the lower abdomen. Mobilization of the recto-sigmoid is accomplished by piezoelectric technique. During the dissection, rectum is pulled by atraumatic forceps, dissection is proceeding down to the pelvic floor. Changing the laparoscop to one of the lateral trocars, a 12 mm stapler is inserted. The rectum is cut by leaving a stump. Orally, another cut is made and the specimen is retrieved via umbilicus. Intraoperatively, the oral edge is checked by the pathologist to have information about concentration of ganglion cells. If necessary, piezoelectric mobilization is continued and another oral resection is performed with another histopathologic check. The next step is the ultimate resection of the anorectal tube: The staple line of the rectal stump is bitten by a forceps proceeding there via the anus. The stump is pulled outside. After transverse opening of the everted stump some holding sutures keep the stump everted. Once again the forceps is introduced from outside into the rectal stump and the aboral edge of sigmoid colon is gripped and pulled through the rectal stump. After another externally performed resection of the rectum, the stump is now about 4–5 cm long, an extracorporeal anastomosis is applied by single sutures. After finalizing the end-to-end anastomosis, an inverted pull-through is made laparoscopically to bring the rectal stump back into the small pelvis.
Results and Summary: During 2010–2012 16 children (5.7–9.5 kg) had the 3 trocar-MIPT. 3 pat. had preexisting Nixon colostomy which was kept 6 weeks further in all cases. There were no complications, e.g. peritoneal inflammation, leakage of the anastomosis, ileus or malperfusion. Feeding started day 2 postop, stool deposition took place day 2 or 3. Stay on ward took 5–7 days. The naturally remaining aganglionosis with the rectal stump is considered high-pressure zone, comparable to the sphincteric structure. It was learned during performing the external anastomosis, that the distance between linea dentata and the anastomosis is not feasible under 1 cm of length although concise preparation. All patients needed to keep a stool-diary. 5 patients were evaluated for relaxation of the internal sphincteric muscle by botulinum-injection 3–6 months postop with a single or double retake after 8–10 weeks with acceptable results in all patients. 3 trocar-MIPT is a simple laparoscopic procedure which can be performed safely by piezoelectric technique. The combination with extracorporeal arrangement of the anastomosis is convincing and facilitates creating safe sutures.
LAPAROSCOPIC-ASSISTED ANORECTAL PULL-THROUGH FOR CLOACAL MALFORMATION
Purpose: Persistent cloacas are complex genitourinary/anorectal anomalies and its surgical treatment is challenging. Abdominal approach is often necessary, especially if the common urogenital channel is deep. Laparoscopic approach is frequently used in anorectal malformation treatment with excellent results. Our aim is to present our technique and early outcomes of laparoscopic anorectal pull-through in the management of cloacal malformation.
Subjects and Methods: We performed laparoscopic assisted anorectal pull-through in 2 patients with cloacal malformation. Left colostomy was fashioned during the neonatal period. The common urogenital channel length was 2.5 and 4 cm respectively and their surgical repair was performed at 18 and 6 months respectively. The first girl's surgery was delayed because she had some difficulties to grow (7.7 kg at 18 months). Our technique used 4 trocars: 5-mm trocar in the umbilicus for the scope, 3-mm trocars 3 cm in the right and in the left of umbilicus and 3-mm trocar in the left iliac fossa. Rectum was dissected circumferentially, mobilized and the fistula between the rectum and the urogenital sinus was tied and sectioned (figure: A: vagina, B: recto-vaginal fistula, C: rectum).
After perineal dissection, the rectum was pulled out after identification of the levator muscles. Urogenital malformation was repaired by total urethral mobilization during the same operative procedure.
Results: There was no intraoperative or postoperative complication. Length of stay was 16 and 12 days respectively. The colostomy was closed at 9 and 3 months. The anal calibration was pursuing during 4 months after the closure. At the last follow-up, the local aspect was good with a mucosal prolapse for one patient but the anus was calibrated easily by a size-12 dilator. The two patients have a laxative treatment and are not yet continent. The first patient (29 months old) has some soiling with stool impaction and the second (15 months old) is constipated.
Conclusion: These two cases demonstrate that laparoscopic-assisted anorectal pull-through is safe and effective in cloacal malformation. This technique gives optimal view of the pelvic organs and minimizes abdominal scars. Urethroplasty and vaginoplasty can be performed during the same procedure. Multicenter study and long-term follow up are necessary to evaluate this surgical repair.
INTRA-ABDOMINAL VENOUS THROMBOSIS AFTER COLECTOMY IN PEDIATRIC PATIENTS WITH CHRONIC ULCERATIVE COLITIS: INCIDENCE, TREATMENT, AND OUTCOMES
Purpose: Children with chronic ulcerative colitis are at increased risk for venous thromboembolism, especially after total colectomy with ileoanal anastomosis. We reviewed our ulcerative colitis population to identify those who developed symptomatic intra-abdominal thrombus after surgery and to better understand the efficacy of our anticoagulation.
Methods: Patients (≤21 years of age) who underwent colectomy for chronic ulcerative colitis from January 1999 to December 2011 were included, and their records were retrospectively reviewed for development of symptomatic intra-abdominal thrombosis (portal, mesenteric, splenic, or hepatic vein).
Results: Of 366 patients who underwent colectomy, 15 (4%) were diagnosed with a venous thromboembolism. All of the patients presented with acute abdominal pain. The locations of thrombus formation varied: 13 (87%) developed thrombi in the portal vein, 4 (27%) in the splenic vein, 2 (13%) in the superior mesenteric vein, 1 (7%) in the hepatic vein, and 1 (7%) in the hepatic artery. The mean number of post-operative days at the diagnosis of thrombus was 38.7 days (range 3–180 days). Thirteen patients (93%) underwent anticoagulation for treatment. Eight patients were initially anticoagulated with low-molecular weight heparin (dalteparin sodium) and subsequently sent home on Coumadin. Four patients were treated with dalteparin sodium only. One patient was treated with aspirin only. The remaining two patients' thrombi dissolved without anticoagulation. The mean number of days until documented resolution on imaging was 96.3 days (range 14–364 days). There was no mortality during follow-up.
Discussion: We conclude that 4% of our patients with chronic ulcerative colitis who underwent colectomy developed symptomatic venous thromboembolism. Given the low incidence of this complication, we believe that the bleeding risk associated with prophylactic anticoagulation outweighs the benefit of preventing thrombi formation. Our data suggests that 3–6 months of anticoagulant therapy is sufficient for the resolution of symptomatic venous thrombi.
LAPAROSCOPIC ANORECTOPLASTY FOR INTERMEDIATE ANORECTAL MALFORMATION (ARM): MIDDLE AND LONG TERM OUTCOME
Introduction: Laparoscopic assisted Anorectal pull-through (LAARP) is becoming an increasing common procedure to correct Anorectal malformation. The aim of review was to evaluate experience with LAARP with regard to especially intermediate type (recto-urethral fistula) of ARM with middle and long term outcome.
Methods: From March 2005 to August 2011, 12 patients with Anorectal malformation of intermediate type underwent follow-up. All the cases as a first stage made with diverting colostomy and underwent LAARP at 3 to 7 months (average 4.67±1.23) of age. Post-operative recovery uneventful. Diverting stoma were closed 3 months after LAARP. Patients were follow-up from 1.2 to 7.5 year (mean 4.14±1.90). The postoperative assessment evaluated by international classification (Krickenbeck) applied.
Results: The average operating times were 179.17±19.28 minutes. Post-operating complication were rectal prolapsed in 4 cases (33.3%) and no patient had post-operative bleeding, infection, urethral diverticulum or recurrent recto-urethral fistula encountered. 10 patients out of 12 were followed more than 3 years so we can evaluate 10 patients according to international classification (krickenbeck) for post-operative result. The result shows that 10 patients (100%) having voluntary bowl movements, 3 out of 10 patients (30%) developed grade 1 soiling and 1 out of 10 patients (10%) developed grade 1 constipation.
Conclusions: Although longer follow-up to evaluate post-operative complication is to come. The laparoscopic approach for intermediate type of imperforate anus is feasible and safe control of the fistula and helped to determine the accurate passage through the levetor ani.
LAP ASSISTED TRANS ANAL PULL THROUGH: DOES THE EXTENT OF RECTAL DISSECTION MAKE AN IMPACT ON THE OUTCOME?
ABSTRACT WITHDRAWN
SINGLE-INCISION LAPAROSCOPIC ASSISTED ANORECTOPLASTY USING CONVENTIONAL INSTRUMENTS FOR CHILDREN WITH HIGH ANORECTAL MALFORMATIONS
Background: Single-incision laparoscopy has been increasingly utilized in pediatric surgery. The current study is the first series to evaluate the safety and efficacy of single-incision laparoscopic assisted anorectoplasty (SILAARP) for children with high anorectal malformations.
Methods: Patients with high anorectal malformations who underwent SILAARP between May 2011 and December 2011 were reviewed. Surgeon stood on the patient's left side. Camera assistant stood on the patient's right side. A 2 cm vertical umbilical incision was made. An extra-long 5-mm 30° laparoscope was inserted through camera port which was placed in midline fascial incisions. Two 3-mm conventional laparoscopic instruments were inserted through working ports which were placed bilateral to camera port at the ends of horizontal umbilical incision. The bladder was evacuated and the retraction stitch was placed through abdominal wall and anterior bladder wall to create the working space. Laparoscopic rectal dissection was performed from peritoneal reflection to the rectourethral fistula. The distal mesorectum was divided by hook cautery along anterior and lateral rectal wall. The fistula to the urethra was identified and transected at the insertion on the posterior urethra. The telescope was rotated 180 degree to detect the transected fistula. The stump of fistula was closed by 5/0 PDS suture. The internal midline identification was based on the location of the distal end of the divided fistula and urethra. The anal area of the perineum was mapped using transcutaneous electro-stimulator externally. A 1 cm vertical midline incision was made in the perineum at the site of the proposed anal orifice. The intrasphincteric plane was dissected bluntly from below to the level of the levator sling using laparoscopic backlighting. A tissue grabbing forceps was passed through the intrasphincteric plane and advanced between the 2 bellies of the pubococcygeus muscle in the midline using laparoscopic guidance, just posterior to the urethra. The rectum was pulled through the midline of external sphincter and levator ani to the perineal wound by the grabbing forceps. The anastomosis between rectum and anus was completed with interrupted 5-0 PDS suture. Early postoperative and follow-up results were analyzed.
Results: Ten patients (median age at operation: 5.16 months, range: 3.43–9.5 months, M/F: 8/2) successfully underwent SILAARPs without conversions. The mean operative time was 2.21 hours (1.83–3 hours). Intraoperative blood loss was minimal. No blood transfusion was required. Mean postoperative hospital stay was 8.8 days (7–10 days). All patients resumed full diet on postoperative day 1. The median follow-up period was 15 months. No injuries of urethral or vas deferens occurred intraoperatively. Postoperative MRI showed that all patients had a centrally placed rectum within the muscle complex. No mortality or morbidities of wound infection, rectal retraction, anal stenosis, mucosal prolapse, recurrent fistula, or urethral diverticulum was observed.
Conclusions: In experienced hands, SILAARP is safe, feasible and effective. In future, combined transumbilical colostomy1 and SILAARP will achieve the goal of scarlessness in children with high anorectal malformation.
1. Hamada Y, Takada K, Nakamura Y, Sato M, Kwon AH. Temporary umbilical loop colostomy for anorectal malformations. Pediatr Surg Int 2012;28(11):1133–6.
TRANSANAL AND RETRORECTAL DUHAMEL PULL THROUGH NOVEL MODIFICATION
ABSTRACT WITHDRAWN
SURGICAL TREATMENT OF SECONDARY MEGARECTUM IN CHILDREN
Actuality: Unsatisfactory results of surgical treatment of secondary megarectum and a high percentage of complications after application of manual rectal intestinal anastomosis.
Materials and Methods: for 2010–2012, in the Department of Surgery, RAMS NTSZD, surgical treatment of 22 children with secondary megarectum in age from 7 to 14 years. In these patients over the past 2–3 years, noted the absence of an independent stool, incontinence episodes of intestinal contents, and the conduct of repeated courses of conservative therapy (enemas, laxatives, electrical, etc.) do not lead to improvement. For the diagnosis of preoperative rectum Swenson biopsy the results of which 40.9% have been identified gipogangliozis, at 36.4% of intestinal neuronal dysplasia, degenerative changes rectum occurred in 100% of patients. Operation of choice is laparoscopic-assisted hemicolectomy with the imposition of a circular low rectal anastomosis end hardware in the side. Level colon resection was determined intraoperatively using special laparoscopic ultrasound probe.
Results: The radical surgery lasted from 2 to 4 hours and is directly dependent on the thickness of hyperinflate colon. Fistulization of them took no more than 15–25 minutes, which greatly speeds up operations and improve accessibility to the rectum. It is important to note that in any case, no postoperative anastomotic failure was noted with the development of pelvic peritonitis. In catamnesis, 3 months, improved function of the colon were detected in all operated patients.
Conclusion: All of the above leads to the conclusion that the conduct of laparoscopic-assisted gemicolektomy hardware overlay low anastomosis is the operation of choice in the treatment of secondary megarectum.
SINGLE-INCISION LAPAROSCOPIC-ASSISTED DUHAMEL PROCEDURE FOR LONG-SEGMENT HIRSCHSPRUNG'S DISEASE WITH COLOSTOMY
Objective: To explore the feasibility and effectiveness of single-incision laparoscopic-assisted Duhamel procedure for the subtotal colectomy through the original incision after colostomy treating the long-segment Hirschsprung's disease (HD).
Methods: From March 2011 to September 2012, 7 children that were encountered a transverse colostomy in newborn with long-segment HD were performed single-incision laparoscopic-assisted Duhamel procedure using the original incision after colostomy. A Triport was placed through the small original incision after mobilized and resected the colostomy. Under the laparoscope, the ascending and sigmoid colon was freed, then the sigmoid colon was invaginated and excised through endorectum extracorporeally. The ascending colon using Deloyers' maneuver was withdrawn through the post-rectal tunnel, an Endo-GIA device was inserted through the anus to stape and divide the posterior rectal wall and the anterior colonic wall.
Results: All of 7 children were successfully completed single-incision laparoscopic-assisted Duhamel procedure. The operation time was 155–210 minutes. The estimated blood loss was 5–15 ml. There were no perioperative complications. During the post-operative short-term follow-up, the curative effects were satisfied. The stool pattern was improving gradually. The anastomotic stricture, constipation recurrence and fecal incontinence weren't observed.
Conclusion: Using the original incision after colostomy, single-incision laparoscopic-assisted Duhamel procedure for subtotal colectomy treating long-segment HD is safe, effective and feasible, without more incisions to set trocars. This technique for two-stage HD operation is more reasonable and minimally invasive than traditional operations.
NATURAL ORIFICE TRANSANAL ENDORECTAL SOAVE PULL-THROUGH FOR SUBTOTAL COLECTOMY UNDER LAPAROSCOPIC GUIDANCE
Objective: To explore the feasibility and safety of natural orifice transanal endorectal Soave procedure for long-segment Hirschsprung's disease under the laparoscopic guidance.
Methods: An 11 month infant with extended Hirschsprung's disease underwent a laparoscopic-assisted Soave pull-through procedures. We modified this technique by obtaining some seromuscular leveling biopsies of the sigmoid and transverse colon and mobilizing the whole colon via rectal muscular sleeve approach under single-port laparoscopic vision in the umbilicus, then transanal endorectal pull-through to complete the subtotal colectomy.
Results: The procedures were completed successfully. The operative time was 155 min. The period of the full bowel action was 1 day. His bowel movement frequency changed from 5–15 per day latest postoperatively to 3–5 per day after 2 months. The clinical outcomes were excellent with no stool incontinence or constipation.
Conclusions: Transanal Soave pull-through subtotal colectomy with single-port laparoscopic guidance is a safe, effective and feasible procedure, with more minimal invasion, invisible scars in the abdomen, and nearly the cosmetic result of NOTES.
KOLLMAR'S PORT PLACEMENT FOR LAPAROSCOPIC APPENDECTOMY IN CHILDREN AND ADOLESCENTS: SINGLE CENTRE EXPERIENCE
Background: Since the introduction of laparoscopic appendectomy (LA), has been subjected to many modifications. LA is usually done through three ports. The mode of port insertion and control of appendiceal stump represent the two crucial issues of LA.
Objective: To assess the operative feasibility and cosmesis in LA comparing Kollmar's approach (KLA) and conventional LA approach (CLA) in children and adolescents.
Materials and Methods: In a prospective assessment study along 30 months, fifty four consecutive patients with non complicated acute appendicitis of pediatric and adolescent age group underwent laparoscopic appendectomy in a single academic institution. Age ranged between 5 and 21 years. Cases were evaluated for length of hospitalization, length of operation, complications, conversion rate and intra-operative diagnosis of other pathologies.
Results: Twenty five cases have been operated by KLA and 29 cases of CLA. All laparoscopic procedures were completed without conversion. In either technique, we employ 2 working ports added to the port for telescope. Operative time ranged between 45 and 85 minutes in KLA as compared to 50–75 minutes in CLA while hospital stay and other pathologies are similar in both groups. There is no significant difference in morbidity among children between both groups. Complications reported as 4/25 in KLA (3 port site infection and small intra abdominal collection in one case) and 5/29 in CLA (3 port site infection, early adhesive obstruction once and intra abdominal collection once). All complications responded to conservative treatment. Despite that the KLA showed longer operative time and need more expertise, the cosmetic results is superior to CLA group.
Conclusions: The authors observed a higher cosmetic satisfaction in KLA group. Despite that the abdominal room is different in children from adults; KLA is effective, feasible and safe in children as well as adolescents with zero conversion. The surgical skill improvement is positive related with reduction of operative time. Larger studies and long-term follow up are needed to support our encouraging results.
JOINT APPLICATION OF LAPAROSCOPY AND HYSTEROSCOPY FOR THE “PELVIC MASS” OF A FEMALE NEONATE: A CASE REPORT
ABSTRACT WITHDRAWN
NEEDLE-ASSISTED LAPAROSCOPIC INGUINAL HERNIA REPAIR IN CHILDREN: EXPERIENCE IN CHITTAGONG, BANGLADESH
ABSTRACT WITHDRAWN
LAPAROSCOPY-ASSISTED CUTANEOUS URETEROSTOMY AT SUPRAPUBIC CREASELINE FACILITATES SUBSEQUENT REIMPLANTATION
ABSTRACT WITHDRAWN
EXTERNAL SQUEEZE TEST (EST) DURING LAPAROSCOPIC HERNIA REPAIR; A NOVEL ON-TABLE ASSESSMENT TECHNIQUE TO PREVENT RECURRENCE OF HERNIA
Objectives: Recurrent inguinal hernia after laparoscopic hernia repair most likely occurred secondary to incomplete closure of the patent process vaginalis (PPV). We introduced the “External Squeeze Test” (EST), a simple assessment tool to test effectiveness of our port-free purse-string technique for laparoscopic inguinal hernia (IH) repair. We reviewed all cases with and without EST and the recurrence of IH after laparoscopic repair at our centre.
Methods: This was a retrospective and prospective review of laparoscopic IH repair at our institution from December 2007 to October 2012. At laparoscopy, during the CO2 insufflation, the gas would flow into the scrotum or labia majora through the PPV, leading to a visible distension of scrotum or labia. Closure of PPV was achieved via creation of purse-string over the inguinal ring with avoidance of important structures i.e. vas deferens. We then performed the EST; we lightly squeezed the scrotum or labia majora whilst the telescope remained focus at the pursed area. If the purse-string created was incomplete, the act of squeezing would cause escape of gas within the scrotum or labia back into the peritoneal cavity and visualized as air bubbles internally; this was taken as a positive EST. A positive EST meant the process vaginalis was still patent, therefore careful additional suturing must be carried out at the area where the bubbles leaked. A complete hernia repair would not produce any bubbles internally upon external pressure, this would be taken as a negative EST.
Results: A total of 260 patients underwent laparoscopic IH repair during this period. Eighty patients also had contralateral PPV which were closed at the same sitting i.e. a total of 340 PPVs were repaired. EST was performed in 256 patients (98.46%) or 336 PPVs (98.82%). EST was not performed in 4 patients (1.54%) or 4 PPVs (1.18%). Five patients had recurrence of the inguinal hernia (1.92%). One of the recurrences happened in a patient who had EST; this was attributed to a slipped ligature; confirmed during the second repair. The other 4 recurrences were all in patients who EST was not performed. Two recurrences occurred before EST was introduced. The other two recurrences were after EST was introduced; by a surgeon who preferred not to do it. All the recurrences were re-repaired via laparoscopy.
Conclusion: EST is a simple, useful and excellent assessment tool for us despite an unfortunate single recurrence of IH in the EST group. We recommend this novel technique for every type of laparoscopic hernia repair especially when the patient has a large inguinal hernia.
LAPAROSCOPIC ASSISTED DELIVERY OF INGUINAL HERNIA SAC THROUGH A MICRO-INCISION AND EXTRAPERITONEAL DIVISION AND LIGATION OF THE HERNIA SAC
Objective: High ligation and division of inguinal hernia is the standard and time tested method in a pediatric open inguinal hernia repair. We describe a laparoscopic method of delivering the hernia sac through a 5 mm micro-incision and extraperitoneal division and ligation of the hernia sac.
Methods: An umbilical port is placed for insufflation and insertion of a thirty degree scope. A needle is inserted through the inguinal skin to locate the position of the internal inguinal ring. The tip of the needle is laparoscopicaly observed as it touches the anterior aspect of the hernia sac about 5 mm distal to the internal ring. A 5 mm incision is made on the skin to introduce a sharp mosquito clamp. The clamp is bluntly pushed through the external oblique fascia and observed with the laparoscope to anteriorly indent the hernia sac. Once the overlying tissues are completely cleared using the clamp, the clamp is used to pull the sac toward the skin. When the sac is externally visible, it is reclamped and pulled outward as adherent tissue is dissected off with a Debakey forceps similar to the standard open technique. When it is delivered sufficiently and the cord structures are pushed down, the sac can be opened to confirm the hernia structure. It is then divided and high ligation is done. The laparoscope is reinserted to confirm ligation.
Results: 72 inguinal hernia repairs were done using the laparoscopic assist method in 54 patients (34 boys, 20 girls). Mean age was 51 months or 4.3 years (range: 1.5–180 months). Mean follow-up at one year showed one recurrence. There were two conversions: one patient was found to have a direct hernia and another patient had a history of two open hernia repair, and the scar was prohibitive.
Conclusion: Our laparoscopic assisted inguinal hernia repair combines the advantage of open repair and laparoscopic contralateral examination. There is minimal scarring, and the recurrence rate is similar to an open operation.
A KIRSCHNER WIRE MAKES THE TREATMENT OF PEDIATRIC INGUINAL HERNIA EASIER
Background: There are many different techniques for laparoscopic inguinal hernia repair in children. For hernia hook method, a 5-mm port is inserted at the umbilical region for insertion of a 5-mm laparoscope and a 3-mm grasper is then introduced for working. Here we introduce a new method that is to taking a 1 mm diameter Kirschner wire instead of the working instrument (3-mm grasper). It makes operation simple and can prevent injury spermatic cord.
Methods: Between February 2010 and July 2012, 108 pediatric patients with inguinal hernia were treated with laparoscopic technique of sac intracorporeal ligation. We use hernia hook repair technique. Briefly a 5-mm port is inserted at the umbilical region for insertion of a 5-mm laparoscope. A 1 mm diameter Kirschner wire was inserted from middle line of hypogastric region to help hernia hook closing the deep ring. The asymptomatic contralateral patent processus vaginalis (PPV) were repaired with same method. Patients were routinely followed for 3 month to 2 years. Perioperative complication and recurrence rate were evaluated.
Results: In total 108 patients were enrolled in final analysis. The mean follow-up period was 8.5 months. Percentage of contralateral PPV was 39%. Mean operation time was 15 minutes for unilateral hernias and 33 minutes for bilateral hernias. No perioperative complications were found. Recurrence and metachronous hernia were not observed so far.
Conclusion: Using a Kirschner wire to help finishing hernia repair technique is safe. It can shorten operation time and prevent side-injury.
HOW TO ADVANCE A 10-MM CLIP THROUGH A 6-MM WORKING CHANNEL: NOVEL DEMOUNTABLE CLIP APPLIER FOR TRANSUMBILICAL SURGERY
Single-incision laparoscopic surgery (SILS) has emerged as a viable alternative to conventional laparoscopy. In our institution, during SILS, it is customary to use an 11-mm, 0° laparoscope (27-cm long) with a 6-mm working channel that is inserted through the 12-mm trocar. In many situations, we have faced the need to apply large (>5 mm) clips, but current appliers for such clip size do not fit into the 6-mm working channel. We created a demountable clip applier that allows the application of large clips through a 6-mm working channel. This novel applier has three demountable parts: 1) a shaft (5 mm in diameter and 45 cm length), 2) a flexible hinge for 10 mm clippers and 3) standard handles for hinge maneuver. In order to fit the applier into a 6-mm working channel, we first advance backwards the shaft with the already assembled hinge into the end of the working channel and then introduce the scope and the applier en bloc into the 12-mm trocar, under laparoscopic vision. Then, we assembled the handles to the shaft, located at the proximal end of the working channel.
LAPAROSCOPIC AND ENDOSCOPIC PANCREATIC CYST-GASTROSTOMY
In this video, we present a 6 year old boy with a pancreatic pseudocyst. Using a combined endoscopic and laparoscopic technique, a pancreatic cyst-gastrostomy is performed. Instead of making a large incision in the anterior gastric surface, the endoscope is used for visualization, and a trocar is placed directly into the stomach for instrumentation. After the cyst-gastrostromy is created, the trocar defect is then converted into a gastrojejunostomy site.
A SAFE TECHNIQUE FOR UPSIZING PEG DEVICE TO LARGER CALIBRE BUTTON GASTROSTOMY
Background: PEG to gastrostomy buttons change is frequently performed under gastroscopic guidance, utilising solid, unyielding dilators. This has the potential for the gastrostomy tract to be lost. Likewise, blind dilatation of the gastrostomy tract risks creating a false passage with the button being placed outside the stomach.
Aim: We describe a safe, more controlled technique for changing primary gastrostomies to a larger calibre gastrostomy button. We demonstrate how this technique has been utilised without any significant complications.
Methods: A reusable guide-wire is passed through the tract (of the removed PEG) along which is passed a series of oesophageal-type dilators to achieve the required calibre. The gastroscope allows direct visualisation of the guide-wire position and dilatation process. Sequential, standard length measuring device and button gastrostomy are railroaded over the wire.
Results: This technique has been used successfully by the senior author for the last 10 years. Patients who had their initial gastrostomy tube (9Fr.) placed during a fundoplication were entered prospectively into a database, in addition electronic operative records were queried for the change of gastrostomy procedure. Thirty five patients were identified by this method. Patients ranged from 0–17 years old (mean 4.5 years) and they had an average weight of 14 kg. Of these 35, 19 were female. All underwent a change of PEG to button gastrostomy device (12 Fr.) by the described technique. No complications occurred following the change of gastrostomy.
Conclusion: We believe this technique offers a controlled method for the dilatation of an unwieldy tract, which is necessary to allow introduction of a balloon gastrostomy following initial PEG placement. Maintaining the guide-wire in the gastrostomy tract throughout the change eliminates the risk of creating a false passage.
PERCUTANEOUS OWN SUTURE TECHNIQUE FOR CLOSURE OF CONGENITAL DIAPHRAGMATIC HERNIA IN CHILDREN
In the treatment of congenital diaphragmatic hernia various surgical techniques are used, according to magnitude and localization of diaphragm defect. Suturing tissue very close to the chest or abdominal wall is difficult because of instrument limitation.
The aim of our study was to present own technique of percutaneous suturing as a way of diaphragm defect closure close to the body wall.
Presented technique was primarily developed in Pediatric Surgery and Urology Department in Medical University of Wroclaw, for laparoscopic internal inguinal ring closure in the treatment of pediatric inguinal hernia called PIRS technique. In laparoscopy the internal inguinal ring is visualized and enclosed with a thread loop, by specific maneuvers of an injection needle pierced through skin over the internal inguinal ring. This technique was also applied for diaphragmatic defect closure in 5 children presented with right or left side defect as supplementary technique to attach the lateral fragment of diaphragm to the chest wall. In two cases this technique was sufficient to repair the total retrosternal diaphragm failure. In all cases adequate closure of the diaphragm defect was achieved.
The percutaneous suture technique under visual control seems to be helpful and successful way for diaphragm defect repair.
THE SCARLESS UMBILICAL PORT INSERTION (SUPI) TECHNIQUE FOR LAPAROSCOPIC SURGERY IN CHILDREN
Abstract: We describe a technique of camera port insertion through the umbilicus for laparoscopic surgery in children which is scarless and has outcomes favourable to standard infra and supraumbilical techniques.
Background: The umbilical defect closes following physiological intestinal embryological herniation in the majority of children but the reminders of its embryological past remain in it its anatomic relations. It is considered by some as a natural orifice suitable for endoscopic cannulation. It is of note that the absence of subcutanous fat, and muscle at the umbilicus facilitates port placement.
The majority of camera port insertions are performed through supra and infra umbilical incisions. The concerns being the umbilicus is a poor site for laparoscopic port placement due to an increased risk of wound infection and incisonal hernia. There are no papers in the adult or Paediatric literature that support these concerns.
Technique: We insert laparoscopic camera ports, both 5 mm and 10 mm, via the umbilical route in neonates, infants and child. After meticulous cleaning of the umbilicus with betadine, the central ‘axal’ of the umbilicus is incised with a straight blade with extension caudally and cranially, remaining within the scar of the umbilicus. The wound is deepened in the midline plane and transversalis and umbilical fascias are divided under direct vision. Once divided the peritoneum is visualised, picked up and opened. The port with trocar is inserted and pneumoperitoneum established. Following the procedure the umbilical ring is closed, with the fascia ring brought together obliquely with 2.0 vicryl and the umbilical scar tissue is opposed with 4.0 vicryl.
Methods: Outcome data was taken from a prospectively maintained database identifying all children undergoing laparoscopic surgery over 4 years, Jan 2008 – August 2012. Follow up is to date.
Results: 292 children, ranging from 2 weeks to 16 years, underwent urological, pelvic and gastrointestinal laparoscopic surgery. SUPI was feasible in 288, and 4 were excluded from the data due to operative conversion. 63 children had 11 mm ports and 226 5 mm. There were no operative complications of the SUPI technique. Difficulties were found in one case due to an elongated umbilical stump. 2 children were noted to have umbilical hernias at the time of surgery, with no sequelae. 1 child developed a wound infection, requiring oral antibiotics and drainage and 2 children developed minor wound infections which responded to topical antibiotics. In 3 children incisional umbilical hernias were noted post operatively, but all resolved spontaneously.
Conclusion: We suggest that the advantages of the scarless umbilical port insertion (SUPI) technique outweigh the theoretical disadvantages. Technical advantages include ergonomic access for visualisation of all areas of the abdominal cavity; the dissection plane remains bloodless to the peritoneum and there is virtually no fat if in the correct plane. Our data shows if meticulous attention is made to cleaning, haemostasis and fascial closure the rates of both infection (1%) and ventral herniation (1%) are favourable to those described for standard entry sites and leave the child with no abdominal camera port scar.
TRANS-ESOPHAGEAL H-TYPE TEF EVALUATION AND CANNULATION USING A SIDE-VIEWING FLEXIBLE ENDOSCOPE, A NOVEL TECHNIQUE FOR GUIDEWIRE PLACEMENT DURING SURGICAL REPAIR
Background: Congenital tracheoesophageal fistula without esophageal atresia (H-type TEF) is an unusual entity that typically presents in the first months of life with clinical signs of aspiration. Repair is usually facilitated by placement of a catheter or wire through the fistula during rigid bronchoscopy. This cannulation allows the surgeon to identify the fistula during dissection of the neck. We describe a case of H-type TEF in which the fistula could not be identified on rigid bronchoscopy but was only visible on esophagoscopy. Cannulation of the fistula was therefore achieved using video-esophagoscopy.
Technique: The patient is a male born prematurely at 34 weeks who was small for gestational age. Respiratiory distress was noted in the first day of life and a contrast study revealed the H-type TEF. Rigid bronchoscopy failed to identify the fistula and primary repair at this time was aborted since, although the fistula was noted on esophagoscopy, the scope did not allow for cannulation given the acute angle of the fistulous opening on the esophageal side. A repeat procedure was undertaken with video-esophagoscopy. The opening was identified and cannulated using a pediatric side-viewing duodenoscope and a slim (5 French) tapered ERCP cannula (Mini-Tome, Wilson-Cook, USA). A .021 soft GI guide-wire (Wilson-Cook, USA) was then placed through the ERCP cannula. Wire placement was done under video and fluoroscopic control. The surgical repair was then performed with the guide-wire in place.
Conclusions: Primary repair of an H-type tracheoesophageal fistula is usually aided by placing a cannula or guide-wire through the fistula under bronchoscopy. In this case, failure to place a wire was due to high takeoff of the fistula within the hypopharynx and difficulty visualizing the opening from the tracheal side. Transesophageal evaluation and guide-wire placement using a side-viewing duodenoscope was undertaken and was successful in this one case. Placement was relatively smooth and atraumatic when compared with rigid bronchoscopy. This index case validates the use of this technique. Expanded experience with this technique would be needed to clarify questions regarding safety and reproducibility. In complex cases with difficult fistula cannulation during bronchoscopy, this technique offers another option for TEF guide-wire placement prior to repair.
LAPAROSCOPIC APPROACH OF A PANCREATIC TUMOR
ABSTRACT WITHDRAWN
ESOPHAGO-BRONCHIAL FISTULA IN A 2 YEAR OLD CHILD TREATED WITH A COMBINED COIL AND GLUE EMBOLIZATION
Introduction: Esophago-bronchial fistula (EBF) after esophageal atresia (EA) with trachea esophageal fistula (TEF) repair is extremely rare. There are no cases reported in literature. It is difficult to treat these fistulae with other minimally invasive techniques described for repair of recurrent TEF.
Case Report: A 2 year old boy who had undergone EA with TEF repair at an outside hospital at birth presented with choking and coughing after feeds and recurrent pneumonia.
Esophagogram revealed EBF between the middle third of esophagus and a subsegmental bronchus of the posterior segment of right upper lobe. Rigid bronchoscopy did not reveal a TEF. The child was made NPO and a Laparo-enodoscopic Gastrostomy tube (LEGT) was placed for feeding.
We describe a novel minimally invasive technique for the treatment of this extremely rare condition.
Materials and Methods: The case records of the child were retrospectively reviewed.
Technique: First attempt: A Pediatric esophagoscope was advanced into the middle third of the esophagus and the EBF was demonstrated. A 3F JB-1 catheter was advanced through the oral cavity under esophagoscopic and fluoroscopic guidance into the esophagus and the fistula was cannulated under direct vision using endoscopic guidance. The fistula was demonstrated and embolized using 0.5 ml 50% nBCA. Second attempt: After cannulation of the fistula as above, a 2 mm×2 cm micro-Nester coil was deployed within the fistula followed by injection of nBCA opacified with tantalum powder and a drop of Ethiodol into the residual channel.
Results: The first embolization with glue alone failed with recanalization at 2 months. Repeat procedure was performed with coil and glue. At 8 months follow up after combined coil and glue approach, the child is doing well with no further episodes of choking or coughing at feeds and complete occlusion on esophagogram. He is on full oral diet and the gastrostomy has been removed.
Conclusion: Esophagoscopy and fluoroscopy guided combined coil and glue embolization technique is a safe and effective treatment option in the management of difficult EBF in infants and children and may avoid major thoracotomy for the same.
USE OF LAPAROSCOPIC APPROACH FOR REMOVAL OF LARGE GASTRIC TRICHOBEZOAR IN CHILDREN
Purpose: To report our technique of laparoscopic removal of large Trichobezoar in children.
Materials and Methods: 9 year old child presented with vomiting and intolerance to oral diet. Upper GI contrast revealed the presence of a large Trichobezoar in the stomach. The Gastroenterologist took the child to the procedure room for gastroscopic removal of the trichobezoar. After several attempts they were only able to remove a bit of it and unfortunately their grasper got stuck into the bezoar. The surgeons were consulted and the patient was then moved in to the OR with the gastroscope and the grasper insitu.
Technique: A 5 mm step trocar was placed as an umbilical port and 5 mm 30 Deg telescope was introduced. A small 2 cm incision was made on the anterior abdominal wall and with a grasper the stomach was pulled up to the anterior abdominal wall. 2 Gastropexy sutures were then to bring the stomach to the anterior abdominal wall. A small gastrostomy was then made and the trichobezoar was then removed piecemeal. The endoscopy grasper was released from the hair ball during the procedure and the gastroscope was removed. Once the trichobezoar was completely removed the gastrostomy was closed with absorbable sutures and the stomach was returned back to the peritoneal cavity. All the ports sites were sutured closed.
Results: The child did well after surgery and was discharged. There were no intraoperative or post- operative complications. At 1 year follow up the child was doing well and the scars were well healed.
Conclusion: Laparoscopic removal of large gastric trichobezoar is safe and effective in children. It should be tried in all children before subjecting them to large laparotomy incisions.
LAPAROSCOPIC REPAIR OF CONGENITAL ABDOMINAL WALL HERNIA IN AN INFANT
Background: Congenital abdominal wall hernias are rare in children.
Purpose: To report our technique of Laparoscopic repair of a rare abdominal wall hernia in an infant.
Materials and Methods: A new born was seen in the clinic with a bulge on the right side of his abdominal wall. On examination there was a muscular defect on the right side of the abdominal wall. This was made more obvious by the child crying. Since this type of abdominal wall hernia is almost unknown in the newborn period the child was given a period of observation and follow up was scheduled in 6 months. At 6 months follow up the defect was more pronounced. He was then taken to the OR for laparoscopic repair of the defect.
Technique: Incision was made in the scar of the umbilicus and a 5 mm step Trocar is introduced. Pneumoperitoneum was achieved and a 5 mm 30 degree scope is introduced. The site of the congenital hernia on the right side of the abdomen was identified. We then made a 2 mm stab incision on the left side of the umbilicus and with a hook diathermy and the peritoneum on the defect was incised and the muscular defect was defined. We then introduced the Granee needle from the skin over the defect and 3’0’ vicryl sutures were placed through the abdominal wall and the defect was repaired. 4–5 sutures were used to close the defect. Once the defect was repaired we closed the peritoneum over the repair. This completed the repair. The repair was accomplished with almost no scars and excellent cosmesis.
Results: The child recovered well for the surgery. There were no intra-op or post op complications. At 1 year follow up the child was doing well with well healed scar that was almost invisible and with no evidence of the abdominal wall hernia.
Conclusion: Abdominal wall hernia in the newborn and infant is very rare with no reports in literature. Laparoscopic repair of the abdominal wall hernia is a safe and effective treatment in infants and should be attempted to reduce large incision related trauma and get excellent cosmetic results.
HOMESIMULATOR - BUILDING AND PRACTICING IN YOUR OWN HOME-MADE ENDOSCOPIC SIMULATOR
Objective: Gaining skills in laparoscopic surgery requires a lot of training. Besides in vivo training, surgeons have to spend a great amount of time practicing in simulators. Various box simulators have been presented, but most of them are expensive or difficult to construct. In 2011, our group presented 5-steps to building a homemade endoscopic simulator (HOMESimulator). Since then, we started organizing workshops for surgeons where they build and practice their own HOMESimulator.
Methods: We designed a workshop where 8–12 participants were to build their own HOMESimulator using easy-to-find cheap materials (a transparent plastic box, a webcam, a USB cable, adhesive tape, Velcro tape, and a rubber sheet) after a short explanation of the assembling steps. Then, the participants used their own HOMESimulator to perform simple endoscopic tasks in dry laboratory. After that, they completed an anonymous query about the difficulty of constructing the simulator, the ability to build their own simulator, the total cost of the simulator, the need of having one, the advantages and disadvantages of the simulator comparing to other commercial simulators they had tried using a scale from too difficult to too easy.
Results: In 2011 and 2012, we held 3 workshops with a total of 30 participants (mostly residents in surgery). Every participant was able to build the HOMESimulator with either minor or no help from the organizing team. 23 replied to the query. 96% found the simulator easy or really easy to build. Comparing to other commercial available box simulators, the majority of participants found the homemade simulator easier to mount and dismount, easier to transport, easier to clean. Quality of light and image was largely dependent of each participant personal computer and the light in the room, that we tried to overcome using better webcams with LED light.
Conclusions: We think the HOMESimulator is a good instrument to widespread basic training in laparoscopy, because it is cheap and easy to build. Any group of surgeons can organize a small workshop like ours to their residents, Although we did not provide our participants ex-vivo tissue for training, it can be an option for dissection tasks. Moreover, when available training with a conventional optic/camera can also overcome image and light problems as well as creating a more realistic endoscopic surgery environment.
MANAGEMENT OF RECURRENT TE FISTULA IN A 11 YEARS OLD CHILD BY ARGON PLASMA COAGULATION AND BIOGLUE
ABSTRACT WITHDRAWN
SINGLE PORT LAPAROSCOPIC ASSISTED CHOLANGIOGRAM FOR SUSPECTED BILIARY ATRESIA
ABSTRACT WITHDRAWN
ENDOSCOPIC REPAIR OF DIAPHRAGMATIC HERNIA USING A PATCH FIXED WITH TITANUM SPIRAL TACKS
Introduction: Laparoscopic and thoracoscopic diaphragmatic hernia repair are increasingly performed in children. Different approaches and techniques have been proposed, but there is not enough evidence in the literature to recommend particular technique.
Materials and Methods: In this paper, we report one case of recurrent Morgagni hernia and one case of Bochdalek hernia, 9 years and 2 days old, respectively, operated on endoscopically in our Department. In the first case, laparoscopy was done. The omentum was trapped in the hernia. The edges of the defect were widely cleared of peritoneum and fat to expose the muscle and fascia of the diaphragm. Intracorporeal nonabsorbable stitches were placed and additionally goretex mesh (GORE® DUALMESH®) was used and was secured in place using 5 mm titanium tacks (Protack, Covidien) In the second one, the defect was large and was not suitable for primary closure. The herniated content (spleen, small and large intestine) was reduced into the abdomen. Tutopatch® was used and was secured in place using titanium tacks.
Results: The intraoperative course was uneventfull. Both patients recovered well and were discharged home on 6 and 19 postoperative day, respectively. No recurrence was evident after 1 and 3 months, respectively.
Conclusions: Patch fixation with titanum spiral tacks seems to be faster and easier than more commonly performed laparoscopic/thoracoscopic suturing. Further reports are needed to confirm the durability of this technique and its potential long term effects.
THE NEW CONCEPT AND MINIMALLY INVASIVE TECHNIQUE OF LAPAROSCOPIC INTRA-GASTRIC SURGERY FOR PEDIATRIC RARE DISEASE USING AUGMENTED REALITY NAVIGATION AND SINGLE INCISION APPROACH
Background and Aims: Laparoscopic intra-gastric surgery was demonstrated to remove the lesion of posterior wall of stomach. We performed this procedure for the pediatric rare disease to ensure the minimally invasiveness and good cosmetic appearance.
14 year old girl admitted due to abdominal distention. CT scan and gastroscopy revealed that intra-gastric mass was two trichobezoars, 20 cm and 5 cm respectively. Trying Crash and extirpation via gasrtoscope was unsuccessful and small size trichobezoar moved into the small intestine. So we planned to perform the single incision intra-gastric surgery. Initially the umbilicus was opened and gastric wall was directly incised and X-gate (Ethicon endosurgery Cincinnati USA) was attached to fix the abdominal wall and gastric wall. Three trocars were inserted via X-gate (Figure 1a). Pneumostomach was established by insufflations of CO2. Huge trichobezoar was crashed by endoscopic forceps (Figure 1b) and extirpated via X-gate completely (Figure 1c). Trichobezoar inside the small intestine was extirpated by umbilicus wound. The volume was 576 g weight. Incised gastric wall and small intestinal wall was directly closed and drain was placed (Figure 1d). The patient had good clinical course after operation.
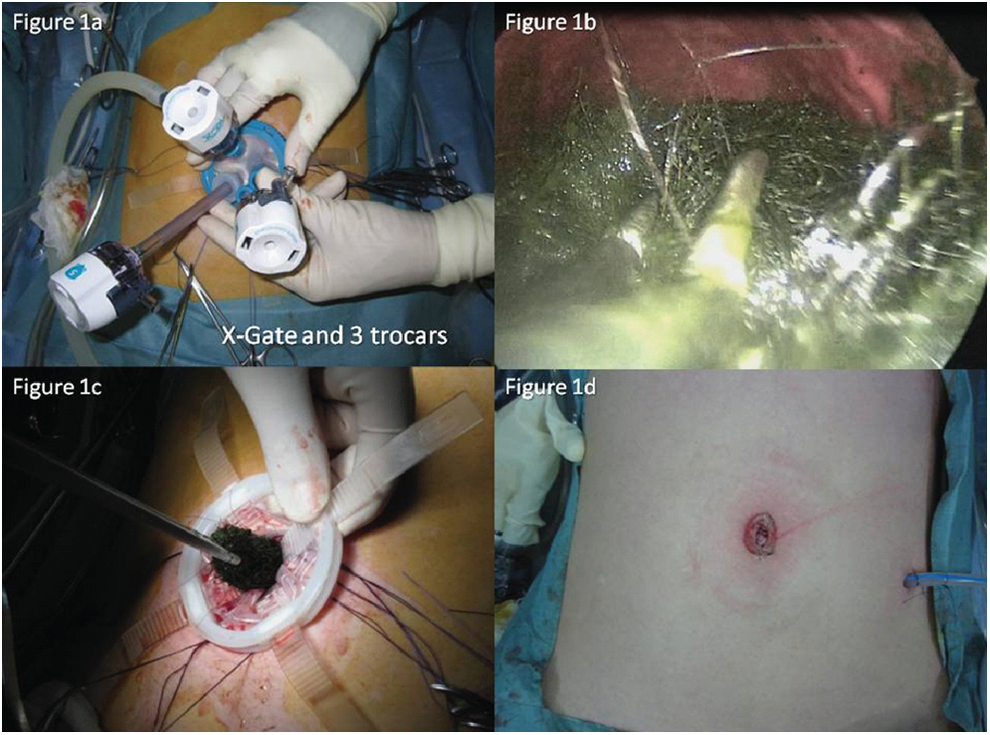
12 year old boy was admitted by hematemesis. Gastrointestinal fiberscope revealed the 4 cm size submucosal tumor located at posterior wall. Located position was near the E-C junction. The tumor was cystic type and seemed to be benign lesion. So we planned to perform the intra-gastric surgery under augmented reality navigation system to prevent the around organ injury. We started using the “Funada-kit II” (CREATE MEDIC CO., Kanagawa, Japan) device with two parallel needles to puncture the stomach and assist suturing the anterior gastric wall to the anterior abdominal wall. In this procedure, all three trocars are placed in the gastric lumen, penetrating both the abdominal and stomach walls in order to perform a laparoscopic removal of gastric lesions under the observation of GI fiberscope. The operation is then carried out in the gastric lumen with currently available laparoscopic instruments and laparoscopic monitoring. Laparoscopic intra-gastric surgery requires a pneumostomach, which is created by CO2 insufflations via GI fiberscope. Volume images were reconstructed by three-dimensional (3D) viewer application. We used an optical tracking system for registration between volume image and body surface markers. The AR visualization was superimposed preoperative 3D CT images onto captured laparoscopic live images. The operator recognized the hidden vascular variation of the splenic artery and vein, spleen (Figure 2a), and pancreas (Figure 2b) by overlaying an image onto a laparoscopic live image. The tumor was resected by ultrasonically activated device (Figure 2c). EC junction was kept without injury. Defect of gastric wall was closed under laparoscopic view (Figure 2d). Pathological diagnosis revealed that the tumor was bronchogenic cyst. The patient had good clinical course after operation (Figure 2e).

Conclusion: Laparoscopic intra-gastric surgery is feasibility, safety, and effective for the pediatric patients.
LAPAROSCOPIC APPENDECTOMY IN CHILDREN: EXPERIENCE IN A SINGLE CENTRE IN CHITTAGONG, BANGLADESH
ABSTRACT WITHDRAWN
LAPAROSCOPIC RESECTION OF GIANT HEPATIC CYSTADENOMA
This is the case of a 22-month-old female infant. The pathology started two weeks before with a gradual increase of abdominal circumference and intermittent hypo-colic stools. A CT-scan of the abdomen showed a large cystic tumor with interior partitions, measuring 16.5 by 10.6 by 12.1 cm in diameter, originating in segments V and VI of the liver, displacing the remaining liver to the left and compressing the right kidney, bowel, celiac artery, gallbladder, and pancreas. A laparoscopic approach for tumor resection was decided on due to the scarce tumor vascularization and entirely cystic consistency. The procedure required 4 ports, three of 5 mm and one of 3 mm, emptying the cystic content of approximately 2 liters of citrine fluid. Dissection was performed using the Ligasure™ vessel-sealing device and monopolar cautery, preserving adjacent vital structures and preventing bleeding. The surgical specimen was removed through the umbilical scar. No transfusion was required and surgery lasted four hours. There were no postoperative complications. As a result, laparoscopic surgery is considered a safe procedure for the excision of large tumors in children provided they are cystic and benign, as emptying the cyst gives broader visualization of the area and permits better tissue handling.
LAPAROSCOPIC-ASSISTED SURGERY FOR ABDOMINAL CYSTIC MASS OF NEONATE
Background: The present study aimed to compare the effect of open surgery and laparoscopic-assisted surgery in neonatal abdominal cystic mass.
Methods: This is a retrospective review of 62 patients with abdominal cystic mass in the department of Neonatal Surgery, Nanjing Children's Hospital affiliated to Nanjing Medical University. These patients were divided into two groups, including open surgery group and laparoscopic-assisted surgery group. Differences in operative time, blood loss, postoperative fasting time, postoperative hospital stay, cost of hospitalization, and postoperative complications was reviewed.
Results: The 29 patients (12 males and 17 females aged 5–28 days, an average of 17.8 days, weight 3.6±0.7 kg) in open surgery group were hospitalized between March 1, 2009 and September 30, 2010, including ovarian cyst in 11 cases, mesenteric cyst in 8 cases, omental cyst in 3 cases, intestinal duplication in 7 cases. The 33 patients (13 males and 20 females aged 4–28 days, an average of 15.9 days, weight 3.5±0.6 kg) in o laparoscopic-assisted surgery group were hospitalized between October 1, 2010 – March 31, 2012, including ovarian cyst in 14 cases, mesenteric cyst in 9 cases, omental cyst in 2 cases, intestinal duplication in 8 cases. There were no differences in age, weight, disease distribution in these two groups. The surgical time, blood loss, postoperative fasting time, postoperative hospital stay, and cost of hospitalization of open surgery group and laparoscopic-assisted surgery group were 56±12.3 minutes vs. 52±15.7 points, 18±5.4 ml vs. 16±13.1 ml, 3±0.7 days vs. 2±0.5 days, 6±0.4 days vs. 4±0.6 days, 8900±683 of vs. 7760±895 yuan. The postoperative fasting time, the postoperative hospital stay, and the cost of hospitalization in laparoscopic-assisted surgery were significantly lower than the open surgery group. No patient was dead in these two groups. No conversion to open surgery in laparoscopic-assisted surgery group. The postoperative complications of open surgery group including wound infection in 2 cases, adhesions in 2 cases, but no postoperative complications in laparoscopic-assisted surgery group. Moreover, good appearance incision was observed in laparoscopic-assisted surgery group.
Conclusion: It is feasible and safe for treatment of neonatal period abdominal cystic mass by use of laparoscopic-assisted surgery.
LAPAROSCOPIC PARTIAL PANCREATECTOMY FOR THE TREATMENT OF PERSISTENT HYPERINSULINEMIC HYPOGLYCEMIA OF INFANCY
Objective: The authors describe the use of laparoscopic partial pancreatectomy for persistent hyperinsulinemic hypoglycemia of infancy (PHHI) and report the outcomes in this article.
Methods: Between September 2008 and April 2011, the laparoscopic partial pancreatectomy was performed in four children with PHHI, three with diffuse nesidioblastosis underwent 90% pancreatectomy and one with focal nesidioblastosis underwent focal resection. All patients were followed-up. The levels of blood sugar and insulin were recorded postoperatively.
Results: The time required for surgery was 170 to 190 min, and blood loss was minimal without necessity for blood transfusion. The average hospital stay period after the operation was 12 to 24 days. The duration of postoperative abdominal drainage was 2 to 7 days. The level of fasting blood glucose after surgery was higher than that before surgery (7.5 mmol/L vs. 2.8 mmol/L). The level of fasting insulin after surgery was lower than that before surgery (7.21 uU/ml vs. 77.39 uU/ml). The duration of following-up was 2 to 32 months. During following-up, the levels of blood glucose and insulin were normal in three patients undergoing 90% pancreatectomy. The patient treated by focal resection underwent reoperation due to recurrence of hypoglycemia. There was no the recurrence of hypoglycemia after reoperation in this patient.
Conclusions: Laparoscopic partial pancreatectomy for children with PHHI is safe and effective.
LAPAROSCOPIC RESECTION OF PANCREATIC TUMOR FOR SOLID PSEUDOPAPILLARY TUMOR IN CHILDREN
Purpose: To investigate the safety and feasibility of laparoscopic resection of pancreatic tumor for solid pseudopapillary tumor (SPT) in children.
Methods: Three children (one boy and two girls, age: 10–16 years) with SPT underwent laparoscopic resection of pancreatic tumor between Aug 2010 and Oct 2010. The location of the tumor was the body of pancreas in one patient, and the body and tail in two patients. The diameter of tumors was 5.5 cm, 4.5 cm and 11 cm separately. All of children were followed-up postoperatively.
Results: The time required for surgery was 190 to 215 min, blood loss was 10–50 ml, and there was no necessity for blood transfusion. The duration of postoperative abdominal drainage was 3–4 days. The hospital stay period after the operation was 3 to 7 days. The time of beginning taking food was 1–3 days postoperatively. The pathology was SPT in three children. All the patients had been followed up and no tumor recurrence.
Conclusions: Laparoscopic resection of pancreatic tumor for children with SPT is safe and effective.
INDWELLING ESOPHAGEAL BALLOON CATHETER FOR BENIGN ESOPHAGEAL STENOSIS IN INFANTS AND CHILDREN
Objectives: Balloon dilatation of benign esophageal strictures is an established mode of therapy in adults and children. There remains a group of patients with refractory stenosis despite dilatation at regular intervals. Intra-esophageal stents to warrant esophageal patency frequently dislodge or obstruct. An indwelling balloon catheter may offer a better alternative and has been used in our institution since 2004. This retrospective study aims to investigate its results.
Methods: Between 2004 and 2011, esophagoscopy with placement of an indwelling balloon catheter was carried out in 11 children with refractory esophageal stenosis. Total number of endoscopies, number of endoscopies with indwelling balloon catheter as well as complications, reoperations and mortality due to use of the balloon catheter were studied.
Results: Patient age ranged from 10 weeks to 15 years. The indwelling balloon catheter was used to treat refractory stenosis after corrective surgery of long gap esophageal atresia (n=2) and esophageal atresia with fistula (n=2). It was also applied in cases of refractory esophageal stenosis due to caustic esophageal burns (n=4), reflux (n=1) and stenosis of unknown cause (n=2). Patients underwent an average total number of endoscopies of 12. Mean duration of balloon treatment was 12, 5 weeks and the median time was 7 weeks. With the indwelling balloon catheter in place, the mean number of endoscopies equalled 4. Complications associated with use of the balloon catheter were restenosis for which a new indwelling balloon catheter was necessary (n=3), two other patients needed 2–5 additional dilations; balloon leakage requiring replacement (n=7 in five patients), sputum retention (n=1) and dislodgement (n=4 in three patients). There was no mortality associated with the use of an indwelling balloon catheter, nor the need for any patient to undergo a rethoracotomy/-scopy.
Conclusion: The indwelling balloon catheter is safe to use and can be used by parents at home. It does not dislodge frequently, is well tolerated, reduces the frequency and number of endoscopies during treatment and obviates the need rethoracotomy/-scopy or esophageal replacement.
TECHNICAL ASPECTS OF NEONATAL LAPAROSCOPIC NEAR TOTAL PANCREATECTOMY FOR PERSISTENT HYPERINSULINEMIC HYPOGLYCAEMIA IN INFANCY (PHHI)
Introduction: A term baby boy was referred to our institution at Day 2 of life for problem of persistent hypoglycaemia since birth. The patient was immediately stabilized at our neonatal intensive care. Within the first week of life he underwent rigorous medical treatment i.e. continuous nasogastric alimentation, glucose infusion, oral diazoxide and subcutaneous octreotide. Genetic study revealed he had presence of homozygous frame shift mutation, A736ffs in exon 16 of ABCC8 gene. Early surgical referral was made at Day 8 of life. Radiological investigation was only confined to ultrasound of the pancreas in which no focal lesion was seen. PET scan was not available at our institution. The genetic result assisted the decision for surgery. The patient was then started on intravenous glucagon on days leading to surgery. It was important to note that the patient had a 2 year old brother who was a known case of diffuse type PHHI and had to undergo open near total pancreatectomy at 4 months of age.
Operative Technique: Laparoscopic near total pancreatectomy was performed at Day 14 of life. The patient was positioned supine under general anaesthesia. The camera port –a 6 mm Hasson was introduced via a supraumbilical wound. Intra-abdominal pressure started at 8 mmHg and increased to 10 mmHg, CO2 insufflation started at gas flow rate of 0.2 l/min to 3l/min., the right working port was 4 mm and the left working instruments were introduced directly i.e. port-free. Two hitch stitches were introduced, the first was to hitch the falciform ligament hence exposing the duodenum and stomach; the second hitch stitch was to elevate the decompressed stomach. Serial traction sutures were put on the pancreas and gradual dissection of the pancreas off the splenic vessels was performed using monopolar hook diathermy from tail to head of pancreas. Ultrasonic scalpel was used to performed pancreatectomy in stages. As the dissection became closer to the head of pancreas, the telescope was introduced intermittently through the right working port to assist visualization of the portal vein and superior mesenteric vessels. Only estimated 5% of pancreatic tissues were left behind. The surgery was successfully completed in 120 minutes. There was no blood loss. Intraoperative blood glucose level became high as resection was getting closer to the head of pancreas, as such the intra-operative glucagon infusion was stopped.
Postoperative Period: The patient was extubated at post-operative day 1 and started on feeding at post-operative day 2. Close monitoring of blood sugar level revealed a couple of hypoglycaemic episodes at post-operative day 8. Subcutaneous octreotide was restarted initially with frequency of thrice a day. Patient was discharged at post-operative day 14. He returned to his home state and remained well.
Follow-up: Histology examination of the pancreas confirmed that it was a diffuse pathology. The patient is currently 1 year old and his development is consistent with his age, he has had no documented episodes of hypoglycaemia. He is still on subcutaneous octreotide but the requirement is reduced to daily dose.
PLACE OF LAPAROSCOPY IN THE MANAGEMENT OF THORACOABDOMINAL FOREGUT DUPLICATION
ABSTRACT WITHDRAWN
INITIAL EXPERIENCES OF LAPAROSCOPIC EXCISION OF CHOLEDOCHAL CYST IN SMALL INFANTS
ABSTRACT WITHDRAWN
LAPAROSCOPIC MANAGEMENT OF INTESTINAL MALROTATION WITH OR WITHOUT VOLVULUS IN NEONATE
Background: Intestinal malrotation in neonates may require urgent surgical treatment, especially midgut volvulus are suspected. There have been a number of small series and case reports describing the use of laparoscopy to diagnose and correct malrotation. We describe a retrospective analysis the clinical outcomes of 44 neonates who underwent laparoscopic management of intestinal malrotation with or without volvulus in our hospital.
Methods: The 44 patients in this series, ages from 1 day to 22 days, underwent a confirmed laparoscopy for suspected intestinal malrotation. For all the patients, malrotation with or without volvulus was diagnosed and all of the patients underwent laparoscopic derotation and Ladd's procedure.
Results: 41 cases (93.18%) underwent laparoscopic management of intestinal malrotation with or without volvulus successfully, and 3 patients (7.82%) required conversion to an open procedure. Hospital stay ranged from 4 to 20 days (average, 7.28 days). 4 patients underwent open redo surgery because of postoperative clinical relapse due to late-occurred punch (4.88%, n=2) and recurrence of malrotation, volvulus, or both occurred (4.88%, n=2).
Conclusion: Diagnostic laparoscopy is the procedure of choice when intestinal malrotation is suspected. The majority of patients can be treated adequately with laparoscopic surgery in the cases. Nevertheless, a low threshold for conversion to an open procedure is mandated where occuring recurrence of malrotation or volvulus and late-occurred punch.
A NOVEL LAPAROSCOPIC GASTROSTOMY TECHNIQUE: DEVELOPING NEW OUTCOME STANDARDS
Objective/Aim: Laparoscopic gastrostomy (LG) avoids visceral injury associated with percutaneous endoscopic gastrostomy (PEG). Current laparoscopic techniques are still associated with significant minor complications. We compare our gastrostomy-related complications and outcomes with published reports on LG and PEG.
Materials and Methods: We reviewed our modified LG between 07/2009-06/2011. The group was subdivided into patients with LG alone and LG with fundoplication (LGF). Complications were defined as major when patient was taken back to operating theatre. Minor complications were wound infection, leakage, excoriation and granulation.
Laparoscopic Technique: 5 mm optical port (umbilical) and one 5 mm instrument left lumbar. Three stab incisions around the marked gastrostomy site at 12, 5 and 7 o'clock. Trans-abdominal stomach-holding sutures are inserted through these stab incisions to attach the anterior stomach wall to the abdomen. The needle is withdrawn through same incision and sutures are buried in the subcutaneous tissue. Seldinger technique is used to puncture the stomach in the middle of these sutures and a balloon gastrostomy tube inserted with a peel away sheath.
Results: 83 children (LG:n=60; LGF:n=23). Median age: LG: 3.7 (range 0.3–16.8), LGF: 1.8 (range 0.3–15.1) years. Our overall minor complication rate was 13% (11/83). Minor complications in LG alone 7% (leakage (2/60), granulation (2/60)) were significantly (p,0,01) lower than in LGF 20% (leakage (2/23), granulation (2/23) and wound infection (1/23)). Incidence of gastrostomy-related major complications (balloon migration through pylorus) was 9% (2/23) for LGF and 0% (0/60) for LG (p<0.01). No visceral injury in both groups, no gastrostomy-related mortality.
Conclusions: Recent literature indicates high minor complication rate with PEG (14–28%), LGF (38%) and LG (26%-42%). The experience with our LG technique has shown encouraging results and establishes a new benchmark standard (11%) for minor complications compared to the published literature. Patient with a combined LG and fundoplication procedure remain challenging having a higher minor complication rate.
LAPAROSCOPIC HEPATOENTEROSTOMY FOR 8 CHILDREN WITH FUSIFORM CHOLEDOCHAL CYST
Background: Laparoscopy has recently become very popular in pediatric surgery. There has been several report on its application in the treatment of choledochal cysts (CDC). Herein we want to discribe laparoscopic radical resection, biliary reconstruction experience for the fusiform choledochal cyst.
Methods: We reviewed 8 patients who underwent laparoscopic hepatojejunostomy between March 2012 to October 2012. Their ages ranged from 3 years to 6 years (average, 4.2 years). The average diameter of the cyst is 1.5 cm. Four trocars were used with 5 mm instrumentation. After the commen bile duct was opened, the 3 mm suction head was inserted into the CBD and flushed with saline until all the protein plug was removed. All the cases underwent distal cyst ligation. Among of which 5 cases routine gallbladder, cyst removal, commen hepatic duct jejunum Roux-Y anastomosis were performed, three cases of intraoperative findings the gallbladder neck position close to the hepatic portal, so gallbladder neck ligation were performed and common bile duct jejunum Roux-Y anastomosis were performed. No blood transfusion was required.
Results: The group of eight patients surgery was successful in all cases, the mean operative time was 3.8 hours (2.8–5.0 hours); blood loss was about 10 to 25 ml; length of hospital stay of 7–10 days. We followed up for four weeks to 8 months, no bile leakage and no anastomotic stenosis was occured, also without intestinal obstruction.
Conclusion: Proper location anastomosis for fusiform type of congenital choledochal cyst can reduce the difficulty of operation, improve the success rate of the surgery.
SINGLE-INCISION LAPAROSCOPIC HEPATOENTEROSTOMY FOR A CHILD WITH FUSIFORM CHOLEDOCHAL CYST
Background: Laparoscopy hepaticojejunostomy for Choledochal cysts in children has recently become popular in pediatric surgery. But rare center can perform single-incision laparoscopic hepaticojejunostomy for CDC. Herein we want to discribe a single-incision laparoscopic hepaticojejunostomy experience for a fusiform choledochal cyst.
Case Reports: A 12-month-old girl was admitted to our hospital in October 2012. Ultrasound and MRCP showed fusiform Choledochal cysts which the diameter is 1.4 cm Operation procedure: Single-port with multitrocar requires 2.5-cm umbilical comma incision which enables the optic lens to be separated. The procedure of Roux-en-Y hepatoenterostomy was divided into two stages. The first stage is jejunojejunal anastomosis which is performed extracorporeally. After the incision was made, the small bowel was pull out and the first anastomosis which is 20 cm from Triz ligament was performed. The bile limb is about 20 cm. Then the bowel was send back to the abodomal cavity. The second step was resect the gallbladder and cyst. Then an end to side anastomosis of hepaticojejunostomy was performed. The three ports should be placed with adequate triangulation of the straight instruments which spaced farthest away within the limits of the skin incision so as to perform surgical procedures more easier. We use two stiches for traction which one stich is in the gallbladder and the other stich is in falciform ligament of liver. So that the cyst can be exposed better. After the commen bile duct was opened, the 3 mm suction head was inserted into the CBD and flushed with saline until all the protein plug was removed. Then the distal commen bile duct was ligated and cutted. commen hepatic duct jejunum Roux-Y anastomosis were performed with 5-0 PDS-2 silk. No blood transfusion was required.
Results: The operative time was 5 hours; blood loss was about 10 ml. The atient was discharged after 7 days of surgery. No bile leakage occurred. Also no other complications occurred.
Conclusion: Single-incision laparoscopic hepaticojejunostomy for CDC is feasible. Skilled separe and suture technology is needed.
GALL BLADDER PERFORATION AND PERITONITIS: SUCCESSFUL TREATMENT WITH ULTRASOUND GUIDED TRANS-HEPATIC CHOLECYSTOSTOMY
ABSTRACT WITHDRAWN
LAPAROSCOPIC MANAGEMENT OF CHOLEDOCHAL CYST IS A SAFE TREATMENT
Introduction: Total excision of choledochal cyst is an acceptable treatment. Laparoscopic excision of choledochal cyst with Roux-en-y hepaticodocho-jejunostomy is being offered as an alternative to open operation for choledochal cyst in children. Here we introduce our initial experience of laparoscopic management of choledochal cyst in 11 cases and assess the safty.
Methods: We reviewed 11 patients who had undergone laparoscopic excision of choledochal cyst. The data was analysed for operative time, type of choledochal cyst, intraoperative problems, postoperative complications and postoperative follow up.
Results: From January 2009 to July 2012, 11 patients have undergone laparoscopic surgery for choledochal cyst. Mean age was 5 years (1.5 years – 12 years), all patients had type I (8 spheroida dilatation and 3 spindle dilatation of common bile duct). The cyst diameter was 3 to 10 cm. Mean operative time was 260 minutes (210 – 410 minutes). Mean intraoperative blood loss was 25 ml (10 – 50 ml). All patients underwent Roux-en-y hepaticodocho-jejunostomy. No patients were converted to open surgery. No post-operative complications occurred. Mean hospitalisation was 6.5 days (5 – 9 days). Follow-up from 3 months to 3 years, only one patient had cholangitis.
Conclusion: Laparoscopic excision of choledochal cyst is a safe alternative to open surgery. Postoperative recovery of the children is quickly even more operating time than open surgery. It is an acceptable treatment for child with choledochal cyst.
COMPARISON OF LAPAROSCOPIC SURGERY AND LAPAROTOMY FOR TREATMENT OF GREATER OMENTAL CYST IN CHILDREN
Objective: The aim of this study is to investigate the feasibility and effectiveness of laparoscopic surgery in management of greater omental cyst in children.
Methods: The clinical data of 12 children with greater omental cyst underwent surgery at our center from November 2003 and February 2012 were reviewed. 6 patients were performed laparoscopic surgery (LS group), and the other 6 patients underwent laparotomy (LP group). Perioperative outcomes and long-time follow-up were compared between LS group and LP group.
Results: The pathologies of 12 patients were greater omental cystic lymphangioma. Greater omental cyst have various forms of presentation: as an abdominal distention in 8 cases (66.7%); as a poor appetite in 8 cases (66.7%); as an abdominal pain in 5 cases (41.7%); as nausea and vomiting in 4 cases (33.3%); as an abdominal mass in 3 cases (25%). And the ratio of female to male was 2 (female/male: 8/4). All cysts are single cyst. The mean of cystic size is (1283.37±701.85) cm3. Septations were seen in 10 cysts (83.3%). Only 2 cysts (16.7%) without Septations. No difference of patient's gender, operative age, weight, clinical presentation, cystic cases, cystic size and operative time was found between LS group and LP group (P>0.05). ALL patients of LS group were completed laparoscopically without conversions. There was significant difference on time to start enteral feeding (1.00 d±0.00 d vs 2.17 d±0.75 d) and postoperative hospital stay time (3.33 d±0.52 d vs 7.00 d±0.00 d) between LS group and LP group (P<0.05). Two groups of children remained in good health, with no postoperative bleeding, infection, intestinal obstruction, intestinal fistula and other short-term complications. In the follow-up time (LS group: 5m-4y10m; LP group: 5y9m-8y8m), there was no recurrence, intestinal obstruction and other long-term complications in all the children.
Conclusions: Laparoscopic management is safe, feasible, and effective, and should be the treatment of choice for most cases of greater omental cyst in children.
TRANSUMBILICAL SINGLE INCISION LAPAROSCOPIC CYSTECTOMY FOR CHILDREN WITH MESENTERIC CYST
Objective: To study the safety and efficacy of transumbilical single incision laparoscopic cystectomy for children with mesenteric cyst.
Methods: Between September 2006 and September 2012, Single umbilical incision laparoscopic cystectomy was performed on 12 children with mesenteric cyst. The prognosis was followed-up and retrospectively analyzed in this study.
Results: All procedures were performed successfully without conversion to open surgery and no complication was noted. the operating time ranged from 30 – 90 min, the patients were followed up for 4 to 48 months, no cyst recurrence was observed.
Conclusions: Transumbilical single incision laparoscopic cystectomy is safe and feasible for the treatment of mesenteric cyst in children.
INFANTILE BILIARY HYPOPLASIA: THE DIAGNOSIS COMES FROM LAPAROSCOPIC CHOLANGIOGRAPHY AND LIVER BIOPSY, AND ITS CLINICAL OUTCOME
ABSTRACT WITHDRAWN
LAPAROSCOPIC HELLER CARDIOMYOTOMY IN CHILDREN: AN EFFECTIVE PROCEDURE FOR THE TREATMENT OF ESOPHAGEAL ACHALASIA
Background: The purpose of this study is to evaluate the efficacy of laparoscopic Heller's myotomy for the long-term clinical treatment of achalasia in children, analyzing the experience of 2 Italian centers.
Materials and Methods: Between 1998 and 2012, 24 children (10 girls and 14 boys, with a median age of 9 years) affected by esophageal achalasia were treated in two different institutions with an esophagomyotomy according to Heller's procedure via laparoscopy associated with an antireflux Dor procedure. In the last 5 years we adopted new hemostatic devices to perform the myotomy.
Results: Surgery lasted in median 100 minutes (85 – 155). Median hospital stay was 4 days. With a maximum follow-up of 14 years, we recorded 2 mucosal perforation and in only 1 case we perform a redo surgery to close the tear. All the patients followed a semiliquid diet for 1 month after surgery. Occasional dysphagia was present in 8/24 patients. All the parents were extremely satisfied from the results of the procedure.
Conclusions: Laparoscopic Heller procedure associated with antireflux procedure, in our experience, remains the gold standard for the treatment of children with esophageal achalasia. New hemostatic devices seem very useful to fasten the surgery and reduce bleeding during the myotomy.
COMPARISON OF THERAPEUTIC EFFECT BETWEEN LAPAROSCOPIC AND OPEN PROCEDURE FOR PEPTIC ULCER PERFORATION OF CHILDREN
Objective: To compare the efficacy of laparoscopic repair for perforated peptic ulcer (d<10 mm) in children with that of open procedure.
Methods: A total clinical data of 42 children with perforated peptic ulcer undergoing surgical treatment from June 2000 to July 2011 were reviewed.
Results: All statistical parameters (bleeding, recovery time after operation, length of incision and postoperative hospital-lization period) in the laparoscopic operation group were better than the conventional operation group; There was no significant difference between two groups in the operating time and hole diameter.
Conclusion: Laparoscopic operation for perforated ulcer of children is safe and reliable and has minimal injury, cosmetic outcome, rapid recovery and shorter time in hospital. Laparoscopic operation is a better method to treat perforated ulcer than open procedure.
RISK FACTORS FOR PERFORATION AND SURGICAL SITE INFECTION FOR LAPAROSCOPIC APPENDECTOMY IN CHILDREN: A RETROSPECTIVE REVIEW
Objective: To investigate and confirm the risk factors associated with the incidence of perforation and surgical site infection for laparoscopic appendectomy.
Methods: The notes of patients who underwent a laparoscopic appendectomy at the 5th Central Hospital of TianJin, between June 2003 and February 2011 were retrospectively reviewed. The patients with perforation and surgical site infection were noted. Other variables recorded were age, sex, course of disease time before operation, white cell count, antibiotic usage, ancillary investigations (e.g. ultrasound) were abstracted. Logistic regression was performed to identify independent predictors.
Results: A total of 510 patients underwent laparoscopic appendectomy were reviewed. Logistic regression identified 3 independent predictors of perforation and surgical site infection: course of disease time before operation 2.5 days or longer [odds ratio (95% confidence interval) OR (95% CI), 1.71 (1.26–2.35); P=0.002], white blood cell count more than 15,000 [OR (95% CI), 1.56 (1.25–1.94); P<0.001], and female sex [OR (95% CI), 1.50 (1.32–2.15); P=0.03].
Conclusions: In this study, course of disease time before operation 2.5 days, blood cell count more than 15,000, and female were considered to be risk factor for perforation and surgical site infection for laparoscopic appendectomy.
ENDOVIDEOSURGERY FOR CHOLEDOCHAL CYST TREATMENT IN CHILDREN
The surgical treatment of congenital biliary disorders is one of the tough issues in pediatric surgery. Choledochal cysts are also of a current interest. Due to development endovideosurgery it became possible to perform difficult reconstructive surgeries on the biliary tract by the aid of laparoscopy. The main goal of our work was to compare the results of surgical treatment in two patient groups: “open surgery” and “endovideosurgery” patients.
Since 2008, 14 patients with choledochal cyst have been treated at National Research Center for Mother and Child Health. Eight of them had complaints on pain at epigastrium, three children – transitory jaundice, and six patients had no clinical symptoms. All the children passed CT and ultrasound investigation. We applied endovideosurgery in 5 children. Roux-en-Y hepaticojejunostomy were performed after laparoscopic choledochocystectomy had been completed. First two cases were a kind of open surgery with laparoscopic assistance. Roux-en-Y hepaticojejunostomy in these patients were performed through arciform incision at umbilicus.
In remained three cases all the stages of intervention have been completed by the aid of laparoscopic surgery. Affected choledoch was incised very close (0.5 cm) to the left and right hepatic ducts conjunction. While performing Roux-en-Y hepaticojejunostomy extracorporeal ties were used. The similar open surgery was perfomed in 9 patients of control group. At postoperative period we used standard antibacterial treatment (wide spectrum antibiotics), parenteral nutrition within three days, and painkillers. No complications during the intra- and postsurgery period were noticed.
For comparative assessment of body's postagressive response to laparoscopic and traditional types of operations we studied: the state of stressful hormones (cortisol, prolactin) and several biochemical blood parameters, reflecting the functional state of the suprarenal glands and liver, the balance of carbohydrate and protein metabolism. The analysis of the comparative evaluation of body's postagressive response to laparoscopic and traditional surgeries has showed that laparoscopic surgery is less invasive, less traumatic, less durable surgical intervention which is characterized to have more favorable postoperative period.
Taking into consideration our experience of laparoscopic surgery for choledochal cysts endovideosurgery could become a method of choice for correction of external biliary ducts disorders.
ENDOVIDEOSURGERY FOR THE TREATMENT OF HEPATIC AND BILIARY DISORDERS
One of the most significant achievements in modern pediatric surgery in the past decades is the widespread introduction of laparoscopic surgery into clinical practice. Pediatric hepatobiliary surgery is one of the most promising trends of endovideosurgery.
Since August 2007, 42 endovideosurgeries have been performed in children with patients with hepatic and biliary disorders at the Department of Pediatric Surgery of National Research Center for Mother and Child Health. Laparoscopic surgery for hydatyd disease of the liver.
We used laparoscopic surgery in the treatment of 18 patients with hydatyd disease of the liver. Solitary and multiple cysts were revealed in 15 and 3 patients respectively. In one case with multiple hydatyd we found one of the cyst located at posterior part of diaphragmatic surface of the liver while carrying out the diagnostic stage of intervention. In addition there were tight adhesions between cyst and diaphragm. So, that is why we had to perform traditional open surgery in this case. The remained patients have undergone laparoscopic surgery that consisted of the following steps: cyst puncture, liquid aspiration, disinfecting by Betadine and 33% ethanol, opening the cyst, removing chitinous cover by the aid of the vacuum extractor, abdominization of residual caverna by excision a part of a fibrous capsule and draining it. Omentopexy by greater omentum was performed in 6 patients. Long term ultrasound examination showed residual caverns in the liver which had been decreasing in size. Laparoscopic cholecystectomy.
The advantages of laparoscopic cholecystectomy are minimal surgical trauma, good visualization of anatomic structures, less pain syndrome, less number of postoperative inflammatory and adhesion complications, decreased length of stay, good cosmetic effect that is very important in pediatrics.
We performed 10 laparoscopic cholecystectomy in patients with cholelithiasis. Mean duration of surgery was about 45 minutes. There were no complications during intrasurgery and postsurgery period. The patient was able to move on the next day after surgery. Consequently, they required less of painkillers and length of stay were reduced.
Laparoscopy surgery for choledochal cyst and biliar atresia. We applied endovideosurgery in 5 children with choledochal cysts. Roux-en-Y hepaticojejunostomy were performed after laparoscopic choledochocystectomy had been completed. First two cases were a kind of open surgery with laparoscopic assistance. Roux-en-Y hepaticojejunostomy in these patients were performed through arciform incision at umbilicus.
In remained three cases all the stages of intervention have been completed by the aid of laparoscopic surgery. Affected choledoch was incised very close (0.5 cm) to the left and right hepatic ducts conjunction. While performing Roux-en-Y hepaticojejunostomy extracorporeal ties were used.
No complications during the intra- and postsurgery period were noticed. In 9 cases at patients with biliar atresia we had been executed a diagnostic biopsy of a liver with intraoperative cholangiography for specification of the diagnosis and definition of further tactics.
The analysis of the literature and ours for the present insignificant experience of use of a laparoscopy shows that laparoscopic access can become a choice method at surgical correction of a pathology of a liver and biliary ways at children.
ENDOVIDEOSURGERY FOR HIRSCHSPRUNG'S DISEASE TREATMENT IN CHILDREN
Hirschsprung's disease possesses the second place (after pylorostenosis) by frequency among the disorders leading to gastrointestinal obstruction in children that require surgical treatment. The main principle of Hirschsprung's disease treatment is a surgical excision of aganglionosis pathologically changed colon at the place of suprastenotic extension.
Introduction of a variety of mini invasive endovideo methods of treatment is a specific feature of modern surgery.
We would like to introduce our experience of Hirschsprung's disease treatment applying endovideosurgery.
There were 9 cases of Hirschsprung's disease treatment by the aid of laparoscopic assistance. The age of patients were between 3 and 14. The rectosigmoidal fom of Hirschsprung's disease were revealed in all the cases while X-ray examination.
After finishing the diagnostics and conducing presurgical treatment a laparoscopic bringing down the colon by K. Georgeson. Surgeries were performed under endotracheal narcosis and consisted of the following stages:
Stage I – laparoscopic. After insertion of three troacars the left side of abdomen were visually investigated. Further, transition fold of peritoneum was dissected and rectum was mobilized circularly deep in small pelvis. In order to assess the adequacy of mobilization and the degree of tension of the mesentery a trial traction of a mobilized colon toward the anus was conducted.
Stage II - perineal. Anal orifice was extended, tack-up sutures were performed around the anus. Dissection and mobilization of rectal mucous coat was performed for 5.0 – 6.0 cm starting 0.5 cm from linea serrata. Then, the colon was resected and brought down to perineum through demucousized channel. This step was conducted under laparoscopic visual control while the correct performance could be seen. The coloanal anastomosis was completed by separate absorbable sutures.
Stage III - laparoscopic revision and sanitation of the pelvis, restoring the transitional fold of peritoneum, elimination of the “window” in the colon mesentery were performed through the abdominal cavity.
No perioperative complications were noticed. Blood loss during surgery didn't exceed 10.0–15.0 ml and didn't require transfusion. In all cases the gastrointestinal contents appeared within 12–18 days after surgery, since that moment enteral feeding has been extended. These patients were under observation of outpatient department at late postoperative period and received anal bougienage by dilators of sizes according to the age. There were no symptoms of stenosis. One of the patients had high body temperature and difficulty of defecation at 7th day after surgery. A cavern of 3.0×4.0 cm with liquid content was revealed while rectal examination and ultrasound examination. In the result of puncture through the posterior wall of the rectum about 30.0 ml of rheumic content with fibrin was aspirated. The cavern was rinsed by insertion irrigating catheter under ultrasound scan control. After these manipulations the cavern have been closed up and infiltration nearby diminished. The patient was discharged in 15 days after the surgery. The other patients were discharged in 8–9 days after surgery. Control observation in 6 month showed good condition of all the patients. There were no complaints, abdominal distention, encopresis or obstipation.
MINIMALLY INVASIVE SURGERY FOR TREATMENT OF SECONDARY INTESTINAL INTUSSUSCEPTION IN CHILDREN WITH BLUE RUBBER BLEB NEVUS SYNDROME. EXPERIENCE ON TWO CASES
Introduction: Intestinal Intussusception (II) in infancy is idiopathic but sometimes could be secondary to lesions of bowel, such as polyps, diverticula, lynphonodes, in older children. The Blue Rubber Bleb Nevus Syndrome (BRBN) is a rare disease characterized by presence of multiple venous malformation on the skin and on the bowel. These malformation can cause several complication as II, bowel stenosis, perforation.
We describe minimally invasive approach for the treatment of II for BRBN.
Methods: MIS was performed using a 30° scope and 2 operative ports. An Hasson port was placed through umbilicus (10 mm), after exploration of abdominal cavity, several vascular malformation were identified on peritoneal wall and on intestinal loop. The ileo-caecal intussusceptions in the first case and ileo-ileal intussuscetion in the second one was seen and reduced by gentle opposite traction of two laparoscopic forceps that showed a vascular lesion responsible of intussusception. Multiple intestinal resections were performed exteriorizing loops through umbilicus, to remove the venous malformation and avoid the recurrence. The operative time was 45 min for the first case and 60 for the second.
Results: Two girls of different age (5 and 12 years old) with BRBN, presenting abdominal pain, vomiting and images of II on USS and bowel obstruction on x-ray abdomen, were successful treated by MIS for resolution of II and for multiple bowel resections without complications.
At 1 year follow-up, the patients were asymptomatic.
Conclusion: MIS is safe and effective for treatment of II in children even in more complicate cases as BRBN when an associate intestinal resection is required.
FUNDOPLICATION WITHOUT ESOPHAGEAL TENSION: AN ALTERNATIVE TO AVOID ITS MIGRATION
Introduction: Fundoplication migration is a frequent complication. In order to avoid it, there have been several proposals such as reinforcing the hiatus closure, fixing the fundoplication to the diaphragm, or a limited dissection of the stomach. These have not eradicated this complication. An alternative that would avoid the traction of the fundoplication to the thorax through the esophagus, bearing in mind it is an elastic muscular organ prone to tension, is to preserve a portion of the abdominal esophagus above the fundoplication without suturing it to the diaphragm.
Material and methods: Prospective descriptive study, patients with gastro esophageal reflux. Fundoplication was performed without esophageal tension through esophageal dissection until obtaining three centimeters of abdominal segment. Esophageal hiatus closed using non-absorbable suture. Fundoplication conducted placing the first suture in an esophagus-stomach-esophagus manner, two centimeters above the union, second suture esophagus-stomach-esophagus in the union, and a mid point suture located in a stomach-stomach position, in order to leave one centimeter of abdominal esophagus above the fundoplication. Contrasted study was conducted after one, six and 12 post surgical months, in order to evaluate the fundoplication location.
Results: From January 2009 to December 2011, 576 patients from a wide range of ages, newborns to 18 year olds, were treated. Average chirurgical time was of 42 minutes without conversions. In 86% of the cases there was symptomatology remission. In seven patients (1.21%) fundoplication migrated towards the thorax, four were asymptomatic, two upon a month and two after six months. Three patients presented abdominal pain and vomit after three, six and eight months respectively. Two patients were related to omentum pyloric obstruction. Of the seven patients with migration, four presented neurological damage and three respiratory symptoms. All patients were re-operated using laparoscopy. In five cases we encountered wide hiatus, two with pyloric obstruction where migration tended to the right, and a tight hiatus. No recurrences with a follow up of 6 months.
Discussion: Fundoplication migration is, as it has been previously argued, a common complication with an unknown etiology. The efforts to avoid its immigration have focused in reinforcing the diaphragm closure or fixing the fundoplication to the diaphragm pillars, have not diminished this issue. The esophagus is an elastic organ that tends to recover its shape after being moved, thus, building a fundoplication in an esophagus without tension avoids thorax migration as it has been reported with a migration frequency of 1.21% in contrast with the widespread reported 7%.
Adequate dissection of the esophagus allows the fundoplication above the esophageal-gastric union according to DeMeester principles. Preserving a portion of the esophagus released from the fundoplication, provides the advantage to allow an adequate movement of the esophagus during breathing, as well as significantly reduces the fundoplication migration and discards the need to suture the fundoplication to the diaphragm.
TRANS HIATAL COLON INTERPOSITION USING MINIMAL INVASIVE PROCEDURE
Introduction: There are various indications that suggest a further esophageal replacement in children, being the most frequent atresia, or peptic and caustic damage to the esophagus. These surgeries have been conducted by moving the abdominal organ to the neck blindly in long procedures. There is only one available report of video assisted colon interposition in children older than one year as published by Estévez. The purpose of this piece is to present a case of a patient that had a long gap esophageal atresia that was treated by video assisted colon interposition, in order to evaluate this procedure and its feasibility, advantages as well as disadvantages.
Case presentation: Child of 8 months of age, with type III esophageal atresia. A tracheoesophageal fistula closure was conducted using thoracoscopic approach locating proximal pouch, with a greater distance than 3 vertebrae. Therefore, both esophageostomy and gastrostomy were practiced. Bearing in mind the patient weight of 8 kilograms, a colon trans hiatal interposition through minimal invasion was programmed. 4 ports were used, one trans umbilical 10 mm, two 3 mm and one 5 mm port, including a 5 mm optic 30 degrees. Transversal colon interposition was conducting irrigating the medic colic, retro pyloric meso colocation, pyloroplasty, colo-colic umbilical assisted anastomosis, and intra corporeal colo-gastric anastomosis. As well, mediastinal dissection under direct vision, colon ascent directed using a catheter placed in the neck, colo-esophageal anastomosis and gastrostomy. Total surgical time was 4 hours, without accidents, a contrasted study was conducted on the seventh day demonstrating adequate colon colocation without fistulae and oral feeding. Patient was discharged from the hospital after 10 days without complications. Follow up of 6 months without evidence of gastrocolonic reflux and adequate tolerance to oral feeding.
Discussion: For some patients with esophageal atresia, whether type I, type III long gap or with caustic esophageal injuries, esophageal substitution might be required. These are long and challenging procedures with significant tissue exposure, in which most of the cases the tissue ascent needs to be conducted blindly. As a result of this previous situation, most of the morbidity reported takes place due to vascular or nerve injury. Minimal invasive procedures in children have been conducted since 2003 for this type of gastric ascents, with only one report that uses colon in patients of more than one year of age. Due to its characteristics, such as irrigation, length and acid resistance, we as well chose to use the colon. Conducting the procedure through laparoscopy also contributed to the reduction of added morbidity with reproduction of the steps used in an open approach. In contrast with open techniques, mediastinal visualization is remarkable. A clear perception of the structures prevents vascular injuries and allows the collocation of the colon safely in the mediastine. For this patient this procedure proved to be feasible in consideration of the previously mentioned advantages, however a greater number of cases are required in order to validate its real utility.
LAPAROSCOPIC SURGERY FOR CONGENITAL DUODENAL OBSTRUCTION: A SINGLE CENTER EXPERIENCE WITH 24 CASES
Introduction: Laparoscopic surgery (LS) for congenital duodenal obstruction (CDO) in children is considered one of the most demanding pediatric laparoscopic procedures, especially in the newborn. Reported experiences with LS for CDO in children have been scanty. The aim of this study is to investigate the feasibility, safety and effectiveness of LS in management of CDO in children.
Methods: Medical records of patients with diagnosis CDO undergoing LS at our center from March, 2009 to October, 2012 were reviewed. Selection criteria were patients with stable cardio-respiratory function, without other gastrointestinal anomaly or generalized infection and with body weight over 1500 g. All the operations were performed by 2 surgeons with extensive experience in LS. For the LS, one infra- or trans-umbilical 5 mm port for camera and two 3 mm ports for instruments were used. Laparoscopic duodeno-duodenostomy was carried out using our technique of oblique “simple” anastomosis with intracorporal knots.
Results: 24 patients were identified (13 boys, 54.2%) with median age at operation 11 days (ranged 3 days – 30 months). Twenty patient (83.3%) were neonates. Fifteen patients (62.4%) had bilious vomiting, 9 patients (37.6%) - nonbilious vomiting. The median weight at operation was 2600 g (ranged 1800 g to 9 kg). In 15 patients (62.5%), duodenal obstruction was caused by atresia type I (duodenal web), in 4 (16.7%) – by annular pancreas and in 5 (20.8%) – by atresia type III (with separation of the proximal and distal end). Laparoscopic duodeno-duodenostomy was carried out in 21 patients, duodenotomy and web resection in 2, and jejuno-duodenostomy in 1 patient. The mean operative time was 108 minutes (ranged 60 – 150 minutes). There was no intra- or postoperative complication related to the surgery, no case of conversion. The median time from the operation to initial oral feeding was 5.0 days. The median postoperative hospital stay was 7.5 days. Follow-up 1 – 40 months, all patients were in good health but one, who had undergone web resection, was re-hospitalized due to recurrent duodenal stenosis 5 months after discharge. A laparoscopic duodeno-duodenostomy was done for this patient with good outcome.
Conclusions: LS is feasible, safe and effective for treatment of selected cases of CDO in children at experienced centers. The technique of oblique simple anastomosis for laparoscopic duodeno-duodenostomy could be a good anternative to the diamond-shape anastomosis.
LAPAROSCOPIC MANAGEMENT OF INTESTINAL DUPLICATION CYST IN CHILDREN
Introduction: The standard approach in management of intestinal duplication cyst (IDC) in children is open surgery. The role of laparoscopic surgery (LS) in management of IDC in children is still not well defined since only limited numbers of cases have been reported. The aim of this study is to investigate the feasibility, safety and effectiveness of laparoscopic management of IDC in children.
Methods: Medical records of patients with diagnosis IDC undergoing LS at our center from March, 2009 to October, 2012 were reviewed. Operations for IDC were performed by surgeons with different laparoscopic experience. One 10 mm umbilical port and 0 to 2 other 5 mm ports were used. Two types of laparoscopic procedures were performed: completely laparoscopic (CL) when the entire operation was carried out intra-abdominally and laparoscopic-assisted (LA) when the IDC was delivered out of the abdomen (after maximal reduction of its volume by puncture and aspiration) via the minimally extended umbilical incision and removal of the cyst or intestinal resection was performed extracorporally.
Results: 26 patients were identified, 15 boys (57.7%) and 11 girls (42.3%), with median age of 24 months (ranged from 10 days to 9 years). The most common clinical presentations were abdominal pain (88.5%), vomiting (61.5%), distended abdomen (30.8), fever (15.4%). Ultrasound and CT showed intestine-like cystic structure in most cases and preoperative diagnosis of IDC was made correctly in 22 patients (84.6%). The remained incorrect diagnoses were cystic lymphangioma, appendicitis, ovarian cyst and choledochal cyst. The mean size of the cyst was 4.2±1.8 cm (ranged from 2 cm to 9 cm). The most common location of IDC is ileum (18 cases, 69.2%), followed by caecum (5 cases, 19.2%), jejunum (1 case, 3.8%), transversal colon (1 case, 3.8%) and duodenum (1 case, 3.8%). The performed procedures were CL in 15 cases (57.7%) and LA in 11 cases (42.3%). In 9 cases, only a single umbilical port was used. Complete excision of the cyst was carried out in 8 cases (30.8%), cystic unroofing in 12 (46.2%) and intestinal resection in 6 patients (23%). All cases of intestinal resection were performed by the LA approach. The mean operative time was 63.8±20 minutes (ranged 30 – 90 minutes). There was no intra- or postoperative complication, no case of conversion. The median postoperative hospital stay was 2 days (ranged 2–4 days). For the follow up from 1–36 months, all patients were in good health, without recurrence.
Conclusions: Laparoscopic management is feasible, safe, effective and could be the treatment of choice for most cases of IDC in children. Both CL or LA approach could be used in selected cases but LA would be preferred in case of intestinal resection.
LAPAROSCOPIC MANAGEMENT OF PYLORIC ATRESIA IN A NEONATE WITH EPIDERMOLYSIS BULOSA
Pyloric atresia (PA) is rare and may be associated with epidermolysis bulosa (EB). Open surgery has been considered standard treatment for PA but in cases of PA associated with EB, postoperative mortality has been reported as high as 50%. No case of PA treated by laparoscopic surgery has been reported to date. We report the first case of PA in a neonate with EB, treated successfully by laparoscopic surgery. A full term girl with birth weight 2000 g was admitted to our hospital with respiratory distress, non-bilious vomiting, lots of blister and erosions on the skin. Plain abdominal X-ray showed one big air bubble of the stomach. Upper gastrointestinal contrast study confirmed complete obstruction of the pylorus. The diagnosis PA associated with EB was made and the child was operated at the age of 7 days by laparoscopic approach, using 3 trocars: one infra-umbilical 5 mm port for camera and two 3 mm ports for instruments. After longitudinal pylorotomy, complete pyloric obstruction by a membrane (4–5 mm thickness) was found. Resection of the membrane and transversal closure of the pylorus were carried out, using interrupted 5.0 PDS sutures. Operative time was 90 minutes. There was no intra- or post-operative complication. The child recovered uneventfully after the operation, started oral feeding at postoperative day 7 and was discharged 5 days later. Follow up after 16 months the child is still alive and can eat well, without vomiting.
LAPAROSCOPIC SLEEVE GASTRECTOMY IN A PEDIATRIC PATIENT WITH PRADER-WILLI SYNDROME
Background: Although the overweight problem has became popular in China, but since the difference of food structure, obesity is not a serious problem in chinese children, rare cases need to receive bariatric operation. But Prader-Willi syndrome, a chromosomal disorder characterized by the presence of hyperghrelinemia, hyperphagia, and obesity, is rarely dignosised in mainland China because of the genetic testing cannot commonly get in most of local hospital. Since the weight loss surgery is the major therapy of this disease, we reported here one case of Prader-Willi syndrome which received the laparoscopic sleeve gastroctomy.
Patient: A 13 yr old boy was hospitalized for pneumonia, respiratory failure, pulmonary heart disease, obesity-ventilation syndrome and sevious obesity. At the time of his admission, his body weight was 160 kg, the height is 137 cm, the BMI was 85. He had to receive intubate ventilation, antibiotics and liver/heart protective therapy. After his symptoms was reduction, a series test was made. Absence of amplification of paternal allele on chromosome 15q11 was detected by MSPCR, the diagnosis of Prader-Willi syndrome was confirmed. He also has a serious sleep apnea hypopnea syndrome and hyperlipidemia. His blood pressure and OGTT is normal.
Surgical Procedure: Laparoscopic sleeve gastrectomy was performed with 5 trocars technique. In brief, a 40-Fr bougie was used as a sizing tube, and sleeve gastrectomy was performed from proximal antrum to the angle of His using multiple cartridges of ENDO-GIA linear stapler. Intragastric instillation of methylene blue solution was used to check integrity of staple line intraoperatively.
Results: The patient had a uneventful recovery after operation. No surgical complication occurred and oral intake was allowed on day 4 after the operation. Upon 6 months after operation, the parents of the child reported significant reduction of food-craving behavior, the weight is 129 kg, lost 31 kg,. the BMI decreased to 65 kg/m2. The symptom of serious sleep apnea was significant reduced and no pneumonia recurrence. His scope of activities increases significantly.
Discussion: The adaptation age of bariatirc surgery is 18 to 55 years old, proposed by the US NIH. But for those Prader-Willi syndrome childern, serious sleep apnea hypopnea syndrome and pneumonia is often life-threatening. Since there is no malabsorptive component in laparoscopic sleeve gastrectomy, nutritional disturbance is minimal and it appears to be more suitable for adolescents. Till et al, repoted that LSG is a safe and effective alternative for the surgical treatment of morbidly obese adolescents, may be used as a stand-alone operation. Fong et al, also reported that significant reduction of body weight and level of serum ghrelin can be achieved with minimal morbidity by LSG or LMGBP in patients with PWS. In our case, the LSG saved our patient life and improved the quality of his life. We believe that laparoscopic sleeve gastrectomy is applicable in these PWS children whose age <14 years old with serious obesity.
DISTAL CYST SUTURE SUSPENSION HELPS TO DO THE COMMON CHANNEL EXPLORATION IN THE LAPAROSCOPIC REPAIR OF CHOLEDOCHAL CYSTS
Aim: We report our experience of distal bile duct exploration during laparoscopic repair of choledohal cyst.
Methods: During 2012, 7 patients with choleduchal cysts (mena age, 3.44 years) have protein pluges in the common channel shown by the MRCP. The laparoscopic cyst excision and Roux-en-Y hepatojejunostomy were successfully done on these children. The operations were done with three conventional trocars technic (right upper quadrant, right paraumbilical and umbilicus). A cholangiography was first taken by cyst puncture to confirm the anomalous junction of pancreaticobiliary duct and protein pluges in the common channel. When the cyst was isolated, a 2-0 melsilk suture was passed through the distal cystic wall and retracte to the abdominal wall. Then the distal cyst was further isolated until the duct became obviously thinner. The second 2-0 melsilk suture was passed through the distal CBD to retract it became straight. A small incision was made at on side of the distal CBD, under direct vision during laparoscopy, a biliary bougie or ureteral catheter was inserted to explorate the common channel or to irrigate and remove the protein plugs. Second cholangiogrphy was taken to confirmed the complete chlearance and a free passage of pancreatic duct and duodenum.
Results: In four of seven cases, biliary bougie can pass into the duodenum, in the other three the ureteral catheter also pass into the duodenum successfully. The irrigation were done and the protein plugs were completely removed. The mean operative time were 3.42 hours. Neither mortality nor complication of postoperative pancreatitis or pancreatic leakage were observed. These patients were followed up for 6 months, no stone formation were found.
Discussion: For congenital choledochal cyst treatment, with development of the laparoscopic technique, laparoscopic choledochal cyst excision, biliary reconstruction, and Roux-en-Y hepaticojejunostomy have been increasingly used in many countries. But the distal bilary tract exploration is difficult under the laparoscope. Some authors have reported using ureteroscope or catheter irrigation combined with cholagiogram to remove the protein plugs in the common channel. Since the angle of junction of pancreaticobiliary duct and tortuosity of the common channel, the actual manipulate is not so easy sometimes. We use one or two retraction suture to suspend the distal cyst. The common channel to the duodenum was stretched straight. The work of irrigation the protein plugs became easier, and the biliary bougie can even pass into the duodenum. Our conclusion is distal cyst suture suspension can improve efficiency rate of the common channel exploration in the laparoscopic repair of choledochal cysts.
ALTERNATIVE LAPAROSCOPIC APPROACHES FOR PANCREATIC PSEUDOCYST IN CHILDREN
Introduction: Pancreatic pseudocyst (PPC) in children could be treated by open surgery, ultrasound guided percutaneous approach, endoscopic or laparoscopic techniques. Several methods were described in the literature. In this video, we present two different laparoscopic techniques.
Video presentation: Laparoscopic cystogastrostomy was performed in a 17 year old girl. Following laparoscopic exploration, omental bursa was opened. A thick wall, large PPC was found. Three cm incisions on the both posterior gastric wall and PPC were made and an anastomosis was performed. In our second patient who was an 8 year old boy, laparoscopic external drainage was preferred. In this patient, the wall of PPC was not thick enough to carry an anastomosis to the gastric wall. Inflammation on the PPC wall was also significant. Following a purse string suturing, an external drainage catheter was placed inside of the cyst.
Conclusion: Laparoscopy has several advantages in PPC surgery. By observation of the characteristic of the cyst, the surgeon chooses the best minimal invasive approach. A direct vision of the cyst prevents possible complications caused by percutaneous techniques. The cosmetic outcome is perfect comparing to the open procedures. The size of the cyst, thickness of the wall, neighboring structures and the degree of inflammation determine which laparoscopic approach would be feasible for the patient.
ENDOSCOPIC ULTRASOUND-GUIDED TRANSGASTRIC DRAINAGE OF PANCREATIC PSEUDOCYSTS IN CHILDREN
Purpose: Endoscopic ultrasound-guided transgastric drainage of pancreatic pseudocysts is well established in adults. There are limited data regarding this procedure in pediatric patients. The aim of this study is to investigate the safety and efficacy of endoscopic ultrasound-guided pseudocyst drainage in children.
Materials and Methods: Between January 2006 and October 2012, five patients admitted to our hospital for pancreatic pseudocysts underwent endoscopic ultrasound-guided transgastric drainage. The clinical data about the therapies and recovery of the patients was reviewed and analyzed.
Results: Five children (aged 10 to 14 years old) had successful endoscopic ultrasound-guided transgastric drainage of pancreatic pseudocysts. All five patients had complete resolution of the pancreatic pseudocyst clinically and radiologically. The median follow-up period was 21 months (range, 10–32 months). No complications and recurrence were found.
Conclusions: Endoscopic ultrasound-guided transgastric drainage pancreatic pseudocysts can be achieved safely in children. It is a safe, effective and minimally invasive therapeutic method for pancreatic pseudocysts in pediatric patients, but larger comparative studies are still needed.
POTENTIAL APPLICATION OF LAPAROSCOPIC TREATMENT IN ACUTE SMALL BOWEL OBSTRUCTION WITHOUT PRIOR LAPAROTOMY HISTORY IN CHILDREN
Background: Pediatric patients with acute small bowel obstruction (ASBO) without prior history of abdominal surgery often require emergent surgical intervention; however, the detailed etiology of pediatric ASBO has not been clarified and the role of laparoscopic treatment for it is even more unclear. The aim of this study was to assess our experiences with ASBO without prior surgical history and to try to define benefits for those patients who are approached laparoscopically.
Patients and Methods: A retrospective review was done of cases surgically treated as ASBO without prior laparotomy history from 2001 to 2011. We excluded neonates and patients with malrotation, intussusception, appendicitis, abdominal trauma, and abdominal tumors. Data obtained included demographics, etiology, intraoperative and postoperative course. Patients were sub-grouped into two categories: group A (n=12) included patients who initially underwent the laparoscopic approach and group B (n=23) included patients who underwent only laparotomy. The operative procedure was decided by the attending doctor. We estimated the feasibility and efficacy of the laparoscopic approach.
Results: In total, 35 children (27 males) were surgically managed for ASBO. Mean age was 79.9±63.4 months. The most common etiologies of ASBO included Meckel's mesodiverticular band (n=12), intestinal volvulus without malrotation (n=8), transmesenteric hernia (n=5), adhesive band (n=4), foreign body (n=3), mesenteric cyst (n=2), and Winslow hernia (n=1). Eleven patients (31.4%) had strangulated and gangrenous bowel, including 5 cases of transmesenteric hernia, 3 cases of intestinal volvulus, 2 mesenteric cysts, and one adhesive band. Excision of the diverticulum was performed in fifteen cases (42.9%), and another nine cases (25.7%) required only reduction or band dissection. In group A, 3 cases (25%) were converted to laparotomy for resection of strangulated intestine. Gangrenous intestine made the working space poorer and organ orientation unclear. Eight cases received diverticulectomy by laparoscopically assisted minilaparotomy, and the other one needed only dissection of the band. In group B, 8 cases needed resection of gangrenous bowel. Seven cases were treated by diverculectomy, and the other 8 cases received reduction of bowel or band dissection. The mean time to restart feeding and the mean length of stay was not remarkably different. Three adhesive intestinal obstruction cases occurred as a complication of laparotomy.
Conclusion: Our results showed that some intraabdominal band was observed as a cause of ileus in about half of the cases (16/35); however, in these cases necrotic change of involved intestine rarely occurred (1/16). When intestinal necrosis is strongly suspected, the laparoscopic approach makes it difficult to get the whole picture of the intraabdominal space; so, open surgery is recommended. If the cases in group B are reviewed from the perspective previously described, 7 of 23 patients could be treated by diverculectomy in laparoscopically assisted minilaparotomy, and 8 of 23 patients could be treated by purely laparoscopic procedure. The laparoscopic approach to ASBO without prior history of surgery is an attractive alternative to the open approach, if the involved intestine is not necrotic.
LAPAROSCOPIC TREATMENT OF PANCREATIC TRANSECTION IN CHILDREN: 2 CASE REPORTS
Introduction: Pancreatic injuries are uncommon in childhood, the most common cause being blunt abdominal trauma. The appropriate treatment of these injuries is still controversial. There are two schools of thought regarding treatment: a conservative approach to all injuries (grade I-IV) versus surgical treatment of grade III and IV injuries. Laparoscopic treatment of grade IV injuries has the potential to become a new management option in children. We report 2 patients who sustained pancreatic transsection from blunt abdominal trauma and were successfully treated with laparoscopic resection.
Case Reports: Patient 1, a 12 year old boy, fell over the handle bar of his bicycle and presented 1 day after the incident. Patient 2, a three year old boy, was involved in a pedestrian vehicle accident and presented on the day of the accident. Both had total transection of the distal pancreas with involvement of the pancreatic duct on CT. In addition, the second patient had a splenic hematoma that had stopped bleeding. In both cases an emergency laparoscopic distal pancreatectomy preserving the spleen was performed on the day of admission. In case 1, the pancreatic stump was oversutured and a drain left in situ. In case 2 the pancreatic duct was not visualized and the area sealed with Glubran2. The first patient didn't receive any special feeds and was discharged on day 5 post-operative. The second patient had a more extensive injury and received TPN for 5 days to be discharged home symptom free on post operative day 7. Ultra-sound follow-up 6 weeks post injury was normal with no pseudo cysts detected.
Conclusion: Our preliminary experience with the laparascopic treatment of traumatic pancreatic transsections in these 2 cases show encouraging results, suggesting that it is not only technical feasible, but well tolerated and seems to have a comparatively good outcome.
THE APPLICATION OF LAPAROSCOPIC SURGERY ON UNDIAGNOSED CHRONIC ABDOMINAL PAIN IN PEDIATRIC PATIENTS
ABSTRACT WITHDRAWN
THE COMBINED TREATMENT OF LAPAROSCOPY AND ENDOSCOPY FOR CONGENITAL FUSIFORM BILIARY DILATATION
Objective: The purpose of the study was to assess the efficacy of laparoscopy and endoscopy for congenital fusiform biliary dilatation.
Methods: Between June 2006 and June 2012, the clinical presentation, radiological features and surgical treatment of 18 cases with congenital fusiform biliary dilatation were analyzed (mean age, 6.5 years, ranging from 1 year 8 months to 14 years). The postoperative symptoms, laboratory examination and bile duct changes were evaluated during follow-up term.
Results: The symptoms included abdominal pain(18), and jaundice(13). In 18 patients, the levels of serum and urinary amylase increased when abdominal pain appeared. Intraoperative cholangiography showed filling defect and dilatation of the common channel and pancreatic ducts visualization in 18 cases, including 9 cases of pancreatic duct dilatation. The protein plugs and/or stones were removed completely under laparoscopy and endoscopy in 18 cases. Patients were followed up for 3 months to 6 years. The biochemical and ultrasound examination showed no increase in pancreatic amylase and recurrence of the stones in the common channel and pancreatic duct.
Conclusions: The children with congenital fusiform biliary dilatation had abdominal pain, with high levels of serum and urinary amylase when abdominal pain appeared and filling defect and dilatation of the common channel showed by radiologic findings, laparoscopy and endoscopy clearance of the protein plugs and/or stones in the common channel in congenital fusiform biliary dilatation is effective, with good long-term results observed.
LAPAROSCOPIC-ASSISTED SUBTOTAL COLECTOMY COMBINED WITH TRANSANAL SINGLE SOAVE PROCEDURE FOR CONGENITAL EXTENSIVE HIRSCHSPRUNG'S DISEASE
Objective: To summarize the experience of laparoscopic-assisted subtotal colectomy combined with transanal single Soave procedure for congenital Hirschsprung's Disease (HD).
Methods: From March 2006 to September 2012, datas of 21 patients with HD were retrospectively collected. All of the patients underwent laparoscopic-assisted subtotal colectomy combined with transanal single Soave procedure.
Results: All the procedures were successfully completed in the 21 cases within an average laparoscopic operation time of (118±7) min and the total operation time of (147±11) min. The length of the resected segmentwas 60∼90 cm, and the estimated intraoperative blood loss was 8–20 ml. 2 cases were diagnosed as Hirschsprung's disease-allied disorder (HAD) by pathology. There were no short-time postoperative complications. Follow-up was available range 1–2 years, during which their defection frequency decreased from 8–18 per day latest postoperatively to 1–3 perday 1 years after the surgery; and no fecal incontinence nor recurrent constipation occurred, except one child sometimes with watery stool had dirt pants at the 6 months after the surgery; anorectal manometry showed results close to normal range.
Conclusion: Laparoscopic-assisted subtotal colectomy combined with transanal single Soave procedure for HD and HAD is a safe and feasible procedure, with lessminimal invasion, invisible scars at the abdomen, and is much better than open surgery.
Key Words: Laparoscopy; Subtotal colectomy; Congenital Hirschsprung's Disease.
PERFORMANCE OF PAEDIATRIC PATIENTS FOLLOWING A WATSON FUNDOPLICATION
Background: Gastroesophageal reflux affects 2–8% children and is associated with significant morbidity and even mortality, normally from aspiration pneumonia. The traditional surgical anti-reflux procedure has been Nissen's operation, involving repair of the crural defect and a 360 degree fundal wrap. However, there has been a significant incidence of mechanical complications that require re-operation (7%). In 1991, David Watson described a partial anterior (180 degree) wrap that achieved good reflux control with reduced gas bloating. Recent randomised controlled trials of outcome at 5 years indicate that this procedure produces long-lasting and superior symptom control relative to Nissen fundoplication.
Aim: We prospectively studied all cases subjected to a Watson fundoplication over a 15 year period in our centre.
Methods: A retrospective review of a prospectively created database was performed. Demographic data was extracted and outcome from intervention studied.
Results: 77 children (50 boys and 27 girls), 26 (34%) neurologically compromised, underwent laparoscopic Watson fundoplication from 1995 to 2012. Freca PEGs were placed at the time of laparoscopy in 11 cases. There were no incidences of perforation and no revisions have been required to date. The overall rate of minor complications was 14.3%. Immediate complications included liver injury in 4 cases (5.2%) and bleeding in 7 cases (9.1%), 1 requiring transfusion. A port site hernia occurred in 2 cases (2.6%). Dysphagia occurred in 9 cases (11.7%), 6(7.8%) of these were confirmed to have tightness at the cardio-oesophageal junction on barium swallow. However none required dilatation. Acid reflux was reported in 14 cases (18.2%) and belching in 3 cases. A single case has a small hiatal hernia which is being managed medically.
Conclusion: Watson partial fundoplication, whether in normal or neurologically compromised children can be performed with minimal complications and with durable results. This technique is a tenable alternative to a Nissen fundoplication.
THE SIMPLIFIED APPROACH TO PEDIATRIC APPENDECTOMY
Aim: Laparoscopic appendectomy has became the routine technique for management of acute appendicitis in children in many centers. However there is still a debate about the best approach. Three trocars usually are necessary to perform laparoscopic appendectomy. To simplify the procedure and reduce the number of incisions and trocars the authors have proposed 3-step protocol utilizing use of one, two or three ports for appendectomy in children. This study aimed to evaluate the results of the one or two port extracorporeal and three port intraabdominal techniques of pediatric appendectomy.
Methods: This is retrospective study of 100 children treated for appendicitis. The surgical technique involved an insertion of one 11 mm trocar through the umbilicus and use of an operative 10-mm laparoscope with a working channel. The appendix was freed and delivered out through the umbilicus. The appendectomy was performed extracorporeally. If the appendix was placed retrocecally or had adhesions, the second port was introduced low in the midline and the appendix was mobilized, exteriorised and resected in the same manner. In the cases of very short or gangrenous appendix the third port was introduced and intraabdominal appendectomy was performed. Patient were compared regarding the duration of operation, operative and postoperative complications.
Results: Laparoscopic appendectomy was performed in 100 children (58 males, 42 females). The operation was successfully completed using one port in 48 children - group 1. The second port was necessary in 27 children - group 2. Twenty five children required the third port insertion - group 3. Mean operative time was 33, 39 and 45 minutes respectively. No intraoperative complications occured. Wound infections occurred in 4 (8.3%) patients in group 1, three (11.1%) in group 2 and four (16.0%) in group 3. One patient in group 3 developed an abdominal abscess managed conservatively.
Conclusions: The one port extracorporeal appendectomy is a feasible and safe technique in children allowing in our experience to operate about half of all patients with acute appendicitis. Additional insertion of the second port allows to mobilize the appendix and perform its extracorporeal resection in further 1/4th of cases. The extracorporeal technique is associated with an excellent cosmetic results leaving in most cases a single abdominal scar in the umbilicus. These approaches have less operative duration compare to a 3-port technique. The use of a 3-port technique was limited only to cases with perforated appendix and/or immobile caecum.
LAPAROSCOPIC COMBINED URETHROSCOPE CHOLECYSTOLITHOTOMY WITH GALLBLADDER PRESERVED TREATMENT CHILDREN WITH GALLSTONE
Objective: To evaluate Minimally invasive laparoscopic combined urethroscope Cholecystolithotomy with gallbladder preserved treatment of children with gallstone.
Methods: Retrospective 13 cases clinical data of our hospital from August 2009 to August 2012 using minimally invasive laparoscopic combined urethroscope Cholecystolithotomy with gallbladder preserved treat children with gallstone, 7 males and 6 females, aged 1 year and 1 month to 11-year-old, multiple and the muddy stone in nine cases, two cases with single stones, two cases gallbladder stones combined with hereditary spherocytosis. Operation procedure: supine position, one 5 mm Trocar was placed in the umbilical incision. pneumoperitoneum pressure is 10∼12 mmHg, exploration liver size, texture, gallbladder filling. According to the bottom of gallbladder, another 5 mm Trocar was inserted at costal margin for grasping forceps, then gallbladder was pulled out the abdominal wall, then the gas was released. 0.5 cm incision was made at the bottom of gallbladder, 0 degrees pediatric urethroscope was inserted into the gallbladder. After checking stone location, quantity and presence of incarceration or not, the stones was removed under the help of electricity cut ring. Small stones can be removed with suction aspiration and saline irrigation. Urethroscope exploration confirm residual stones. Cholangiography with 38% diatrizoate confirm whether the residual stones in commom bile duct and pancreatic duct abnormality. 5-0 PDS suture gallbladder incision. Laparoscopic splenectomy was performed the casesof cholecystolithiasis with hereditary spherocytosis.
Results: 13 cases were successfully completed surgery, operative time (30 min-90 min; Average: 50 min), bleeding (2 ml-5 ml), no intraoperative blood transfusion. Follow-up time is from 6 mon–3 years. All clinical symptoms disappear after surgery. No gallstone recurrence in 11 cases, 1 muddy stone patient found a small stone in the gallbladder after surgery with the size of 0.1 cm without any clinical symptoms. 1 patient was lost.
Conclusion: Laparoscopy combined urethroscope gallbladder treatment of children with gallstone can reserved gallbladder function, the operation procedure is simple with rapid postoperative recovery and fewer complications. It is a feasible method of treatment for children with gallstone.
LAPAROSCOPIC-ASSISTED RESECTION OF MECKEL'S DIVERTICULUM
Objective: To explore the diagnosis and treatment of Meckel's diverticulum by laparoscopy.
Methods: From January 2008 to December 2012, 45 cases of Meckel's diverticulum diagnosed by laparoscope, and they were resected under laparoscope or were pulled out through the umbilical incision for resection and anastomosis.
Results: All of patients of Meckel's diverticulum were cured, which involved 36 cases (80.0%) with the main clinical manifestation of lower gut bleeding, 6 cases (13.3%) of abdominal pain and 3 cases (6.6%) of intestinal obstruction. About 18 cases (40.0%) were diagnosed definitely only through laparoscope. The operative time was 30 min to 65 min, mean 42 min. The hospital stay was 3 d to 7 d, mean 4.5 d.
Conclusions: Meckel's diverticulum administrated by laparoscopy is a very effective treatment with less trauma, slighter pain and quicker recovery, and also a confirmed diagnosis for abdominal complex diseases.
Keywords: Meckel's diverticulum; Laparoscopy; Children.
LAPAROSCOPIC REPAIR OF HIATUS HERNIA IN CHILDREN
Objective: To investigate the efficacy of the laparoscopic repair with Nissen fundoplication of hiatus hernia in infants.
Methods: 29 patients, 21 boys and 8 girls, with hiatus hernias underwent laparoscopic repair with Nissen fundoplication between September 2007 and October 2012. The average age of the patients was 1.2 years (range 7 days to 5.5 years).
Results: The procedure was completed laparoscopically in 27 cases and the median operating time was 147 min (range 90 to 390). Two cases were turned to open procedure, because of huge defect of the diaphragm and severe adhesions in the abdomen respectively. No complication occurred; 25 patients were asymptomatic at last follow-up (range 1 month to 5 years). 4 patients relapsed in 3 to 18 months after surgery; 3 of them were re-operated by laparoscopic repair and the other one, suffering a huge diaphragmatic defect, underwent a repair of biological patch.
Conclusions: Hiatus hernia can be reduced and repaired safely with laparoscopic access, which have the advantages of good efficacy, quick recovery, minimal invasion, and safety.
SINGLE-INCISION LAPAROSCOPIC ROUX-EN-Y HEPATICOJEJUNOSTOMY: THE INTRAOPERATIVE CHOLANGIOGRAM FOR CHILDREN WITH CHOLEDOCHAL CYSTS
Objective: In single-incision laparoscopic Roux-en-Y hepaticojejunostomy, the chlangiogram is difficulty. We have had some experience for intraoperative cholangiogram.
Methods: From April 2011 to April 2012, we reviewed 75 children who underwent SILH. All underwent intraoperative cholangiogram successfully. First, extracorporeal stay suture of 2/0 silk on a curved needle was inserted just below the right costal margin and passed through the serosa of fundus of the gallbladder for cephalad liver retraction to expose the hepatic hilum and fix the gallbladder. Then a 20-gauge angiocatheter puncture through the abdominal wall and the gallbladder fundus, at last, we injected the 30% Iohexol and used the Siemens Mobilett XP Digital DR to take a film.
Results: By the cholangiogram, we can know the morphology of gallbladder, cyst, hepatic duct, and pancreaticobiliary conjunction.
Conclusions: By this method we can get the cholangiogram to direct the operation.
Keywords: Single-incision laparoscopic, choledochal cysts, cholangiogram.
LAPAROSCOPIC LYSIS OF THE TREITZ LIGAMENT TREATMENT FOR SUPERIOR MESENTERIC ARTERY SYNDROME IN 9 CHILDREN
Objective: To analyze the etiology, diagnosis and treatment of superior mesenteric artery syndrome (SMAS).
Methods: From November 2007 to February 2012, nine patients suffered SMAS had been successfully treated by laparoscopic lysis of the Treitz ligament.
Results: All patients achieved complete relief of their symptoms and were able to take a regular diet.
Conclusion: Laparoscopic lysis of treitz ligament should be considered an alternative treatment for SMAS which shows excellent outcome based on the current literature.
LAPAROSCOPIC ASSISTED DUHAMEL OPERATION FOR TOTAL COLONIC AGANGLIONOSIS
Purpose: To describe the surgical technique and initial outcomes of laparoscopic assisted Duhamel operation for total colonic aganglionosis (TCA).
Methods: Four trocars were used. The mesentery of the colon was divided. An ileostomy was taken down. A tunnel was made through the posterior space of the rectum. The rectum was divided with a stapler at the level of the peritoneal reflection. The posterior wall of the rectum was incised tranversally 1 cm above the dentate line. The ileum was pulled through the rectal opening. The posterior rectal wall and the anterior ileal wall were divided longitudinally and anastomosed together using a stapler.
Results: From August 2009 to August 2012, 17 patients suffering from total colonic aganglionosis were operated.
Patient ages varied from 10 months to 14 months (mean: 13.1 months±1.9 months). The mean operative time was 169.2 minutes±18.9 minutes (range: 150 – 210 minutes). The hospitalization mean was 5.3 days±0.6 days (range: 4 – 6 days). There were no intraoperative complications. There were no intraoperative or postoperative deaths. There were no early postoperative complications. Follow up from 3 months to 36 months was obtained in 17 (100%) patients. Constipation has not seen in any patient, 5 patients (29.4%) had 1–2 defecations per day, 7 patients (41.2%) had 3 – 4 defecations per day, and 5 patients (29.4%) had more than 4 defecations stools per day. 6 patients had mild soiling. 4 patients had sometimes diarrhea. 2 patients had enterocolitis. 3 patients had perianal excoriation.
Conclusion: Laparoscopic assisted ileal pull-through is feasible, safe and provides good continence outcomes for total colonic aganglionosis.
LAPAROSCOPIC DIAMOND-SHAPED ANASTOMOSIS FOR CONGENITAL DUODENAL STENOSIS DUE TO ANNULAR PANCREAS FOUND IN SCHOOL-AGE IDENTICAL TWINS
Background: About half the cases of annular pancreas show onset in the neonatal period as duodenal atresia, but the remaining half are diagnosed in elder infants or adults by symptoms of epigastric pain, feeling of fullness after eating, nausea and vomiting, and pancreatitis. Here, we report a very rare case of congenital duodenal stenosis due to annular pancreas in school-age identical twins, which were performed laparoscopic diamond-shaped anastomosis.
Case Report: [Case 1] An 8-year-old boy exhibited vomiting after meals and showed poor weight gain but had not been treated. At the age of 8 years old, hepatic dysfunction was noted, and ultrasound examination revealed mild dilatation of the common bile duct and pneumobilia. In upper GI series, stenosis was observed in the descending part of the duodenum, and a diagnosis of duodenal stenosis due to annular pancreas was made based on abdominal CT, MRI and upper gastrointestinal endoscopy. Surgery was performed laparoscopically by 4 ports. After mobilization of the duodenum, annular pancreas was identified, and we confirmed that there was no pancreaticobiliary maljunction by intra-operative cholangiography. Diamond-shaped anastomosis could be done easily by using the same method as open surgery. The operation time was 4 hours 47 minutes and there was no intra-operative complication and no conversion to open procedure.
[Case 2] An 8-year-old boy was the identical twin brother of case 1. The same examination as case 1 was performed because of poor weight gain, and stenosis in the descending part of the duodenum due to annular pancreas was found. Surgery was performed in a manner similar to that described in case 1.
Conclusion: Laparoscopic diamond-shaped anastomosis in elder children has no difference in caliber, and provides a good field of view, thus making anastomosis relatively easy, but the position of duodenal papillae and presence of pancreaticobiliary maljunction must be checked before or during surgery.
EARLY EXPERIENCE WITH SINGLE INCISION ENDOSURGICAL PEDIATRIC NISSEN FUNDOPLICATION
Introduction: Single incision paediatric endosurgery is rapidly gaining popularity. It offers excellent cosmetic results, and may be associated with decreased post operative pain. We have employed this technique for Nissen fundoplication.
Method: Between May 2011 and October 2012 we performed nine single incision fundoplications. Three disposable trocars were used through separate fascial incisions. A long 45 cm 30° laparoscope, standard straight instruments and a roticulating dissector (Covidien) were used. A minimal esophageal mobilisation was done. In the first 6 patients, an extra corporeal suture technique was used to create the wrap. In the last three patients, an intra corporeal technique was used. Different techniques for liver retraction have been used. In the last three patients we used a homemade needlescopic liver retractor.
Results: There were no intra operative adverse events or major post operative complications. Mean operative time was 95 minutes. Follow-up range was from 1 month to 17 months, and reflux subsided in all patients.
Conclusion: Laparoscopic Nissen fundoplication can be done safely and successfully using single umbilical incision approach. Operation time is longer, and the technique is more difficult, but as experience is gained, and with advances in instrumentation and equipment, these problems will be overcome.
(A short video is available, if accepted for oral presentation.).
LAPAROSCOPY-ASSISTED RESECTION FOR MECKEL'S DIVERTICULUM IN CHILDREN
Objective: To investigate the diagnostic and applicative value of Laparoscopy for Meckel's diverticulum in children.
Methods: The clinical data of 35 children with Meckel's diverticulum who underwent resection between April 2008 to December 2011 retrospectively analyzed. All cases were cured by laparoscopy. The intra-operative accidental injury, postoperative complications, postoperative general condition and prognosis were evaluated analysis.
Results: Laparoscopy-Assisted resection for Meckel's diverticulum was successfully performed on all cases. The mean duration of laparoscopic dissection was 42 minutes (range, 35–75 minutes). The mean blood loss was 7 ml (range, 5–20 ml). After 2 days, all patients regained normal intestinal motility and the patients could eat liquid on the third day after operation. All infants had uneventful postoperative recovery without wound infection. During a follow-up for 6–36 months (mean, 22 months) there was no recurrence case.
Conclusions: Laparoscopy had obvious superiority for the children's and treatment, which should be the best choice.
NEONATAL INTRAHEPATIC CHOLESTASIS CAUSED BY CITRIN DEFICIENCY IN NORTH CHINA: A CASE REPORT
We report a 2-month-old Chinese baby boy with neonatalintrahepatic cholestasis caused by citrin deficiency (NICCD). On review of the family history, it was found that the patient had an elder sister, who died of biliary atresia. His stools were pale yellow in colour. Although he was thriving well, he was noted to be jaundiced from the first week of life and was investigated for prolonged jaundice. The investigations showed hyperbilirubinaemia 144.9 (control range 1.6–20.6) umol/L with conjugated fraction 133.2 (control range 0–6.5) umol/L, ALT 94 (control range 0–40) u/L, AST118 (control range 0–40) u/L, fasting blood glucose 2.04 (control range 3.9–6.1) mmol/L. The amino acid and acyl-carnitine analysis showed citrin deficiency in blood. He received expectant treatment in department of pediatrics for 2 weeks, and the investigations showed no improvement. The clinical features of NICCD may include intrahepatic cholestasis, diffuse fatty liver with parenchymal cellular infiltration associated with hepatic fibrosis and variable liver dysfunctions, such as coagulopathy and hypoalbuminaemia. This may lead to extensive investigations in the affected infant to exclude biliary atresia. Progonosis is much better in biliary atresia patients who were administrated by Kasai procedure below 2 months old. Otherwise, biliary liver cirrhosis should be inreversible though the operation was performed, liver transplantation may be inevitable. Then his extra-hepatic biliary tract was explored using laparoscope, and the cholangiography was performed to explore his intra-hepatic biliary tract, but no abnormality was detected. Laparoscope exploring technique accompany with cholangiography is not only used as a therapeutic approach to treat some biliary tract disease like concentrate bile thrombus syndrome, it is also used as a prophage diagnosis method to identify some severe biliary tract malformation like biliary atresia, which should be accept operation. Furthermore, this minimal invasive technique is even used for some pathological jaundice disease like obstructive neonatal hepatitis and NICCD, which should be accept medical treatment. Because of excluding some severe biliary tract malformation using the laparoscope exploring technique accompany with cholangiography, we acquire valuable chance to avoid inconvertible liver cirrhosis for some pathological jaundice disease.
COMPARISON BETWEEN LAPAROSCOPLC AND OPEN LADD'S PROCEDURE FOR NEONATES WITH INTESTINAL MALROTATION
Objective: To compare the efficacy and feasibility of laparoscopic with open Ladd's procedure intreatment of intestinal malrotation in neonate.
Methods: From February 2008 to October 2012, 32 patients (aged 2∼28 days, weighing 2.0∼3.6 kg) with intestinal malrotation underwent laparoscopic Ladd's procedure (Group A) and 21 patients (age 3∼28 days, weighing 2.1∼4.0 kg) with intestinal malrotation underwent open Ladd's procedure (Group B).
Results: Fifty-three cases suffered from intestinal malrotation were mangaged successfully by Ladd's procedure. The average length of postoperative hospital stay ranged for group A was 6.4 days, that for group B was 5.5 days. Two of group A were complicated by adhesive ileus, the other of group A was not postoperative complication. One of group B was complicated by incisional hernia. Follow-up observations were 2∼24 months.
Conclusions: Laparoscopic Ladd's procedure is a safe and effective technique, which has more advantages then open Ladd's procedure.
Key words: Laparoscopes; open; Ladd's procedure; intestinal malrotation.
LAPAROSCOPY NISSEN FUNDOPLICATION TREATING NEONATES AND SMALL INFANTS WITH HIATUS HERNIA
ABSTRACT WITHDRAWN
LAPARSCOPIC REPAIR OF CONGENITAL DUODENAL OBSTRUCTION IN NEONATE
Objective: To evaluate the curative effect of laparoscopic surgery treatment of congenital duodenal obstruction (CDO), such as web or annular panctreasl, in neonate.
Methods: Sixteen neonates with CDO who underwent laparoscopic surgery were analyzed retrospectively from October 2010 to September 2012 (12 with web, and 4 with annular panctreas). Outcomes of interest were operative time, postoperative leaks, and postoperative full time of feeding.
Results: The laparoscopic procedures were completed without intraoperative complication in 16 neonates. Average operating time was 87±23 minutes. There were no duodenal anastomotic leaks. Time to initial feeding 5.1±1.9 days, and time to full oral intake 9.3±2.1 days. Average hospitalization time was 11.5±2.0 days. Follow-up upper gastrointestinal tests show no evidence of stricture or obstruction.
In one newborn open abdominal operation was required.
Conclusion: The laparoscopic surgery treatment of CDO is safe and efficacious.
Key Words: Laparscopic, congenital, duodenal obstruction.
THE SOLUTION FOR POLLUTION IS DILUTION – LAPAROSCOPIC TREATMENT OF APPENDICULAR PERITONITIS IN CHILDREN
While laparoscopic appendicectomy (LA) is the most common procedure in pediatric surgery, the laparoscopic therapy for appendicular peritonitis (AP) still remains a subject for discussion because of the potential for complications to occur, particular on the learning curve. The latest publications, nonetheless, advocate in favor of the laparoscopic approach. In line with these, we report a series of successful outcomes of laparoscopic technique (LT) of various forms of AP, which, until recently, were managed in our unit by the means of open surgery. Twenty six children with AP have been treated with the use of the LT along with 122 consecutive cases of LA carried out during 2012 (February-November). The patient age ranged between 2–16 years. Clinical presentation apart from the abdominal signs comprised sepsis manifestation in fifteen children, which in one of them was also associated with small bowel obstruction (SBO). The intra-operative findings included local peritonitis (n-8), appendiceal mass/abscess (n-11), diffuse panperitonitis (n-6) and a combination of panperitonitis with pelvic abscess and adjacent multiple inter-intestinal collections causing SBO (n-1). The LT involved a dissection of the inflammatory mass/collection, drainage of the pus, completion of appendicectomy and copious peritoneal lavage (PL) of the contaminated areas, followed by the placement of a pelvic drain (PD). The operative procedures were performed by a team of four surgeons. Those of them who were on the learning curve were provided with the close supervision and back-up by the experienced team leader. As a result, all operative procedures were effectively completed with zero conversion rates. There were no intra-operative complications encountered. The operative time ranged between 55 to 150 minutes (mean 87 minutes). The pelvic drains were removed after 24–48 hours. No postoperative morbidity occurred. All children made prompt, uneventful recovery (normal temperatures, restored gastro-intestinal function, regained full range of activity, drop in high WCC) within 2–5 days. In conclusion, LT of AP with the use of PL is safe and efficacious in achieving the best possible outcomes in the shortest post-operative period. The role of PL with following PD as the curative element of the LT, should not be underestimated. Additionally, the safety of the operative performance should be and can be secured with the participation of an experienced surgeon (operating/assisting/supervising).
THE SIGNIFICANCE OF MRCP AND IOC IN THE SURGICAL TREATMENT FOR CONGENITAL CHOLEDOCHAL CYST
Background/Purpose: There are many anatomic variations at the proximal end and the distal end of the choledochal cyst. Intrahepatic biliary dilation and stenosis are the common accompanied conditions. Mistake in dealing with these malformations would be an important factor in the postoperative ascending cholangitis. Meanwhile, PBM (pancreaticobiliary maljunction) occurs in almost all patients with choledochal cyst. In dealing with the distal end of the cyst, special attention should be paid to avoid excessive stump being left, or the pancreatic duct being damaged. So, it is very important to know the morphology of the bile duct in detail before surgery, especially laparoscopic surgery. Imaging by MRCP (magnetic resonance cholangio- pancreatography) and by IOC (intraoperative cholangiography) may contribute certain helpfulness in this point of view.
Methods: A retrospective study was made on 23 patients, of 2010–2012, with choledochal cysts who were examined by MRCP and IOC accordingly.
Results: According to Todani's classification, there were type Ia 12 cases, type Ic 3, and type IVa 8 (left hepatic duct stricture 2, common hepatic duct 5, and confluence of left and right hepatic duct 1). According to Komi's detail classification of PBM, MRCP showed PBM in 10 cases (43%), including type Ia in 4, type IIa in 2 and type IIb in 4; while IOC showed PBM in 19 cases (83%), including type Ia in 5, type Ib in 3, type IIa in 2, type IIb in 6, IIIa in 2, and IIIb in 1. The shape of the cyst and the range of the biliary dilation were well illustrated in both MRCP and IOC. The 3D image of MRCP might show the different aspects, so that the stricture could be easily located. The image of the cyst was delineated clearly in IOC, but sometimes, misled by possible overlapping and resulted in oversight. In addition, the diameter of the bile duct appeared little bit bigger in IOC than in MRCP. It was due to the injection pressure. The detectability of PBM by IOC was much better than MRCP (p<0.01). All positive findings of biliary strictures were proved and corrected during operation before anastomosis with jejunum. Under the guidence of imaging, the distal end of the cyst was cut close by the pancreatico-biliary junction and no injury of pancreatic duct occurred in this study.
Conclusion: MRCP combined with IOC is, although some invasive, significant in raising the accuracy and confidence in the operation of choledochal cyst.
MINIMALLY INVASIVE SURGERY FOR ALIMENTARY TRACT DUPLICATION CYSTS IN CHILDREN
Background: The current trend of therapy for alimentary tract duplication (ATD) is minimally invasive surgery (MIS). The reported conversion rate, however, is considerably high, up to 30%, particular in newborns and infants. We present our experience with the MIS allowing us to successfully manage ATD with the minimal possible conversion rate.
Methods: Twenty four MIS procedures carried out in 22 children with various types of ATD in our tertiary referral hospitals during 2007 to 2012 were retrospectively analyzed.
Results: The patient age ranged between 5 days to 15 years. The group of newborns and infants included 12 patients (54.5%). 13 children (59%) were symptomatic. In the rest the diagnosis was made with the incidental findings. The diagnostic workup involved US, CT, contrast studies and MRI imaging. The anatomic localization of ATD was supradiaphragmatic in 9 cases, infradiaphragmatic in 12, thoracoabdominal in 1, multiple lesions were in 2. Total MIS were carried out in 20 cases, assisted MIS – in 2. The laparoscopic approach was used in 14 cases for the following lesions: esophageal (n-1), gastric, (n-5), gastric in the pancreas (n-1), duodenal (n-1), jejunal (n-2) and ileocecal (n-3). Thoracoscopic procedures were carried out in 10 cases for esophageal cysts (n-9) and duodenal duplication extending into the thoracic cavity (n-1). The Interval procedures combining both laparo- and thoracoscopic approchers were carried out in 2 cases of multiple lesions. The operative technique involved endoscopic enucleation with/or without suturing of the muscle coat in 21 cases of cystic non-communicating duplication of various localization and unroofing of duodenal cyst in 1. The conversion was proceed with in two cases (8.4%) due to encountered technical difficulties: in one – of the complex thoraco-abdominal cyst and another – massive adhesive process in the abdomen after previous open surgery. Intraoperative complications such as mucosal perforations occurred in 2 cases (8.4%). The endosurgical repair with suturing was performed in one of them and in another one of the missed duodenal perforation laparotomy was undertaken on the next day. Postoperatevely all patients made uneventful recovery. The follow up completed in 20 patients showed no evidence of recurrence.
Conclusion: Total or assisted MIS procedures for ATD are efficacious and safe and can be successfully performed in children including newborns and infants. Furthermore, simple enucleation should be considered as the optimal endosurgical technique for non-communicating cystic type ATD.
ROLE OF DIAGNOSTIC LAPAROSCOPY AND APPENDICECTOMY IN CHILDREN WITH CHRONIC PAIN ABDOMEN AND SIGNIFICANT MESENTERIC LYMPHADENOPATHY
ABSTRACT WITHDRAWN
LAPAROSCOPIC SPLENECTOMY FOR THALASSEMIA MAJOR - TRICKS OF THE TRADE
ABSTRACT WITHDRAWN
PANCREATECTOMY FOR DIFFUSE PERSISTENT HYPERINSULINEMIC HYPOGLYCEMIA OF INFANCY
Aim: For diffuse persistent hyperinsulinemic hypoglycemia of infancy (PHHI), most published series agree that that a “near-total” pancreatectomy is required. However, which extent of pancreatectomy should be executed is still controversy. This article tries to discuss what extent of pancreatectomy is suitable for patients who suffered from diffuse PHHI.
Methods: From 2009 to 2012, there were 5 diffuse PHHI patients enrolled in our center. All patients presented with hypoglycemia immediately after birth. The laboratory findings displayed persistent hypoglycemia and hyperinsulinism in all of the infants. Although glucocorticoid, diazoxide and octreotide were used, hypoglycemia could not be controlled at a satisfying level. CT scan and PET-CT were performed before the operation which helped to exclude the focal PHHI. Intraoperative frozen section biopsy analysis has also been used to differentiate between focal and diffuse disease. Laparoscopic pancreatectomy were performed in 4 patients. Open technique was used in one patient. During the operation, the tail, body, uncinate process and part of pancreatic head are resected, only leaving a rim of pancreatic tissue surrounding the common bile duct and along the duodenum. Patients were followed up for a median of 12.5 months.
Results: In our group, the median weight at surgery was 7.5 kg and the median age at procedure was 4.5 months (range, 1–8 months). Before the operaiton, the baby″s blood sugar manifested with 0.9–1.2 mmol/L. The plasma insulin level reached 24.1–27.3 U/L. The average operation time was 115–163 min. Three days postoperatively, the blood sugar level improved to averaged 14.3 mmol/L. All patients recovered uneventfully. Four of them need insulin injection when they discharged. Six months after the operation, only 1 patient still depend on insulin. The blood sugar level was controlled in all patients.
Conclusion: Extensive pancreatectomy (98%) may not be warranted as the first procedure for patients with PHHI. Pancreatectomy leaving a rim of pancreatic tissue surrounding the common bile duct and along the duodenum is enough for diffuse PHHI patients. It could avoid biliary tree injury, and pancreatic endocrine and exocrine insufficiency.
HOW I REMOVE AN ILEOCECAL DUPLICATION
Introduction: When a duplication is placed into the ileocecal valve, we have to perform a conservative procedure. It is possible to remove it close to the muscular layer and without opening of the cyst, but there is a risk of ileal perforation. We report a procedure to perform a safe enucleation of this kind of duplication.
Materials and Methods: The first step is to stabilize the ileocecal junction with 2 transparietal threads through the antimesenteric edge of the ileum and through the cecal taenia. Then, we could open the duplication after coagulation and its bulging part was resected to expose the deep mucosal layer. Then the mucosa was grasped and dissected progressively close to the muscular layer. At the end of the procedure, the pression on the ileum allowed to control the absence of perforation. The ileal wall was closed with a few knots.
Results: Since 2008, a prenatal diagnosis of duplication in the right flank was done in 6 children and was confirmed by postnatal ultrasonography. They were symptom-free and they underwent a laparoscopy between 2 and 4 months. A seventh child, 5 years old, had also an ileocecal duplication and needed an excision. The laparoscopy confirmed the diagnosis of duplication of the ileocecal junction in these 7 children. The procedure was performed easily in the 6 babies, without perforation of ileum or cecum. It was more difficult in the 5-year-old child with more adhesions between the mucosa and the muscle, but no perforation occured. The follow-up was uneventful and the 7 children were discharged at day 1 or day 2 with a normal food. There was no relapse with a follow-up of 26 months.
Conclusion: The enucleation of ileocecal duplications is feasible easily in infants and children with a transparietal stabilization of the ileocecal junction and resection of the bulging part of the duplication before to remove the deep part of the mucosa.
TRANSVERSE COLONIC VOLVULUS IN A CHILD: SUCCESSFUL MANAGEMENT WITH DECOMPRESSION AND DELAYED LAPAROSCOPIC COLOPEXY
Abstract: We report a case of transverse colonic volvulus in a 7 year child with normal development. Operative findings at laparotomy showed a 270 degree transverse colonic volvulus (TCV), with un-usual ligamentous abnormalities. A loop ileostomy was formed following detorsion, with delayed laparoscopic colopexy. This is the first case to describe decompression by diversion ileostomy as management in the acute phase of transverse colonic volvulus and allowed delayed laparoscopic colopexy, so avoiding unnecessary bowel resection.
Case Study: A 7 year old boy presented with abdominal pain and vomiting and constipation for 5 days. His pulse was elevated at 118 but was haemodynamically stable and apyrexial. His abdomen was soft but distended with palpable tender loops of bowel. Digital rectal exam revealed a rectum loaded with hard faeces. Plain abdominal radiograph showed an abnormally dilated transverse colon, but no sequential dilation above, and faeces in the rectum.
The child was taken to theatre. Initial colonoscopy showed soft stool in rectum, empty sigmoid and descending colon, and colonoscope was unable to advance beyond. A midline laparotomy was performed where a massively dilated, torted transverse colon was found. A 270 degree clockwise volvulus was reduced and inspection revealed no obvious gangrenous bowel. Normal small bowel rotation but an absent hepatocolic and abnormal splenocolic ligaments were noted. Following detorsion, a diversion loop ileostomy was formed.
He was brought back four months later for laparoscopic assisted stoma closure and colopexy. The redundant transverse colon was fixed at multiple points to the ligamentum falciparum. He has been reviewed in clinic 18 months following closure and is thriving and opening bowel regularly using a small amount of laxative.
Conclusion: This is the first case describing formation of loop ileostomy following acute detorsion with delayed laparoscopic colopexy. Classically the ubiquitous redundant transverse colonic loop is resected either acutely or at an interval to prevent recurrence. Initial decompression, without resection, and delayed colopexy offers a safe, conservative approach in the case of non-necrotic transverse colonic volvulus.
DIAGNOSIS AND MINIMALLY INVASIVE SURGICAL TREATMENT OF MECKEL DIVERTICULUM BY DOUBLE BALLOON ENTEROSCOPY
Background/Purpose: To demonstrate the diagnosis of Meckel diverticulum by double balloon enteroscopy and its guidance for minimally invasive surgery.
Materials and Methods: From August 2011 to March 2012, 16 pediatric patients with bloody diarrhea received anal examination using double balloon enteroscopy. The distal small intestine examination was performed through the repeated sequential inflation of the inner endoscopic balloon and the jacket tube balloon. When the dual-chamber-like intestine was detected, with enteroscopic guidance, a small incision was made at the navel ring or abdominal wall to perform lesion tissue removal and intestinal anastomosis.
Results: A total of 12 cases of Meckel diverticulum were diagnosed and successfully treated with surgery. No recurrence was observed during the follow-up.
Conclusion: Double balloon enteroscopy is an ideal tool to non-invasively diagnose and minimally invasively treat Meckel diverticulum.
CLINICAL ANALYSIS OF ENTIRELY LAPAROSCOPIC RESECTION FOR MECKEL'S DIVERTICULUM
Objective: To compare the clinical efficacy and complications in laparoscopic resection for Meckel's diverticulum with that of the laparoscopic-assisted or traditional ones.
Methods: The clinical data of 58 cases of Meckel's diverticulum resected by laparoscopy between January 2006 and January 2011 were analyzed. Laparoscopic surgery in 13 cases, laparoscopic-assisted resection in 25 cases and laparotomy in 20 cases. Laparoscopic group was compared with the other two groups, for the differences of the operation time, flatus defecation time, the incidence of postoperative complications and postoperative hospital stay.
Results: They were not significantly different between laparoscopic group and laparoscopic-assisted group, but they were significantly different between laparoscopic group and laparotomy group.
Conclusions: Compared with conventional laparotomy, laparoscopic technique is safe, efficient, minimal invasion, less pain, shorter operative time, fewer complications and shorter recovery period, which should be promoted in the application. If mature of the technology or conditions permitted, laparoscopic surgery can be carried out.
LAPAROSCOPIC LIVER RESECTION IN CHILDREN: A REPORT OF 4 CASES
Objective: Laparoscopy for the resection of liver masses in children has remained undeveloped despite the wide acceptance of laparoscopy in the field of adult liver surgery. The authors report 4 cases of nonanatomical or anatomical laparoscopic hepatic resection of in children.
Surgical Techniques: Under general anesthetic, the patient was positioned supine. Four to five trocars were placed including a 10-mm port in the umbilicus by using Hanson technique. Three additional 5-mm ports were inserted in the right and left upper quadrant. An additional liver retractor was placed in the epigastrium. Pneumoperitoneum was established and maintained at 10–15 mm Hg during tumor resection. For anatomical left hepatectomy extra-hepatic artery or potal vein was isolated and ligated. Ultrasound guidance was used to guide diathermy scoring of the liver capsule in preparation as necessary. The superior liver parenchyma was then dissected by using Harmonic scalpel. Moderate vessel was dissected by an ultrasonic dissector and sealed by the LigaSure (Valley lab). Finally the linear EndoGIA was used to staple off the specimen from branch of the left hepatic artery and the vascular stapler remained for the hepatic vein. The specimen was removed by an extended umbilical/port incision or a small Pfannenstiel incision.
Results: There were 2 boys and 2 girls with an age range from 2 months to 5 years old. The other operative parameters were shown in the table. No perioperative complication was observed. The patients have been followed up for three months to six years and have remained asymptomatic since surgery.
Characteristics of Patents of Laparoscopic Liver Resection
Conclusion: These cases demonstrate the feasibility of laparoscopic hepatic resection, even for balking large tumors, employing standard principles of liver surgery and safety.
Objectives: The recently developed transorally inserted anvil (OrVilTM; Covidien, Mansfield, MA, USA) is a reconstruction technique of intracorporeal circular stapling esophagojejunostomy, aimed to simplify the anastomotic procedure. This technique is being gradually wide applicated in upper-GI cancer patient during laparoscopic total gastrectomy in adult. We used this skill to treat one child of congenital esophageal stenosis located in lower esophagus.
Methods: A 3-year-old girl had the symptom of intermittent vomit lasting over 2.5 years. The semifluid and solid food could not be eaten. The esophageal contrast study showed upper esophagus expanded and lower part at 10th thoracic vertebral level really narrow. No gastroesophageal reflux was detected by 24hrs PH monitor. Balloon dilatation for several times was ineffectively. The stenosis was comfirmed by esophageal endoscopic examination. Five trocars were placed in abdomen. The narrow segment of esophagus was resected by endo-GIA under laparoscopy. Under the esophageal endoscopy monitoring, the anastomosis of the esophagus and stomach was finished by OvilTM technique (20-mm DST SeriesTM EEATM OrVilTM device). The Thal procedure to prevent the gastroesophageal reflux and the pyloroplasty were done at the same time.
Results: The patient stayed in hospital for three weeks. No anastomotic leakage and infection in mediastinum and abdomen after surgery. Full oral feeding 7 days postoperation and no vomit happened again. The mature cartilage of tracheobronchial remnants and esophagitis was detected by the pathological examination of resected segment. The girl has been following up over 18 months. All the symptoms were disappeared after surgery and everything could be eaten. No symtem related to gastroesophageal reflux. Balloon dilatation was performed in one and two months respectively after surgery to treat the anastomotic stricture.
Conclusions: The principles of a good anastomosis are good vascular supply, must be tension-free, and the use of a high-quality surgical technique. Congenital lower esophageal stenosis adapt for treating by OrvilTM technique in laparoscopic surgery. The use of the OrVilTM is safe, quicker and easier and to avoid huge surgical trauma of the traditional method through thoracic and abdomen simultaneously.
MANAGEMENT OF APPENDICEAL ABSCESS IN CHILDREN WITH LAPAROSCOPIC APPENDECTOMY
Background: It remains a matter of major controversy in management of appendiceal abscess on the treatment techniques choice: immediate appendectomy, interval appendectomy or nonoperative management. Purpose: this study investigated the value of laparoscopic appendectomy in management of appendiceal abscess in children.
Materials and Methods: 17 cases of appendiceal abscess were hospital admitted from January 2010 to November 2011. 16 cases had 5–7 days symptoms and one case suffered from leukemia had 14 days symptoms before hospital admission, age varies from 2 to 7 years old, male/female ratio: 15:2, all cases had fever waved from 38.5 degree C to 40 degree C and had significant peritonitis. All appendectomies were performed in a 3-trocar technique including one 10 mm tracor inserted into the abdomen through an infraumbilical incision and two 5 mm tracors inserted into the abdomen at left and right lower side abdomen respectively. The mesoappendix was divided with harmonic scalpel the base of the appendix was ligated with 2 endoloops, then it was resected and removed through the umbilical trocar using an endocatch bag. The right lower abdominal cavity and pelvic cavity were irrigated with 800–1500 ml saline and 0.5% flagyl (ratio: 1:1), and then drainage was inserted in cases of peritonitis.
Results: All appendectomies were performed successfully without conversion to open appendectomy, the mean operating time was 78 minutes, the duration of hospitalization was 7.2 days, postoperative complication only included wound infection (2 of 17) without intraperitoneal abscess.
Conclusion: Laparoscopic appendectomy is an acceptable alternative to management of appendiceal abscess in children.
LAPAROSCOPIC LADDS AND DUODENOJEJUNOSTOMY IN A VERY LOW BIRTH WEIGHT PREMATURE INFANT
Background: Laparoscopic repair of duodenal atresia (DA) and intestinal malrotation has been well established previously. This approach however, has not been frequently reported in the very low birth weight (VLBW) premature infant.
Materials and Methods: We present a case of a 1400 g premature infant born with prenatally diagnosed duodenal atresia and polyhydramnios. The infant was hemodynamically stable without supplemental oxygen requirement but with abdominal distension. A postnatal abdominal x-ray demonstrated a double bubble (Figure 1). Nasogastric decompression alleviated the distension and non-bloody non-bilious fluid was noted. A postnatal echocardiogram confirmed the presence of a structurally normal heart and a patent ductus arteriosus.

Using a four-port technique, 3 mm minilaparoscopy was used for diagnostic laparoscopy. Duodenal atresia along with intestinal malrotation without volvulus was diagnosed. A laparoscopic Ladd's procedure followed by a side-to-side vertical duodenojejunal anastamosis was completed with intracorporeal knot tying techniques. The appendectomy was performed extracorporeally via the umbilicus.
Results: Upon completion of the Ladd's procedure, a side-to-side duodenojejunostomy was easily fashioned. Given the small size of the bowel, only four stitches were necessary on the front and back wall. The orientation of the bowel subjectively made the anastamosis easier.
A postoperative GI series confirmed a patent anastamosis without extravasation on postoperative day 5 (Figure 2) and feedings were initiated. The infant was on full feeds within three days.

At one-year follow-up, the infant has thrived, does not have any reflux and has required no further intervention.
Conclusions: Laparoscopic management of duodenal atresia with malrotation may be considered in very low birth weight premature infants. After surgical correction of the rotational anomaly, the anatomic orientation allowed for better visualization and positioning for a side-to-side duodenojejunostomy.
LAPAROSCOPIC VENTRICULO-GALLBLADDER SHUNT IN A NEUROLOGICALLY IMPAIRED CHILD WITH A HOSTILE ABDOMEN
Backgound: Internal decompression of severe hydrocephalus is frequently required in neurologically impaired (NI) children. Peritoneal, atrial and subgaleal shunts are the preferred route of drainage respectively. Other comorbidities, non-neurosurgical operations and infectious complications may require alternate internal drainage routes in a small percentage of NI patients. Ventriculo-gallbladder (VGB) shunts are often a last resort and performed infrequently. Current literature indicates that these are performed via laparotomy.
Materials and Methods: We present a case of a 12-year-old neurologically impaired (NI) child with CPMR, multicompartmental hydrocephalus, posterior fossa cyst, spastic quadraparesis who presents with mediastinitis, severe bacterial endocarditis, an abdominal pseudocyst and pneumonia. His past medical history is significant for necrotizing enterocolitis requiring laparotomy and bowel resection with reanastamosis, gastroesophageal reflux and failure to thrive requiring open fundoplication and gastrostomy tube placement. Additionally, he has had multiple ventriculoperitoneal shunts that had to be removed due to infectious complications. He has also had two ventriculoatrial shunts, the most recent of which had to be removed due to severe endocarditis with valvular vegetation and regurgitation.
A laparoscopic VGB was successfully performed using a three-port technique. The shunt was tunneled in subcutaneous tissue from the scalp to the abdomen and inserted into the gall bladder using a modified Seldinger technique. A laparoscopic double pulse string using monofilament absorbable suture was used to anchor the shunt within the gallbladder.
Results: Operative time was 125 minutes. Laparoscopic adhesiolysis was performed for 75 minutes. Shunt function was established and documented immediately. The child required a shunt revision within the first 48 hours at the level of the valve. The distal portion of the shunt did not have to be revised.
At 23-month follow-up, the VGB shunt remains in place without having required any other revisions.
Conclusions: Laparoscopic VGB shunt may be performed even in a patient with complex abdominal surgical history. To our knowledge this is the first report of a laparoscopic approach to this shunt.
LAPAROSCOPIC TRANSVERSALIS FASCIAL ILEO PUBIC REPAIR FOR LARGE GROIN HERNIA IN PEDIATRIC AGE GROUP
Introduction: Laparoscopy became widely used in the management of pediatric inguinal hernia (PIH) due to its many advantages. Herniotomy is not suitable for large PIH including wide internal ring.
Aim: We present a procedure with suturing the transverse abdominal fascial arch to the ileopubic tract laparoscopically in order to repair large groin hernia.
Patients & Methods: 22 consecutive children with large unilateral PIH were treated along a 5-year period in a tertiary academic center. All cases were subjected to laparoscopic exploration followed by laparoscopic hernia repair as a day case surgery. Sutures were placed on from the fascial arch to the ileopubic tract avoiding the spermatic vessels and duct in interrupted manner using 2/0 Vicryl suture. In some cases, a purse string suture is added to narrow the internal ring. The knot is tied either intra corporeally or extra corporeally according to surgeon's preference.
Removal of the suture and needle done transabdominally. Operative findings and post operative results and complications were assessed. The patients were followed for a period ranged between 6 and 55 months.
Results: We have 21 boys and one girl. Operative age ranged between 1 year and 15 years. Three or four sutures were placed in either case. Operative time ranged between 26 & 60 min in unilateral cases without conversion. Scrotal edema reported in 4 cases, 3 cases of port infection were reported and treated conservatively. One case of recurrence was reported and no case of testicular atrophy was reported in the follow up period. Cosmetic outcomes were excellent.
Conclusion: This procedure is helpful in the functional reconstruction of the inguinal canal. Laparoscopic inguinal herniorraphy by this technique is feasible and safe. Consequently, there is lower risk of injury to the spermatic duct or vessels than the conventional herniorrhaphy. Larger studies and long-term follow up are needed to support our encouraging results.
LAPAROSCOPIC TRANSPERITONEAL DIVISION OF PATENT PROCESSUS VAGINALIS WITH PURSE STRING CLOSURE OF PROXIMAL PERITONEUM FOR HYDROCELE IN CHILDREN – IS LAPAROSCOPIC HIGH LIGATION ENOUGH? - ARE THEY ALL COMMUNICATING?
Background: Laparoscopy is being routinely used in the treatment of inguinal hernia in children. Many different techniques have been described. There is however no information about the role of laparoscopy in the management of hydrocele in children. Are they all communicating? Is laparoscopic high ligation with scrotal aspiration enough?
Purpose: To retrospectively report our technique of laparoscopic transperitoneal division of patent processus vaginalis with purse string closure of proximal peritoneum for hydrocele in children.
Materials and Methods: The records of 6 patients who underwent laparoscopic repair for hydrocele over a period of 3.5 years were retrospectively reviewed. Median age was 6 years.
Technique: Incision was made in the scar of the umbilicus and a 5 mm step trocar is introduced. We then place a 5 mm 30 degree telescope through this port after pneumoperitoneum was achieved. Internal/deep rings were identified on both sides. In all cases a communication was identified on the side of the hydrocele. If there is a patent PPV identified on unilateral/bilateral side then a unilateral/bilateral repair is performed respectively. We use the previously described technique of trans-peritoneal division of the hernia sac with purse-string closure of proximal peritoneum. Two small 2 mm incisions are made on either side of the umbilicus about 5 cm apart and instruments were directly introduced. The peritoneum surrounding the deep ring was circumferentially divided and the proximal peritoneum was closed with purse-string suture thus completing the high ligation of the PPV. Pneumoperitoneum was evacuated, port was withdrawn and umbilical fascia was closed with 2’0’vicryl suture. Skin sites were apprimated with dermabond glue. The scrotal fluid/hydrocele was then aspirated with a 14 G angiocath.
Results: All patients tolerated the procedure well and none had any intraoperative or postoperative complications. Contralateral PPV was found in one child. Bilateral repair was done in one child. Over a Median follow up of 1 year none had any ipsilateral or contralateral recurrences, wound infections or testicular atrophy. Cosmesis was excellent in all kids and the scars were almost invisible.
Conclusion: Laparoscopic repair of patent processus vaginalis is safe and effective treatment of hydrocele in children with no complications or recurrences in our small series. They were all communicating hydroceles and some kind of communication was always identified. Laparoscopic high ligation with scrotal aspiration was adequate treatment for this condition. However, our study is limited by the small numbers and medium term follow up and more number would be needed to draw serious conclusions.
LAPAROSCOPIC MANAGEMENT OF ABDOMINAL CYSTIC LYMPHANGIOMA (ABOUT 10 CASES)
Cystic lymphangioma of the abdomen is a rare congenital tumor. It represents 1/6 of all cystic lymphangiomas of the body and corresponds to 7% of intra-abdominal cyst.
We report in this retrospective study 10 cases of abdominal cystic lymphangioma managed by videosurgery in the Department of Pediatric Surgery at the Children's Hospital of Rabat-Morocco (north Africa) during 12 years (from 2000 to 2012). The average age is seven years with six boys and four girls.
The clinical symptoms was dominated by the abdominal pain followed by the abdominal mass. The clinical examination was nonspecific. The diagnosis was made by ultrasonography and computerized CT Scan.
All patients were managed firstly by laparoscopy. The procedure was achieved laproscopically in seven cases. In three cases intestinal resection was needed and the bowel was exteriorised through the umbilical incision after aspiration of the cyst. In 2 cases conversion to laparotomy with a minimal trans-umbilical incision was needed.
In one case the cystic lymphangioma was extended to the retroperitonal space and was resected.
No death was noted in our series.
We conclude that laparoscopy is very useful in the diagnosis and the management of abdominal cystic lymphangioma. The complete resection is possible in the main cases.
When laparotomy is needed laparoscopy permits to minimize the abdominal incision.
LAPAROSCOPIC EXCISION OF A COMPLEX PERI-PANCREATIC MASS
Introduction: Peri-pancreatic cystic masses in children are most commonly simple cysts associated with pancreatitis or trauma. Complex cysts or those without an explanatory history increase concern for malignancy. Laboratory tests and imaging can aid in the diagnosis, but definitive diagnosis and treatment often requires operative intervention. We present an interesting case of laparoscopic surgical excision of a complex cystic peri-pancreatic mass in a pediatric patient.
Case Description: A 14-year-old male presented to an outside hospital with a left sided abdominal mass, postprandial pain, and weight loss of several pounds over the past month. He denied recent illnesses or abdominal trauma. An ultrasound of the abdomen demonstrated a complex cystic, septated mass in the left upper quadrant measuring 10×10 cm. A CT of the abdomen showed the mass was anterior to the pancreas. Tumor markers AFP, B-hCG, VMA, and HVA were negative and serum lipase was only mildly elevated (660 U/L). Due its location posterior to the stomach, the mass was easily evaluated by endoscopic ultrasound with fine needle aspiration. Fluid cytology, mucin, and amylase were all negative. The decision was made to perform laparoscopic excision of the mass. Three ports were used, two 5 mm trocars in the right and left lower quadrants and a 12 mm trocar at the umbilicus. The cystic mass was carefully dissected off of the pancreas and an intraoperative frozen section was negative for malignancy. A drain was placed anterior to the pancreas for postoperative surveillance of a potential pancreatic injury. Postoperatively, the patient did well. He tolerated a regular diet, and required minimal pain medication. On postoperative day one amylase levels were normal on fluid analysis and the drain was removed. He was discharged on postoperative day one. Final pathology was consistent with pancreatic pseudocyst. Follow-up ultrasound was normal at 8 weeks.
Conclusion: Complex peri-pancreatic masses in children can be effectively resected by the laparoscopic approach. In our experience, this approach provides great visualization, mobilization, and relative ease of resection.
LAPAROSCOPIC APPROACH FOR ENTEROCOLITIS-RELATED ACUTE INTESTINAL PERFORATION: INITIAL EXPERIENCE
Background: Acute intestinal perforation secondary to enterocolitis is a severe event that requires immediate treatment. Exploratory laparotomy has been the gold standard in the past decades. Recently, several reports described that minimal invasive surgery has been successfully applied to colonic perforation in emergent setting for both adult and children. The authors would introduce the experience on laparoscopic approach for acute intestinal perforation for children and evaluate operative feasibility and outcomes.
Methods: Between June 2009 and October 2012, 6 patients under 18 years old underwent laparoscopic surgery for acute intestinal perforation secondary to enterocolitis. The demographics of the patients, operative details, postoperative compilcations and the time resuming oral intake were retrospectively collected by chart review.
Results: The age ranged from 2 to 15 years, with median age of 9 years. Gender distribution was 4 boys and 2 girls. All perforations were solitary and located at cecem in 2 cases, ascending colon in 2 cases, ileum in 1 case and appendix in 1 case. A diversity of opative methods were made, encompassing tube cecostomy in 1 case, primary repair with tube cecostomy in 1 case, primary repair in 3 cases, appendectomy in 1 case. No conversion to laparotomy was needed. The time resuming oral feeding was between postoperative day 5 to day 8. For two cases receiving tube cecostomy, constant stool leaking beside the tube predisposed to chronic wound infection and granoloma which required excision. Otherwise, there was no other complication recorded, such as surgical site infection, intestinal obstruction.
Conclusion: Laparscopic approach for acute intestinal perforation secondary to enterocolitis is technically feasible and provides benefits of less complication, better wound outcomes. For cases of solitary intestinal perforation, primary repair can be safely performed through laparoscopy.
INTRAPANCREATIC DUODENAL DUPLICATION: TRANS-DUODENAL LAPAROSCOPIC REMOVAL IN A 18-YEAR-OLD GIRL
Background: Due to the low frequency of duodenal duplications (DD), there are rare case reports of the laparoscopic treatment of such cysts. Although congenital, about 30% are treated in young adults, and are usually misdiagnosed as pancreatic or choledocal cysts before the operation. The authors present the laparoscopic complete resection of a non-communicating DD using 3 ports.
Case Report: An 18-year-old adolescent girl had cronic abdominal pain and recurrent vomiting since the age of 12, variable hyper-amilasemia. Imaging tests and endoscopy now revealed a 6-cm cyst in the area of the pancreas head or distal choledocus, and partial obstruction of the duodenal lumen. Cholangiography discharged choledocal cyst, and showed a light deviation of the choledocus by the cyst. Laparoscopy was performed using 3 ports, transparietal sutures allowed good exposure of the structures. A Kocher maneuver helped evaluate the dorsal area of the duodenum and pancreas. The cyst was completely inside the pancreas along the left duodenal wall. It was carefully dissected and resected using a monopolar cautery and blunt dissection, through a longitudinal duodenotomy at the second segment, where a spheric proeminence could be seen inside the duodenum. The left sided cyst wall had the mucosa removed preserving the outer muscular wall intact. The cyst had a dense, gray, bad smalling and viscous material. After duodenorraphy and drainage, the postoperative (PO) period was uneventfull, the patient had nothing per oral for 3 days, received amikacin and metronidazole, and then was home by the 5th PO day. During the first 4 months the girl had episodic epigastric pain without hyperamilasemia or hyperlipasemia, and resolved medically. Endoscopy by 2 and 8 months PO were normal, showing a slight depression at the site of the cystectomy. Nowadays she is asymptomatic.
Conclusion: Videolaparoscopy is a safe and efficient approach to remove pancreatic duodenal duplications, and the transduodenal dissection allows little if no pancreatic manipulation, reducing the morbidity of the operation.
SUBCUTANEOSCOPIC SURGERY IN CHILDREN: STEALING THE SCAR
Background: Benign neck, axilla and face lesions are traditionally treated through an overlying incision. The resultant scar can be aesthetically displeasing. We report experience of subcutaneoscopic surgery for benign lesions of the neck, axilla and face.
Methods: The study uses a retrospective review of 8 elective subcutaneoscopic procedures from March to October 2012. The lesions included sternocleidomastoid torticollis, external angular dermoid, an enlarged cervical lymph node and BCG axillary adenitis. Outcome measures included need for conversion, cosmetic outcome, and complications.
Results: All procedures were successfully completed using the subcutaneoscopic approach. The distribution of cases and approach is shown in table. Postoperative pain was controlled with acetaminophen, and all patients were discharged from the hospital the same day. There were no intraoperative complications. All families were pleased with the cosmetic results.
Conclusions: A subcutaneoscopic approach can be applied effectively to a variety of benign lesions of the neck, axilla and face, allowing adequate exposure for dissection, and resulting in a quick recovery. Scar is stolen and small scars are well hidden and inconspicuous.
LAPAROSCOPY IN NEONATES IN BANGLADESH: TECHNICAL CHALLENGES AND EXPERIENCE IN CHITTAGONG
ABSTRACT WITHDRAWN
MINIMALLY INVASIVE SURGERY FOR LARGE EXTRA-OVARIAN TERATOMAS WITH A SUBSTANTIAL SOLID COMPONENT: A REPORT OF 3 PEDIATRIC CASES
Introduction: Pediatric patients with large extra-ovarian teratomas with a significant solid component are usually treated by open surgery. Although minimally invasive surgery is increasingly used for ovarian and extra-ovarian teratomas in adults, it is far less commonly used in children, because the intracorporeal cavity is usually too small for manipulating a large tumor. We describe 3 pediatric patients who underwent minimally invasive surgery for large extra-ovarian teratomas with a substantial solid component.
Case 1: An 11-month-old female patient presented with a palpable abdominal mass. Computed tomography revealed a large teratoma (12×7.3×10.8 cm) in the left upper retroperitoneal cavity. The tumor had a large amount of sebaceous material and displaced the vena cava (black arrow) and superior mesenteric artery (white arrow) ventrally (Figure). The alpha-fetoprotein (AFP) level was slightly elevated (17 ng/ml). Laparoscopic surgery was performed using 4 ports. The tumor volume was reduced via intraoperative needle aspiration of the cystic component. The tumor was separated from the large vessels laparoscopically and was then removed via a Pfannenstiel incision. The pathological diagnosis was mature teratoma with a focal immature epithelial element and a negative surgical margin. During careful monitoring for 3 years, chemotherapy has not been required. No recurrence or elevation in the AFP level was noted.

Case 2: In an 8-year-old female patient, calcification was incidentally noted on an abdominal roentgenograph. Computed tomography revealed a large teratoma (9.4×9.1×7.4 cm) in the left upper retroperitoneal cavity that contained multiple cysts and a substantial solid component. The renal artery and vein were displaced to the back and front, respectively, and the aorta was almost completely encased by the tumor. Tumor marker levels were not elevated. Laparoscopic surgery was performed using 4 ports. Intraoperative ultrasonography was used to identify and aspirate the cystic components. The pathological diagnosis was mature teratoma. No recurrence was noted 20 months after the operation.
Case 3: A 3-year-old female patient with persistent cough for 1 month showed an abnormal shadow in the left thoracic cavity on chest radiography. Computed tomography revealed a multi-cystic mass arising from the anterior mediastinum. One of the cysts was particularly large (10 cm in diameter) and protruded into the left thoracic cavity. The left main bronchus was compressed by the tumor. Tumor marker levels were not elevated. Complete thoracoscopic surgery with 4 airtight ports and carbon dioxide insufflation was performed. The largest cyst was punctured through the left thoracic wall and aspirated. The tumor was removed via an extended axillary port site incision. Atelectasis in the left lung after the operation healed with conservative treatment. The pathological diagnosis was mature teratoma. No recurrence was seen after 17 months.
Conclusion: All patients had a good cosmetic result and no long-term complications. Preoperative and intraoperative imaging was effective in revealing major vessel anatomy, which was important for planning surgery. Despite the substantial solid component, intraoperative needle aspiration of the cystic content provided sufficient working space and enabled safe separation of the major vessels from the tumor.
LAPARSCOPIC REPAIR OF INGUINAL HERNIA IN CHILDREN. AN ENDLESS DEBATE
Introduction: Inguinal hernia repair is one of the most frequently performed pediatric surgical operations. Unresolved debate still exists regarding the benefit of using laparoscopy over conventional repair. The aim of this study was to retrospectively analyze the files of all children who underwent inguinal herniotomy, open and laparoscopic, in a single pediatric surgery centre in UAE, and to compare both procedures to conclude which procedure is more feasible.
Patients and Methods: The study was a retrospective study conducted in pediatric surgery department, Al Qassemi hospital, Sharjah, UAE in the period from January 2009 till December 2011. File review was done by independent reviewer for all cases who had inguinal herniotomy being done during this period whether open or laparoscopically.
Results: A total of 320 cases of inguinal herniotomy, 120 laparoscopically (LH) versus 200 open (OH). Mean age for LH was 54 month versus 32 months for OH. In LH 12.5% were bilaterally operated (13 male, 2 female) versus 9% in OH (18 male). Mean operative time in LH (unilateral only) was 24 min versus 19 min in open group. In LH there was one case (0.8%) of internal ring hematoma due to injury to inferior epigastric vessels which was stopped spontaneously, there was no intraoperative complications in the open group. Follow up period ranged from 8 months to 2 years, there was no residual hydrocele in both groups, no recurrences in OH, 1 (0.8%) recurrence in LH group. There was one case (0.5%) of post open herniotomy ascending testis which required orchidopexy.
Conclusion: Our preliminary results for laparoscopic inguinal herniotomy in children above one year show comparable results to open technique in the short term follow up.
Laparoscopic technique is superior in exploring the contralateral side.
We will conduct a prospective study with longer follow up and younger age group to have more accurate validated data.
Keywords: Laparoscopy, inguinal hernia, children.
CLINICAL APPLICATION VALUE OF SUSPENSION WITH SILK THREAD DURING THE PEDIATRIC LAPAROSCOPY
Purpose: The aim of this study was to evaluate the application value of suspension with silk thread during the pediatric laparoscopy.
Methods: Suspension with silk thread was used in many kinds of pediatric laparoscopy in our department: Anderson-Hynes, Ureterolithotomy, Partial Nephrectomy, Plication of Diaphragmatic Eventration, Repair of Paraesophageal Hernia, Repair of Congenital Diaphragmatic Hernia, Cardioplasty, Excision of Choledochal Cyst, Biliary Enteric Anastomosis, Appendectomy, Excision of Ovarian Neoplasms and Intestinal Duplication Operation. The data of operative techniques, operative effect and operation time were summarized and analyzed.
Results: Suspension with silk thread during the pediatric laparoscopy could be used to enlarge the operation space, shorten the operation time, reduce the number of trocars used in operation and raise the operation accuracy so as to overcome the difficulty of small intraperitoneal space in children and make laparoscopy operation much easier.
Conclusions: Suspension with silk thread should be used and generalized in pediatric laparoscopy, which could produce very high applied value in clinical practice.
THROSCOPIC PROCEDURE FOR TUMOR OF MEDIASTINUM
Background/Purpose: Tumors of mediastinum mostly require surgical excision, preferably before the onset of complication. Recently, it has become feasible to accomplish the excision thoracoscopically in children. We herewith reviewed our experience of thoracoscopic excision of mediastinum tumors in children.
Methods: We managed 15 children with mediastinum tumor between July 2006 and November 2012. The mediastinum tumors were excised thoracoscopically. Of the 15 patients, there were 6 girls and 9 boys. The median age was 49 months (range from 11 m to 9 y) All patients underwent computed tomography (CT). The tumors were cystic or solid with a median diameter of 7.9 (range from 5 cm to 12 cm) cm.
Results: The operations were completed successfully in all patients. The operating time ranged from 90 to 220 minutes (median=125 minutes). There was no operative complication and no conversion. The blood loss was minimal. There was no pneumothorax, hydrothorax in our series. The recovery was uneventful and the median hospital stay was 4 (range from 3 to 7) days. No complication was detected at the follow-up visits. The patients were followed up for an median of 39 (range from 6 months to 5 years) months.
Conclusions: Our preliminary results show that throcoscopic excision of mediastinum tumors in children is both feasible and safe. It curtails further complication of the tumors. In addition, the thorocoscopic approach minimizes surgical trauma.
Keywords: Neoplasm; thoracoscope; mediastinum tumor; children; minimally invasive surgery.
TREATMENT OF LAPAROSCOPIC CYST-EXCISION WITH ROUX-Y HEPATOENTEROSTOMY FOR CHOLEDOCHAL CYST
Background: To explore the treatment and complication of prevention in laparoscopic excision of choledochal cyst and Roux-Y hepatoenterostomy of choledochal cyst in children.
Methods: Under the guidance of laparoscope, cholecystography was operated to understand the expansion condition of choledochus, and abnormality of intrahepatic duct and pancreatic duct. Laparoscopic excision of choledochal cyst and Roux-Y hepatoenterostomy were carried out.
Results: Fifty-eight cases of choledochal cyst were examined with B-ultrasound and CT before operation. Fifty-five cases were carried out with laparoscopic excision of choledochal cyst and Roux-Y hepatoenterostomy. Three cases turned to laparotomy because of severe inflammation of cyst wall and much bleeding. Anastomotic leakage appeared in one case after operation, because the drain stabed anastomotic stoma with the child's dysphoria and much unsteady. The case was carried out with laparotomy and anastomosis. Pancreatic leakage appeared in one case after operation, disappeared after being drained 1 month. The operation times were 2.5–6.5 hours. The patients were aged from 4 months to 14 years.
Conclusions: Laparoscopic excision of choledochal cyst and Roux-Y hepatoenterostomy for the treatment of choledochal cyst was effective and safe procedure in children. But the laparotomy must be carried out in heavy inflammation of cyst wall, longer time of operation and the deformation of intrahepatic duct and pancreatic duct. The key is the skilled technique, the cautious procedure and the careful nurse.
LAPAROSCOPIC RESECTION OF RETROPERITONEAL EXTRALOBAR PULMONARY SEQUESTRATION: A CASE REPORT
We herein report a case of retroperitoneal extralobar pulmonary sequestration (EPS) in which laparoscopic resection was successfully performed. At 22 gestational weeks, ultrasound and MRI revealed a subphrenic mass (3 cm in diameter) in the fetal abdomen. The size of the tumor did not change during the gestational period. The baby was born at 38 weeks of gestational age. After birth, a diagnosis of neuroblastoma was ruled out based on the levels of tumor markers in the blood and urine. Due to the lack of growth of the tumor, elective surgery was performed. At two months of age, CT angiography showed multiple feeding arteries arising from the aorta and the celiac artery and a large drainage vein flowing into the portal vein. At eight months of age, laparoscopic surgery was performed under a diagnosis of retroperitoneal EPS. Four trocars and one liver retractor were used. Laparoscopy revealed that the large drainage vein ran across the front of the esophagus from the left to the right and flowed into the portal vein. After dissecting the abdominal esophagus, a vessel loop was placed around the esophagus. The esophagus was drawn out to a ventral position, and the origins of the feeding arteries were identified. After dividing the feeding arteries using a vessel sealing device and hemo-clips, the large drainage vein was divided with a stapler. Finally, the tumor was extirpated successfully without any complications. Performing laparoscopic resection of retroperitoneal EPS is safe and feasible under a precise evaluation of the feeding and drainage vessels obtained with CT angiography.

THE ROLE OF ENDOSURGERY IN TREATMENT OF CHILDREN WITH ONCOLOGICAL DISEASES
Over the past 20 years, mini-invasive access has become the procedure of choice in different fields of pediatric surgery. But, pediatric oncological surgeons still doubt the benefits of endosurgery, especially when discussing operations on little patients with oncological diseases.
The aim of our study was to determine the place for endovideosurgical methods in the treatment of children with different oncological diseases, including patients in severe condition.
Materials and Methods: Our hospital started treating children with oncology in January 2012. Since then we performed 322 operations, 41 of which were endosurgical procedures. The age of patients ranged from 25 days to 19 years old. Of these 41 operations, 32 were laparoscopy (9 biopsies, 16 removals of different neoplasms, and 7 common surgical procedures) and 9 were thoracoscopy (5 biopsies, 4 removals of neoplasms).
There were 3 intraoperative complications. Intraoperative hemorrhages from well-vascularized neoplasms were resolved in 2 cases with endoscopic coagulation and the use of BiClamp (Erbe), and in 1 case a thoracotomy was required to stop the bleeding. There were 6 conversions in total. In 2 cases (abscesses of the abdominal cavity) we conversed to laparotomy due to strong inflammatory changes in the bowel wall caused by long duration of the pyoinflammatory processes with the background of immunosuppression and cytopenia. In 1 case of intususception we started with a laparoscopic diagnostics, but continued with a laparotomy, being under the threat of a bowel rupture because of a marked swelling of the bowel walls. In 1 child, after a transplant of hematopoietic stem cells with the gastrointestinal form of the reaction “graft versus host disease”, the symptoms of “acute abdominal pain” appeared after diagnostic fibrogastroduodenoscopy with the biopsy of mucosa. We found dissecting submucosal hematoma of the duodenum while performing diagnostic laparoscopy, but had to convert to laparotomy, because of the patient's severe condition. And, one thoracoscopic biopsy was converted to thoracotomy because of a failure to localize the tumor node in lung parenchyma.
There were no postoperative complications.
Conclusion: We consider that mini-invasive access can be widely used in children with oncology in spite of severe premorbid conditions, assuming close agreement and cooperation with hematologists, oncologist and anesthesiologists.
MASSIVE PNEUMOPERITONEUM IN A PREMATURE INFANT. IS THERE A ROLE FOR NON-INVASIVE MANAGEMENT?
ABSTRACT WITHDRAWN
IS OPEN SURGERY EXPERIENCE ESSENTIAL FOR LAPAROSCOPIC SURGERY?: LEARNING CURVE FOR LAPAROSCOPIC PYLOROMYOTOMY
Background: Because there are numerous pediatric surgical institutions in Japan, the number of pediatric operations performed in a single institution is quite low. We wished to assess whether experience in open pyloromyotomy (OP) is essential to perform laparoscopic pyloromyotomy (LP) and to determine the number of operative experiences with hypertrophic pyloric stenosis (HPS) required for surgical trainees to pass the learning curve. This report examines our experiences with LP to define the learning curve.
Patients and Methods: We reviewed retrospectively the cases of 81 patients with HPS who underwent LP over 15 years. LP was performed by 7 operators including 3 board-certified instructors (A, B, C), 3 residents of pediatric surgery (D, E, F), and 1 resident of general surgery (G). Cases with intraoperative complications were excluded. Learning curves were assessed according to the operative time (presented by the duration of carbon dioxide insufflation). In addition, each surgeon's experiences in OP, LP assistance, laparoscopic surgery in adults, and laparoscopic appendectomy in children were recorded.
Results: Board-certified instructors (A: 33 cases, B: 30 cases, C: 2 cases): Mean operative time decreased from 30(A)/53.8(B) minutes for the first 5 patients to 25.8(A)/37.4(B) minutes for the next 5 patients, and finally to 14.4(A)*/41.6(B) minutes for the last 5 patients. A definite learning curve was observed in this group, especially for the first 5–10 cases.
Residents of pediatric surgery (D: 4 cases, E: 2 cases F: 1 case): Despite no previous experience in OP, operative time was less in the first case—19(D)/23(E)/12(F) minutes—because of experience in LP assistance, laparoscopic surgery in adults, and laparoscopic appendectomy in children (more than 30 cases). Resident of general surgery (G: 9 cases): Despite no experience in OP or LP assistance, a steep learning curve was observed. Mean operative time decreased from 44.3 minutes for the first 3 patients to 30 minutes for the second 3 patients, and finally to 34 minutes for the last 3 patients. (*: P<0.05).
Conclusion: LP can be performed without any prior experience in OP on the basis of the learning curve and our experience of young residents performing LP. Experience in LP assistance, laparoscopic surgery in adults, and laparoscopic appendectomy in children might be more helpful in performing LP rather than experience in OP.
COMPLETE THORACOSCOPIC VERSUS VIDEO-ASSISTED THORACOSCOPIC RESECTION OF CONGENITAL LUNG LESIONS
Background: Minimally invasive surgery is becoming recognized as a safe and feasible resection technique for congenital lung lesions. In our hospital, video-assisted thoracoscopic surgery (VATS) was initially performed for these lesions through a 4–5 cm incision with the insertion of several trocars under differential lung ventilation (assisted-VATS). In 2009, complete thoracoscopic surgery (complete-VATS) with artificial pneumothorax was introduced, which allowed surgery in smaller infants. The purpose of this study is to compare the outcomes of complete-VATS and assisted-VATS for congenital lung lesions.
Methods: Between January 2004 and October 2012, 22 children underwent pulmonary lobectomy by either complete-VATS or assisted-VATS at our hospital. The intraoperative and early postoperative results of these patients were retrospectively reviewed.
Results: Of the 22 children, 10 underwent assisted-VATS and 12 underwent complete-VATS for congenital cystic adenomatous malformation (CCAM), sequestration, bronchial atresia, lung tumors, or anomalous systemic arterialization of the lung. The age at operation was 53.9±24.8 months (range: 17–96 months) and 64.7±58.7 months (range: 3–163 months) in the assisted-VATS and complete-VATS groups, respectively (P=0.61). Body weight was not significantly different between the two groups (15.6±4.0 kg vs 22.1±16.3 kg, P=0.26). Still, four patients in the complete-VATS group, but none in the assisted-VATS group, weighed <10 kg, indicating that complete-VATS is feasible for smaller children. The mean operative time was longer, although not significantly, in the complete-VATS group (247±81.7 min vs 188.3±41.1 min, P=0.06). Intraoperative bleeding was significantly less (45.2±56.1 g vs. 150.7±153.2 g, P=0.047) and hospital stay was significantly shorter (5.8±2.0 days vs 9.0±2.4 days, P=0.0043) in the complete-VATS group than in the assisted-VATS group. One patient with CCAM in the assisted-VATS group with intraoperative bleeding required conversion to open surgery; no conversions were required in the complete-VATS group. Postoperative complications included transient paralysis of the affected arm caused by intraoperative compression of the brachial plexus and transient atelactasis in one patient each in the complete-VATS group.
Conclusion: Complete-VATS can be safely performed with less bleeding and shorter hospital stay than assisted-VATS. Since differential lung ventilation is not necessary in complete-VATS, it can also be performed in small infants. Recent developments in vessel sealing systems and autosuture devices may allow for shorter operations using complete-VATS, supporting its use in the near future.
LAPAROSCOPIC SPLENOPEXY INTO THE PREPERITONEAL SPACE AS TREATMENT FOR “WANDERING” SPLEEN
Purpose: To demonstrate laparoscopic splenopexy into the preperitoneal space as a treatment option for wandering spleen.
Methods: The patient is a 12-year-old male with a past medical history significant for myelomeningocele repair, VP shunt, vesicoureteral reflux, and neurogenic bladder. During his genitourinary surveillance he had been found to have an incidental finding of wandering spleen. This correlated clinically to intermittent episodes of abdominal pain related to intermittent torsion of the spleen and ischemia.
A bump was placed on his left side. A 10-mm port was placed at the umbilicus using the open Hasson technique. Under direct visualization, a 5-mm port was placed in the left midclavicular line and another 5-mm port in the midline cephalad to the umbilicus. On inspection the spleen did look somewhat atypical probably due to intermittent ischemia from torsion of the hilum. It was completely unattached to either the diaphragm, the lateral peritoneal wall, or the kidney.
The left lateral abdominal wall and peritoneum were identified, and a peritoneotomy was created via electrocautery and extended with electrified scissors. Blunt dissection was used to expand this pre-peritoneal cavity. The spleen was mobilized and subsequently implanted into the extraperitoneal space. The peritoneotomy was closed with an endo-stitch using Tycron sutures (Closure can also be performed in an intracorporeal fasion using 2-0 interrupted silks).
Results: He did well post-operatively. He was subsequently discharged on post-operative day one, tolerating a general diet. He had no post-operative complications. Three years later, during a workup for pyelonephritis, CT imaging demonstrated splenic viability.
Conclusions: Laproscopic extraperitonealization of the spleen is technically feasible and safe in the pediatric population.
MULTIMODAL APPROACH TO TREATMENT OF A RECURRENT H-TYPE TRACHEOESOPHAGEAL FISTULA IN AN INFANT
Objective: To highlight a multimodal approach using endoscopy and exoscopy in management of an infant with a recurrent H-type tracheoesophageal fistula (TEF).
Synopsis: A 7-month-old boy was referred to us after two attempted closures of a TEF. We evaluated the patient and confirmed that he had an H-type TEF at the C7-T1 level. We initially attempted an endoscopic repair with combined fistula de-epithelialization and fibrin glue that failed early. We then chose a multimodal strategy combining endoscopic localization of the fistula with the VITOM® high-definition exoscope for magnification and enhanced visualization of critical structures. We used a low right cervical approach to achieve adequate exposure of the fistula. The boundaries of the fistula were clearly identified and the fistula was divided. Both trachea and esophagus were closed with interrupted sutures and then the incision closed. The patient had a successful recovery with no residual TEF.
Conclusion: Along with traditional endoscopy, the VITOM® was a critical component of the multimodal strategy used in this complex case, and also provided superb documentation of this unusual clinical situation for future teaching purposes.
THE APPLICATION OF ENDOSCOPIC STERNOCLEIDOMASTOID AMPUTATION IN TORTICOLLIS OF CHILDREN
Objective: To discuss the clinical application of sternocleidomastoid amputation with endoscopy in the treatment of muscular torticollis.
Methods: A total of 7 children with muscular torticollis had been treated from July 2008 to May 2012. The age ranged from 14 months to 6 years. A 5 mm trocar was inserted in the anterior axillary fold. Established a subcutaneous space with CO2 in pressure of 6 mmHg. Blunt dissected a subcutaneous tunnel towards the cervical region with a 5 mm endoscope lens. Another two 3 mm incisions parallel to neck transverse striation were made for the introduction of a 3 mm electric hook and a 3 mm curved forceps. Enlarge the subcutaneous space big enough to carry out the operation. The stemocleidomastoid muscle and tight fibrous tissue were dissected out and cut off with Electrocoagulation until the omohyoid muscle was exposed clearly.
Results: All the 7 operations were successfully completed. The mean operation time was 70 min (ranged from 50∼130 min). No major blood vessel and nerve were injured. Follow-up for 6 months to 2 years showed that neck movement, head tilt, facial asymmetry were greatly improved after operation and cervical scars were almost invisible.
Conclusions: Sternocleidomastoid amputation with endoscopy in the treatment of muscular torticollis has sure efficacy and good cosmetic effect.
LAPAROSCOPIC REINSERTION OF PERITONEAL DIALYSIS CATHETERS
Purpose: Peritoneal dialysis (PD) is the preferred long-term dialysis modality in the pediatric population but removal followed by reinsertion at a later time is often performed for complications such as infection, malfunction, or in cases of failed kidney transplantation. We sought to evaluate the feasibility and outcomes of laparoscopic reinsertion of PD catheters.
Methods: An IRB-approved retrospective review of patients undergoing laparoscopic PD catheter reinsertions at a single center from 2007–2012 was performed. The following variables were assessed: reason for removal of original PD catheter, concomitant operations performed, duration of surgery, and hospital stay. Catheter failure was defined as reoperation for infection or malfunction. Survival analysis was performed to account for differences in follow up period and time to resolution of renal failure (either spontaneous or due to renal transplantation). Analysis time was months until reoperation or first censored event (e.g. renal transplantation or last follow up).
Results: Ten patients with median age 12 years (range 0–20) and median weight 43 kg (range 7–92) underwent laparoscopic PD catheter reinsertions. One of these patients had a prior catheter reinsertion which was converted from a laparoscopic to open procedure to facilitate performing a concurrent gastrostomy. No other conversions were required during the time period. The reasons for prior catheter removal were infection in 5 (50%); malfunction in 4 (40%); and failed transplant in 1 (10%). The median time interval between removal of old PD catheter and reinsertion was 5 months (range 0 to 154). Eight (80%) patients had prior open abdominal operations. Five patients (50%) were noted to have significant adhesions. Concomitant operations were performed in 7 (70%) patients: 3 omentectomies, 2 hemodialysis catheters, 1 inguinal hernia repair, and 1 ventral hernia repair. Median time from incision to closure was 1.3 hours (range 1.0–4.3). Median hospital stay was 6 days (range 1–23). Mean follow up for patients undergoing successful laparoscopic PD catheter reinsertion was 33 months (range 3–52). Three (30%) patients have developed at least one episode of peritonitis, but they were successfully managed with antibiotics and have not yet required catheter removal. One patient required removal for malfunction at 3 months. Four patients had removal at time of transplantation at median 8 months (range 2–21). The current catheter lifespan for the remaining five catheters is 11 months (range 3–37). The hazard rate for catheter failure was 0.94 events per 100 catheter-months.
Conclusions: Laparoscopic reinsertion of PD catheters is feasible with excellent outcomes even in the setting of prior open abdominal procedures, history of peritonitis, and significant intraabdominal adhesions. Laparoscopy offers the potential benefits of improved visualization and cosmesis as well as decreased morbidity and length of stay.
AN INANIMATE MODEL FOR TRAINING TORACOSCOPIC REPAIR OF TEF/ESOPHAGEAL ATRESIA
Aim: Present the evolution of a model developed for specific training in toracoscopic repair of TEF/Esophageal atresia.
Materials and Methods: The video starts showing the view of a complete repair using the final version of the model done with a 4 mm lens, 3 mm instruments, 6/0 sutures and an HD camera. The procedure is being done by a postresidency fellow trained in open surgery who has never participated in a MIS TEF assisted by a senior MIS surgeon after being trained in basic inanimate models (Pediatric FLS) and practising endoscopic suturing for 144 hours. Exercises consisted in dividing and suturing the fistula and doing an esophageal anastomosis with a transanastomotic tube. Extracorporeal and intracorporeal sliding knot tying were used.
Aspects of the same model using 5 mm instruments, 5/0 sutures and a 10 mm lens inside the pediatric FLS trainer follows. This was the previous environment that we have used.
Finally the domestic materials utilized are shown. We started with tubular balloons of 2 different colours to simulate the esophageal mucosal layer and a bent piece of plastic corrugated tube (PVC) for the traqueal simulation, always reproducing the view in an almost prone position. A small piece of wood was used as a support and half of a larger plastic corrugated tube as a toracic posterior wall resembling ribs and intercostal spaces. A white plastic ribbon as the vagus nerve and, a half inflated round balloon as the lung were added and everything covered with an auto adhesive film as pleura. At the beginning we used it inside the Pediatric FLS trainer which was replaced by a plastic toy pink suitcase which can be perforated in the upper surface, making it easily portable.
Results: A pediatric surgeon with little experience in MIS and none in neonatal MIS was able to complete a TEF/Esophageal atresia repair in the final version of the model in 70 minutes assisted by an experienced MIS surgeon. Cost of the matherials was less than 50 US$.
Discussion: A reproducible unexpensive inanimate model has been developed as an additional tool to facilitate the learning curve for MIS TEF surgery. Future validation is needed.
SINGLE TROCAR LAPAROSCOPIC-ASSISTED SURGERY FOR BENIGN OVARIAN CYSTIC TUMOR IN CHILDREN
Introduction: Management of benign ovarian cystic tumor (BOCT) in children by laparoscopic surgery has become popular but mainly by conventional 3-trocars technique. The aim of this study is to investigate the feasibility, safety and effectiveness of single trocar laparoscopic-assisted surgery (STLAS) for BOCT in children.
Methods: Medical records of patients with diagnosis BOCT undergoing STLAS at our center from February, 2009 to October, 2012 were reviewed. For the STLAS, a 10 mm umbilical trocar was placed and a 10 mm camera with engrafted 5 mm working channel was used. The ovarian cystic wall was grasped and brought to the umbilical site and then the cystic fluid was aspirated outside the peritoneal cavity. After maximal decreasing of the cystic volume, the cyst was brought out of abdomen via the umbilical incision (with or without minimal enlargement) and excision of the cyst was performed extracorporally, sparing ovarian tissue when possible. In case of short adnexal pedicle, making delivery of the cyst to the umbilical site impossible, aspiration of the cyst was performed by needle puncture through the abdominal wall under the laparoscopic control. The cyst then was delivered out of the abdomen via a minimal transversal suprapubic incision and cystic removal was performed as described.
Results: 18 patients were identified, with median age of 3 years (ranged from 8 days to 15 years). Three cases were diagnosed prenatally by ultrasound. The median size of the cyst was 7.0 cm (ranged from 3 cm to 11 cm). In eight cases the cyst was mature teratoma, in 6 – folicular cyst and in 4 – dermoid cyst. In 14 patients the cyst was excised via the umbilical incision and in 4-via the suprapubic incision. Ovary sparing was achieved in 15 cases (83.3%). The mean operative time was 45.5±16.5 minutes (ranged 15–90 minutes). There was no intra- or postoperative complication. The mean postoperative hospital stay was 1.8±0.6 days (ranged 1–3 days). For the follow up from 1–36 months, all patients were in good health, without recurrence. The postoperative cosmesis was excellent.
Conclusions: STLAS is highly feasible, safe, effective, with excellent cosmesis and could be a viable approach in minimally invasive management of BOCT in children.
CONTINUOUS TYPE SPLENOGONADAL FUSION: WHAT MORE SHOULD YOU EXPECT?
Background and Aim: Splenogonadal fusion is a very rare congenital anomaly and usually found incidentaly during inguinal hernia repair, or during exploration for undescended testis or testicular mass. It has two subtypes; continuous and non-continuous, and continuous type usually seen with other anomalies. We present a continuous splenogonadal fusion case incidentaly found during indirect hernia repair, further exploration with laparoscopy revealed isolated polysplenia as the origin of continuous type splenogonadal fusion.
Case Report: 7-year-old boy admitted to our clinic with left groin bulging lasting for 3 years. The diagnosis was left indirect inguinal hernia, and elective repair was planned. During inguinal hernia repair, a fibrous cord like structure was discovered in hernia sac, running from intraabdominal cavity and attaching to the upper pole of the testes. Exploration revealed a round structure fused to the upper pole which was clearly different from testicle. This structure was excised with preserving testicle. Since a cord like structure entering the abdomen through the hernia sac, we decided to proceed with diagnostic laparoscopy as in contralateral hernia sac investigation. We inserted a 5-mm laparoscopy port through left hernia sac and laparoscopic exploration revealed polysplenia as the origin of continuous splenogonadal fusion. An additional 5-mm port was inserted suprapubicaly, and extensive splenic tissue and cord like structure was excised with bipolar cautery. He was fed 2 hours after operation and discharged home on same day. Detailed post-operative examination conducted 1-week after operation showed no additional anomaly.
Conclusion: Although splenogonadal fusion is a rare anomaly, its subtypes, associated anomalies, and its treatment are well known. In our case, proceeding with laparoscopy was made possible the diagnosis of accompanying polysplenia and proximal excision of the excess cord like tissue which may cause future intraabdominal complications. This simple case demonstrates the readiness of laparoscopic instruments and laparoscopy as an integral part of operating room is very useful to manage such unexpected cases in clinics which their laparoscopy experience is still evolving.
ALTERNATIVE TIMING FOR HERNIA SAC HIGH LIGATION? - A RETROSPECTIVE CLINICAL STUDY OF 1017 CASES OF INGUINAL HERNIA IN MALE INFANTS AND CHILDREN
Objective: Firstly, to compare the effect and complication of laparoscopic hernia sac high ligation and open procedure in infants and children with inguinal hernia, Secondly, to explore the suitable age of the patient to accept the surgical treatment, from the sight of testis development.
Materials and Methods: Clinical data of 1017 cases of inguinal hernia in male infants and children, including the evaluation of the volume and blood supply of the testis post the operation, were analyzed retrospectively.
Results:
(1) The occurrence rate of pediatric inguinal hernia merge incarcerated is related with age factors (=15.834, P=0.004), of which 6–12 months old is the highest (see Tables 1 and 2). (2) The comparison of the evaluation of the volume and blood supply of the testis pre- and post-operation. (3) General comparison of the effect and complication of laparoscopic hernia sac high ligation and open procedure.
The Age Distribution and the Incidence of Incarcerated Hernia
Conclusions: Laparoscopic hernia sac high ligation treatment for pediatric inguinal hernia is safe and effective, and has more advantages than the traditional open hernia sac high ligation.
The incidence rate of incarcerated inguinal hernia of infants and children is age-related, which is highest in the 6–12 month old infants, indicating an earlier surgical treatment should be considered, instead of waiting until older than 12 months.
The evaluation of the volume and blood supply of the testis supports the appointment mentioned above.
In general, we advocate the use of laparoscopic hernia sac high ligation surgery in earlier age, preferably at 6–12 month old.
Key words: inguinal hernia; laparoscopic surgery; surgical age; testis; children.
Background: Paraovarian cysts account for under 10% of all adnexal cysts and are even rarer in adolescent girls. They are normally asymptomatic but may present acutely as lower abdominal pain due to haemorrhage, rupture or torsion. Large cysts have a high risk of torsion, which can involve local structures including the ovary. Prompt intervention may preserve function and fertility. Unlike ovarian cysts, the risk of malignancy in paraovarian cysts is extremely low.
Case Reports and Procedures: We present videos of two cases of torted paraovarian cysts.
Both patients recovered well and were discharged the day following surgery.
Discussion: Paraovarian cysts rarely resolve spontaneously and have a high risk of torsion. When presenting acutely, ultrasonography is of limited value, as distinction from ovarian lesions is difficult. Laparoscopy is useful in both diagnosis and therapy. As malignancy is very rare, laparoscopic decompression and detorsion is safe and effective and enables preservation of ovaries.
OVARIAN SPARING LAPAROSCOPIC TERATOMA EXCISION
Background: Solid ovarian tumors are uncommon in childhood. Diagnosis is based on clinical features (age and hormonal status), imaging and tumor markers. Complete tumor resection is mandatory, but for benign lesions, healthy ovarian tissue must be preserved, while tumor spillage must be avoided. The role of laparoscopy to manage pediatric solid ovarian tumors is controversial.
Aim: This video describes a technique that combines the advantages of laparoscopy to remove a benign, solid pediatric ovarian tumor, while preserving healthy ovarian tissue and avoiding tumor spillage.
Case Report: A five-year-old female presented with a 2-month history of right lower quadrant pain but no palpable mass. She had no signs of premature menarche or virilization to suggest hormonal activity. Serum tumor markers were negative. Abdominal ultrasound and MRI revealed a 3 cm calcified solid mass in the right ovary. We suspected a benign teratoma.
The patient was brought to the operating room. Under general anesthesia, she was positioned supine, in reverse Trendelenburg. The surgeon stood on the patient's left. The assistant stood on the patient's right and operated the camera. The monitor was at the foot of the bed. A 5 mm port was inserted at the umbilicus and pneumoperitoneum was obtained to pressure of 10 mmHg. A 5 mm 30-degree camera was placed through the umbilical port. A 5 mm port was inserted in the left lower quadrant and a 12 mm port was inserted in the supra-pubic skin crease for optimal triangulation.
The peritoneum around the right adnexa was incised with the Maryland dissector and a laparoscopic Debakey grasper. The blood supply to the ovary was not disturbed. It was mobilized, enclosed in an endobag and brought out through the 12 mm port site. The risk of tumor spillage was avoided.
The mass was separated from the normal ovarian tissue by hydro-dissection technique. A 30-gage needle was inserted under the ovarian visceral peritoneum and saline was injected slowly. A plane developed between the ovary and the peritoneum, as well as between the normal ovary and the mass. The peritoneum was circumferentially incised. Peanut dissection easily separated the mass from the normal ovarian tissue and it was removed intact. The ovary was then reconstructed by approximating the edges of the ovarian cortex with fine absorbable suture.
Ovarian attachments, the fallopian tube and blood supply were not disturbed. The structures were returned to the abdominal cavity. The left ovary appeared normal. No abnormalities were noted in the abdominal cavity. The abdomen was desufflated, the ports were removed and port sites were closed with absorbable suture. The pathologist confirmed a benign 3 cm teratoma, completely removed and intact.
Results: The operating time was 75 minutes. The patient was discharged on postoperative day 1 without complications. At follow-up evaluation, she is asymptomatic.
Conclusion: For pediatric patients with small solid ovarian tumors, and negative tumor markers, this video technique combines the advantages of laparoscopy with the principles of complete tumor removal, preservation of normal ovary and avoidance of tumor spillage.
COMPARISON OF HOSPITAL PROFITS OF THE TREATMENT OF ACUTE APPENDICITIS AT PEDIATRIC SURGERY AND GENERAL SURGERY DEPARTMENTS IN JAPANESE HOSPITALS
Background and Aim: Appendicitis is one of the most common pediatric conditions. Many children are treated by general surgeons, especially in Japan. The aim of this study was to compare the profits collected after performing appendectomies at the pediatric surgery and general surgery departments of hospitals.
Materials and Methods: Data were gathered from two hospitals. Hospital A is a private hospital with a pediatric surgery department and is located in an urban area. Hospital B is a public hospital in Japan without any pediatric surgeon. The Japanese medical insurance system was revised in April 2012. Patients' data were collected from April 2012 to October 2012. All patients underwent laparoscopic appendectomy. We calculated treatment outcomes on the basis of age, perforation rates, hospitalization duration, and hospital profits.
Medical Insurance: The entire Japanese population is covered under the same social medical insurance. This insurance system is revised every 2 years. The hospital income is determined by a system called Diagnosis Procedure Combination System. In this system, the treatment cost is determined by the diagnosis and duration of hospitalization. In pediatric cases, special charges, including pediatric hospitalization management charges are added. Hospitals are divided into five ranks according to the number of pediatric physicians and surgeons working at the hospital, the number of inpatients, and the number of surgeries performed, etc. Hospital A was classified into rank I and $ 344 was added every day for each child. On the other hand, Hospital B was classified into rank IV and $ 156 was added.
Results: During the study period, 34 children (20 boys and 14 girls) were operated at Hospital A and six (5 boys and 1 girl) were operated at Hospital B. There was no significant difference in the duration of hospitalization (5.7 days vs. 5.2 days in Hospitals A & B, respectively; P=0.66) and for perforation rates (29% vs. 33%; P=0.85). The patients were younger in Hospital A than in Hospital B (8.9 years vs. 13.1 years, P=0.01), and the profits were higher in Hospital A than in Hospital B ($9925 vs. $7547, P=0.01).
Conclusion: The severity of appendicitis was considered equal in both groups because there were no significant differences in the duration of hospitalization and perforation rates. However, the facility with a pediatric surgery department earned more. Therefore, financial differences mainly resulted from different management charge according to the Japanese insurance system.
LAPAROSCOPIC PEDIATRIC SURGERY IN THIRD WORLD COUNTRY; ARE WE READY TO ACCEPT THE CHALLENGE?
There is a growing trend towards laparoscopic surgery in children in the world. It is an established fact that laparoscopic surgery offers better results with shorter hospital stay and fewer complications. However, it involves more expenditure. But, in our country, its acceptance is poor. We are sharing our results of laparoscopic pediatric surgery which we have started recently in our hospital, by a same surgeon after completing specialized fellowship training in Pediatric Laparoscopic Surgery.
Objectives: The objectives are twofold. To see the results of laparoscopic surgery in children and to see the family's preference.
Materials and Methods: It's a five years audit conducted in Aga Khan University hospital. This is the largest tertiary care private hospital in the cosmopolitan city of Karachi, Pakistan. A Performa was designed and filled after reviewing the medical records, interviewing patients in clinics and telephonic survey. Data was entered in SPSS version 17. Categorical variables were analyzed by Chi square test and numerical variable by T – test.
Results: A total of 24 laparoscopic procedures were performed including laparoscopic appendectomies, laparoscopic cholecystectomies, laparoscopic orchidopexies, laparoscopic diaphragmatic hernia and laparoscopic repositioning of ovaries. We have found significant difference between the numbers of surgeries done laparoscopically and open surgery. The wound complications are less and the hospital stay is shorter. However the total expenditure is more. There is no statistical difference between the outcomes of both approaches.
Conclusion: Laparoscopic pediatric surgery is at a steady rise in our country but still there are some limitations in accepting the role of laparoscopic pediatric surgery. The orthodox surgeons don't want to change. The parents showed a clear preference towards laparoscopic surgery. There is a dire need to realize that minimal invasive surgery will be the future. Trainees must be oriented with the minimal invasive techniques.
MINIMAL ACCESS ANTERIOR SPINE SURGERY FOR CONGENITAL MALFORMATIVE SPINAL DISORDERS
Congenital malformative spine disorders can be addressed through a combined anterior and posterior approach or through a single anterior or posterior approach. Thoracoscopy and retroperitoneoscopy are now considered safe and feasible for addressing spinal disorders even in patients with a weight of less than 20 kg.
We present a consecutive series of seven patients, six of whom underwent a thoracoscopy and one a thoracoscopy and a retroperitoneoscopy. Six patients had congenital malformative scoliosis due to single or multiple hemivertebrae, one had kyphosis with saggital instability due to L1 hypoplasia. Mean age at surgery was 3 years 2 months (1y 3m-9y 3m), mean weight at surgery was 15,4 kg (11–30). Lung exclusion time averaged 157 min (90–266), operating time averaged 184 min (130–303). There was no intraoperative respiratory complication or conversion to open surgery. Procedures were six thoracic hemivertebrectomies, one lumbar hemivertebrectomy and one T12-L1 fibular graft. All patients had a posterior procedure during the same anesthesia. Mean blood loss was 351 ml (174–742). One patient had a secondary concave chest wall thoracostomy and rib to rib VEPTR. For patients with congenital scoliosis, average improvement of the main curve between preoperative and latest follow-up was 58% with an average Cobb angle improvement of 25° (9–42). For the kyphosis case, stability was obtained with a reduction of the regional kyphosis of 6°.
Congenital spine disorders in small children can be addressed by minimal access anterior surgery with results comparable to open surgery.
INTERVAL APPENDICECTOMY FOLLOWING APPENDIX MASS
Background: Appendix mass can be successfully managed with initial conservative treatment followed by interval appendicectomy. However recent publications have questioned the need for elective appendicectomy on the basis that around 80% of cases do not suffer further symptoms.
Aims: To ascertain the performance of all cases of an appendix mass managed by interval laparoscopic appendicectomy by a single surgeon over a 7 year period. To assess the risk and outcomes of this strategy.
Methods: All interval appendicectomies between 2005 and 2012 were prospectively entered into a database which documented the operative and post operative course. This was combined with a case notes review to record the initial management and readmissions prior to surgery. In addition the histology of all cases was reviewed.
Results: 13 patients 9 female, between 2 ½ & 16 years old underwent an interval laparoscopic appendicectomy during the period of study. The operative time was 43 mins (s.d.13.9) and endo-loops were used in all cases, 2 operations were performed via a single incision laparoscopic technique and the remainder by standard 3 port technique. At surgery the appendices were macroscopically normal in 2, inflamed in 5, thickened in 4, perforated in 2 and 1 was fibrosed. Adhesions were present in 10 cases and a mass had persisted in 3. Postoperatively all patients received paracetamol and NSAIDs none required opioid analgesia. Following surgery the average time to full feed was just over 7 hours, nearly half (5/13) were discharged the same day the remainder stayed in hospital for a single night.
Preoperatively 4 patients were admitted (for 10 days total) with abdominal pain during the wait for interval appendicectomy. The stay at initial presentation was 5.38 d (s.d. 2.75). The interval to surgery was 3 ½ months (103 d (s.d. 84.7)). 2 patients were readmitted in the postoperative period, 1 with self limiting vomiting and one with chest pain. Histology revealed inflammation in 5 cases, pinworms in 2 cases, an obliterated lumen in 2 cases and no suppurative inflammation in 3 though pus was seen in the lumen of one of these.
Conclusions: One third of our patients had symptoms necessitating admission prior to interval appendicectomy; this represents a significant ongoing morbidity following conservative treatment of an appendix mass. Interval appendicectomy was uncomplicated, with short post operative stays, without requirement for opioid analgesia. No patients suffered long term symptoms post appendicectomy. Macroscopically or histologically there was evidence of ongoing inflammation in most of the patients, which may have led to ongoing morbidity had appendicectomy not been undertaken.
SAFETY AND EFFICACY LAPAROSCOPIC BIOPSY FOR PATIENTS WITH NEUROBLASTOMA
Background: Pathological and biological conformation is an essential procedure for diagnosis and treatment of neuroblastoma. In the era of minimally invasive surgery, it has been becoming popular to use laparoscopic technique for biopsy and treatment for the malignant disease. We reviewed the 35 laparoscopic biopsies for neuroblastoma patients in our two hospitals for 14 years to discuss the safety and efficacy of this procedure.
Materials and Methods: We reviewed the charts of patients with neuroblastoma from November 1998 to September 2011. The patients who underwent laparoscopic biopsy were enrolled. The collected data were patients' clinical courses, characters such as age, sex, body weight, and surgical status such as operative time, blood loss, complications.
Results: Thirty-five patients were enrolled. Median and average age were 8 months and 22.1 months. Median and average weight were 9.2 kg and 11.0 kg. Male to female ratio was 22:13. The average operation time—other procedures such as insertion of central venous catheter and bone marrow aspiration were included in some patients—was 110 minutes.
In twenty-eight of 35 patients the blood loss during the operation was less than 1% amount of body weight. Three patients lost 1.5 to 2 %, and the other three patients lost 3.2%, 7.4% and 22.5%, respectively. We converted to an open surgery in one patient to control the bleeding. One patient had postoperative hemorrhage and a blood transfusion was needed. Two patients died within 1 week after their operations. One had preoperative tumor rupture and deteriorated postoperative condition due to massive bleeding. The other lost blood in only 0.8% of body weight, but died of the disease progression itself.
Most patients started oral intake in 2 days. It took 5 days on average to start the chemotherapy after the operation; the mode was 2 days though. All procedures were productive for the pathological and biological diagnosis. No port recurrences were observed.
Discussion: Our experience suggests that most laparoscopic biopsies for neuroblastoma are performed safely, and productive for the pathological and biological diagnosis. But we should think that bleeding in laparoscopic biopsy is the most important concern and a possible lethal complication. We avoid the laparoscopic biopsy when we observe preoperative tumor rupture or massive intra-tumor hemorrhage, now.
The minimally invasive procedure can shorten time to recover from the surgery. When the open surgery would be performed as a radical excision after chemotherapy, the best incision area for laparotomy could be decided independently of small biopsy wounds. In some cases, we only apply chemotherapy to the patients for treatment after the biopsy. The laparoscopic biopsy also has a possible advantage regarding cosmetic issue for both chemotherapy-only patients and radical-operation patients.
SOFT COAG MODE IS EFFICIENT IN COAGULATING THE RESIDUAL INNER LAYER OF LARGE SPLENIC CYST AFTER LAPAROSCOPIC DOME RESECTION
Background: Symptomatic large splenic cyst is a rare disease and evidence-based treatment guidelines are not available. Laparoscopic splenectomy is one of the treatment options, but total splenectomy may cause severe postoperative infection and thrombocytosis, and is not recommended for pediatric patients. Therefore, a spleen-preserving treatment strategy is recommended, although high recurrence rates have been reported in the literature. In order to prevent recurrence, the free part of the splenic cyst must be resected as much as possible (dome resection) and the residual inner layer of the cyst should be coagulated by electronic cautery or an argon beam coagulator (ABC). When applying these devices, tissue damage is caused to some extent, the coagulated tissue may fall off later and cause postoperative bleeding, and the high pressure of ABC on the vessels may result in a severe complication, gas embolism. The newly developed electrosurgical generator, the VIO300D (ERBE Elektromedizin GmbH, Germany), has a unique coagulation output mode called “SOFT COAG”, that automatically regulates its output voltage to keep it below 200 volts (V), and does not cause tissue carbonization. Proteins within the target tissue are effectively coagulated at temperatures of between 70 and 80OC by the regulated energy. Here, we present a pediatric patient with a large splenic cyst that was managed by laparoscopic dome resection followed by coagulation of the residual inner layer of the cyst with the “SOFT COAG” mode.
Case Report: The patient was a 12-year-old girl. Her chief complaint was prolonged vomiting. Ultrasonography of the abdomen revealed a 7 cm cystic mass at the left upper abdomen. Abdominal computed tomogram demonstrated that the cyst was a large splenic cyst at the lower part of the spleen. Prolonged vomiting was due to this lesion, and laparoscopic dome resection and coagulation of the residual inner layer were performed. First, intracystic fluid was partly suctioned using a SAND balloon®. Then, the cyst wall was excised with an ultrasonic coagulating device. There was little hemorrhage from the cyst wall. Finally, we used the “SOFT COAG” mode to coagulate the residual inner epithelium of the splenic cyst wall. The pathological diagnosis was a true cyst and the ablated site of the cyst wall that had been taken at the operation showed degenerative or necrotic change at the epithelial cell layer only. There has been no relapse one year after the operation.
Conclusions: A 12-year-old girl with giant splenic cyst underwent laparoscopic dome resection and ablation of the residual epithelium of the cyst wall using the “SOFT COAG” mode. In the “SOFT COAG” mode, one can set the electrocoagulation depth; therefore, it is capable of cauterizing only the cystic epithelial cell layer without injury of the adjacent vessel and deep splenic tissue. This is a preliminary report, and the safety and efficacy of the “SOFT COAG” mode for coagulation of the epithelium of the splenic cyst must be studied in a greater number of patients with long-term follow-up.
THE ROLE OF LAPAROSCOPY IN DIAGNOSIS AND TREATMENT OF ABDOMINAL PSEUDOTUMORS IN CHILDREN
Malignant tumors should always be included in differential diagnosis of any solid mass detected in imaging studies in children. Diagnostic difficulties may be encountered especially in patients in whom there is no good correlation between clinical signs and symptoms and results of imaging studies. In such patients minimally invasive surgery may play a very useful role not only as diagnostic modality but a therapeutic tool as well.
The aim of the study was to present the role of laparoscopy in diagnosis and treatment of abdominal mass in children.
Between 2009 and 2012 in our department we diagnosed and treated 10 children with abdominal mass which were found in imaging studies during prenatal or postnatal period. Results of ultrasound and CT studies showed lesions that potentially could be malignant. However, other signs and symptoms led to different final diagnosis. Due to discrepancy between results of imaging studies and clinical signs and symptoms, explorative laparoscopy as a final diagnostic tool was undertaken.
In all operated cases abdominal mass was found and whole abdominal cavity was inspected. In 3 cases conversion to open surgery was necessary due to technical difficulties during the procedure while in other cases laparoscopy proved to be a useful tool for resection of the mass. Even in converted cases laparoscopy was helpful to choose the most appropriate abdominal wall incision.
Histopatological examination of resected masses revealed diaphragmatic cyst, choriostoma, extralobar pulmonary sequester, enlarged lymph nodes, lymphangiomas, ovarian cyst, twisted and detached ovary.
Laparoscopy is a safe and very useful method of diagnosis and treatment of abdominal masses.
THE EFFICACY OF LAPAROSCOPIC ASSISTED CONTINUOUS AMBULATORY PERITONEAL DIALYSIS CATHETER INSERTION
Background: Although laparoscopic treatments for continuous ambulatory peritoneal dialysis (CAPD) catheter-related complications have been reported, we are performing laparoscopic assisted CAPD catheter insertion (LAPD) for reducing postoperative complications such as migration or occlusion of the catheter and the occurrence of communicating hydrocele. Our operative technique and the efficacy of LAPD are presented.
Methods: We experienced 37 cases of LAPD for the patients with chronic or end-stage renal failure, or the pre/postoperative condition of kidney transplantation, during the period from 2006 to 2012. The average age of our patients was 10.3 years old, with a range from 11 months to 27 years old.
Operative Technique: (1) Three ports (supraumbilical 5 mm scope port, 5 mm working port at the position of the inner cuff in right rectus muscle, 5 mm working port at left upper abdomen). (2) Minimal omentectomy, if necessary. (3) Removal of working port at the place of the inner cuff and extending the incision to 2 cm in length. (4) Fixation of the inner cuff to the peritoneum, and positioning the inner cuff and catheter in rectus tunnel. (5) Under direct vision, leading the tip of catheter to the Douglas' pouch with locating behind sigmoid colon and sigmoid mesocolon. (7) The operation for persistent of internal ring by inguinal approach, if necessary.
Results: In 25 cases, we performed additional operations such as minimal omentectomy, inguinal hernioplasty, peritoneum biopsy, and adhesiolysis at the same time of LAPD. Although we experienced postoperative complications such as migration or occlusion of the catheter and the occurrence of communicating hydrocele in the early 10 cases, no postoperative complications occured after modification of operative method.
Conclusion: Our current operative procedure of LAPD led to reduction of catheter-related complications after CAPD catheter insertion, and we think that the fixation of the tip of catheter is not needed.
A NOVEL LAPAROSCOPIC-ASSISTED APPROACH TO THE REPAIR OF PEDIATRIC FEMORAL HERNIAS
Background: Femoral hernias in young children are relatively rare and can be difficult to diagnose as they are often mistaken for inguinal hernias. While a few reports have described laparoscopic techniques, most traditional repair methods still focus on an open approach using either an inguinal or crural incision. In this paper, we describe a laparoscopic-assisted technique which is buttressed by a small cigarette of mesh for the repair this uncommon pediatric entity.
Methods: A 5-mm, 30-degree laparoscope is placed in the umbilicus to visualize the femoral hernia. Transillumination of the sac with the scope allows the surgeon to make a 1-cm skin incision over the defect. Via the skin incision, the sac is dissected free of the surrounding tissue, twisted, and ligated. A small piece of prolene mesh is rolled into a cigarette shape and used to reinforce the wall defect. The subcutaneous tissue and skin are closed over the repair.
Results: This technique was used to repair right femoral hernias in two males, aged 8 and 9 years. The first had previously undergone open repair of a right inguinal hernia. No contralateral femoral or additional inguinal hernia was identified in either patient. Operative time averaged 40 minutes. Both patients went home on the day of surgery and had uneventful recoveries. Follow-up at six months revealed excellent cosmesis and no recurrence.
Conclusion: This laparoscopic-assisted approach to pediatric femoral hernia repair with the addition of a small mesh plug is a safe, effective, and efficient technique. Its minimally-invasive component aids with diagnosis of this unusual pediatric condition and also allows for examination of the contralateral groin to assess for the presence of a femoral hernia. The addition of a small mesh plug facilitates the closure of the abdominal wall defect, which can be rather large, and appears to be safe even in children. Since only two incisions are required, in the umbilicus and above the sac, postoperative pain is minimal and cosmesis is excellent. However, more patients and longer follow-up are essential to accurately judge the long-term implications of this novel technique.
THE EYE OF THE BEHOLDER: PARENTAL ATTITUDES ABOUT MINIMALLY-INVASIVE SURGERY AND SURGICAL SCARS
Background: As minimally-invasive techniques become increasingly popular within pediatric surgery, much attention has been paid to parental concern about, or aversion to, surgical scars. However, parental beliefs about scars may not be as extreme as portrayed. In order to determine the level of parental worry about post-operative cosmesis, we asked parents to rate their concern about several features of surgical scars.
Methods: 100 parents were approached during pre-operative visits to Pediatric General Surgery clinic. They were given a questionnaire aimed at assessing surgical scars in terms of potential appearance, length, width, and location on a scale from 1 (not at all) to 6 (very) concerned. Parents also were asked about their preferences for minimally-invasive surgical (MIS) vs. open techniques.
Results: When given the option, the vast majority of parents surveyed (96%) preferred MIS to open approaches. However, only 15% of parents considered switching their child's care to another facility in order to have the procedure performed minimally-invasively. Parents were also surprising neutral in their concern for all aspects of surgical scars: potential appearance (mean=3.02, SD 1.81), length (mean=3.00, SD 1.88), width (mean=3.01, SD 1.81), location (mean 3.00, SD=1.80). No significant differences were found based on gender or age of children or parents.
Conclusion: Although parents do seem to enter clinics with a pre-operative preference for an MIS approach to surgery for their children, it is not necessarily a concern for cosmesis that is driving this inclination. Indeed, parents were surprisingly neutral when asked to rate their concerns about the physical aspects of surgical scars from length to width and location. Thus, it may other benefits, such as a decrease in post-operative recovery time and pain, rather than the avoidance of surgical scars that motivates a parental preference for MIS.
LAPAROSCOPIC & INTERNET-TRAINING COURSES IN PEDIATRIC SURGERY IN THE RF
Aim: For the purpose of development endo - and laparoscopic treatment methods in pediatric surgery in the Russian Federation, in our clinic was established the newest integrated videoendoscopic surgical complex named ≪OR-1≫ by “Karl Shtortz” & laparoscopic surgical simulators by Simbionix - LAP Mentor allowing to carry out complete training of experts.
Actuality: Considering the sizes and territorial remoteness of some regions of our country, exit training cycles are possible not always, therefore introduction of the given operational complex and the use of the laparoscopic simulator during the training cycles allows to rise training of all experts on qualitatively new high update level.
Materials and Methods: Thanks to HD technologies, ≪OR-1≫ allows to receive high definition and detailed images. The equipment allows to move by desktop pressing of several buttons, adjusting and changing modes of devices, optimizing visualization of images on monitors, carrying out digital record, simultaneous transmission of sound (an explanation of the operating surgeon) allow conduct high quality training, operation and directly respond to questions.
Also we have few laparoscopic surgical simulators - LAP Mentor system - because difficult to provide the necessary at once training in the operating room. The LAP Mentor provides a safe and motivating learning environment, as well as providing a complete educational solution integrated into training programs.
Results: Carrying out on line translations from the operational limits to a local network or through the Internet allowed to spend us for the past 2,5 years −23 training cycles for more than 270 regional experts in pediatric surgery. Most of the students were also trained on simulators (43). However, on our observations, training courses is more effective in groups no more than 5 – 6 persons as at intrernet training and during training on simulators.
Conclusions: Perfectioning of methods of integration in operating systems, able to broadcast qualitative HD signal in the worldwide web, as well using the LAP Mentor with tactile experience when using the surgical tools allows you to experience of tissue resistance during surgery simulation, allows to develop new systems of qualitative vocational training that, undoubtedly, gives the positively affects on the general professional level of profile experts.
MINIMALLY INVASIVE SURGERY IN NEONATES LESS 2500 GR
ABSTRACT WITHDRAWN
LAPAROSCOPIC COLPOPOIESIS BY SIGMOID INTERPOSITION AND CERVICAL CANALIZATION FOR CONGENITAL CERICOVAGINAL ATRESIA
Introduction: Congenital cericovaginal atresia is a rare Mayer–Rokitansky–Kuster–Hauser syndrome (MRKH). The conventional surgical approach is open laparotomy. We presented a laparoscopic colpopoiesis by sigmoid interpositing and cervical canalizating for a case with congenital cericovaginal atresia.
Materials and Methods: A 13 year old girl complained of primary amenorrhoea and cyclic, monthly abdominal pain for two months. CT scan showed her uterus's appearance and density is normal, but her cervix and vagina were absent. The laparoscopic surgery involved vagina reconstruction by sigmoid interposition, cervical canalization and end-to-end anastomosis with the neocervix and sigmoid colon by the use of an 16F Foley catheter as a stent into the uterine cavity.
Results: The operative time was 4 hours. Diet recovered at the 4th day after operation. No intraoperative and postoperative complications occurred. The patient recovered regular menses, relieved cyclic pain without severe infection and other post-operative complications.
Conclusion: Laparoscopic colpopoiesis by sigmoid interposition and cervical canalization is a safe and effective surgical approach for congenital cericovaginal atresia and has minimally invasive cosmetic results.
IS LOOKING FOR A CONTRALATERAL OCCULT HERNIA WITH LAPAROSCOPY REASONABLE IN CHILDREN?
Background: Inguinal hernia repair is a common procedure in daily pediatric surgical practice. Although children mostly present with unilateral symptomatic groin hernia, 6% can develop metochronous hernia on the contralateral side. The relatively high incidence of occult contralateral hernia in young children has led to the practice of laparoscopic contralateral exploration. Controversy exists, however, regarding its use in older children. The aim of this study is to compare the patients who underwent transinguinal laparoscopic exploration (TILE) and the ones who did not had TILE regarding the incidence of contralateral metachronous hernia development.
Methods: A retrospective review was completed of all cases of open inguinal hernia repair from January 2004 to October 2012. The patients who were explored laparoscopically through the ipsilateral hernia sac to assess the contralateral groin were compared with the ones who did not have TILE. The parents were called to get latest information. Mean follow-up time was 65±48 months. Chi-square test was used to assess the statistical difference.
Results: A total of 1599 children underwent open inguinal hernia repair. 1123 (70.2%) of the patients were male and, 476 (29.8%) of them were female. Mean age of the patients were 12 months (newborn-18 years). 951 (59.5%) and 489 (31.5%) of the patients had right and left sided inguinal hernia, respectively. 159 (9%) of the patients presented with bilateral hernia. Among 1440 patients presented with unilateral hernia, TILE was performed in 942 (65.4%) of the patients and a hernia or contralateral patent processus vaginalis was found in 18% of them (n=178). No complications occurred because of laparoscopy. TILE was not performed in 498 (34.6%) of the patients. 3 (0.3 %) of the patients who had TILE and 28 (5.6 %) of the patients who did not have TILE developed metachronous hernia (p<0.005).
Conclusion: Diagnostic transinguinal laparoscopic evaluation of the contralateral side during pediatric inguinal hernia repair is a simple, effective and reasonable method which clearly reduces the incidence of a metachronous hernia at a later date. The main drawback of this study is the short follow-up period which may be reflected as a lower incidence of metachronous hernia development in patients who did not have laparoscopic groin exploration.
MINIMAL INVASIVE SURGERY IN CHILDREN UNDER ONE YEAR OLD
Aim: As the minimal invasive procedures become more available and applicable in Pediatric Surgery, the age range of children at the time of operation has declined progressively. However the safety of minimal invasive surgery in children less than one year old is still on debate. The aim of this study is to investigate the results of patients under one year old who had undergone laparoscopy or thoracoscopy.
Patients and Method: The charts of neonates and infants who had undergone laparoscopy or thoracoscopy between November 2006 and November 2012 were evaluated retrospectively. The patientswere evaluated according to age, minimal invasive procedure, conversion, treatment and complications.
Results: In this study 354 patients were evaluated with a median age of 5 months (range 0–12 months). Transinguinal laparoscopic contralateral hernia exploration was performed in 218 (62%) children. Contralateral patent processus vaginalis was found in 85 of the children. Laparoscopic Nissen fundoplication±gastrostomy was performed in 39 (11%), hiatal hernia repair in two, gastrostomy in three, gastropexy in one, pancreatectomy in four, nefrectomy in two, pyeloplasty in two, diagnostic laparoscopy in 14 (4%), orchiectomy in one, oopherectomy in two, intestinal biopsy in two, intraoperative cholangiography in six (2%), liver biopsy in four, intussusception reduction in nine (2.5%), laparoscopic mass excision in six (2%), transanal pull-through in eleven (3%), ptrimary esophageal atresia repair and tracheo-esophageal fistula repair in six (2%), VATS in one, aortopexy in one, diaphragmatic hernia repair (Bochdalek or Morgagni) in 12 (3.4%), lobectomy in seven (one with pneumotocele, six with congenital cystic adenomatid malformation) and thoracoscopic mass excision in five (1.5%) children. There were three conversions from laparoscopy to laparotomy, two from thoracoscopy to thoracotomy and seven from thoracoscopy to thoracotomy ie. the conversion rate was 12%. There were recurrence in two neurologically impaired patients with gastroesophageal reflux disease and one patient with thymic teratoma. Two children encountered intestinal obstruction, one was neurologically impaired patient who had undergone Nissen fundoplication and gastrostomy and the second had undergone laparoscopy-guided transanal pull-through and laparotomy was performed in postoperative first week in both children.
Conclusion: In centers where education on minimal invasive surgery is well organised, the experience of pediatric surgeons on minimal invasive surgery increases and therefore the number of patients who are treated with minimal invasive procedures increases and the age range of the patient decreases progressively. As a result, in experienced centers minimal invasive procedures have become safer, even in children less than one year old.
THE RABBIT IS A VERY GOOD MODEL FOR NEONATAL ENDOSCOPIC SURGERY HANDS-ON COURSES
Objective: In recent years, various benefits of minimally invasive surgery in newborns have been documented. Training before performing neonatal endoscopic surgery plays a very important role in the safe widespread of these nouvelle techniques. In 2009, we developed a 3-day hands-on course using the rabbit as a neonatal training model.
Methods: The course was divided in theoretical sessions (10 hours) and training sessions (14 hours). The theoretical sessions were lectured by top international faculty. Both national and international faculty members mentored the practical sessions on 2 participants per monitor ratio. The rabbits were live and anesthetized during the practical training. Different procedures were performed by each participant. Every participant filled a query evaluating the course.
Results: From 2009 to 2012, 56 participants from 20 different countries took our hands-on neonatal endoscopic surgery course. All participants enjoyed performing thoracoscopic (esophageal atresia) and laparoscopic surgery (fundoplication, intestinal anastomosis) in the rabbit model. 55% of the participants found the course excellent. 43% found it very good.
Discussion: The rabbit is a reliable animal model for neonatal endoscopic surgery. Hands-on courses using this model is a good option for training pediatric surgeons.
MINIMAL ACCESS SURGERY FOR SELECTED SOLITARY TUMORS IN PEDIATRIC POPULATION
Background: Minimal access surgery for “pediatric” tumors is still controversial and literature is mostly focused in the “open” procedures. We are presenting our experience with children's who underwent laparoscopic/thoracoscopic resection for selected tumors with estimated low malignant potential. Special attention was paid to the adequacy and safety with assessment of the impact of minimal access approach on postoperative recovery, morbidity, cosmesis and recurrence.
Methods: Retrospective review of 16 consecutive patients who underwent complete tumor excision by MAS approach over the last 4 years. Patients weight ranged from 2.9 to 58 kg and ages from 1 month to 16 years. Most of the tumors were found incidentally with different imaging modalities.
Results: Seven patients underwent thoracoscopic and nine laparoscopic resection. The median age was 4.5 years. The median weight was 13.5 kg. All cases were done with 2/3, 5-mm ports and one 10-mm port for endo-bag evacuation. Tumor size ranged from 3 to 8 cm maximum diameter. There were no complications and all patients resumed oral feeds about 8 hours after surgery. The mean hospital stay was 2.5 days. The need for narcotic analgesia was minimal. Final diagnoses included: Ganglioneuroma (n=6), Neuroblastoma (n=1), Pheochromocytoma (n=1), and Dermoid tumor (n=8). No recurrence was detected in relatively short mean follow-up 1.76 y.
Conclusions: MAS for tumor resection can be performed safely in selected pediatric patients with excellent outcomes in terms of minimal discomfort, rapid recovery, and excellent cosmesis. Studies with larger volume of patients and longer follow up are required to adequately assess recurrence rate.
LAPAROSCOPIC DIAGNOSIS OF A CYSTIC MASS WITHIN THE HERNIA SAC IN MALES: IS IT A RARE ENTITY?
Aim: The small evagination of parietal peritoneum which is called the canal of Nuck is homologous to the processus vaginalis in the male. Hydrocele of the canal of Nuck is reported as very rare in the female. A similar clinical picture in the male, is described as an extremely rare entity which can easily be confused with other diseases that cause acute scrotum. The torsion of a cyst within the tunica vaginalis is described in these cases.
Methods: Five male patients presented with a cyst within the processus vaginalis. Two were admitted with an inguino-scrotal swelling and erythema. Remaining three were found incidentally during routine hernia repair, two of which were treated laparoscopically.
Results: A hernia sac was present in all patients. Emergency exploration of the inguinal canal revealed a torsioned hemorrhagic cystic mass within the hernia sac in two. Macroscopically, the hernia sac enveloped the comma-shaped cystic mass at one end with a tail directed cranially toward the inguinal canal. The testis, testicular vessels and spermatic cord were normal. A mass mimicking Nuck's cyst was identified and resected before running a purse suture laparoscopically in two other cases. Histomorphologic findings were compatible with benign cysts lined by flat mesothelial cells with hemorrhagic content in two.
Conclusion: Laparoscopic inguinal intervention may aid in revealing the presence of such a silent cyst which may be easily overlooked during an open hernia repair. It is obvious that the unique cystic mass presented in this study is more common than expected in the male population and deserves an entirely new clinicopathological description.
MUSCLE BIOPSY: A MODERN SERIES
Purpose: Muscle and skin biopsy are commonly used diagnostic procedures in the evaluation of neuromuscular and genetic disorders. However, there are few modern reports documenting the safety (surgical and anesthetic), diagnostic yield, and clinical utility of open skeletal muscle biopsy and skin biopsy. Our aim was to review our institution's experience with muscle and skin biopsy between January 2008 and April 2012.
Methods: The records of 169 patients were reviewed with particular attention to the presenting symptoms, preoperative clinical diagnosis, preoperative EMG results, pathology reports, intra- and post-operative complications, and the resultant change of diagnosis and treatment plan of the child based on muscle biopsy and skin biopsy. Further review of the genetic studies for those who have shown specific pathological features was performed.
Results: Muscle biopsy was successful in reaching a specific diagnosis in only 15% (26/169) of our patients and disease-specific therapy based on the results with anticipated improvement was started in only 4.1% (7/169) of our patients [86% (6/7) of them had inflammatory myopathy]. Preoperative EMG had a very low sensitivity and specificity (58% and 56% respectively). Concomitant skin biopsy at the same time of muscle biopsy for electron microscopy examination showed a negative result in 98.6% (70/71), even when the muscle biopsy had showed specific pathological changes. All patients diagnosed with mitochondrial disease showed negative results upon subsequent genetic studies. The only reported intraoperative complication was a femoral vein laceration when the vastus medialis muscle was chosen as a site of biopsy. Zero reported complications from the use general anesthesia were noted even in patients with electromyography evidence of myopathy. Three of five patients who had evidence of dystroglycanopathy in the muscle biopsy harbored the most common mutation in the causative gene upon subsequent genetic analysis.
Conclusion: Open muscle biopsy resulted in specific pathologic diagnoses in 15% of patients and an overall change in treatment outcome in 4%. Preoperative EMG lacked both sensitivity and specificity in detecting muscle pathology. Electron microscopy results of skin biopsy were negative in almost every case even when the muscle biopsy showed positive pathology. The muscle biopsy is considered a safe procedure even when done under general anesthesia. The diagnosis of mitochondrial disease should not be based on the result of the muscle biopsy alone. These results may help in counseling parents and patients and give them a realistic picture of the diagnostic yield of open muscle and skin biopsy.
Specific Diagnoses Obtained by the Histological Examination of the Muscle Biopsy
Introduction: The laparoscopic-assisted endorectal Soave pull-through procedure (LAEPT) and transanal endorectal pull-through (TOSEPT) procedure had been adopted widely for children with Hirschsprung's disease in the last two decades, but soiling occurred more commonly except shorter hospital stay, less analgesia requirement, and better cosmesis. We present our experience using the trans-umbilic laparoscopic-assisted modified Swenson approach (heart shape anastomosis) for Hirschsprung's disease child and technical modifications to reduce complications.
Methods: From 2012 May to 2012 October, we had 10 children with mucosa biopsy-proven HD including 6 boys and 4 girls (from 3 months to 5 years, average 1.8 y) treated by our team; all cases were underwent the modified Swenson procedure (heart shape anastomosis). Following one week bowel preparation using a daily rectal enema, 10 patients underwent trans-umbilic laparoscopic-assisted modified Swenson approach (heart shape anastomosis) procedure.
Three trocars were placed at the umbilic edge by open (hasson) method or puncture, the colon mobilizing procedure were same to the traditional trans-umbilic LAEPT except the rectum, the pelvic dissection was started from the upper segment of rectum, the mesorectum were dissected exactly along the posterior wall of the rectum by ultrasonic knife until 0.5 cm above the dentate line, in the anterior wall of rectum, only peritoneal reflection were opened by ultrasonic knife or electrocautery, the lateral of rectum were dissected by a oblique angle. Then the rectum was everted under the laparoscopy surveillance and incised to mobilize the proximal colon through the anus, the anterior wall of the rectum was incised 3.0 to 4.0 cm above the dentate line, the posterior wall was incised 0.5 cm above the dentate line, creating an oblique anastomosis.
The operating time, blood loss during operation, post-operation pathology, and incidence of postoperative complications (anastomotic leakage, enter-ocolitis, constipation, and soiling) were reviewed.
Results: The diagnosis of Hirschsprung's disease was verified by pathology. No conversion was required in all patients, mean operating times (minutes) were 162 (140 to 210). Mean blood loss were 7.5 ml. Median first bowel movement time was 22 hours, there were not perioperative comlication in all cases. Median daily defecation frequency was 3.2 within 2 weeks postoperatively, there were no soiling in all cases. Two cases have enterocolitis and one have constipation again during the follw-up, all of them were solved by conservative treatment.
Conclusions: The trans-umbilic laparoscopic-assisted modified Swenson approach (heart shape anastomosis) provides a convenient and cosmetic procedure for children Hirschsprung's disease, good continence may be expected for less pelvic nerves and vessels injury and fewer aganglionic segment residual.
JOINT APPLICATION OF PEDIATRIC LAPAROSCOPY AND HYSTEROSCOPY THE “PELVIC MASS” OF A FEMALE NEWBORN: 1 CASE REPORT
Objective: To explore and discuss the possible usage of joint application of pediatric laparoscopy and hysteroscopy in further exploration of “pelvic masses” in pediatric patients.
Methods: To Investigate the diagnosis of one case of “pelvic masse” of the female newborn, joint application of pediatric laparoscopy and hysteroscopy was utilized in the exploration. The clinical data of the case in our hospital on January 21, 2010 was analyzed retrospectively.
Results: The female neonate was 3 days old, the hospital diagnosis is intestinal obstruction, with a finding as “pelvic mass, enlarged uterine” in the examination of CT, MRI and ultrasonography. In the the multidisciplinary consultation discussion, it is suggested that hysteroscopy combined with laparoscopic exploration may be useful to the diagnosis. During the operation, vagina atresia was firstly excluded by hysteroscopy, no malformation of uterine was found. Followed by laparoscopic exploration, part of sigmoid colon and descending colon were found to be enlarged, indicating a diagnosis as congenital megacolon. Biopsy of the distal “narrow part” of colon was conducted and the pathologic finding convinced the diagnosis as aganlionosis.
Conclusions: Joint exploration of Pediatric Laparoscopy and Hysteroscopy may be a useful choice in cases with “pelvic mass” which is difficult to make the differential diagnosis through regular examination such as X-ray, ultrasonograghy, CT scan or MRI. Yet, more attention should be paid to in the future use, especially when and how to apply.
Key Words: female neonate pelvic mass laparoscopy, hysteroscopy, joint application.
ENDOSCOPIC TREATMENT OF PANCREATIC COLLECTION IN CHILDREN
ABSTRACT WITHDRAWN
TRANSCROTAL APPOACH ORCHIOPEXY UNDER SINGLE-PORT LAPAROSCOPE
Objective: To investigate the feasibility and efficacy of transcrotal approach orchiopexy for high inguinal cryptorchidism under the laparoscopic vision through the an umbilical port.
Methods: From August 2010 to May 2012, 30 children with 35 undescended testes in the inguinal canal or the abdomen were encountered transcrotal access orchiopexy assisted by single-port laparoscopy via the umbilicus. After a transverse incision was made on the scrotum, the tissue forceps was inserted into the inguinal canal or abdominal cavity through the scrotum and the external ring, and then the testis was grasped and pulled through extracorporeally. The processus vaginalis was separated off the cord structure to release the testis from cephalad retraction, the testis was fixed within the dartos pouch. Finally, under the laparoscopic guidance, the patent processus vaginalis was closed with a homemade two-hooked core endoneedle percutaneous extraperitoneally.
Results: All 35 testes were successfully descended transcrotal access under the laparoscopic guidance. The operative time was 30–100 minutes. There were no introperative complications. All of the testes maintained an adequate size and intrascrotal position with no atrophy or recurrent inguinal hernia during a follow-up of 6 to 22 months.
Conclusions: Transcrotal endoinguinal pull-through orchiopexy with single-port laparoscopy is a safe, effective and feasible procedure. It offers excellent cosmetic outcomes.
Keywords: Cryptorchidism; Laparoscopy; Scrotum; Orchiopexy.
ROBOTIC RESECTION OF A LARGE SPLENIC CYST AND INTRODUCTION OF THE ROBOTIC TISSUE SEALER
As robotic systems advance, new robotic instrumentation has evolved as well. We present a video presentation of a robotic resection of a large splenic cyst using a new robotic instrument called the Tissue Sealer which has identical thermal sealing and cutting properties as the widely used laparoscopic and open surgery devices such as the Ligasure. However, the Tissue Sealer also has the added advantage of an articulating movement which can be used for dissecting, sealing, and cutting in more precise planes.
A 16 year old girl had progressive symptoms of nausea and early satiety which slowly worsened over nearly a year. Eventually, she was hospitalized for emesis and dehydrationand work up demonstrated a large splenic cyst measuring 9×10×11 cm impinging on the stomach. There was no recent history of trauma or other symptoms but she retrospectively recalled an episode of left sided abdominal pain following a skiing accident about a year before this presentation.
Utilizing three 8 mm robotic ports and one 5 assistant port the patient underwent resection using the Da Vinci surgical robot. The robotic Tissue Sealer played a pivitol role and was used almost exclusively throughout the procedure. Robotic console time was 44 minutes, total case time was 1 hour 4 minutes, There were no complications and she went home on post-operative day number one with a complete resolution of her symptoms.
The robotic Tissue Sealer is capable of sealing vessels up to the same diameter as the Ligasure (7 mm). In addition to the case seen here, we have already used this robotic device for the mesentery in bowel resections and on other cases with medium sized vessels with excellent results, no bleeding, and no failures to date. The robotic Tissue Sealer may prove to be a game changer in robotic surgery similar to how the Ligasure was when it debuted in laparoscopic surgery.
INFANT ROBOTIC PYELOPLASTY: INITIAL EXPERIENCE
ABSTRACT WITHDRAWN
SINGLE INCISION LAPAROSCOPIC SURGERY WITH CONVENTIONAL INSTRUMENTS: EXPERIENCE IN CENTRAL INDIA
Background: Single Incision Laparoscopic Surgery (SILS) is an advanced minimally invasive operative approach in which operations are undertaken laparoscopically through a single small incision, typically placed at the patient's umbilicus. The most important prerequisite for SILS is the availability of specially designed instruments such as special port systems, endoscopes and instruments. In the developing world therefore, the advantages of SILS are overshadowed by the cost involved. We share the Jabalpur experience with the spectrum and technique of SILS in children being performed with conventional instruments.
Methods: At Jabalpur University, between March 2010 and October 2012, we have performed 108 procedures with SILS and have analysed the utility and limitations of the technique in children. All procedures were performed with umbilical incision and use of conventional instruments.
Results: Table.

5 procedures were converted to three port surgery and 2 were converted to open. There were few complications like: Umbilical wound infection(1), Omental prolapse(1), Poor cosmesis(2) and umbilical hernia(1). Otherwise, the procedures were safe and effective in terms of results and cosmesis.
Conclusion: We experienced that conventional instruments are cost effective and feasible for SILS in developing world. We feel most of the cases of appendicitis are easily managed with SILS which constitute maximum number in our series. Regardless of shortcomings, however, patients are increasingly demanding scar-less surgery and laparoscopic surgeons have to meet their demands for which SILS is a useful option for selected indications.
SINGLE-INCISION LAPAROSCOPIC PERCUTANEOUS EXTRAPERITONEAL CLOSURE MAY BE AN ALTERNATIVE TO STANDARD MINIMALLY INVASIVE SURGICAL TECHNIQUES FOR PEDIATRIC INGUINAL HERNIA
Background: Laparoscopic inguinal herniorrhaphy in children is an alternative to conventional open hernia repair. Numerous minimally invasive surgical techniques have been proposed for pediatric inguinal hernia. Ligation of the hernia sac without leaving a peritoneal gap was recently introduced to decrease the recurrence rate. Laparoscopic percutaneous extraperitoneal closure (LPEC) is one of the most simple and reliable procedures for laparoscopic pediatric inguinal herniorrhaphy, and has a low recurrence rate. We introduced the single-incision approach for LPEC in December 2009 to reduce the invasiveness of LPEC and to improve cosmesis. In the present study, we compared the safety and feasibility of single-incision LPEC (SILPEC) with those of standard LPEC. We also examined whether SILPEC could become a standard minimally invasive technique for pediatric inguinal hernia.
Patients and Methods: From February 2007 to October 2012, 909 laparoscopic herniorrhaphy procedures were performed at our center by 1 of 10 pediatric surgeons with assistance from another surgeon. A 3 mm laparoscope was inserted through a transumbilical incision. A 3 mm grasping forceps was inserted into the lower abdomen during LPEC, and through the same transumbilical incision with a different entrance for SILPEC. The hernia sac was closed extraperitoneally using the LPEC needle, which includes a wire loop to hold the string. We first compared the demographic data and outcomes of 909 children who underwent either technique. Next, the changes in pneumoperitoneal duration for each surgeon according to the number of operations were examined, and the target pneumoperitoneal duration was determined based on the learning curve plateaus. We also calculated the number of operations in which each pediatric surgeon achieved the target pneumoperitoneal duration.
Results: From February 2007 to November 2009, 286 LPEC procedures were performed, while from December 2009 to October 2011, 623 SILPEC procedures were performed. There were no significant differences in demographic characteristics between the two groups. There were no severe operative complications in either group. The mean pneumoperitoneal time was similar for girls and boys in both groups. One patient after LPEC and two patients after SILPEC relapsed with hydrocele of the testis. Although the learning curves were slightly different among the surgeons, all of the surgeons achieved the target pneumoperitoneal duration for SILPEC (females, 14.8 min; males, 16.6 min) after performing at least 40 procedures.
Conclusion: SILPEC was a safe, effective, and feasible procedure that was comparable with LPEC in this group of 10 pediatric surgeons. The surgeons were able to master SILPEC after a sufficient number of procedures. Therefore, we consider that SILPEC could become the standard laparoscopic technique for pediatric inguinal herniorrhaphy.
SINGLE PORT ACCESS LAPAROSCOPIC RIGHT HEMICOLECTOMY IN CHILDREN: TREATMENT OF CHRONIC INTUSSUSCEPTION CAUSED BY ILEOCECAL BURKITT LYMPHOMA
Background: The umbilical laparo-endoscopic single-site surgery (LESS) is to minimize the unnecessary trauma and achieve the combination of minimally invasion with cosmetic advantage for scarless surgery. We report in this paper a new technique of umbilical single port access (SPA) laparoscopic right hemicolectomy complying with conventional surgical oncologic principle and technique of minimally invasive colectomy in children.
Methods: Preliminary experience with umbilical SPA right hemicolectomy in a 5-year-old child with chronic intussusception caused by ileocecal Burkitt lymphoma. The patient was offered this approach after having given informed consent of his parents. With a thorough preoperative preparation, laparoscopic exploratory operation was performed under general anesthesia. Firstly, a 5 mm trocar was placed in the middle of umbilicus after a two-centimeter-incision was cut along the right edge of umbilical ring and artificial CO2 pneumoperitoneum was established with a 9 mmHg. Thereafter, two plastic 5 mm trocars were placed up and down side of the incision respectively. Through laparoscopy, one mass of 6 cm×5 cm×4 cm size was confirmed ileum-colon-colonic type of intussusception, with nested appendix and lots of swelling mesenteric lymph nodes. After restoring intussusception, we found a tumor with 3 cm×2 cm×2 cm size beside the ileocecus, then resected lateral peritoneum of ascending colon and gastrocolic ligament in liver area by ultrasonic knife, freed and extracted ileocecus and right hemicolon outside the abdominal cavity through expanding umbilical incision up to 3 cm. Surgical dressings were placed around the umbilical incision, then resection of terminal ileal and right colon and ileum-transverse colon anastomosis were performed in vitro according to the results of frozen biopsy, malignant lymphoma and reactive proliferative lymph nodes. Moreover, the anastomotic intestine was return into peritoneal cavity and umbilical incision was sutured layer by layer.
Results: Umbilical SPA laparoscopic right hemicolectomy was performed successfully with conventional laparoscopic instruments. Operative time was 90 min and the volume of hemorrhage was 20 ml. No intraoperative and postoperative complications were recorded. Diet recoveried at the fourth day after operation.
Conclusion: Umbilical SPA laparoscopic right hemicolectomy is feasible and safe in children when performed by experienced laparoscopic surgeons. Umbilical SPA laparoscopic right hemicolectomy can not only follow the traditional surgical oncological principles of surgery, but also achieve minimally invasive cosmetic results due to soft pain, quick recovery and hidden incision similar to scarless surgery, which may have the advantage over NOTES approach to offer the safety of laparoscopic colectomy especially for children colorectal disease.
THE SINGLE PORT LAPAROSCOPIC TECHNIQUES FOR INGUINAL HERNIA AND HYDROCELE IN CHILDREN
Purpose: To investigate the single port laparoscopic techiniques for inguinal hernia and hydrocele in children.
Methods: From Jan 2011 to June 2012, one hundred-eighteen children (76 chidren with inguinal hernia and 42 children with hydrocele) underwent the single port laoparoscopic ligation of internal ring.
Results: All of children underwent this operation successfully. The mean duration of surgery was 15 minutes in children with unilateral lesion, and the mean time required for surgery was 28 minutes in children with bilateral lesions. The average hospital stay period after surgery was 1.5 days. All the patients had been followed up and no recurrence.
Conclusions: the single port laparoscopic techniques for inguinal hernia and hydrocele in children is safe and effective.
TRANSUMBILICAL MULTIPORT LAPAROSCOPIC NEPHROURETERECTOMY FOR CONGENITAL RENAL DYSPLASIA IN CHILDREN
Objective: To assess the clinical utility and safety of transumbilical multiport laparoscopic nephroureterectomy (TMLN) for the treatment of congenital renal dysplasia in children by analyzing consecutive cases performed by a single surgeon.
Methods: Five female children underwent TMLN procedure due to dysplastic kidney between January 2010 and December 2012. The surgery was transperitoneally performed through three transumbilical incisions for two 5-mm and one 3-mm ports, which duplicated the standard laparoscopic steps with the usual laparoscopic instruments. Demographic, perioperative, and follow-up data were analyzed.
Results: TMLN was successfully performed in all patients, without additional ports or conversion to open surgery. The mean operation time was 108.4 minutes (range 100–125) and the blood loss was minimal. There were no intraoperative or postoperative complications. The postoperative recovery was uneventful in all patients. No severe incision complications or umbilical hernias occurred. The cosmetic result was excellent as the incision scar was hidden inside the belly button.
Conclusion: TMLN is a feasible and safe procedure for the management of congenital renal dysplasia in children with good cosmesis. Future randomized studies with a larger number of cases and a longer follow-up are warranted to elucidate the benefits and limitations of TMLN in children.
LAPAROSCOPIC MANAGEMENT OF OVARIAN CYSTS IN NEWBORN AND INFANTS: GOOD INDICATION FOR SINGLE INCISION LAPAROSCOPIC SURGERY
Background and purpose: There is no standard treatment for ovarian cysts in newborn and infant. This condition frequently causes ovarian torsion/necrosis, so the main aim of treatment is to preserve ovarian function. In our institution, we treat ovarian cysts according to the following strategy. (1) Simple cysts should be monitored, regardless of size. Patients with cysts <3 cm can undergo outpatient, while those with cysts >3 cm should be admitted. (2) Surgery is indicated complex cysts, non-shrinking simple cysts, difficult differential diagnoses, wandering cysts, and symptomatic patients. From 2007, we performed laparoscopic-assisted surgery for this status. Here we report our experience of laparoscopic management for ovarian cyst in newborn and infant, especially our latest single incision procedure.
Materials and Methods: From 2007 to 2012, 13 patients underwent laparoscopic surgery for ovarian cysts. Nine were neonates and four were infants (mean age at operation was 29.8). Indication for operation was non-shrinking cyst for one and complex cysts for other 12. All patients were diagnosed prenatally. From 2007 to 2011, we performed two incisions laparoscopic surgery in principle. In 2012, we started single incision laparoscopic-assisted surgery (SILS) with EZ access (Hakko Medical, Japan).
Results: Two of 13 had ovarian cyst without torsion, so underwent only fenestration and aspiration of the cyst. Eight of 13 had cyst with torsion and necrosis, and underwent detorsion, fenestration (including biopsy of cyst wall) and aspiration. In other three patients, ovarian cysts were amputated at the operation, so we performed cystectomy. In 2012, four of five cases underwent SILS. The concept of the treatment was the same as the cases before 2011. In another one patients, because of hard adhesion between cyst and peritoneum, we needed another port and performed synechotomy, aspiration and detorsion. In all cases, we confirmed normal contralateral ovary laparoscopically. In all 13 cases, post operative cause was uneventfully and persistant cyst wall have not caused any trouble. Microscopically, viable ovarian parenchyma was found on some specimens of cyst wall, even in amputated cyst.
Conclusion: In our series, laparoscopy-assisted management of ovarian cyst was very useful and performed safety. In most cases, SILS could be performed safety. If there is some difficulty to perform SILS, we can add some extra ports without any trouble. Our strategy to preserve most part of the cyst seems appropriate.
SINGLE-PORT NON-ASSISTED LAPAROSCOPIC TREATMENT OF INDIRECT INGUINAL HERNIAS IN GIRLS
ABSTRACT WITHDRAWN
TRANSUMBILICAL SINGLE-INCISION LAPAROSCOPIC CLOSURE OF THE INTERNAL RING FOR INGUINAL HERNIA IN CHILDREN
Objectives: To explore the feasibility of transumbilical single-incision laparoscopic closure of the internal ring for inguinal hernia in children.
Methods: 313 children patients (283 males, 30 females) with inguinal hernia were performed an operation of transumbilical single-incision laparoscopic closure of the internal ring. All the cases of patients are aged from 6 months to 13 years old (mean age 3.98 yeas), of which 205 cases were preoperative right inguinal hernia, 93 left inguinal hernia, 15 bilateral inguinal hernia. 3 cases relapsed after the traditional high ligation of the hernial sac, and 135 preoperative unilateral inguinal hernia (diagnosed bilateral inguinal hernia intraoperatively).
Operation steps: Endotracheal anesthesia was conducted in all this cases, prostration or trendelenburg position. A 5-mm incision was made on the right side of the umbilicus, pneumoperitoneum needle penetrated into abdominal cavity, establishing pneumoperitoneum (pneumoperitoneum pressure 9–12 mm Hg). Then trocar was placed in this incision, laparoscope (0°or 30°) introduced through the umbilicus. A 3 mm or 5 mm incision was made on the left side of the umbilicus, trocar inserted into it, regular needle holder introduced into abdominal cavity. Under the direction of the laparoscope, whether both internal rings have been closed could be checked. At the skin projection of the internal ring on the side of hernia, a round-tip needle with 2-0 silk suture was pierced into the abdominal cavity and grasped by a regular needle holder. Then the peritoneum was sutured from the lateral of internal ring by a circle and ligated with a surgical knot in case of loosening, the suture cut off, the needle penetrated out of the abdominal wall via the roof of the internal ring. The pneumoperitoneum and trocar were removed. The umbilical incision was subcuticularly sutured with 5-0 antibiosis absorbable line and adhered with medical adhesive dressing.
Difficulties: Laparscopy and needle holder were introduced into abdominal cavity from the same direction, rebelling the principle of triangle, it is difficult for surgeons to operate because of mutual interference between them. But once grasping the skills, it is much easier and more smooth to perform the surgery.
Results: None of the patients underwent conversion from single-incision laparoscpic to open approach or conventional laparoscopic surgery. The operational time was 5–30 minutes, without injury to intestine spermatic cord or spermatic duct. The patients were discharged the day after operation. No postoperative bleeding, hematoma of scrotum, or incisional infection occurred. Follow-up checkups in the all cases in 1 month showed no recurrence.
Conclusion: Transumbilical single-incision laparoscopic closure of the internal ring is a reliable, safe, feasible, and cosmetic herniorrhaphy for the treatment of pediatric inguinal hernia.
SINGLE-INCISION LAPAROSCOPIC SURGERY FOR RECURRENCE ABDOMINAL PAIN
Background: Laparoscopy is the acceptable treatment for abdominal diseases in children, especially for difficult diagnosis of abdominal pain. The benefits of the techniques include a shorter hospital stay and faster return to feeds. The standard laparoscopic approach based on the 3-port technique using two incisions to pass operating instruments. In contrast to the standard laparoscopic technique, the single incision laparoscopic surgery (SILS) requires only one incision. We report on our experience with this surgical approach.
Materials & Methods: Between April 2009 and April 2012 a total of 14 children with recurrence abdominal pain underwent a laparoscopic approach, all patients in SILS technique. The single incision was carried through the center of the umbilicus. The Trocar for optic telescope was inserted through an umbilical incision. The working instruments were introduced in a two-dimensional direction into the peritoneal cavity via the same umbilical incision. Afterwards, the different reasons of abdominal pain were explored. The different treatments were performed by the diseases.
Results: All SILS procedures were performed successfully with no conversion rate. We found chronic appendicitis in 4 cases, Meckle's diverticulum in 4 cases, allergic purpura in 2 cases, duplication of intestine in 1 case, mesenteric lymphadenitis in 2 cases, heterotopic pancreas in 1 case. There were no differences in the preoperative parameters compare to standard 3 trocars technique. There were no operative or postoperative complications.
Conclusions: SILS trocarless laparoscopic technique is a safe alternative to standard laparoscopic technique with three trocar approach. The minimal scarring guarantees an attractive cosmetic result. This technique can be applied for diagnosis and treatment of recurrence abdominal pain in children.
TREATMENT OF INGUINAL HERNIA IN CHILDREN WITH AN UMBILICAL SINGLE-INCISION LAPAROSCOPIC PERCUTANEOUS EXTRAPERITONEAL CLOSURE USING A SYRINGE NEEDLE
Background/Purpose: To report an umbilical single-incision laparoscopic percutaneous extraperitoneal closure (SILPEC) by syringe needle to treatment of inguinal hernia in children.
Materials and Methods: Between March 2011 and October 2012, 1170 children with inguinal hernia were treated with umbilical SILPEC by syringe needle at Anhui Provincial Children's Hospital. 5-mm and 3-mm Trocars were inserted through an umbilical incision, through which a laparoscope and grasping forceps were placed into the abdomen. A No. 9 syringe needle with folded No. 1 thread in the core and No. 7 thread in the No.1 thread loop at the tip was stabbed to the anterior extraperitoneal wall of internal ring. After the needle was extraperitoneal punctured the inner semi-circle of internal ring to reach the posterior wall of internal ring, the needle was punctured into the peritoneum to enter the abdominal cavity. The No. 7 thread was pulled out from the No. 1 thread coil, and then the needle was slowly extracted to the anterior peritoneal wall of internal ring. Using the same method, the needle was extraperitoneal punctured the outer semi-circle of internal ring to reach the posterior wall of internal ring, and was punctured into the peritoneum to enter the abdominal cavity. The No. 7 thread sewn into the abdominal cavity in the inner side was pulled into the No. 1 thread coil using the grasping forceps. After the coil was tightened, the needle was extracted to take out the No. 7 thread. The thread was ligatured, and then was cut to complete the high ligation of the hernia sac.
Results: All patients were successfully treated with the surgery with minimal invasion. No recurrence was observed during the follow-up.
Conclusion: The method reported here is reliable, safe and minimally invasive with low cost.
EVOLUTION TOWARDS LESS IN PYLOROMYOTOMY - ADVANTAGES AND PITFALLS OF LAPARO-ENDOSCOPIC SINGLE-SITE SURGERY
Introduction: The reduction of invasiveness is a current topic in pyloromyotomy. We compare the outcome of open pyloromyotomy (OP), standard 3-port laparoscopic (3-TP) and Laparo-Endoscopic Single-Site pyloromyotomy (LESS-P) in children and present a video of LESS-P.
Methods: We reviewed the medical files of 233 children operated on by pyloromyotomy between February 2004 and October 2012 in a university teaching hospital. 141 patients underwent OP, 71 3-TP and 21 LESS-P. We compared the incidence of intraabdominal complications like mucosal perforation and intraabdominal lacerations, wound infections, as well as the median±SD for duration of operation in minutes and time until toleration of oral feeding in days.
Results: (Table 1) The incidence of mucosal perforations was 9/141 in OP, being higher (P=.01) than in the laparoscopic procedures 3-TP and LESS-P (0/92). The duration of operations did not show differences between OP vs. 3-TP (P=.19), OP vs. LESS-P (P=.90), and 3-TP vs. LESS-P (P=.48) and were 39.5±76.8 min. (OP), 40.0±16.1 min. (3-TP), and 38.5±14.3 min. (LESS-P). The incidence of wound infections did not differ significantly (P=.71) between the different procedures and were 4/141 for OP, 2/71 for 3-TP, and 2/21 for LESS-P. All wound infections in 3-TP and LESS were associated with the use of tissue adhesives. Wound infections in 3TP and LESS-P were abolished after re-initiation of wound closure with sutures. Time until toleration of oral feeding was higher for OP when compared to either 3-TP (P=.00) and LESS-P (P=.00) and were1±.67 days (OP), 0±.29 days (3-TP), and 0±0 days (LESS-P).

Investigated Parameters in Pyloromyotomy
Conclusions: We report that LESS-P and 3TP are superior to OP with regard to mucosal perforations and have a similar duration of operation. Wound closure with tissue adhesives appears to promote wound infections in laparoscopic procedures.
Background: Laparoscopic repair has been regarded as a safe and effective technique in repairing pediatric inguinal hernia and hydrocele. This minimally invasive technique has the advantages of better cosmesis, faster recovery, decreased requirement for oral analgesics, better visualization of the anatomy, and detection and even repair of the contralateral patent processus vaginalis. Different laparoscopic techniques for hernia repair have been described including intracorporeal suturing and extracorporeal ligation of open inguinal rings. Here we describe our new technique for laparoscopic processus vaginalis repair with subumbilical single-port using a holed Kirschner pin that achieves transfixation ligature of the processus vaginalis and that may further reduce recurrence.
Methods: A 5-mm port was inserted at the infraumbilical region for insertion of a 5-mm laparoscope and carbon dioxide pneumoperitoneum was maintained at 10 to 12 mm Hg. A Kirschner pin with a hole in one flat terminal which a 2-0 nonabsorbable suture was threaded through the hole was inserted at the point of the internal inguinal ring. The pin was then advanced extraperitoneally over the testicular vessels/spermatic duct or under the round ligament by performing dissection within the preperitoneal space (Fig. A). After this dissection, the pin penetrated the peritoneum on the opposite side, and a small opening was made in the peritoneum (Fig. B). The laparoscope was inserted into the loop of suture and the Kirschner pin was withdrawn with the end loop of the suture remaining in the abdominal cavity (Fig. C) and the ends remaining above the skin. Then the Kirschner pin with another nonabsorbable suture easily reached the upper half of the internal inguinal ring extraperitoneally and was advanced on the same opening of the peritoneum and entered the loop (Fig. D). Using the same method the Kirschner pin was withdrawn leaving the second suture loop in the abdominal cavity (Fig. E). The first suture was then removed from the abdomen together with the second suture. The processus vaginalis was closed and the circuit suturing was tied extracorporeally (Fig. F).
Results: Between September 2010 and September 2012, 211 children (130 cases of inguinal hernia and 81 cases of hydrocele) underwent processus vaginalis repair using this novel technique. The mean operative time was 10 minutes (5–25 minutes). All patients were discharged uneventfully from the hospital within 24 hours postoperatively. The mean follow-up period is 10 months (range 2–24 months), and no recurrence has been observed to date.
Conclusions: This article describes an unique technique of extracorporeal circuit suturing of processus vaginalis using a minimally invasive technique as afforded by a reused modified Kirschner pin. Single-port laparoscopic processus vaginalis repair using this instrument is feasible and seems to be safe. Further studies are required to determine whether this approach would benefit patient compared with standard laparoscopic techniques and long-term outcomes remain to be defined.
THE CURRENT STATE OF SINGLE INCISION PEDIATRIC ENDOSURGERY (SIPES): AN INTERNATIONAL PERSPECTIVE
Purpose: The application and awareness of Single-Incision Pediatric Endosurgery (SIPES) is increasing. A variety of SIPES surgical techniques and indications have been independently described by select centers around the world. In order to facilitate a cooperative approach towards advancing and investigating the practice of SIPES, it is necessary to understand its current prevalence in terms of geography, technique, and acceptance. We therefore conducted a survey among members of the International Pediatric Endosurgery, asking them about their experience and attitudes towards SIPES.
Methods: After IRB approval, an invitation to participate in an anonymous online survey was sent out to all International Pediatric Endosurgery Group (IPEG) members. Questions focused on demographic information including location, practice patterns indications and equipment used regarding SIPES.
Results: Of the 560 contacted active IPEG members, 115 completed the survey (recall 21%). The respondents represented pediatric surgeons from 32 countries on 6 continents. Of respondents, 97% had heard of SIPES, while 71% had performed SIPES. Reasons for not having performed SIPES included disbelief in benefit (59%), lack of proficiency (34%), and having inadequate resources (28%). The most commonly performed SIPES procedures were appendectomy (85%), cholecystectomy (66%), splenectomy (42%), pyloromyotomy (35%), intestinal surgery (13%), as well as Nissen fundoplication and gynecologic adnexal pathology (7%). The utilized equipment and techniques show large variation and include some self-devised, innovative, low-resource approaches. Perceived benefits and drawbacks are presented in the table. Complications with SIPES reported by the survey participants included technical difficulties, wound infection, prolonged operating time, bleeding, increased pain, umbilical hernia, and wound dehiscence.
Reported Benefits and Drawbacks of SIPES
Conclusions: SIPES is being performed worldwide for a large spectrum of common indications in pediatric surgery. The equipment and techniques employed are different depending on geographic location and resources. Some encountered complications are common to those seen with conventional minimal-invasive surgery, while others may be SIPES-specific. Interestingly, different respondents reported conflicting views on pain, operating time, and cost. Besides reporting the current state of SIPES in the IPEG community, this study serves as a plea for networking between centers in an effort to standardize techniques and study these novel approaches systematically.
Objective: To evaluate the feasibility and efficiency of transumbilical single port laparoscopic spermatic vessels cluster high ligation in treatment of children's varicocele.
Methods: A lengthwise cut in the upperlimb of the umbilicus was made, through which one 5 mm trocar was inserted into the abdominal cavity as viewport. Two other 5 mm trocars were inserted at the 4 o'clock, 8 o'clock position in lowerlimb of the umbilicus respectively. Laparoscopic spermatic vessels cluster high ligation completed by using the lengthen operating apparatus.
Results: A total of 22 cases of transumbilical single port laparoscopy were performed successfully without complications. The mean operative time was 39.4 min (34∼58 min) and mean postoperative hospital stay was 3.5 d (2∼5 d). Patients were followed up 6∼12 months after operation. No case of relapse and testicular atrophy happened.
Conclusions: Transumbilical single port laparoscopic spermatic vessels cluster high ligation is safe, scarless, effective and is worth promotion as a novel surgical approach for children's varicocele.
USEFULNESS OF TRANSUMBILICAL LAPAROSCOPIC-ASSISTED APPENDECTOMY IN CHILDREN: EXTERIORIZATION OF THE APPENDIX IS A SIMPLE AND COST-EFFECTIVE SURGICAL PROCEDURE
Background/Purpose: Laparoscopic appendectomy in children is a well-established surgical procedure. Single-incision laparoscopic appendectomy was recently introduced as a less-invasive surgical technique, and is increasingly being performed. We have started to perform transumbilical laparoscopic-assisted appendectomy (TULAA) in children. In this study, we assessed its feasibility, efficacy, and cost-effectiveness compared with conventional multiport laparoscopic appendectomy (MLA).
Patients and Methods: We retrospectively reviewed all of the patients who underwent laparoscopic appendectomy between August 2009 and October 2012. The patients were divided into two groups: those who underwent MLA (between August 2009 and July 2011) and those who underwent TULAA (between July 2011 and October 2012). Patient characteristics, operation time, length of stay, postoperative complications, cost-effectiveness, and cosmetic results were retrieved from medical records. MLA was performed via the umbilicus with a camera port and working ports placed in the right upper and left lower quadrants of the abdomen. The mesoappendix was separated by laparoscopic coagulating shears (LCS) and double ligation of the appendix root was performed using thread loops. TULAA was performed through a single vertical umbilical incision, and a single disk with multiple ports was inserted. After pneumoperitoneum, the appendix was exteriorized through the umbilical incision and dissected outside the abdominal cavity, as in open surgery. If the appendix could not be reached from the umbilical incision, an intracorporeal approach was performed through the single incision. The base of the appendix was then dissected and ligated. Additional ports were added if the surgeon thought this was necessary for a safe operation.
Results: A total of 85 patients underwent laparoscopic appendectomy, with MLA performed in 48 patients and TULAA performed in 37 patients. The age ranged from 4 to 16 years old. TULAA was successful in 34/37 patients (92%). In three cases, dissection of the appendix from the surrounding tissue was so difficult that an additional port for TULAA or conversion to MLA was necessary. There were no significant differences in mean operative time (71.1±36.7 vs. 73.0±30.0 min) or the mean length of hospital stay (5.83±2.54 vs 6.78±2.75 days) between the TULAA and MLA groups. There were no postoperative complications in the TULAA group. In the MLA group, two patients developed superficial wound infections and two patients suffered from prolonged paralytic ileus. Cost analysis demonstrated a markedly reduced cost associated with TULAA compared with MLA, because TULAA requires fewer disposable materials and a standard laparoscopic setup. TULAA also provided nearly scarless surgery.
Conclusion: TULAA is a safe and effective procedure for acute appendicitis in children by combining open and laparoscopic techniques to provide cost-effective treatment and excellent cosmetic results.
SINGLE-INCISION LAPAROSCOPIC VERSUS CONVENTIONAL LAPAROSCOPIC ENDORECTAL PULL-THROUGH FOR HIRSCHSPRUNG'S DISEASE: A COMPARISON OF SHORT-TERM SURGICAL RESULTS
Background: Single-incision laparoscopy has recently become popular in pediatric surgery. The current series is the largest study to evaluate the operative complications and results of single-incisin laparoscopic endorectal pull-through (SILEP) for the treatment of HD through a retrospective comparison with conventional laparoscopic endorectal pull-through (CLEP).
Methods: Twenty eight patients who underwent single-incision laparoscopic endorectal pull-through for HD between July 2010 and August 2011 were compared to thirty patients who underwent CLEP. Patients' age, gender, transitional zone, operative time, blood loss, intraoperative and postoperative complications, as well as short-term results were assessed.
Results: A total of 28 patients were included for SILEP and historical reported 30 patients were completed by CLEP. The SILEP and CLEP groups were similar in regard to age, gender, transition zone, operative time, blood loss, hospital stay, and intraoperative complications. Postoperative results were no different, including equal daily defecation frequency and early postoperative complications, no patients with recurrent constipation were seen. Two patients with transitional zone in descending colon in the SILEP group were added a 3 mm trocar in left abdomen, and there were no conversions in the conventional laparoscopic group.
Conclusion: We have shown that in selected HD patients, the SILEP technique was safe and technically feasible in experienced hands. It results in similar operative results compared with conventional laparoscopic endorectal pull-through. However, the operation would be more difficult if a transition zone was higher than the rectosigmoid.
REDUCED PORT SURGERY: OUR INITIAL EXPERIENCE AND DESCRIPTION OF NEW DEVICE
Background: Minimally invasive surgery is the current accepted approach in children. However, less invasive techniques such as single incision laparoscopic surgery (SILS) are being used more frequently in adult. It has been proposed to improve the cosmesis and decrease the morbidity associated with multiple ports sites. Experience with SILS technique in pediatric surgery is still limited. This report describes our initial experience with SILS and Reduced Port Surgery (SILS plus one puncture; SILS-POP) in children.
Materials and Methods: We reviewed all the patients who underwent SILS or SILS-POP at our department. We used trans-umbilical multi trocars or a multi-channel single laparoscopic port inserted through a minimal skin incision to achieve access to the abdominal cavity. In case of requiring additional instrument, we used an instrument 2 mm in diameter by direct puncture method (SILS-POP).
Results: Totally 25 patients have undergone SILS or SILS-POP at our department, including appendectomy in 20, Nissen fundoplication in 2, splenectomy in 1, and total colectomy in 2 (ulcerative colitis, 1; Hirschsprung's disease, 1). SILS or SILS-POP was successfully completed in all cases and none required conversion to open or conventional laparoscopic surgery. There were no intraoperative surgical complications. Postoperative complication (superficial incisional site infection) presented in 2 cases (appendectomy, 1; Hirschspurung's disease, 1).
Conclusions: Our initial data show that SILS and SILS-POP is an effective technique for pediatric indications. SILS needs the highly skilled techniques to eliminate the influence of the loss of the manipulate-angle, working inline with the camera, and the instruments crowding. However, in SILS-POP, an additional fine instrument makes some advanced procedures reproducible and viable. By using new instrument, reduced port surgery can be one of the choices of pediatric surgical procedure that can be accomplished with conventional laparoscopic techniques. Additionally, excellent cosmetic results can be obtained as evidenced by imperceptible umbilical scarring.
SILS VERSUS LAPAROSCOPIC PAEDIATRIC CHOLECYSTECTOMY/SPLENECTOMY—CASE SERIES REVIEW
Background: Minimal invasive surgery gained great achievements in paediatric population in the last decades. Currently, the new generations of training surgeons adopt this technology and it is commonly applied in a most of surgical procedures including cholecystectomy and splenectomy. SILS procedures have been advocated in some paediatric laparoscopic centres.
Aim: To review outcome of minimal invasive surgical procedures including SILS for cholecystectomy and splenectomy in paediatric age group, which have been performed by single experienced laparoscopic surgeon.
Methods: A retrospective case-note review has been carried out of all paediatric laparoscopic cholecystectomies and or splenectomies including SILS performed in the period between May 2009 and November 2012 (42 months). All operations have been performed by same surgical team in two different paediatric surgical units (tertiary centres). Patients' demographic details, underlying pathology, operative time, hospital stay and complications are collected and analysed.
Results: All the operations were planned procedures. 24 patients (4 boys and 20 girls) underwent a total of 30 minimally invasive procedures including SILS: laparoscopic cholecystectomies (14 procedures), splenectomies (13 procedures), appendicectomy (1 procedure) and liver biopsy (2 procedures). SILS have been carried out in 5 procedures; 3 splenectomies and 2 cholecystectomies. None of the SILS procedures were converted to multiple port procedures. No extra port has been used in SILS procedures. The range of patients' age is (6–15) years. Mean surgical follow up period was 3 months. The majority of patients have haemolytic disorders including (spherocytosis, β-thalassemia and sickle cell disease). ASA grade is 3 for most of the patients. All operations completed successfully without conversion to open except the first case in the addressed period. The range of operative time is (270 minutes in combined procedures) and (75 minutes in single procedure). Post-operatively, all patients received PCA (patient control analgesia) to control pain. Average hospital stay postoperatively is 3 days, however extended for a week in medically complicated cases. No mortality and no significant morbidity have been reported.
Conclusion: Minimal invasive surgery for cholecystectomy and splenectomy is becoming a standard choice. It is safe and feasible procedure among medically complicated cases. In current series, no significant differences in the outcome between multiple ports and SILS procedures have been noted. However, SILS has superior cosmetic outcomes. We encourage wide use of SILS in other procedures in paediatric age group. Also, we recommend PCA in post-operative period particularly after SILS procedures to minimize port site pain.
LAPAROSCOPIC METHODS IN THE TREATMENT OF CONGENITAL DUODENAL OBSTRUCTION FOR NEONATES
Objective: To evaluate the feasibility and indication of the laparoscopic methods for neonates with congenital duodenal obstruction.
Methods: From September 2009 to October 2012, 40 newborns with duodenal obstruction underwent exploratory laparoscopy. With a lower-pressure pneumoperitoneum of 5∼8 mmHg and a suspending suture for right liver elevator, the procedure was performed using 4 trocar of 5 mm diameter. Under the laparoscopic vision, the causes of duodenal obstruction were diagnosed, and then the operation methods were determined by the type of the obstruction.
Results: Of all the cases, 4 was duodenal atresia, 8 were duodenal stenosis, 8 were annular pancreas, and 20 were congenital intestinal malrotation. The cases with duodenal diaphragmatic stenosis were performed a partial excision of the diaphragm after vertical incision of the anterior part of duodenum followed laparoscopically by a transverse suture. For the case with duodenal atresia and annular pancreas, a diamond anastomosis of duodenum was successfully carried out through a laparoscopic approach. Ladd's operational method was performed in the cases with congenital intestinal malrotation. Feedings were started on postoperative day 3 to 7, without abdominal distention and vomit, out the hospital on postoperative day 9 to 14.
Conclusion: Congenital duodenal obstruction is common malformation in neonates. laparoscope is an important method of diagnosing, and correct operational methods are the key to improve the therapeutic effect in the treatment of congenital duodenal obstruction. Laparoscope has the value of small incision, micro-invasion, better recovery in diagnosis, and treatment for congenital duodenal obstruction. The laparoscopic methods can be performed in neonates securely and appropriated for a full-term newborn with tolerance CO2 pneumoperitoneum.
TRANS-UMBILICUS LAPAROENDOSCOPIC SINGLE-PORT SURGERY IN TREATMENT OF MECKEL'S DIVERTICULUM IN CHILDREN
Ojective: To study the clinical value of trans-umbilicus laparoendoscopic single-port surgery in treatment of Meckel's diverticulum in children.
Methods: A total of 20 infants with Meckel's diverticulum were treated with trans-umbilicus laparoendoscopic single-port surgery during April 2010 to September 2012.
Results: Surgical procedure was done for all children. The average operational time was 90 min. The post-operative hospitalization was 5 days. After three to sixteen months followed-up, there were no complications and recurrence occurred.
Conclusion: Trans-umbilicus laparoendoscopic single-port surgery for treating Meckel's diverticulum in children is a safe, minimally invasive operation with little injury. It should be recommanded in pediatric surgery.
PREFORMED SIS (SINGLE INCISION SURGERY) PORT: ADVANTAGES IN MAJOR MININVASIVE SURGICAL PROCEDURES
Introduction: The single incision surgery (SIS) is the last challenge of mininvasive surgery in pediatric population. In patients with major surgical problems it could represent a valid alternative to conventional miniinvasive or videoassisted techniques. We report our recent experience.
Materials and Methods: From January 2010 to January 2012 we have performed 20 SIS procedures; 7 of those patients (3 female and 4 male, aged between 2 and 16 years) were affected by major surgical disease. They were: 2 cases of ileo-ceco-colic stenosis in Crohn disease; 1 vaginal agenesis in Rokitansky syndrome; 3 non functioning kidneys (1 pelvic ectopia); 1 rare large renal tumour. The SIS technique was applied as laparoscopic or retroperitoneoscopic procedures. The SIS port was placed through the umbilical scar for bowel preparation and ileo-cecal resection in Crohn disease; in the left iliac fossa for vaginal reconstruction as auxiliary minilaparotomy to insert the distal part of the circular stapler, in the retroperitoneal space for nephrectomy and renal biopsy. In all these patients pre-incision local analgesia at the level of the SIS access was achieved with 2% mepivacaine.
Results: All the SIS procedures were completed without conversion, no intraoperative or postoperative complications occurred. The mean operative time (113 minutes) was acceptable according to the major procedures. We didn't find technical difficulties, at the opposite in these selected cases the SIS access avoided the need of an additional laparotomic incision. Afterwards the presence of the SIS port, instead of a mini surgical opening, allowed pneumoperitoneum maintenance for further mininvasive steps. The postoperative management was uneventful, characterized by low need of analgesia, fast bowel movements, short hospital stay (range: 2–6 days). The patients submitted to ileo-cecal resection for Crohn disease and sigmoid vaginoplasty had a very satisfactory postoperative course with bowel opening to air since the second day. In nephrectomies the recovery was faster.
Conclusion: The conventional preformed SIS port requires a 2 cm incision, but it represents a valid access to carry out major surgical operations. It allows complex procedures such as intestinal resection, anastomosis, vaginal substitution using also mechanical sutures, moreover the extraction of any size specimens results easy and safe. In major mininvasive abdominal surgery the SIS port gives the advantage to maintain pneumoperitoneum and have a better working space for subsequent laparoscopic steps. The operative time and the postoperative recovery seems to be very satisfactory.
TROCAR-LESS SINGLE INCISION LAPAROSCOPIC SURGERY: FEASIBILITY FOR PEDIATRIC APPENDECTOMIES
Background: Single incision laparoscopic surgery for appendectomy has recently been accepted widely. We started a single trocar laparoscopic surgery (STLS) in 2007 (presented at IPEG2009), and a trocar-less single incision laparoscopic surgery (TLSIS) in 2009 (presented at IPEG2011). We report our experience using the STLS and TLSILS techniques for appendectomies in the pediatric population.
Methods: A retrospective chart review was performed on our patients to undergo appendectomies with STLS or TLSILS or traditional three-trocar laparoscopic appendectomy (LAP) at Kinki University Hospital.
Results: A total of 88 patients underwent appendectomy. 34 patients were done by STLS, 31 patients by TLSILS, and 23 patients by LAP. Perforated appendicitis was seen in 8 patients of STLS group, 8 of TLSILS group, and 6 of LAP group. Wound infection was seen in only two patients of STLS. There was no difference in hospital stay.
Conclusion: Our trocar-less single incision laparoscopic appendectomy is safe and effective in pediatric population. Larger studies and further technical implements will be necessary to assess the true benefit of this procedure.
LEARNING CURVE AND INITIAL EXPERIENCE WITH LAPARO-ENDOSCOPIC SINGLE SITE (LESS) OVARIECTOMY USING A MULTITROCAR PORT, ANGLED TELESCOPES AND ARTICULATING INSTRUMENTS IN THE DOG
Objective: To define the learning curve, describe the surgical technique and evaluate the outcome for dogs that had a Laparo-Endoscopic Single Site (LESS) ovariectomy using a commercially available multitrocar port with articulating instruments and a 30 degree angled telescope in dogs.
Design: Retrospective case series.
Animals: 25 client-owned dogs.
Procedures: A commercially available multitrocar port was inserted into the abdomen through a 15–20 mm incision at the umbilicus. A LESS ovariectomy was performed bilaterally using a multitrocar port, articulating graspers, a bipolar vessel-sealing device and a 300 telescope. The excised ovarian tissue was removed through the multitrocar port incision between ovaries.
Results: Twenty-five dogs had a LESS ovariectomy. Median body weight was 20.3 kg (range, 3.5–41 kg). Median surgical time was 30 minutes (range, 15–90 minutes). Median patient age was 334 days (range, 184–2913 days) For a single surgeon; a Chomsky learning curve revealed that after the 12th procedure the surgeon would reach 90% of the fastest time expected (p=0.046) with a 95% confidence interval (0.26,24.1). Complications included minor hemorrhage due to a splenic laceration for dog #13 and one incisional infection postoperatively in dog #14. All patients were discharged from the hospital.
Conclusions and Clinical Relevance: The learning curve for the LESS ovariectomy is short and definable. Although the procedure is safe, caution should be taken to avoid splenic trauma during multitrocar port insertion.
EVALUATION OF THE SINGLE PORT ACCESS GASTROPEXY AND OVARIECTOMY USING ARTICULATING INSTRUMENTS AND ANGLED TELESCOPES IN DOGS
Objective: To describe the technique and evaluate the outcome for dogs that had a single port access gastropexy and ovariectomy (SPAGO) using a commercially available multitrocar port.
Design: Retrospective case series.
Animals: 18 client-owned dogs.
Procedures: A commercially available multitrocar port was inserted into the abdomen lateral to the rectus abdominus muscle and 2–5 cm caudal to the right rib. Dogs were tilted 45 degrees and an ovariectomy was performed bilaterally using articulating graspers, a bipolar vessel sealing device and a 300 telescope. The laparoscopic assisted incisional gastropexy was performed post-ovariectomy at the multitrocar port insertion site by grasping the antral portion of the stomach with a 10 mm DuVall forcep and suturing the seromuscular layer of the antral region of the stomach to the transversus abdominus muscle.
Results: Eighteen dogs met the inclusion criteria and were included in the study. Median weight was 34,5 kg (range 14.7–59.2 kg). Median surgical time for the SPAGO was 65 minutes (range, 50–225 minutes). Intraoperative complications included, incorrect multitrocar port placement location (3) and mild hemorrhage from a splenic laceration (1). All dogs recovered from surgery and were discharged from the hospital.
Conclusions and Clinical Relevance: Single port access gastropexy and ovariectomy is a feasible procedure to provide prophylaxis against gastric dilation-volvulus and a simultaneous means of sterilization in female dogs. Careful and accurate initial multitrocar port insertion is necessary to have optimal operative visualization as well as to reduce the chances of inadvertent splenic laceration.
SINGLE-INCISION LAPAROSCOPIC ROUX-EN-Y HEPATICOJEJUNOSTOMY FOR CHILDREN WITH GIANT CHOLEDOCHAL CYSTS
Background: Conventionally, giant choledochal cyst (CDC) is thought to be a challenge for one-stage laparoscopic definitive surgery. The current study is the first series to evaluate the safety and efficacy of single-incision laparoscopic hepaticojejunostomy (SILH) for children with giant CDCs.
Methods: Seventeen patients with giant CDC underwent SILH between April 2011 and November 2012. A vertical umbilical skin incision was made. An extra-long 5-mm 30° laparoscope was inserted through camera port which was placed in midline fascial incisions. Two 3-mm conventional laparoscopic instruments were inserted through working ports which were placed bilateral to camera port at the ends of horizontal umbilical incision. With laparoscopic guidance, the anterior cyst wall was punctured extra-corporeally by 20-gauge angiocatheter or intra-corporeally by a 3 mm electrocautery. The cyst was then evacuated by suction to create the working space. A series of retraction sutures were placed through abdominal wall and 1) serosa of gallbladder fundus; 2) proximal common hepatic duct; 3) mid-portion of anterior cyst wall; and 4) distal portion of anterior cyst wall. The assistant adjusted the strength and direction of suture retraction extra-corporeally to facilitate dissection and anastomosis. The distal stumps were left unligated because distal common bile ducts were stenotic in all patients. Ductoplasties were performed in patients combined with hepatic duct strictures. Roux loop formation and hepatojejunal anastomosis was carried out. Early postoperative and follow-up results were compared with those of our historical controls.
Results: Two patients (an 8.5-year-old girl and a 9-year-old boy) converted to 4-port laparoscopic hepaticojejunostomies for difficult dissections and bleedings induced by severe infections and dense adhesions. SILH was successfully completed in 15 patients (F/M: 9/6, Todani's classification: Type IV/I: 7/8). Twelve patients presented jaundice and additional one presented vomiting. All patients were cystic dilatations (diameter: 10–11.5 cm; length: 10–13 cm). Six patients (40%) combined with common hepatic duct strictures, which were corrected by ductoplasties. Protein plugs were detected in 7 patients (46.7%) and completed removed by saline irrigations. The mean age at operation was 3.8 months (1.5–10 months), significantly younger than 6.3 months (28 days-9 months) in our historical control group who underwent conventional laparoscopic hepaticojejunostomy (CLH)1 (p<0.01). The diameter of anastomotic stoma was 1–1.5 cm. The mean operative time was 3 hours, significantly shorter than 6.3 hours in CLH in our previous study1 (p<0.001). No blood transfusion was required. Postoperative hospital stay, resumption of feed, duration of drainage in SILH were 5.40, 2.33 and 2.93 days respectively, which were comparable to or faster than those in our historical controls1 (p=0.85, <0.001, 0.58 respectively). The median follow-up period was 7 months. No mortality or morbidities of anastomotic stenosis, bile leak, intrahepatic reflux, cholangitis, pancreatic leak, pancreatitis was observed. Liver function parameters normalized postoperatively (p<0.001).
Conclusions: With case accumulation and technical improvement, SILH is safe and obtains comparable or even better short-term results compared to our previous CLH outcomes for huge CDCs.
Reference: 1. Li L et al. Laparoscope assisted resection of huge choledochal cysts. J Clin Pediatr Surg 2003;2 (4): 250–252.
SINGLE INCISION LAPAROSCOPIC ILEOCECECTOMY FOR PEDIATRIC CROHN'S DISEASE
ABSTRACT WITHDRAWN
THORACOSCOPIC REPAIR FOR CONGENITAL DIAPHRAGMATIC HERNIA IN CHILDREN
Introduction: Congenital diaphragmatic hernia are traditionally treated by open techniques via laparaotomy or Thoracotomy. Minimally inasavive surgey for repair of congenital diaphragmatic hernia has been described. The aim of this study is to present our experience of repair of congenital diaphragmatic hernia using thoracoscopic technique.
Materials and Methods: The medical records of all cases who underwent thoracoscopic repair for congenital diaphragmatic hernia in past five years was retrospectively reviewed. The surgical procedure was performed with three 5 mm instruments and scope. Diaphragm defect was repaired by placement of thoracoscopy.
Results: 43 children were underwent thoracoscopic repair for congenital diaphragmatic hernia. Their age ranged from 2 days to 7 days. All patients were symptomatic disease at the time of surgery. Average operating time were 135 minutes, all cases were completed successfully using minimal invasive surgery. Chest drain was remained 3 to 5 days, there was no recurrence of diaphragmatic hernia, however, one case was operated because of malrotation post-operation, one cases was re-done laparaotomy for intestinal atresia.
Conclusion: Thoracoscopic repair for congenital diaphragmatic hernia in children is feasible, safe and effective alternative for open surgery. It offers patients less pain, faster recovery and good cosmosis. However, other abnormalities should be concerned at the same time.
NEUROENDOSCOPY FOR THE TREATMENT OF OBSTRUCTIVE HYDROCEPHALUS AND INTRAVENTRICULAR ARACHNOID CYSTS IN CHILDREN
ABSTRACT WITHDRAWN
COMPARISON OF LAPAROSCOPIC WITH OPEN SPLENECTOMY FOR IDIOPATHIC THROMBOCYTOPENIC PURPURA IN CHILDREN
Objective: To explore clinical results of laparoscopic splenectomy (LS) and open splenectomy (OS) in children patients with idiopathic thrombocytopenic purpura (ITP).
Methods: From January 2003 to February 2012, 30 splenectomy cases have been done in ITP children, including 12 cases of LS (LS group); OS 18 cases (OS group). LS group of 12 patients, 7 males and 5 females; aged 5 to 13 years, an average of 8.2 years; average spleen size of 10 cm×6 cm×4 cm; history of seven months to six years, with an average of 2.2 years. OS group, 18 patients, 11 males and 7 females; ages 5 to 12 years, an average of 9.5 years; spleen size is an average of 11 cm×7 cm×4 cm; history of eight months to six years, an average of 2.9 years. Two groups of preoperative platelet count were (24±10)×109/L and (33±15)×109/L. Two groups of cases choice no obvious difference. All of the patients were diagnosed by bone marrow biopsy, pathologic examination. The treatment effect of internal department for more than half years were disappointing, splenectomy were selected.
Results: LS group and OS group operation were successful, the LS group all children are fully implemented laparoscopic surgery, without conversion to open a case. Two groups operative time are (118±45) min and (140±28) min, LS group is shorter than the OS group; During the operation, the amount of bleeding were (26.67±26.4) ml and (43.18±18.7) ml. LS group amount of bleeding less than OS group (LS group bleeding amount is less than that of OS group); group LS and group OS with accessory spleen discovery rates were 50% (6/12) and 44% (6/16), the difference between the two groups was not statistically significant. The diet of postoperative recovery time average about 2 day and 2.5 days, the average hospital stay was 8.5 d, 11.5 d, LS group recovery was significantly faster than the group OS; complication rate: LS group were no complications occur, the OS group 1 patients appear incision subcutaneous fat the liquefaction (5.5%, 1/18), recovered after treatment. Two groups of treatment effect: after one weeks of platelet number rose to (458±246)×109/L and (411±136)×109/L, postoperative efficient LS group was 91.67% (11/12), OS group was 94.44% (17/18), long-term follow-up found with ITP treatment efficiency: LS group was 80% (8/10) the OS group 75% (12/15), the difference was not statistically significant (P>0.05). The effect of poor children with platelet count also increased compared with the preoperative significant bleeding does not occur again.
Conclusions: 1. The effciency of LS and OS for treating ITP is similar. The two operation methods can be used as an effective treatment of ITP treatment measures, the treatment effect is independent of the surgical approach. 2. Compared with OS, Laparoscopic splenectomy has advantages of micro-invasion, fewer complications, safety and quick recovery in the treatment of ITP, and is worthy of generalization and application. 3. LS is safe and effective for the treatment of children's ITP, may take the place of OS as a measure of the treatment of children with ITP.
SINGLE-PORT LAPAROSCOPIC APPENDECTOMY IN CHILDREN: COMPARISON WITH CONVENTIONAL LAPAROSCOPIC APPENDECTOMY
Purpose: Less postoperative pain, shorter hospitalization, faster recovery of the bowel function, and cosmetic benefit over the open approach, these advantages lead laparoscopic appendectomy (LA) to be the first choice when acute appendicitis is diagnosed by pediatric surgeons. Moreover, with improvement of the laparoscopic instruments and particularly the technique handled by the surgeons, single-port laparoscopic appendectomy (SPLA) has been popularized recently. We aimed to elucidate its potential advantages by comparing two groups of pediatric patients with acute appendicitis who accepted SPLA and conventional tri-port laparoscopic appendectomy (TPLA) separately.
Methods: Pediatric cases of acute appendicitis being treated in Xinhua Hospital, Shanghai Jiaotong University School of Medicine, from January 2009 to December 2011 were reviewed retrospectively. To minimize the technical difference among operators, all cases being chosen were operated by the same surgeon who performed most amount of LA. The items being compared include age, time due between onsets of the abdominal pain to operation, operative time, length of stay, and pathological type of the appendicitis.
Results: 116 patients of acute appendicitis were included in this study. There were 69 cases in the TPLA group and 47 cases in the SPLA, with a mean age of 7.26 yrs in the TPLA group and 6.83 yrs in the SPLA group. Mean time dues between the onsets of the abdominal pain to operation were 19.67 hrs in the TPLA group and 16.81 hrs in the SPLA group. No statistic differences had been found between these two groups before operation. Mean operative time was 41.13 mins with its mean hospital stay of 4.70 days in SPLA group. Comparing to those (37.39 mins, 5.33 days) in TPLA group, no statistic differences had been found. Further more, there is no difference between these two groups comparing their pathological type by square test.
Conclusion: Single-port approach is feasible and safe for laparoscopic appendectomy in children. The true benefit of the technique should be assessed by randomized controlled trials.
SINGLE-INCISION PEDIATRIC ENDOSURGERY (SIPES) FOR OVARIAN PATHOLOGY
Background and Objectives: Despite being pioneered by gynecologists, single-incision endosurgery has not been widely reported for the treatment of ovarian and adnexal pathology in neonates, children, and adolescents. We describe our initial experience using single-incision pediatric endosurgery (SIPES) for these indications and discuss advantages and drawbacks.
Methods: All children who underwent SIPES with a preoperative diagnosis of ovarian or adnexal pathology were included in the study. Data on age, operative time, complications, length of hospital stay, and outcomes were collected.
Results: From January 2010 until January 2012, 20 girls (median age 11.1 years, range: 6 days to 20 years, weight range 4.0 to 90 kg) underwent SIPES procedures for ovarian or adnexal diagnoses, including hemorrhagic/follicular/paratubal cysts (n=9), torsion (n=7), tumor (n=3), and parauterine cyst (n=1). The operations included cyst unroofing (n=4), detorsion and oophoropexy (n=7), (salpingo) oophorectomy (n=5), marsupialization of cyst (n=3), and cyst aspiration (n=1). Median operative time was 41±30 minutes; there were no conversions to conventional laparoscopy or open surgery. Sixteen patients (80%) were discharged within 24 h after the procedure. There were no peri- or postoperative complications. Histopathology showed hemorrhagic/follicular/paratubal cyst (n=8), necrotic/calcified ovarian tissue after torsion (n=6), cystadenofibroma (n=1), granulosa cell tumor (n=1), and mature teratoma (Grade 0) (n=1).
Conclusion: SIPES is an excellent alternative to conventional laparoscopy for the treatment of adnexal pathology. Using a single umbilical incision that can be enlarged instead of 3 smaller trocar sites facilitates the resection and extraction of ovarian masses without compromising cosmesis.
A COMPARISON BETWEEN OPEN SURGERY AND LAPAROSCOPIC SURGERY FOR POSTOPERATIVE ADHESIVE INTESTINAL OBSTRUCTION IN CHILDREN
Purpose: Postoperative adhesive intestinal obstruction sometimes requires surgical intervention. The laparoscopic release of adhesive intestinal obstruction was first reported in 1991. The latter procedure not only is less invasive, but also it reduces complications, decreases postoperative pain, and reduces the operative duration and length of admission. However, in some cases such as diffuse adhesions and delamination damage of organs, it is necessary to perform traditional open surgery. We performed a retrospective study on postperative adhesive intestinal obstruction in 30 patients comparing open surgery with laparoscopic surgery.
Methods: The medical records of all patients admitted to our hospitals between January 1994 to October 2012 with the diagnosis of adhesive intestinal obstruction were reviewed retrospectively. Of these 30 patients, 12 patients underwent open surgery and 18 patients underwent laparoscopic surgery. The analyzed factors were sex, original diagnosis, the age when the procedure for adhesive intestinal obstruction was done, decompression of bowel before operation, operation time, postoperative period until first oral ingestion, duration of hospitalization and bowel resection. In addition, we analyzed the rate and the reason for conversion to open surgery.
Result: The most common original diagnosis causing adhesive intestinal obstructions was Hirschsprung's disease (13.3%), followed by congenital diaphragmatic hernia (10.0%), Wilms tumor (10.0%), esophageal hiatus hernia (10.0%), intestinal perforation (6.7%), and post V-P shunt (6.7%). The average age at which the laparoscopic procedure for adhesive intestinal obstruction was performed, was significantly older than the age at which the open procedure was performed (123.9 months old vs. 50.9 months old, p<0.05). While decompression of bowel was performed in 75% of patients before open surgery for the obstruction, it was performed in all patients before laparoscopic surgery. Operation time (p=0.90), postoperative period until first oral ingestion (p=0.12) and duration of hospitalization (p=0.38) tended to be shorter in those who underwent the laparoscopic procedure. Most of the cases of bowel resection were done with open surgery, except for one. In 5 of the 18 patients, laparoscopic surgery was converted to laparoscopy-assisted surgery or open surgery. The main reason for these conversions was limited operation space due to dilation of the intestine. No patient underwent conversion due to damage of organs by the laparoscopic procedure.
Conclusions: Laparoscopic surgery is a minimally invasive procedure for postoperative adhesive intestinal obstruction. The laparoscopic procedure is advantageous in cases of adhesion of intestinal obstruction compared with open surgery. However, it is necessary to perform open surgery in some particular cases, such as cases with limited operation space due to dilation of the intestine. Thus, we recommend performing preoperative evaluation and decompression of bowel as much as possible.
SINGLE-PORT LAPAROSCOPIC ASSISTED PERCUTANEOUS EXTRAPERITONEAL CLOSURE USING AN INNOVATED APPARATUS FOR INGUINAL HERNIA IN CHILDREN
Background: To explore the applicable effects of single-port laparoscopic percutaneous extraperitoneal closure (SPLPEC) using an innovated two-hooked core hernia apparatus for indirect inguinal hernia in children.
Methods: Between June 2008 and October 2011, 72 children with indirect inguinal hernia received SPLPEC procedures with an innovated two-hooked core hernia apparatus. Without assistant working port, SPLPEC using the two-hooked core hernia apparatus could be readly kept in an identical subcutaneous path for introducing and withdrawing the suture, the extraperitoneal knot-tying could tautly enclose the hernia defect without peritoneal gaps and upper subcutaneous tissues. During the same period, 63 children with inguinal hernia underwent SPLPEC with a single hook-pin device that is slightly modified from LPEC needle (control group). Technical essentials, mean operation time, intra- and postoperative complications were compared.
Results: The internal orifice of the hernia sac was closed faster by SPLPEC with an innovated two-hooked core apparatus than the single hook-pin (unilateral: 13.21±3.86 vs. 17.92±4.37 minutes, P<0.05; bilateral: 17.18±4.69 vs. 25.36±7.38 minutes, P<0.01). There were no postoperative complications or evidence of early recurrence in the two-hooked core apparatus group. The median hospital stay or recovery was similar to the control group. However, one recurrence and one subcutaneous ligature abscess were postoperatively observed in control group. Cosmetically, SPLPEC proved to be an excellent procedure because the surgical scar was hidden within the umbilicus.
Conclusion: SPLPEC with the two-hooked core hernia apparatus proves to be a successful procedure and the median operative time is short compared to control group. It is safe, feasible and lends to quick recovery for inguinal hernia in children.
SINGLE-PORT LAPAROSCOPIC SPLENECTOMY: THE 256-SLICE CT FOR PREOPERATIVE EVALUATION IN CHILDREN
Objective: To evaluate the 256-slice spiral computed tomography for determination of splenic volume, splenic vascular anatomy and presence of accessory spleens in children who were undergoing single-port laparoscopic splenectomy (SLS).
Methods: Between October 2010 and November 2012, 18 children with various hematologic and autoimmune disorders who were candidates for SLS underwent the 256-slice spiral CT that included examination of the anatomic type of splenic pedicle, the adjacent relationship between the splenic vessel and pancreas, splenic volume, and presence of accessory spleens. An individual SLS could be performed according to the anatomic parameters of spleen provided by preoperative CT in each patient. The parameters were recorded by telerecording during SLS and compared with those by preoperative CT using Chi-square test.
Results: Two anatomic types of spleen pedicle and two different adjacent relations between splenic vessels and pancreas were detected by CT. There were no difference between the indexes by CT and those by SLS, including the anatomic types (X2=0.8, P>0.05) and the adjacent relations (X2=1.9, P>0.05). SLS was successfully performed following the anatomic information provided by preoperative CT. Especially, CT angiograms correctly showed polar vessels in all cases.
Conclusions: The 256-slice spiral CT volumetric and anatomic evaluation provided accurate and reproducible information. The individual SLS route and schedule can be successfully determined on the basis of various kinds of reproducible anatomic frameworks of the spleen provided by preoperative CT.
LAPAROENDOSCOPIC SINGLE SITE (LESS) PARTIAL NEPHROURETERECTOMY FOR UPPER URINARY TRACT DUPLICATION ANOMALIES: INITIAL EXPERIENCE
ABSTRACT WITHDRAWN
PEDIATRIC LAPAROENDOSCOPIC SINGLE SITE (LESS) ORCHIDOPEXY: COMPARISION TO CONVENTIONAL LAPAROSCOPIC ORCHIDOPEXY
ABSTRACT WITHDRAWN
SINGLE-INCISION MULTIPORT LAPAROENDOSCOPIC (SIMPLE) PROCEDURES IN ADNEXAL SURGERY IN PEDIATRICS: VIDEO
Objective/Purpose: The aim of this video is to describe the technical details of SIMPLE using standard instruments in the treatment of adnexal cysts/gonadal disorders.
Methods: Procedures included treatment of adnexal pathology requiring an specimen removal: 5 complicated ovarian cysts diagnosed in perinatal period, 4 fallopian tube cysts in adolescents and 4 bilateral gonadectomies in patients with DSD. Patients age ranged from 8 days to 16 years and weight from 3 to 47 kg. Procedures included laparoscopic oophorectomy in 4, fallopian tube cyst resection in 4, bilateral gonadectomy in 4 and ovarian cystectomy in 1. We used a 4 or 5 mm 30-degree 18 to 29 cm long lens and 1 or 2 3 or 5 mm standard laparoscopic ports. Different models and lengths were combined to avoid collision. The operating scope was placed through a transumbilical incision and the ports or isolated instruments were placed around the umbilicus using the same skin incision. Different directions were used depending on the affected side. A percutaneous hypodermic needle was used in an infant for retraction. A 3 mm bipolar forceps or a 5 mm bipolar sealer were used depending on the age of the patients. Specimens were removed through the umbilical incision cutting the fascial bridge left between 2 of the 3 punctures.
Results: All procedures were completed successfully by the senior fellow assisted by the senior author without need for conversion to standard laparoscopy or open surgery. There were no operative or postoperative complications. The median operative time was 80 min (range 45–100). The median postoperative hospital stay was 1 day (range 1–3 days).
Discussion: Encouraged by this initial experience which probed to be safe, reasonable, easy to learn and without extra cost we are planning to include adnexal surgery in the list of procedures for training in SILS in the context of a prospective randomized trial.
SINGLE INCISION LAPAROSCOPIC EXCISION OF PEDIATRIC SOLID TUMORS
Introduction: Single incision laparoscopic surgery (SILS) has been utilized for a wide range of pediatric surgical conditions with equivalent clinical outcome and superior cosmetic results. Most of the procedures reported involved basic laparoscopic procedures. We report our mini-series of pediatric solid tumor resections with the SILS technique.
Patients and Methods: A prospectively collected SILS database was reviewed and patients with solid tumors were identified. Data was recorded on patient demographics, intra-operative findings and postoperative outcomes. Surgical techniques to facilitate the SILS procedures will be discussed for each patient.
Results: Three boys underwent SILS resection for solid tumors (Table). All cases were performed by two attending surgeons using the Gelpoint Device (Applied Medical, Rancho Santa Margarita, CA). There were no intra-operative or postoperative complications. Resection margins were negative for the hepatic and pancreatic tumors and neither patient required adjuvant therapy. The patient with neuroblastoma also had lymph node sampling which were positive, thus he received chemotherapy per protocol.
Conclusions: SILS can be applied to the resection of pediatric solid tumors successfully. Patient selection and adherence to oncologic surgical principles are of the utmost importance.
SINGLE INCISION LAPAROSCOPIC APPENDECTOMY (SILS-A) IN CHILDREN WITH COMPLICATED APPENDICITIS (CA)
Background: SILS-A in children is an emerging approach recently demonstrated in a prospective randomized trial to have similar outcomes (post-op wound infection and abscess) compared to standard 3 trocars laparoscopic appendectomy for simple appendicitis (SA) despite longer operative time and higher surgical difficulty with a higher conversion rate. Outcomes of patients with CA (gangrenous appendix, perforation, phlegmon, abscess and peritonitis) managed by SILS-A may even be worse due increased technical difficulty. The objective of this study is to compare the outcome of patients with CA managed in 2 time periods by a single surgeon - Jan 2010 to May 2011(Period A before SILS-A) and June 2011 to Nov 2012 (Period B after SILS-A).
Methods: This is a retrospective study of all patients undergoing surgery for appendicitis by a single surgeon between Jan 2011 to Nov 2012. Prior to June 2011, the three trocars laparoscopic technique was the method of choice for appendectomy in patients with simple and complicated appendicitis. After June 2011, SILS-A became the preferred surgical method. The primary outcome variables were postoperative infection (wound infection and abscess), operative time, and length of hospital stay, conversion rate and OR supply charges. Various methods were used for the SILS-A. In most cases the appendix was mobilized outside of the umbilical incision and resected externally. All patients with CA were treated with the same antibiotic regimen in the post-operative period.
Results: During the study period, 159 patients underwent appendectomy for suspected appendicitis, two of whom did not have appendicitis. Ten other patients underwent interval appendectomy for medically treated appendicitis. These 12 patients were excluded from our analysis. Patients' demographics and outcomes in the 2 study periods are summarized in the table below.
No infectious complications were seen in this series with a follow-up ranging from 24 months to 2 weeks. There were 2 conversions in from SILS-A to standard laparoscopic approach. One patient had a retrocecalphlegmon/abscess with a very friable cecum that cannot be mobilized with SILS-A technique requiring insertion of a 5 mm port in the suprapubic location to complete the operation. The second conversion involves a small child (18.5 kg) whose appendix was necrotic with appendiceal base involvement. Two extra 5 mm trocars were placed to facilitate a partial cecectomy. This patient developed a bowel obstruction 4 days after discharge requiring an operation for adhesiolysis.
Conclusion: SILS-A is a safe method for surgical treatment of complicated appendicitis with similar outcomes compared to standard 3 trocars technique and conversion rate is low. In the current series, the OR supply charge is significantly lower associated with the SILS-A technique due to the lack of stapler usage.
LAPAROSCOPIC SINGLE PORT CECOSTOMY BUTTON PLACEMENT FOR CHRONIC SLOW COLONIC TRANSIT CONSTIPATION IN CHILDREN
Background: Antegrade continence enema (ACE) using the appendicostomy was first described for the treatment of stool incontinence in children with spina bifida. Subsequently it has been used in the treatment for constipation with good results. The same can be achieved with a minimally invasive cecostomy placement. We describe our technique of single port laparoscopic cecostomy for slow transit constipation in children.
Purpose: To retrospectively report our technique of single port laparoscopic cecostomy for slow transit constipation in children.
Material and Methods: The records of 10 children (Median age 9 yrs) with chronic slow transit constipation who underwent laparoscopic cecostomy placement over a period of 3.5 years (April 2009 to Oct 2012) were retrospectively reviewed. All patients had manometric evaluations of the colon, contrast enema and marker studies.
Technique: The patient was laid in a supine position and the abdomen was painted and draped. An incision was made in the scar of the umbilicus and a 5 mm step trocar was introduced using the modified Hasson's technique. A 5 mm 30 degree telescope was used for visualization through this port. A suitable site was chosen for cecostomy placement in the right lower quadrant and under laparoscopic visualization 4 ‘T’ Fastners were placed into the cecum percutaneously. A skin incision was then placed at the neo-cecostomy site and a needle was placed through this incision into the cecum exactly into the center of the square formed by the 4 ‘T’ fastners. Satisfactory position of the needle within the cecum was confirmed using water soluble contrast material. A guide wire was placed through the needle in to the cecum and a serial dilator peel away sheath combination was advanced over the wire. The serial dilator was then removed and the peel away sheath left in situ. An appropriate size Mickey button (Kimberly Clarke) was introduced through the peel away sheath and the peel away sheath was removed. The 4 ‘T’ Fastners were then tied subcutaneously pexing the cecum to the anterior abdominal wall. The cecostomy button was left to gravity drainage for 48 hrs and cecostomy washouts are started after 2 days.
Results: All patients tolerated the procedure well. None had any intra or postoperative complications. The patients were followed up by GI and surgical teams at regular intervals. One patient needed subsequent conversion to an ileostomy since she also had small bowel motility disorder. The other 9 patients did well after the cecostomy button and were free of constipation with one washout a day until last follow up (Median 1.8 yrs). One of the 9 patients was able to evacuate spontaneously without cecostomy washout after one year of continuous treatment and had her cecostomy removed.
Conclusion: Laparoscopic single port cecostomy button placement for chronic slow colonic transit constipation in children is a safe and effective technique. Laparoscopy provides excellent visualization and fluoroscopy confirms placement into the cecum. The procedure has minimum complications and is easily reversible.
UMBILICAL INCISION/ACCESS AND SUBSEQUENT RECONSTRUCTION OF THE UMBILICUS DURING SINGLE INCISION LAPAROSCOPIC SURGERY (SILS) IN CHILDREN: HOW TO GET A NORMAL LOOKING UMBILICUS
Background: Single port surgery is now being commonly used for the surgical procedures in children. One of the major advantages of this approach is to be able to hide the scar within the umbilical ring without altering the anatomy of the umbilical ring.
Purpose: To report and share our technique of umbilical incision/access and subsequent reconstruction of the umbilicus to get excellent cosmetic results during single port laparoscopic surgery in children.
Over the past 3.5 years more than 200 single port laparoscopic surgeries have been performed at our institution by a single surgeon. The technique we have used for umbilical access to the peritoneal cavity and subsequent umbilical reconstruction has produced a normal looking umbilicus in all our patients.
Technique:
1. Opening the umbilical ring: The limits of the umbilical ring are first defined and marked using a marking pen. A vertical incision is then made passing exactly through the center of the umbilical scar. It is important to be in the center of the scar to obtain direct access into the peritoneal cavity. If you are in the center there is always a blob of fat (Umbilical fat sign) that can be used as a guide. Direct access can be obtained into the peritoneal cavity through this point. A grooved director is then used through this blob of fat to obtain access to the peritoneal cavity. The umbilical fascial incision is then extended using the grooved director on either side. A 10–12 mm incision is usually enough for single port laparoscopic surgery in children as long as you remain within the umbilical ring. Once the adequate access incision is obtained the Olympus Triport is then introduced.
2. Closure/reconstruction of the umbilicus: Once the appendectomy is done the port is withdrawn. The umbilical fascia is closed using interrupted ‘0’ vicryl sutures. Multiple sutures are used. The grooved director is used to assist closure. The umbilical ring is then approximated with 3’0’vicryl stay sutures. Dermbond glue is then used for umbilical skin closure and the stay sutures are removed.
SINGLE PORT VERSUS CONVENTIONAL LAPAROSCOPIC APPENDECTOMY: A COMPARATIVE STUDY
ABSTRACT WITHDRAWN
MULTI-CENTRE EXPERIENCE OF SINGLE INCISION LAPAROSCOPIC SURGERY (SILS) IN CHILDREN
ABSTRACT WITHDRAWN
REDUCED PORT SURGERY - SPIN-OFF OF SILS
Aim: Single incision laparoscopic surgery (SILS) seems to be a popular alternative to conventional multiport laparoscopic surgery. We evaluated our experience of SILS and analyzed role of additioal trocar to simplify the surgery.
Methods: Since March 2009 all patients who underwent SILS were studied prospectively. The data were collected and results analyzed.
Results: Since March 2009 42 patients under went SILS. Mean age was 6 years (range 3 months–16 years). Indications were appendicectomy (26), cholecystectomy (4), fundoplication (8), nephrectomy, omental cystectomy, ovarian cyst and simple cyst of right lobe of liver (1 each). Initial 9 cases (appendicectomy 4, cholecystectomy 2, fundoplication 3) were performed by transumbilical single incision multiport technique using convention instruments. Mean operative times were prolonged compared to conventional multiport laparoscopy. The procedures appeared to be more difficult than conventional multiport technique. However addition of 1 trocar away from the umbilicus reduced the operative time significantly (62 minutes vs 107 minutes, p value<0.05) The procedures appeared easy, less demanding and reproducible.
Conclusion: Reduced port surgery as compared to SILS is easier, less demanding, reproducible and can ber performed with conventional laparoscopic instruments.
AN INSIGHT IN THE SURGERY OF TOMORROW
ABSTRACT WITHDRAWN
THORACOSCOPIC REPAIR OF DIAPHRAGMATIC EVENTRATIONS
Introduction: Surgical management for diaphragmatic eventration with plication of the diaphragm is conventionally performed via a thoracotomy which carries significant post operative morbidity and can be associated with chronic surgical pain. The minimally invasive approach to plication of the diaphragm results in quicker recovery time than traditional open techniques.
We report a 13 year surgical experience of thoracoscopic diaphragmatic eventration repair.
Patients and Methods: All operatively managed diaphragmatic eventrations presenting to our department from December 1997 to December 2010 were identified using theatre logbooks and an electronic database. Patients were determined to have diaphragmatic eventration on chest radiography with or without ultrasound. Case notes were retrospectively analysed to determine clinical presentation, aetiology and surgical approach. All documented follow up consultations were examined for evidence of symptomatic improvement, complications and recurrence.
Thoracoscopic plication became our first line approach in 2003 for the operative management of diaphragmatic eventration.
Results: From December 1997 to December 2010, 19 consecutive patients underwent operative repair of diaphragmatic eventration. Two patients were excluded from analysis due to incomplete data leaving 17 patients for analysis. Median follow up was 2.9 years (range, 0–7 years). Two patients underwent re-do operations, giving a total of 19 procedures; 7 left-sided and 12 right-sided. Median age at operation was 1.2 years (range, 4 days to 7 years). Sixteen patients were symptomatic. Indications for surgery were: respiratory infection (10, of which 9 were recurrent), respiratory compromise (6, of which 3 were intubated and ventilated), recurrence (2) and vomiting (1). From 1997 to 2003 diaphragmatic plication was predominantly performed using an open approach: thoracotomy (4), laparotomy (3), and thoracoscopic (1). From 2003, 10 out of 11 procedures were completed thoracoscopically. One patient underwent a laparotomy and Ladds procedure for concurrent malrotation. Chest drain was used in 3 out of the 11 thoracoscopic procedures.
No recurrence was observed following thoracoscopic plication. There were recurrences in 2 patients who underwent plication via laparotomy. Both recurrences were successfully repaired, one thoracoscopically and the other at the same time as an open fundoplication and gastrostomy via a second laparotomy. Four patients had costal flaring on long term follow up.
All symptomatic patients displayed improvement post-operatively. All ventilated patients were successfully extubated within a week of surgery. Nine patients (82%) were discharged within 3 days following thoracoscopic repair (median 1; range, 1–94 days). Two patients had multiple comorbidities requiring extended stay following thoracoscopic plication. Median length of stay for following open repair was 7.5 days (range, 5–18 days).
Conclusions: Our evolving surgical experience provides further evidence that thoracoscopic plication for diaphragmatic eventration results in excellent outcomes with minimal morbidity and short hospital stay. Diaphragmatic eventration should be repaired in symptomatic patients. We advocate using a three port totally thoracoscopic technique without the need for chest drains or single lung ventilation.
THORACOSCOPY ASSISTED MINIMALLY INVASIVE NUSS PROCEDURE FOR CHILDREN WITH CONCOMITANT PECTUS EXCAVATUM AND CONGENITAL HEART DISEASE
Objective: To investigate the feasibility of minimally invasive Nuss procedure in pediatric patients with concomitant anomalies of congenital heart disease (CHD) and pectus excavatum (PE).
Methods: We included 15 patients with concomitant CHD and PE, who were treated at our institution from June 2008 to June 2012. Eight of them, including 5 males and 3 females with an average age of 6 years and 1 month (range: 4 years to 13 years and 4 months), received cardiac operation and Nuss procedure simultaneously. Four patients underwent minimally invasive surgical closure of ventricular septal defect (VSD) with Amplatzer device, 2 patients with atrial septal defect (ASD) were implanted with the same device, one received VSD repair under cardiopulmanory bypass (CPB), and the other one had VSD and double-chambered right ventricular repair under CPB. The other 7 patients received Nuss procedure after cardiac operation. They were 5 males and 2 females, with an average age at cardiac operation of 1 year and 9 months (range: 6 months to 3 years and 10 months) and an average age at Nuss procedure of 6 years and 2 months (range: 4 years and 7 months to 8 years). Six of the 7 patients had VSD repair under CPB, and the other one had correction of TOF. Chest tube and/or pericardium and mediastinum tube were placed before closing routinely.
Results: All the patients went through the operations well. The 8 patients receiving simultaneous correction were extubated 5–14 h (mean 8.75±2.59 h) after operation, and the 7 patients receiving staged procedure were extubated in 4–8 h (mean 5.86±1.24 h). Tubes in pericardium, mediastinum or chest were removed 48–72 h later. No major complications such as hemorrhage or impairment of thoracic organ occurred. Correction of cardiac anomalies and lung functions were confirmed by postoperative examinations. Each group had one patient with delayed wound healing and both recovered well after proper treatment. Good results were seen in all the patients in 6 months to 4 years of follow-up.
Conclusions: Nuss procedure is safe and feasible in correction of PE after cardiac operation, as well as performed simultaneously with cardiac operation in clinically needed pediatric patients.
THORACOSCOPY ASSISTED MINIMALLY INVASIVE NUSS PROCEDURE FOR CORRECTION OF PECTUS EXCAVATUM IN CHILDREN
Objective: To investigate the advantages of thoracoscopy assisted Nuss operation in treatment of child pectus excavatum.
Methods 406 cases, 313 boys and 92 girls (M:F=3.4:1), underwent thoracoscopy assisted Nuss operation, which aged 3 years and 6 months to 17 years 6 months (average 6 years and 9 months). Associated diseases included 9 cases of congenital heart disease and 2 cases of congenital pulmonary cyst.
Results: The operations were performed successfully and no operative mortality. The operation time was 30–85 min (average 45 min). Length of hospital stay was 5–61 d (average 10 d). The intra-operative blood loss was less than 10 ml. Early post-operative complications included: 9 cases of pneumothorax (2.2%), pleural effusion in 6 patients (1.5%), which was cured by drainage. Wound healing in 2 cases (0.5%) were cured by nutritional support. Followed up for 3 months to 6 years, 2 cases of scoliosis, 3 cases of bar migration, the patients were cured by reoperation of NUSS procedure; allergy in 2 cases (0.5%), one case improved after conservative treatment, the other cases received bar removal in advance. 154 cases (40.0%) patients had bar removal surgery. Excellent results were maintained in 387 patients (95.3%), good results in 12 (3.0%) and poor in 7 (1.7%).
Conclusions: Thoracoscopy assisted Nuss operation has many advantages such as small and masked incision, short operation time, little blood loss, quick recovery, little trauma and satisfied results. It is a safe and reliable technique for correction of pectus excavatum.
THORACOSCOPIC RESECTION OF TWO COSTAL EXOSTOSES IN A CHILD PRESENTING WITH SPONTANEOUS HEMOTHORAX
A 14-year-old boy with a genetic disorder known as hereditary multiple exostoses (HMEs) was transferred from a general hospital to our pediatric intensive care unit (PICU) with a diagnosis of spontaneous hemothorax. He suffered from left-sided chest pain and mild dyspnoe. Chest radiography showed a left pleural effusion. CT scan revealed an important hemothorax and two costal exostoses. The child underwent thoracoscopy. Hemothorax was aspirated, the two exostoses were identified, resected with an endoscopic rongeur, shaved and covered with TachoSil patch. Postoperative course was uneventfull. Chest tube was removed on the 4th postoperative day, patient was discharged on the 6th postoperative day. 18 months follow-up shows no complaints and no recurrence.
MINIMALLY-INVASIVE REPAIR FOR TYPE C ESOPHAGEAL ATRESIA IN CHINA: PRELIMINARY EXPERIENCE IN A MAJOR TEACHING CHILDREN'S HOSPITAL
Backgroud: Esophageal atresia affects about 1 in 4000 neonates. In the most common form of the disorder, the proximal esophagus ends in a blind pouch and the distal esophagus forms a tracheo-esophageal fistula (TEF) (Type C). Less common types include pure esophageal atresia (no TEF). Refinements in optical technology, instrumentation and most importantly, surgical skill, has lead to the rapid progression and evolution of minimally-invasive surgery. The use of thoracoscopy has expanded to multiple purposes in children including primary management of esophageal atresia (EA) and distal tracheoesophageal fistula (TEF)(1–3). We report our initial experience and outcomes in a major teaching children's hospital in Shanghai, China.
Materials and Methods: We retrospectively reviewed 13 cases of thoracoscopic repair of esophageal atresia performed at Shanghai Children's Medical Center from August 2006 through June 2012. twelve cases (92%) were diagnosed with standard short gap EA with TEF confirmed by chest and abdominal radiography, barium upper pouch study and intra-operative rigid bronchoscopy. There was one case of pure esophageal atresia. There were five girls and eight boys, age and weight at time of surgery ranging from 3 days to 2 months and 2300 to 3600 grams, respectively. 9/13 (69%) had associated congenital heart anomalies (non-cyanotic) demonstrated on echocardiography.
In patients with EA/TEF, our first approach was via three port (5 mm) thoracoscopy with clip ligation of the fistula and intracorporeal esophageal anastamosis. Thoracostomy was routinely performed.
In the one patient with pure EA, open gastrostomy was initially performed with the esophagus lengthened, and continuity eventually established via a modified thoracoscopic Foker procedure over 3 months. Post-operatively, all patients underwent routinely barium swallow study one week after surgery.
Patient in left decubitus position, an initial 5 mm port was placed in the fourth intercostal space, anterior axillary line. Two other working ports were placed in the third and fifth intercosal space mid to posterior axillary line.
Results: Three patients (23%) were converted to open thoracotomy repair due to difficult visualization (2), and significant intra-operative bleeding (1). Two patients (20%) had post-operative anastomotic leak which sealed uneventfully with conservative medical management including thoracostomy. Both patients had esophageal dilatation at one month after surgery and have not required subsequent dilations. The remaining ten patients have not required esophageal dilation. Mean follow-up for these patients was two years.
In the patient with pure EA, thoracoscopy including lengthening was performed three times at one month intervals with primary anastamosis performed at 3.5 months. There was no esophageal leak on swallow study post-operatively and patient has undergone esophageal dilation once. He is doing well at one year follow-up.
Conclusions: Thoracoscopic TEF repair is technically challenging, but can be performed with good surgical outcome in China. One should not hesitate to convert to traditional thoracotomy as outcome is still acceptable. Patient selection and surgeon's experience appear to play a major role in the success of thoracoscopic TEF repair.
THORACOSCOPIC REMOVAL OF A MEDIASTINAL COIN
Introduction: Although coins are the most frequent foreign bodies ingested by children, they generally pass through the alimentary canal without incident. In rare cases, coins which become lodged in the esophagus may erode through the esophagus into the mediastinum, causing complications including espohagitis, chronic suppurative mediastinitis, tracheoesophageal fistula, and fistulazation with the great vessels causing sudden death from hemorrhagic shock.
Methods: A case is presented in which a 15 month old female with complaints of several months of vomiting was found to have radiologic evidence of two coins lodged in her proximal esophagus. During upper endoscopy, however, only one coin was identified and retrieved. CT scan demonstrated that the second coin had migrated extraluminally into the superior mediastinum below the level of the clavicular heads, cephalad to the aortic arch and posterior to the brachiocephalic trunk causing displacement and intrinsic compression of the trachea. A thoracoscopic approach was used to extract the second coin without complications.
Results: The patient had no postoperative complications. She continued to experience persistent dysphagia with solid foods and had evidence of esophageal stricture on esophagram which required esophageal dilatation.
Conclusion: Historically, mediastinal foreign bodies have been managed using either a cervical approach or thoracotomy. This case report suggests that thoracoscopy is a valuable modality for retrieval of mediastinal foreign bodies in children.
EFFICACY OF VIDEO-ASSISTED THORACOSCOPIC SURGERY (VATS) IN CHILDREN WITH EARLY EMPYEMA THORACIS IN COMPARISON TO OPEN THORACOTOMY
Background/Purpose: VATS is more effective in early empyema which includes exudative and early fibrinopurulent phase. This study evaluates the role of VATS and compares the results with open decortications done during the same period for early empyema thoracis.
Methods: A prospective study was carried out over a period of 4 years (March 2008–March 2012) at a single large centre involving 274 cases of empyema thorax between ages 2 ½ months & 11 yrs (Mean age 3.8 yrs). Of these cases, 155 were male while 119 were female children. Early empyema thorax was found in 96 cases. Of these 55 were males & 41 were female children who underwent VATS. The inclusion criteria for considering as early empyema included presence of symptoms for <2 weeks, finding of loculations, absence of thickened pleura. The exclusion criteria of early empyema are symptoms >3 weeks, absence of loculations, presence of thickened pleura, previous thoracic surgery destroyed lung, diagnosed bronchopleural fistulas, or a shrunken hemithorax on CT scan. The collected data included age, clinical presentation, radiological investigation, pleural fluid analysis, intraoperative findings, histopathological findings and post operative course. The length of stay and the post-operative time taken for clinical and radiological lung expansion was compared with cases of open decortication done for early empyema during the same period.
Results: Of the 274 cases of empyema, 96 underwent VATS and open decortication in 178 children. Postoperatively patients became afebrile in 2±1.2 days in VATS and 7±3.2 days in open decortication. Clinical and radiological expansion was earlier in VATS with 3±2.1 and 6±2.2 days respectively.
Conclusions: The prospective study concludes that VATS is more effective and less invasive than open thoracotomy for early empyema thoracis in decreasing the morbidity and has better cosmoses.
PEDIATRIC THORACOSCOPIC LOBECTOMY FOR CONGENITAL CYSTIC ADENOMATOID MALFORMATION (CCAM): OUR EXPERIENCE AND A REVIEW OF THE LITERATURE
Background: Congenital cystic adenomatoid malformation (CCAM) is a subset of congenital lung malformations with a reported incidence of 0.94 per 10000 live births. The favoured surgical intervention is a lobectomy, which can be performed thoracoscopically, or via a thoracotomy. Pediatric thoracoscopic lobectomy has been gaining popularity since first reported in 1970. Technical feasibility and safety have already been established. To date, most of the reported series stem from the United States and Europe. We would like to present our series of pediatric thoracoscopic lobectomy for CCAM as one of the few from Asia and the first in the region.
Materials and Methods: We retrospectively reviewed all patients who underwent thoracoscopic lobectomy at our institution. Data in this Institutional Review Board approved study was obtained from electronic operating theatre record (OTPACS) and patients' case notes. Details included patient demographics, pre-operative presentation, operative details and post-operative follow up.
Results: A total number of 10 patients (7 boys and 3 girls) with a median age of 2.2 years (range 1.4 years to 6 years) were scheduled for thoracoscopic lobectomy within the period from March 2009 to June 2012. The median weight was 11.8 kg (range 9.4 kg to 21.1 kg). Nine patients had a diagnosis of CCAM; one was an oncology patient with right middle lobe pulmonary aspergilloma (excluded from the study). Of the patients with CCAM, 6 were diagnosed antenatally. The remaining 3 presented in early childhood with chest infection. Only 4 patients were totally asymptomatic prior to surgery.
Thoracoscopic lobectomy was attempted in all patients. Conversion to open thoracotomy was required in 3 patients; one due to intra-operative hypotension and the other two because of poor anatomical visualization. Only one of these patients had preoperative lung infection. Our operative time ranged from 124 to 384 mins (mean 236 mins, median 212 mins). All of our patients had chest tubes inserted post operatively with median chest tube duration of 4 days. The mean duration of hospital stay was 6 days (range 3–8 days).
There were 2 significant morbidities: one haemothorax requiring thoracoscopic exploration and one delayed pneumothorax requiring readmission for chest tube insertion. All patients have good cosmetic and functional results on follow up.
Conclusion: Thoracoscopic lobectomy confers the advantages of a superior cosmetic and functional results compared to open surgery. The operation is feasible with minimal morbidity. Preceding lung infection before surgery should not be a contraindication for thoracoscopic surgery. With regards to timing of surgery, factors to consider include the skill of the surgeon, risk of infection in an asymptomatic patient, preservation of long-term pulmonary function and prevailing social perceptions.
DESIGN OF MANAGEMENT FOR PRIMARY SPONTANEOUS PNEUMOTHORAX IN CHILDREN: OUR 12-YEAR EXPERIENCE
Background: As the number of patients treated by thoracoscopic stapler bullectomy increased, the postoperative recurrence rate had risen unexpectedly. Especially the rate of recurrence in children is higher than that in adults. We contrive the management of primary spontaneous pneumothorax to prevent recurrences.
Patients and Methods: From 2000 to 2012, we experienced 22 patients who had primary spontaneous pneumothorax and were operated. Medical records of 22 patients were retrospectively reviewed. We separate the patients to 3 groups. From 2000 to May 2011 we operated on with video-assisted thoracoscopic surgery (VATS) and made a wedge resection of the apical part of lung (bulla) with endostapler device and mechanical pleurodesis (group A). From July 2011 to December 2012, we used a PGA (absorbable plyglycolic acid) sheet with fibrin glue (group B), or Surgicel Absorbable Hemostat (ORC: oxidized regenerated cellulose) (group C) after bullectomy on VATS. We investigated the length of surgery, the duration of postoperative chest drainage, hospital stay after the operation and the recurrence rates.
Results: In the 12 years, we had 22 patients with spontaneous pneumothorax. Patient age ranged from 11 to 16 years old (median, 14.4). We had 18 boys and 4 girls. In group A, we had 16 patients (19 sides) and 3 patients had recurrence after operation (the recurrence rates were 15.8%). In group B, 6 patients (include 3 recurrent cases) were operated and 1 patient had recurrence (16.7%). This case was re-recurrence case. At first time, he underwent bullectomy and pleural abrasion. At second time we used PGA sheet after bullectomy. In group C, we had 3 patients and no recurrence was found.
Discussion: VATS is an effective, safe methods for spontaneous pneumothorax in children. However, thoracoscopic stapled bullectomy resulted in an expectedly high incidence of recurrence. Pleural abrasion have been performed for a long time with low recurrence rates; however, they cause the lung to adhere to the parietal pleura, often resulting in complications such as postoperative bleeding. We changed the management of operation from pleural abrasion to coverage of the staple line with PGA after bullectomy. PGA sheet act as a foreign body on the pleura and induce local inflammatory adhesion between the apical pleura after bullectomy. However, we experienced recurrence, and we tried to use ORC sheet instead of PGA sheet after bullectomy. ORC sheet protect the apical pleura and induce mild adhesion. We had a few cases at plesent, we have to investigate more cases in the future and contrive the management for spontaneous pneumothorax, for example total pleural covering technique or sealing with a sheet-type PGA at the time of stapled resection.
TREATMENT STRATEGY OF PURE ESOPHAGEAL ATRESIA OPERATED WITH THORACOSCOPIC AND LAPAROSCOPIC SURGERY
It is often challenging to conduct radical surgery on pure esophageal atresia at an early stage. Delay in conducting radical surgery leads to a delay in acquisition of ingestional function. Additionally, esophageal atresia often requires addition of anti-reflux surgery for GER (gastroesophageal reflux) that needs to be taken in consideration within the treatment strategy. We decided to adopt a therapeutic strategy based on the gap between the two esophageal ends. We chose a laparoscopic and thoracoscopic gastric pull-up and esophago-esophagostomy modality in the right thorax combined with intrathoracic fundplication in patients with long gaps (≧5 vertebrae). We chose thoracoscopic elongation surgery (Foker technique) in patients with relatively smaller gaps (3 or 4 vertebrae). In cases where fundoplication were required, we conducted laparoscopic Nissen fundoplication. Wherever possible, we chose to conduct primary thoracoscopic anastomosis in patients with a gap that is less than two vertebrae (≤2 vertebrae). These procedures were successfully employed in infants with pure esophageal atresia. We report three cases of pure esophageal atresia treated with thoracoscopic and laparoscopic surgery.
Case 1: An eight-month-old girl underwent gastrostomy on day 1 after birth at another hospital. She was diagnosed as having pure long gap esophageal atresia (gap=5 vertebrae). Her distal esophagus was not recognized as vanishing. Therefore, we concluded that there is no indication for operation of elongation of the esophagus. We waited for her weight to become 6 kg and conducted a laparoscopic and thoracoscopic gastric pull-up and esophago-esophagostomy in the right thorax combined with intrathoracic fundplication when the patient was 8 months old. She is eating well without vomiting.
Case 2: A 1835 g girl was born at 36 weeks of gestation. She was diagnosed as having a gap that was 3 vertebrae. We conducted thoracoscopic elongation surgery (Foker technique) when the girl was 9 days old with body weight being 1835 g. We operated radical thoracoscopic surgery on day 22 when she weighed 1952 g. We then performed laparoscopic Nissen fundoplication on day 179. She was soon able to begin taking adequate amount of milk orally.
Case 3: A 2211 g girl was born at 39 weeks of gestation. She was diagnosed as having no gap when we performed gastrostomy on day 1 after birth. We operated primary thoracoscopic anastomosis on day 8 when the patient weighed 2230 g. Postoperative contrast study showed GER, but she began taking adequate milk orally. She was discharged on day 53.
We conducted radical surgery relatively early in pure esophageal atresia cases of varied gaps utilizing thoracoscopy and laparoscopy, taking in consideration the anti-reflux surgery for GER. This treatment strategy enabled our patients to avoid ingestional dysfunction, and there is potential to reduce postoperative complication, such as skeletal muscle injury, mortility disorder of scapula, respiratory obstruction, scoliosis, or chest-wall deformity.
DIFFERENT PLICATION PROCEDURES IN ENDOSCOPIC SURGERY FOR PEDIATRIC PATIENTS WITH DIAPHRAGMATIC EVENTRATION
Objective: To discuss how to choose different plication procedures in endoscopic surgery for pediatric patients with diaphragmatic eventration.
Methods: It is retrospectively analyzed the data of pediatric patients (November 2008 to August 2012) with diaphragmatic eventration who underwent laparoscopic or thoracoscopic surgery, and discussed about two different endoscopic surgeries and three plication procedures.
Results: 19 patients were identified, There were 17 boys and 2 gilrs ranging in age from 3 months to 3 years (median age was 11 months). 17 of them had a right diaphragmatic eventration, 2 had a left eventration. 17 right diaphragmas were all repaired by thoracoscopic approach while 2 left diaphragmas by laparoscopic approach. 3 kinds of plication procedures were used, namely “Reefing the Mainsail” technique (8 patients), Invaginating the diaphragmatic dome technique (9 patients), Pleating technique (2 patients). Descending distance of diaphragm after surgery were from 1 to 4.5 intercostal spaces, with mean distance of 2.7 intercostal space in chest radiographic exam. The follow-up was from 2 to 35 months. Clinical results were satisfactory with obvious improving symptoms and diaphragm rising again less than one intercostal space compared with the first examination after operation.
Conclusions: For pediatric patients with diaphragmatic eventration, different endoscopic surgeries and different plication procedures are all get satisfactory results. We believe that the choice of the plication procedure over the other depends only on the surgeon's experience.
VIDEO-ASSISTED ORTHOPAEDIC RESECTION OF THORACIC EXOSTOSES: EXOTIC CONDITIONS DON'T ALWAYS NEED EXOTIC FIXES
Background & Aims: Hereditary Multiple Exostoses (HME) is a rare autosomal dominant neoplastic trait, which typically presents in the first decade with multiple exostoses (osteochondromas). Thoracic exostoses are less common than lesions affecting the long bones. Lesions may be sessile or pedunculated, and manifest due to pleural inflammation and/or trauma to the adjacent lung or diaphragm.
This report aims to share early experience with video-assisted orthopaedic resection of thoracic exostoses. Our minimally invasive approach is distinct from other reports due its reliance on only conventional thoracoscopic and orthopaedic instruments.
Procedural Steps.
(1) preoperative: joint assessment by an orthopaedic surgeon with a specialist interest in HME and paediatric endoscopic surgeon, including cross-sectional imaging
(2) perioperative: left/right endobronchial intubation to maintain ipsilateral lung collapse throughout the procedure
(3) thoracoscopy: two 5 mm ports are inserted to confirm lesion morphology and location, as well as divide overlying pleura and vessels using monopolar diathermy
(4) orthopaedic resection: video-assisted resection using 2–5 mm Mercian Kerrison Rongeurs and/or appropriately sized osteotomes introduced via a limited intercostal incision precisely sited at thoracoscopy
(5) haemostasis: monopolar diathermy to lesion base/stalk
(6) lesion extraction: 5 mm port exchanged for a 15 mm port prior to removal of bone fragments using an endoscopic specimen retrieval bag
(7) intercostal chest drain: inserted via the remaining 5 mm port incision, and retained for <24 hours
Procedural Experience: We have performed video-assisted orthopaedic resection of thoracic exostoses in two adolescent male HME patients. The first patient presented with recurrent pneumothoraces, and the second with pleurisy. On both occasions, lesion resection and removal proved straightforward, with no intra- or post-operative complications. The chest drain was removed within 24 hours of surgery, and the patient was well for discharge on the 2nd/3rd postoperative day. Both remain symptom free after 12 and 6 months follow-up respectively.
Conclusions: We commend this approach to video-assisted resection of symptomatic thoracic exostoses, which in our limited experience has been successful and low-morbidity. Importantly, the use of only conventional thoracoscopic and orthopaedic instruments makes the described approach highly suited for application in local centres by appropriately trained endoscopic paediatric surgeons.
MINIMAL-INVASIVE SURGERY FOR PEDIATRIC THORACICOABDOMINAL DISEASES
Background and Purpose: Thoracicoabdominal diseases mainly involve congenital diaphragmatic hernia, diaphragmatic eventration, hiatal hernia and achalasia. Poor visualization due to the anatomical location and increased surgical injuries were the major defects of open procedures at this site. Thus laparoscopic and thoracoscopic procedures were theoretically considered to have advantages for these operations. We retrospectively analyzed the data of this group of patients who had received minimally invasive surgery (MIS) in our hospital.
Methods: A retrospective analysis of children who were treated with MIS for thoracicoabdominal diseases from July, 2011 to Novermber, 2012 was conducted. Thoracoscopic procedure with 3 pores was performed on the children with congenital diaphragmatic hernia and diaphragmatic eventration. These children received hernia reduction and diaphragmatic repair or plication. Laparoscopic procedure with 4 pores was performed on the children with hiatal hernia and achalasia. These children received hiatal repair and Nissen fundoplication or modified Heller's cardiomyotomy and Dor fundoplication. No drainage was used for these patients.
Results: A total of 21 children ranging from 6 months to 12 years old were included with 2 congenital diaphragmatic hernias, 6 diaphragmatic eventrations, 11 hiatal hernias and 2 achalasias. All procedures were finished without conversion to open procedures. The operation time ranged from 45 minutes to 2.5 hours and 5 to 30 ml blood loss were recorded. Patients with hiatal hernia were allowed oral intake on the second postoperative day while others on the first day. Children were discharged 4–6 days after surgery. Follow-up revealed that one hiatal hernia patient experienced vomiting 1 month after surgery and was relieved by medical therapy. And 1 child with diaphragmatic eventration was noted with slight elevation of the diaphragm during his radiological exam 3 months after surgery and was closely followed. The other patients had satisfactory recoveries.
Conclusions: Minimally invisive surgery for thoracicoabdominal diseases has better visualization, less surgical attack and better cosmetic effect for patients. It also shortens the surgical time and has faster recoveries. Short term results are good. We feel this technique could be recommended for this group of patients.
THORACOSCOPIC SURGERY FOR THE TREATMENT OF PLEURA EMPYEMA IN CHILDREN
Objective: Pleura empyema is one of the most common diseases in pediatric thoracic surgery. The pathological progression in empyema can be divided broadly into three stages. The therapeutic choice is different according to the stages and remains controversial. Minimally invasive surgery is considered to do well in treating empyema of exudative phase and fibropurulent phase. In this study, we retrospective analyzed the empyema cases that had been treated thoracoscopically to summarize the experience of minimally invasive surgery in children's empyema.
Methods: We retrospectively analyzed the empyema cases that had been treated thoracoscopically from June 2011 to September 2012. The patient was placed in a lateral decubitus position. Telescopy was inserted in the the 7th intercostalspace in the posterior axillary line, and the thoracic cavity was explored to determine the lesions and stages. Thoracic drainage tube was placed directly through the camera pore at exudative phase. At fibropurulent phase, other 2 incisions were made in the midaxillary line in the 4th interspace, and infrascapular line in the 9th interspace. Pleural effusion and pleural peel were swept out until the lung was re-expanded. The pleural peel was sent to laboratory for pathologic examination and thoracic drainage tube was placed in position.
Results: A total of 41 patients with the age ranging from 10 months to 9 years old were included with 5 exudative phase and 36 fibropurulent phase. 6 cases were reoperative patients due to ineffective chest tube drainage, 3 cases were bilateral empyema. All cases were successfully completed thoracoscopically. The operation time ranged from 25 minutes to 2 hours and 5 to 60 ml blood loss were recorded. Postoperative pathologic results revealed that 8 cases were tuberculous empyema. Chest X-ray was performed on the 2nd post-operative day and the drainage was removed on the 3rd to 6th day. Postoperative recovery was assisted by cough and pulmonary ventilation practice. The 8 tuberculous empyema patients and 4 cases with severe pneumonia were transferred to the respiratory department to accept advanced medical treatment. There were no postoperative complications in the other cases and postoperative hospital stay ranged from 6 to 8 days. All children did well in the short term follow-up.
Conclusion: Thoracoscopic treatment for empyema can help the surgeons to choose the appropriate surgical approach by intraoperative exploration. Compared with open surgery, thoracoscopic procedure can reduce operative trauma, recovery time, postoperative complications, hospital stay and gain better cosmetic outcome. In addition, this procedure can also help diagnose tuberculosis.
THORACOSCOPIC LOBECTOMY IN CHILDREN—A REVIEW OF FIVE CASES
ABSTRACT WITHDRAWN
THORACOSCOPIC RESECTIONS FOR MEDIASTINAL MASSES: A REPORT OF 6 CASES
Background and Purpose: Thoracoscopic surgeries had better visualization and less invasion compared with open procedures. Mediastinal masses especially those located in the apex of thorax could be difficult to expose during traditional open procedures, which made the minimally invasive approach more advantageous. Our study reviewed and analyzed the experience of 6 children who had received thoracoscopic mass resections at our hospital.
Methods: We retrospectively analyzed the 6 cases who had received mass resections thoracoscopically from July 2011 to October 2012 in our institution. The patient was placed in a lateral decubitus position, and three incisions approach was applied. The telescope was introduced in the posterior axillary line in the 7th intercostal space, in the midaxillary line in the 4th interspace, and in the infrascapular line in the 9th interspace, two 1–2 cm incisions were made for instruments. Single-lung ventilation was applied to the children over 10 years old and bilateral ventilation to the children under 10. Lungs were retracted with the thoracoscopic lung clamp to expose the mediastinal mass. The pleura were divided around the base of the mass, and blunt combined with sharp dissection was used to resect the mass completely. The specimen was placed in an endoscopic specimen bag and removed through the lowest incision. A chest tube was placed in position.
Results: 3 boys and 3 girls ranging from 2 to 10 years old were included in this study. No symptoms were noted preoperatively except that one child presented with Horner syndrome due to compression at the root of the neck. All procedures were finished thoracoscopically without conversion. The operating time was 35 min to 2 hours and the estimated bleeding was 10 to 40 ml. Pathological exams revealed 2 foregut duplications, 1 neuroblastoma and 3 ganglioneuromas with the biggest 4.5 cm in diameter. Chest X-ray were performed at the first post-operative day and the drainage was removed at the second day. No pulmonary infection occurred and postoperative recovery was assisted by cough and pulmonary ventilation practice. All children did well in the short term follow-up with no sign of recurrence on CT scan. The child with Horner syndrome had relieved symptoms after surgery.
Conclusion: Thoracoscopic surgery has better visualization, less surgical attack and better cosmetic effect for patients. It also shortens the surgical time and has faster recoveries. Short term results are good. We feel this technique could be applied to these patients, even to children with I-II stage of neuroblastomas.
THORACOSCOPE-ASSISTED NUSS PROCEDURE FOR PECTUS EXCAVATUM
Background: The Nuss procedure for the treatment of pectus excavatum has been widely applied gradually in China. However, this procedure is also in controversy for its two operation methods i.e. thoracoscope-assisted and non-thoracoscope-assisted procedures. The controversy lies in the surgery security and the injury degree though both two techniques are actually effective. In this study, we retrospectively analyzed the data of the pectus excavatum cases that had received thoracoscope-assisted NUSS procedure in our hospital and evaluated the safety and injury degree of this procedure.
Methods: Patients with pectus excavatum that underwent thoracoscope-assisted NUSS procedures in our department from July 2010 to October 2012 were analyzed retrospectively. Surgical technique, operation duration and blood loss were analyzed. Postoperative complication, hospital stay length and recovery were evaluated.
Results: In this study, there were totally 167 cases, 112 males and 55 females. The age ranged from 4 to 25 years old. Double bars were inserted in 33 cases for their serious chest deformity. With the guidance of thoracoscope, all procedures were completed smoothly without occurrence of pericardium, heart, great vessels or lung injury. All patients were kept stable vital signs during operation. No additional incision was made with the telescope introduced from the right side incision and no chest tube was used. The operative times ranged from 40 to 70 minutes (51 minutes in average) and 5 ml to 10 ml blood loss were recorded. The postoperative pain was most severe on the first postoperative day and alleviated as the time passed. On the third postoperative day, the pain alleviated significantly. No postoperative pneumonia, pleural effusion or other complication occurred. A mild pneumothorax could also be absorbed within one week. Patients discharged from hospital 4 to 6 days after operation. All patients did well in the short term follow-up with obvious improvement in chest shape.
Conclusion: Thoracoscope-assisted Nuss procedure is safe and feasible in the treatment of pectus excavatum. Compared with non-thoracoscope-assisted Nuss procedure, thoracoscope-assisted Nuss procedure doesn't increase the operation time, incision, or chest tube usage. Under the guidance of thoracoscope, the bar can be inserted and placed precisely. Thus the intra-operative complication is decreased and the recovery is speeded up.
THORACOSCOPIC REPAIR OF H-TYPE TRACHEOESOPHAGEAL FISTULA: TWO TECHNICAL CASE REPORTS
Objective: To present the experience of early diagnosis and thoracoscopic treatment for H-type tracheoesophageal fistula (type V).
Methods: A retrospective review of the clinical data of 2 cases of children with congenital H-type tracheoesophageal fistula undergoing repair via thoracoscopy was analyzed. One case was at the age of 27 days, whose fistula was at T2 level, diagnosed by diatrizoate esophagogram before operation. The other was 1 year and 6 month years old, whose fistula was at left main bronchus, diagnosed by the combined examination of gastroscopy and bronchoscopy.
Results: Both 2 cases were cured. The neonate was healed by one-stage operation, and without any fistula or esophageal stenosis during 1 year follow-up after operation. The elder child underwent the bronchoscopy-assisted thoracoscopic repair, anastomosis fistula of esophagus occurred in 7 days after operation, and underwent second thoracotomy.
Conclusion: The H-type tracheoesophageal fistula (type V) is comparatively infrequent in all types of the esophageal atresia. The thoracoscopic repair of this type is feasible, Early diagnosis, strict indications and advanced skills in the thoracoscopic procedure may benefit to the good prognosis.
THORACOSCOPIC TREATMENT OF PULMONARY HYDATID CYST IN CHILDREN
Background and Aim: Surgical treatment has remained the standard option in the management of hydatid disease. Surgeons were able to replicate the principles of conventional surgery using minimally invasive techniques. Herein, we report 15 pediatric patients of pulmonary hydatid cyst treated successfully using the thoracoscopic approach.
Materials and Methods: From April 2005 to June 2012, 15 children (10 male, 5 female), age range of 4 to 16 years, underwent thoracoscopic procedure for an echinococcosis cyst of the lung (10 left, 5 right side). All patients were diagnosed with clinical and radiological findings on plain X-ray chest and CT (Computed Tomography). All of them received oral albendazole 12 mg/kg/day soon after diagnosis. The patients were put in a full lateral decubitus position with simple lung intubation. Using a 5/10-mm camera and 5/10-mm working ports. Three ports were placed in a triangular fashion to the mid axillary line. A 5/10-mm 30 o telescope was introduced through middle port. For a non-complicated cyst the hypertonic saline was injected, and then the endocyst was extracted using a 10 mm endobag. Irrigations, partial decortications and partial excision of the exocyst were performed and the cyst in using suture ligation for air leak. Infected endocysts and partial exocyst were extracted as the same manner. A chest tube was placed through the lower port site.
Results: It was a vomited cyst in 3 cases, a pyopneumocyst in 4 cases, and a non-complicated and univesicular cyst in 8 cases. The patients had uneventful postoperative courses. At mean follow up of 4 years (6 months to 7 years), they were free of symptoms with no recurrence on the chest x-ray.
Conclusion: All stages of the surgical treatment of hydatid cyst of the lung in children can be easily accomplished by thoracoscopy. It is our impression that thoracoscopic management of pulmonary hydatid cyst is safe, offers the advantages of less pain, rapid recovery, less short-and long term morbidity, and good cosmesis.
THERAPEUTIC BRONCHOSCOPY: INNOVATIVE IDEAS
ABSTRACT WITHDRAWN
HEMODYNAMIC EFFECTS OF THORACOSCOPIC SURGERY IN NEONATES WITH CARDIAC ANOMALIES
Introduction: Thoracoscopic procedures are in advance in babies and even premature infants. Technical aspects as well as the size and weight of the child are no longer limiting factors. However, there is a lack of knowledge about the influence of pneumothorax on the cardiovascular system, especially in infants with cardiac anomalies. Clinical experience indicates a good adaption of the healthy neonate, but there are limited data regarding the hemodynamic effects of pneumothrax and the insufflation of CO2 in children with heart defects. The aim of this study was to clarify the hemodynamic effects of thoracoscopy in term and preterm neonates with cardiac anomalies.
Methods: Retrospective, single institution study including all term and preterm neonates with cardiac anomalies undergoing thoracoscopic procedures from January 2004 until November 2012. 15 neonates (11 term, 4 preterm) were identified. Median age at the time of surgery was 3 days (range 1–15 days) and median weight at the time of surgery was 2.9 kg (range 1.2–4.1 kg). In this study, cardiac anomalies, type of operation, operative time, insufflation pressure and hemodynamic effects in the postoperative course were evaluated.
Results: Thoracoscopic esophageal atresia repair was the most common procedure (n=10). Five neonates underwent thoracoscopic treatment of a congenital diaphragmatic hernia. All infants were known to have cardiac anomalies preoperatively without hemodynamic instability at the time of surgery. Cardiac anomalies included atrial septum defect (ASD), persistent foramen ovale (PFO), patent ductus arteriosus (PDA), ventricular septum defect (VSD), tetralogy of Fallot, dilated cardiomyopathy and mitral valve insufficiency. Seven neonates had an uneventful postoperative course without hemodynamic effects. Three patients presented transient hypotension and in four neonates reduced urine output was noted. Altogether, three neonates required dopamine or dobutamine treatment in the postoperative course, but there were no events of hemodynamic instability or shunt-inversion.
Conclusions: From this experience it appears that thoracoscopy can be performed safely in term and preterm neonates with cardiac anomalies. Even in babies with multiple cardiac anomalies and complex heart defects different thoracoscopic procedures could be performed without hemodynamic instability. Nevertheless, individual evaluation of the type of defect and evaluation of a firm pediatric cardiologist is indispensable to reduce the risk of hemodynamic instability and shunt-inversion in this delicate group of patients.
THORACOSCOPIC REPAIR OF ESOPHAGEAL ATRESIA WITH OR WITHOUT TRACHEA-ESOPHAGEAL FISTULA
ABSTRACT WITHDRAWN
TECHNICALITIES OF THORACOSCOPIC EXCISION OF A PIG'S BRONCHUS
Aims: Upper lobe bronchi originating from the trachea above the carina are thought to be the result of an abnormal tracheal out-pouching early in embryonic life. Also referred to as PIG bronchus (due to the fact that this configuration is usual in swine, cattle, sheep, goats, giraffes and camels), it has a reported incidence of 2–10% and is more common on the right. We detail the case of a 2 yr old girl who presented with a history of recurrent chest infections predominantly affecting the right upper lobe, developmental delay and failure to thrive.
Methods: CT imaging and bronchoscopy findings confirming the diagnosis are presented. Technical aspects of resecting this aberrant brochus from the trachea and completing right upper lobectomy are demonstrated.
Results: The patient had no postoperative complications and was discharged on the 5th postoperative day. All symptoms were resolved and the patient is thriving at six month follow up.
Conclusion: A pig's bronchus is a rare bronchial abnormality which can occasionally be symptomatic. Thoracoscopic excision is possible.
THORACOSCOPIC THYMECTOMY IN JUVENILE NON-THYMOMATOUS MYASTHENIA GRAVIS
Aims: Thymectomy in myasthenia gravis (MG) has been shown to improve symptoms in up to 75% of patients with or without thymic abnormality. We present the outcomes following thymectomy and present a thoracoscopic technique.
Methods: Retrospective, single centre review of 9 patients with MG who failed medical management (1999–2012). Pre-operative symptoms were assessed using the Osserman classification. Response to thymectomy was classified using the De Fillippi classification. Other parameters assessed were: operative approach, intensive care unit (ICU) stay, hospital stay, pre and post operative drug dosages, need for plasmaphoresis and post operative complications. A video is presented to illustrate the procedure.
Results: Nine patients (4 male, 5 female) underwent Thymectomy: Sternotomy 5, Thoracoscopic 4. Median age at surgery was 11.5 years (range 8–16). The median duration of symptoms was 6 months. Average post operative intensive care unit stay was: Sternotomy 1, Thoracoscopic 0 days. Median Postoperative stay was 6.4 for the open and 2 days for thoracoscopic. No chest drains were kept following thoracoscopic thymectomy. 8 patients had improved Osserman classification post Thymectomy (sternotomy 5, Thoracoscopic 3). 2 sternotomy patients had complete symptomatic improvement. There were 2 patients (thoracoscopic) that required post operative plasmaphoresis, both with significant disease. 1 sternotomy patient developed a keloid scar. There were no procedure specific complications. 8 patients had a reduction of pyridostigmine dosage. Of the 6 patients who had corticosteroids preoperatively, 4 did not require steroids and 2 had dose reductions.
Conclusion: Thymectomy can produce symptomatic improvement in Juvenile MG when medical therapy has failed. Symptomatic improvement is disease specific. Thymectomy can offer long term remission in children. Thoracoscopy evidently offers reduced pain and surgical morbidity, cosmetic advantages, shorter hospital stay and equally good MG outcomes.
THORACOSCOPIC LUNG PARENCHYMA SPARING SURGERY IN CONGENITAL PULMONARY AIRWAY MALFORMATIONS
Purpose: Parenchyma sparing surgery and segmental resections are performed in number of conditions including localised lung cancer. This concept is not commonly applied to congenital lung lesions. We aim to evaluate our surgical experience with the Congenital Pulmonary Airway Malformations (CPAM) with parenchyma preserving resections.
Materials and Methods: All patients with the diagnosis of CPAM who underwent lung resections, performed at a single tertiary referral centre between 1995 and 2012 (n=115) were retrospectively reviewed. The cases that underwent lobectomy were excluded from the evaluation. Preoperatively all children underwent CT scans with IV contrast for diagnosis, anatomical localisation and vascular supply. Investigations, pathological diagnoses and post operative outcomes were evaluated. Cases were followed up postoperatively in clinic for up to five years.
Results: Thoracoscopic resections were carried out generally using 3 ports, central endotracheal intubation and intra-thoracic insufflation with CO2 (7 mm pressure and 1.5 lt/min flow rate). Antenatally diagnosed cases were operated on between 9 months to 18 months (median 12 months), following investigations. Parenchyma preserving surgery was considered in all cases where the preoperative imaging demonstrated a CPAM that occupied less than 40% of the lobe, including intra-lobar sequestrations with systemic blood supply. When feasible the postnatally diagnosed congenital lobar emphysema were also resected preserving the non-emphysematous segments. Complete resection was achieved by dissecting just within normal parenchyma using Ligasure device (Vellylab, Covidien). Intra-operatively residual air leaks were sutured over. Sealants/glues were used in some of the earlier cases to attempt to contain the air leak, but these were not found to be effective. Intra-operative blood transfusion was required mainly in infected cases. Conversions were related to significant vascular inflammatory adhesions in four patients and involvement of two lobes in two. Inter costal drains were placed in all cases after pulmonary resections. Postoperative pain was effectively managed either by port site long-acting local anaesthetic infiltration or by intercostal blocks. Postoperative air leaks were observed in five cases, three of which required further surgery. There were no mortalities or long-term complications.
Conclusion: Our experience suggests that lung parenchyma sparing surgery is feasible in majority of the congenital lung lesions. The morbidities related to these resections were acceptably low. Infected CPAM were more likely requiring conversion and lobectomy.
THORACOSCOPIC APPROACH IN MEDIASTINAL MASSES
Aim: The aim is to present the experience on thoracoscopic surgery in mediastinal masses.
Patients and Methods: Between January 2009 and November 2012 a retrospective chart review of 13 patients with mediastinal mass who were undergone thoracoscopic surgery was performed. Demographic data, complains, dimensions of the mass, operating time, feeding time, timing of chest tube removal postoperatively, conversion to open, presence of intraoperative and postoperative complications and histopathological results were evaluated.
Results: Seven of the patients were male and six were female who had chest pain (n=3), coughing (n=6), dyspnea (n=3) and weight loss (n=2). Median age was 7 years (2 months-15 years). The masses were 10–120 mm (mean of 50 mm) in diameter in computer tomography. Mean of operating time was 75 minutes (25–210 minutes). The surgery was converted to thoracotomy in one patient because of excessive adhesions to aorta. There were no intraoperative and postoperative complications. The patients were fed on postoperative first day and the mean of chest tube removal was 5 days (3–10 days). Histopathological examination revealed neuroblastoma (n=2), leiomyoma, lymphangioma, schwannoma, teratoma, Ewing's sarcoma, lymphoma (n=2), rabdomyosarcoma, metastasis of Wilm's tumor and inflammatory reaction. The patient with thymic mature cystic teratoma had recurrence twice and underwent thoracoscopy in first recurrence and thoracotomy in the second.
Conclusion: Thoracoscopy is safe and feasible in total excision or incisional biopsy of mediastinal masses when performed by experienced pediatric surgeons on minimally invasive surgery.
FIBEROPTIC BRONCOSCOPY-GUIDED PERCUTANEUS TRACHEOSTOMY IN INFANTS
Tracheostomy is a routine procedure in critically ill patients which prevents some complications of extended tracheal intubation. Percutaneous tracheostomy is a cost-effective alternative to surgical tracheostomy with lower postoperative risk of bleeding and infection. The addition of bronchoscopic guidance has increased the safety of the procedure and may prevent complications. The aim is to present two infants with body weight of 3500 g who were undergone fiberoptic bronchoscopy-guided percutaneous tracheostomy.
Both 3500 g infants who were followed intubated because of neurological problems since their birth was planned to have tracheostomy. One of the infants was also diagnosed as subglottic stenosis. Under general anesthesia, first patient was extubated and laryngeal mask was placed. Pediatric fiberoptic bronchoscope was inserted through the laryngeal mask. In the second patient the bronchoscope was inserted through the endotracheal tube. The needle was introduced into the trachea with the guidance of bronchoscope light and a guidewire was inserted through the needle. Following multiple dilatations, 3.5F tracheostomy cannula was placed. No perioperative or postoperative complication occured in both of the patients. The literature survey revealed that these patients are the youngest presented cases with the lowest body weight undergone fiberoptic bronchoscopy-guided percutaneous tracheostomy.
Although surgical tracheostomy has been successfully established in low body weight infants, fiberoptic bronchoscopy-guided percutaneous tracheostomy is an effective and safe alternative technique to surgical tracheostomy.
FOREIGN BODY EXTRACTION WITH OPTICAL VERSUS NON-OPTICAL FORCEPS DURING RIGID BRONCHOSCOPY
Background: There are currently two types of forceps used for foreign body removal at rigid bronchoscopy, these can be classified as side used standard bronchoscopy forceps and optically guided grasping or alligator tipped forceps. In order to find out the safer tool we evaluated broncoscopy procedures regarding the technique used for foreign body removal.
Materials and Methods: Records of patients who underwent bronchoscopy for evaluation of foreign body aspiration (FBA) in our unit from 2008 to 2012, inclusive, were reviewed retrospectively. Age, sex, history of FBA, symptoms, results of radiologic studies, bronchoscopy findings, type of forceps used for foreign body removal, number of attempts to remove the foreign body, the duration of the procedure complications, and outcome were recorded and statistically analyzed to find out which technique is the best and safer for foreign body removal.
Results: A total of 204 bronchoscopies were done (142 boys, 62 girls) presenting with a mean age of 2,2±0.3 years. FBA was confirmed in 165 (81%) patients, whereas normal bronchoscopic findings, signs of pulmonary infection, and endobronchial granulation tissue were noted in 12 (5.8%), 24 (11,7%), and 3 (1.4%) of the patients, respectively. Bronchoscopic removal of foreign bodies was succeeded in all children with foreign body. Optical forceps were used in 76 (46%), standard forceps in 62 (38%), aspiration in 15 (9%) and fogarty catheter in 12 (7%) patients. Mean number of attempts to remove foreign body was 2±0.9 with optical forceps and 5±1.9 with standart forceps, (p<0.05). Mean duration of the prodecure was 12±1.4 minutes and 24±3.9 when optical forceps and standart forceps used, respectively. Serious hypoxemia and bradycardia had occured 5 times with optical forceps and 12 times with standart forceps during the procedures. The complications were laryngeal edema (n=6), and reversible cardiopulmoner arrest which was resulted with brain death (n=1). All of them occured in the procedures when standart forceps were used.
Conclusion: We conclude that clear advantages were found when the optically guided forceps were compared with the standard bronchoscopy forceps as shorter duration of the procedure and less complications. We think that optical forceps are safer as foreign body can be removed through broncoscopy tube without need of recurrent entubations with broncoscope. They also eliminate the possibility that foreign body can be trapped while passing through vocal cords.
EARLY EXPERIENCE WITH THORACOSCOPIC REPAIR OF CONGENITAL DIAPHRAGMATIC HERNIA IN CHILDREN
Background: To describe the surgical technique, initial results, and outcome of thoracoscopic repair of posterolateral congenital diaphragmatic hernia (CDH).
Patients and Methods: A retrospective review was undertaken of the patients with CDH who underwent thoracoscopic repair from June 2009 to June 2012. Pleural insufflation with carbon dioxide was maintained at a pressure of 4–6 mmHg. Three trochars were used. The hernia defect was repaired by using nonabsorbable extracorporeal interrupted sutures.
Results: There were 10 patients, with mean age of 4±2 days. Mean operative time was 75±15minutes. There were 3 conversions because size of the defect was very large and patch application could not be done safely. 2 patients with severe pulmonary hypoplasia died postoperatively Mean hospitalization time was 10±5 days. No recurrences occurred among the survived CDH patients during 20±4 month follow up.
Conclusion: Thoracoscopic repair is feasible and safe for children with CDH. The technique causes minimal trauma, and promotes early recovery.
THORACOSCOPIC LEFT LUNG TRISEGMENTECTOMY IN THE TREATMENT OF CONGENITAL CYSTIC ADENOMATOID MALFORMATION (CCAM) – A CASE REPORT
One-year old female child was diagnosed prenatally with congenital cystic adenomatoid malformation involving left upper pulmonary lobe. The child has not presented any symptoms during her first year of life. The diagnosis was confirmed by the CT at the 6 months of life.
She underwent an elective thoracoscopy which showed involvement of the both lobes of the left lung. For this reason left trisegmentectomy was performer thoracoscopically with the use of Ligasure LS1000 and removal of the segments 4, 5 of the upper and 6 of the lower lobe. Her postoperative course was uneventful and she was discharged on the day 4 after the chest drain was removed. She is currently symptom- and recurrence-free at 4 months after surgery.
USE OF ENDOSCOPIC SURGICAL SPACER TO IMPROVE SAFETY DURING THORACOSCOPIC REPAIR OF CONGENITAL DIAPHRAGMATIC HERNIA
Thoracoscopic repair of congenital diaphragmatic hernia (CDH) has recently become more common, and the challenge of managing neonatal cases is increasing. Meanwhile, there have been reported intraoperative complications or conversion to open surgery due to injury of herniated viscera and inability of organ reduction. We used the endoscopic surgical spacer SECUREA™ (Hogy Medical Co., Ltd., Tokyo, Japan), which is an elliptical sponge made of polyurethane with a radiopaque marker, for preventing these complications in five cases of CDH. The first case was a late presentation in a 10-month-old girl, and the other cases were prenatally diagnosed neonates without severe pulmonary hypertension. All cases were left-sided hernias without sacs. At operation, the SECUREA was grasped using forceps, and the viscera were pushed back gently to avoid injuring the spleen or the short gastric vessels in all except the first case. The SECUREA was intended to prevent intestinal injury during defect repair in all cases, with placement of the SECUREA between the edge of the diaphragm and the reduced intestine. The procedures in all patients were completed with no complications and without the need for conversion.
THORACOSCOPIC CLOSURE OF PERSISTENT DUCTUS ARTERIOSUS—INITIAL EXPERIENCE
Purpose: The surgical repair of persistent ductus arteriosus in Poland is performed only by open-heart surgeons who have insufficient experience with thoracoscopic procedures. The aim of the study is to present our initial experience with thoracoscopic closure of persistent ductus arteriosus performed in cooperation between experienced endoscopic pediatric surgeon and open-heart surgeons.
Materials: Retrospective analysis of medical records of consecutive 23 children operated in the last 12 months.
Results: The procedure was performed in general anesthesia with the patient lying prone. Two 5 mm and one 3,5 mm trocars were placed into the left pleura. In smallest babies the instruments were placed directly to the chest apart the telescope. The 5 mm 300 telescope was used. Only in the last five cases an attempt was made to selective right main bronchial intubation There were 7 babies with the weight below 1000 g. The smallest one has 670 g. The age of operated patients was between 2 weeks and 4 years (mean 12,4 months). In each case the visualization of recurrent nerve was perfect but it was difficult to see the anterior border of ductus. The ductus was closed with 5 mm titanic clips, only in two cases 10 mm clips were applied. The time of procedures was between 20 min and 90 min (mean 54 min.). The time corresponded well with the age of patients - it was much longer in older patients because of longer dissection of ductus. There was no intraoperative and postoperative complications and blood loss. All cases had echocardiogram study in operating theatre just after finishing the operation. One case because of incomplete closure confirmed on echocardiogram needed reoperation that was performed during the same anesthesia.
Conclusion: The thoracoscopic closure of ductus arteriosus persistent proved to be safe and effective and based on our experience it is the procedure of choice. We believe that good cooperation between experienced endoscopic pediatric surgeon and open-heart surgeons was mandatory to start this procedure.
HYBRID ENDOSCOPIC THYMECTOMY - COMBINED TRANSESOPHAGEAL AND TRANSTHORACIC APPROACH IN A SURVIVAL PORCINE MODEL
Objective: Video-assisted thoracoscopic surgery (VATS) thymectomy has been used in the treatment of Myastenia Gravis and thymomas (coexisting or not). In natural orifice transluminal endoscopic surgery (NOTES), new approaches to the thorax are emerging as alternatives to the classic transthoracic endoscopic surgery. In this study, the authors assess the feasibility and reliability of hybrid endoscopic thymectomy (HET) using combined transthoracic and transesophageal approach.
Methods: Twelve consecutive in vivo experiments were undertaken in the porcine model (4 acute and 8 survival). For HET, an 11 mm trocar was inserted in the 2nd intercostal space in the left anterior axillary line. Then, a 0° 10 mm thoracoscope with a 5 mm working channel was introduced. Transesophageal access was created through a submucosal tunnel using a flexible gastroscope with a single working channel introduced through the mouth. Using both flexible (gastroscope) and rigid (thoracoscope) instruments, the mediastinum was opened, the thymus was dissected and the vessels were ligated using electrocautery alone.
Results: Submucosal tunnel creation and esophagotomy were performed safely without incidents in all animals. Complete thymectomy was achieved in all experiments. All animals in the survival group lived for 14 days. Thoracoscopic and postmortem examination revealed pleural adhesions on site of the surgical procedure with no signs of infection. Histological analysis of the proximal third of the esophagus revealed complete cicatrization of both mucosal defect and myotomy site.
Conclusions: HET is feasible and reliable. HET could be regarded as an alternative to classic thoracoscopic approach for patients requiring thymectomy.
LAPAROSCOPY ASSISTED GASTROSTOMY: IS IT THE WAY FORWARD IN PEDIATRIC MINIMAL ACCESS GASTROSTOMY?
Background/Purpose: Percutaneous Endoscopic gastrostomy (PEG) is considered to be the “gold standard,” to assist feeding in children with feeding difficulties. After three decades of PEG use, publications of outcome data from large case series has consistently indicated a significant risk of major complications. Laparoscopy Assisted Gastrostomy (LAG) has emerged as a safe alternative to PEG to avoid major complications associated with PEG. The aim of this study is to compare the LAG and PEG related to the outcomes including the number of procedural anesthetics per patient, complication rate, post operative length of stay and the rate of repeat gastrostomy following complications.
Materials and Methods: A retrospective review of all minimal access gastrostomy insertions performed in a tertiary pediatric surgical center between 2003 and 2012 (nine years) was undertaken. Children who had fundoplication with gastrostomy were excluded from the study. The data collected include type of procedure (PEG and LAG), patient demographics, co morbidities, risk factors for complications, length of post operative stay, complications, number of procedural anesthetics until a low-profile button is inserted, and the number of repeat gastrostomy insertions for complications. Simple descriptive analysis using STATA version II was used for data analysis. Chi-Square and Fisher's exact tests were used for calculation of statistical significance.
Results: Of the total number of 149 patients studied (PEG, n=115; LAG, n=34), the mean age at insertion of PEG was 4.27 years compared to 3.94 years in LAG group which was not significantly different. Most common co morbid factors were cerebral palsy, seizures, neuromuscular disorders and cardio respiratory disease in both groups. In the PEG group 77.88% (88/112) of patients required two general anesthetics to achieve a low profile button compared to 5.88% (2/34) of LAG patients which was statistically significant (p<0.05). Major complications occurred in 11.30% (13/115) of PEG and 2.94% (1/34) of LAG patients where there was merely a trend but not statistically significant (p=0.191). Re-operation rate following complications was 21.74% (25/115) for PEG and 5.88% (2/34) for LAG which was statistically significant (p=0.042). Mean post-operative hospital stay was 11.39 days in PEG group and 3.94 days in LAG group, but the difference was not statistically significant.
Conclusions: Laparoscopy assisted gastrostomy has significantly less reoperation rate following complications compared to PEG and it obviates the need for a second procedural anesthetic to achieve a low profile button, making it a safe alternative to PEG in children with feeding difficulties.
THE IMPACT OF LAPAROSCOPY ON POSTOPERATIVE SMALL BOWEL OBSTRUCTIONS IN CHILDREN
Purpose: There is limited published data regarding post-operative small bowel obstructions (SBO) in the pediatric patient population. In order to better characterize the impact of surgical technique on bowel obstructions, a retrospective review was performed.
Methods: After IRB approval, a retrospective chart review over ten years (2000–2010) was performed analyzing data of patients who were admitted to a tertiary care children's hospital with symptoms of a bowel obstruction. Patients without a history of prior abdominal surgery, with cystic fibrosis, or Hirschsprung's disease were excluded. Statistical analysis was performed using SPSS software and evaluated with a chi-square and non-parametric Mann-Whitney U test. A p value≤0.05 was deemed as statistically significant.
Results: During the designated time there were 250 qualifying admissions from 219 different patients. Of those, 21% had a history of prior laparoscopy (LAP) and 79% had undergone a prior laparotomy (OPEN). LAP patients presented with post-operative SBO significantly earlier when compared to OPEN (192 vs. 841 days. SD±378.8 and±1326.4, p=0.001). The most common documented cause of obstruction for both LAP and OPEN was adhesive disease (78.2% and 62.5% respectively, p=0.19). Regardless of the type of prior surgery, there was no difference in the percentage of patients requiring operative intervention (LAP=71%, OPEN=72%, p=0.405). The type of prior operative technique (LAP vs. OPEN) did not impact the operative approach for postoperative SBO requiring surgical intervention (p=0.12).
Conclusions: We conclude that minimally invasive surgery appears to impact the timing of presentation of post-operative SBO in children. However, the initial approach (LAP vs. OPEN) does not seem to have an impact on the need for surgical management of postoperative bowel obstructions.
COMPLICATIONS OF LAPAROSCOPIC REPAIR OF COMPLETE RECTAL PROLAPSE. ARTICLES REVIEW AND CASE REPORT
Background: Rectal prolapse is relatively common condition in children. It is usually self-limited problem and requires no surgical treatment. Many local and open surgical procedures are with relative success advocated for children with persistent rectal prolapse. Recently, laparoscopic approaches become standard choice for management successfully. It is feasible and safe procedures, however complications may occur.
Purpose of Study: This article is literature reviewing recorded complications of laparoscopic mesh repair of complete rectal prolapse in children and reporting first case of adhesive bowel obstruction post-surgery.
Patients and Methods: Review all available English language literatures published in Medline, PubMed and Cochrane database. Search is based on key words; complications, laparoscopy, complete rectal prolapse and children. All published reviews, articles and case report are retrospective studies carried out after ethical approvals granted from local institutes. Permission from parent has been granted to report the case. The rest of published data have been gathered, tabulated and analysed.
Case Report: 11 year old healthy girl has been referred with ten month history of persistent rectal prolapse. The problem has been more frequent and difficult to reduce spontaneously. Oral laxative has been prescribed by gastroenterologist. No previous history of diarrhea or constipation. Physical and digital rectal examination are unremarkable. Colonoscopy, routine blood test and Sweat test results are normal.
The patient underwent laparoscopic rectosigmoidopexy with mesh applied to fix the redundant sigmoid colon to the sacral promontory. Post-operative period was uneventful and patient recovered smoothly. Oral laxative has been prescribed for three months. Satisfactory follow-up appointment has warranted no active abdominal complaint and no symptoms of recurrence.
Week later (2-months post-surgery), she presented with symptoms of bowel obstruction. After resuscitation, conservative management commenced with no progress. Decision has been made for laparotomy and proceeds. Two bands firmly adherent to mesh have been excised, release of intra-abdominal simple adhesions and partial omentectomy have been performed. Smooth post-operative recovery was reported. Patient has been reviewed with satisfactory outcome.
Results: Male to female ratio is variable; however, boys are predominant. Median age was 6.9 years. Patients were exposed to conservative management for a variable period. However, persistency of rectal prolapse caused significant distress, pain, occasionally anal bleeding and embracement for patients and their families. No intraoperative complications were reported. Postoperative complications were reported with no significant morbidity and mortality. Few cases were lost to follow-up, but majority were reviewed. Follow-up period was relatively short (7.2 months and 36 months). Recurrence is not documented with laparoscopic mesh; however, it is documented when sutures only are used (total recurrence and partial mucosal prolapse). Constipation happened in few cases. Temporary Colonic fistula documented in one case. We report first case with adhesive bowel obstruction post laparoscopic mesh repair.
Conclusion: Small number of trials and relative short period of follow-up has been identified in paediatric age group. Use of laparoscopy in management of complete rectal prolapse becomes common and improving functional outcome. Surgical complications can still happen; however, current practise doesn't show significant morbidity and mortality. Larger RCTs with long term follow-up are needed.
PORTAL VEIN THROMBOSIS AFTER LAPAROSCOPIC SPLENECTOMY DURING CHILDHOOD
Background: Portal vein thrombosis (PVT) is a rare but potentially life-threatening complication of laparoscopic splenectomy (LS) and can lead to bowel ischemia or portal hypertension. In childhood, this complication is reported in 5–10% of the cases whereas it can be up to 50% in adult population. Our aim was to evaluate PVT incidence after LS in children and associated risks factors.
Subjects and Methods: A retrospective chart review identified 35 children (18 females, 17 males) who consecutively underwent elective laparoscopic during a seven year period (2005–2012) at a single teaching hospital. Age and weight were respectively 7.3 years (range 2–17 years) and 24 kg (range 10–60 kg). The main indication for LS was spherocytosis (n=15), sickle cell disease (n=13) and idiopathic thrombocytopenic purpura (n=5), traumatologic cases were excluded. Splenomegaly was present in 80% of the cases with a spleen longest axis ranging from 8.5 to 23 cm (median=12.5 cm). A cholecystectomy was also performed in 10 patients. Thromboembolic prophylaxis was not routinely given.
Results: Duration of surgery was 125 min (range 67–197 min). A conversion to laparotomy was necessary in 7 cases (specimen extraction=5, bleeding=2). Hospital length of stay was 4 days (range 2–13 days). Maximum platelet counts was recorded at 458.109/L (range 188–1,290. 109/L). Doppler ultrasound scan (USS) was performed post-operatively in 22 cases. Post-operative course was uneventful in all but one patient. She was a 17 year-old girl (60 kg, 167 cm) previously operated for an ovarian Sertoli-Leydig cell tumor with hyperandrogenism. Histopathology revealed a 23 cm spleen with a splenic lymphoma. Thromboembolic prophylaxis was used with subcutaneous low molecular weight heparin (LMWH). At day 4, while she was asymptomatic, a systematic USS showed a PVT extending in the right and left portal branches. LMWH was used initially and transitioned to fluindione for 3 months, adjusted to achieve an INR between 2.0 and 3.0. Over our series, she was the only patient with platelet count over 1,000,000/μL. Follow-up abdominal imaging studies performed 1 and 4 months postoperatively demonstrated complete resolution of the PVT.
Conclusion: PVT after pediatric LS is a rare event in our series (<5%). Clinician should be cautious in oncologic cases and if very large spleen or if thrombocytemia >1,000.109/L is present. If detected early, PVT can be treated efficiently; we therefore recommend a systematic USS during the first post-operative week.
RECURRENCE OF CONGENITAL DIAPHRAGMATIC HERNIA IN CHILDREN TREATED WITH MINIMALLY INVASIVE TECHNIQUES—IS IT A FREQUENT PROBLEM?: OWN OBSERVATIONS
Congenital diaphragmatic hernia (CDH) is an inborn failure associated with severe complications. Outcome improvement in the past 20 years is related to application of new techniques mainly in intensive care. In recent years minimal invasive surgery techniques were also introduced for surgical treatment of CDH.
The aim of the study was to present cases of diaphragmatic defect recurrence among children operated because of CDH with minimally invasive techniques.
In the past 5 years in our center 19 patients with CDH underwent laparoscopic and thoracoscopic repair. The diagnosis was determined basing on routine prenatal ultrasound, post- natal radiography (during newborn period and later). Age at the time of surgery depended on child's clinical status and the time of diagnosis and ranged from several hours to over 4 years. Among 19 patients 3 required secondary intervention because of CDH relapse. 2 patients (with left lateral defect) underwent thoracoscopy as primary procedure, 1 (retrosternal defect)- laparoscopy. All secondary interventions were laparoscopies, conversion was necessary in one case. Period between interventions ranged from 3 months 12 days to 10 months 15 days. Based on retrospective analysis of intraoperative video records, we suspect that high tension in the suture line was the main cause of relapse. Minimal invasive techniques can be associated with misjudgement of tension in the line of defect closure. Same technique can be applied for secondary intervention.
LAPAROSCOPIC PALOMO VARICOCELECTOMY FOR VARICOCELES IN CHILDREN
ABSTRACT WITHDRAWN
FLEXIBLE URETEROSCOPY FOR UPPER URINARY TRACT CALCULI IN CHILDREN
Objective: To explore the clinical value of flexible ureteroscopy in the treatment of the upper urinary tract calculi in children.
Methods: A total of 17 children (10 boys and 7 girls), with upper urinary tract calculi (including 4 cases with melamine-induced stones) underwent 20 flexible ureteroscopic procedures. Among them, 11 had the upper ureteral calculi and 6 renal calculi. The median age of the children was 5.5 (range 2.3 to 16) years. The calculus involved the left side in 9 cases, the right side in 5 and both sides in 3 (upper ureteral calculi). The median stone diameter was 1.1 (range 0.7 to 1.5) cm. All of the cases had mild or moderate hydronephrosis in the ipsilateral kidney. Retrograde flexible ureteroscopy: Children with renal calculi routinely recieved ureteral double-J stent preoperatively. Pediatric rigid ureteroscope was inserted into the upper ureter, Then a guidewire was inserted into the ureter, and a sheath for flexible ureteroscope was placed into the target ureter following the guidewire. The flexible ureteroscope was inserted near to the stone, which was fragmented by holmium laser. If the ureteric sheath for flexible ureteroscope could not be inserted, a double-J stent would be indwelled, and the second ureteroscopy would be performed after 1 to 2 weeks. Antegrade flexible ureteroscopy in mini-percutaneous nephrolithotomy: A conventional percutaneous nephrolithotomy channel was established. Rigid ureteroscopy was performed to deal with the stone using holmium laser. If the stone could not be found, the flexible ureteroscope was used through percutaneous nephrolithotomy channel, and the stone was fragmentated by holmium laser. A double-J stent and a renal fistula were indwelled anterogradly.
Results: Thirteen of fifteen retrograde flexible ureteroscopic procedures were successfully performed, two failed due to rigid ureteroscope not being inserted into the upper ureter. A double-J stent were inserted. A flexible ureteroscopic procedure was successfully performed after two weeks. Two flexible ureteroscopic procedures in mini-percutaneous nephrolithotomy were successfully performed. All the stones were successfully found and fragmentated in all the children after a single holmium laser lithotripsy under direct vision achieved by a flexible ureteroscopy. The median operative time was 50 (range 40 to 80) mins. There was no major perioperative complication. Double-J stent was removed after 2 to 4 weeks when no residual stones were found more than 3.0 mm in size. Patients were followed up from 3 to 26 months. No stone recurred, and no ureter stricture and vesicoureteral reflux occured.
Conclusions: Flexible ureteroscopy is a safe and feasible method for the treatment of the upper urinary tract calculi in children. It is suitable for the stones in the pelvis and calyceal stones which the rigid ureteroscopy could not reach, as well as for the stones which moved to the collection system of kidney. It is especially suitable for the children with minor stones, without significant hydronephrosis, with a procedure of failed ESWL, with the residual stones not be found by pediatric rigid ureteroscope, or with a high risk of mini-percutaneous nephrolithotomy.
Key words: Flexible ureteroscopy; upper urinary tract calculi; children; holmium laser.
EFFICACY OF THE TREATMENT OF RETROPERITONEAL LAPAROSCOPIC DISMEMBERED PYELOPLASTY FOR URETEROPELVIC JUNCTION OBSTRUCTION(UPJO) IN CHILDREN
Objective: To evaluate the clinical value of retroperitoneal laparoscopic dismembered pyeloplasty for ureteropelvic junction obstruction (UPJO) compared with open surgery in children.
Methods: The clinical data of 35 children who underwent retroperitoneal laparoscopic dismembered pyeloplasty for UPJO from September 2003 to October 2011 were retrospectively compared with those of 32 children who underwent open dismembered pyeloplasty through a retroperitoneal flank approach. The youngest child was just 7 months old in laparoscopic group. Pediatric laparoscopic instruments were used in 11 cases. Three children with giant hydronephrosis underwent retroperitoneoscopic nephroplication and nephropexy, one child with pelvic calculus underwent retroperitoneoscopic pyelolithotomy, and one child with multiple renal calculi underwent mini-percutaneous nephrolithotomy simultaneously. In open surgery group, two children with multiple renal calculi underwent pelviolithotomy.
Results: All operations were performed successfully in both groups. There is no difference in the operation time, the duration of retroperitoneal drainage tube, complications and the therapeutic effect (P>0.05). But the estimated blood loss, analgesic requirements, recovery of intestinal function, incision length, and postoperative hospital stay in laparoscopic group were better than that in open surgery group (P<0.05). Patients were followed up from 3 to 90 months, intravenous urography (IVU) or magnetic resonance urography (MRU) showed no stricture at UPJ. Compared with the preoperative, B ultrasound found that the renal parenchyma became obviously thick and hydronephrosis significantly reduced.
Conclusions: Retroperitoneal laparoscopic dismembered pyeloplasty is a safe, minimally invasive, less suffering and quicker-recovery procedure for pediatric UPJO. It appears to be the first line choice for the treatment of pediatric UPJO. Moreover, the accompanied diseases could be treated with minimal invasion in one procedure. The pediatric laparoscopic instruments could lead to better cosmetic results.
Key words: Laparoscopy; Pyeloplasty; Retroperitoneal.
TRANSUMBILICAL LAPAROSCOPIC SINGLE-SITE SURGERY FOR DUPLEX KIDNEYS IN CHILDREN (REPORT OF 3 CASES)
Objective: To explore the clinical application value of transumbilical laparoscopic single-site surgery (LESS) for duplex kidneys in children.
Methods: Three children with surgical indications of duplex kidneys in children were subjected to transumbilical LESS heminephrectomy, including 1 boy and 2 girls. The boy was 15 years old, due to a medical examination finding that the right side of the duplex kidney hydronephrosis. The girls were 7 and 10 years old, respectively, who were found the duplex kidney hydronephrosis due to recurrent urinary tract infections examination. Under general anesthesia, the cases were placed in the lithotomy position. Ureteroscopy and indwelling ureteral catheter to affected side were performed before the operations, and then the affected side was elevated. One 5-mm trocar and two 10-mm trocars were inserted into the abdomen cavity through a 3 cm incision at the medial margin of umbilicus. According to the standard laparoscopic method, no function duplex kidney and ureter were resected after full free of kidney. Then methylene blue would be injected through the pre-indwelling ureteral catheter. After it was confirmed that there were no collection system injury, the specimens were put into homemade bag and removed through the slightly enlarged medial margin of umbilicus.
Results: All the 3 procedures were successfully performed without conversion to open surgery. The median operative time was 155 mins. The median blood loss was 185 ml. The patients resumed ambulation on postoperative day 1. Two patients resumed nutrition on postoperative day 2. The abdominal drainage was removed on postoperative day 3 to 4. Among them, 1 patient underwent intestinal function recovery delay and abdominal distension, whose intestinal function and diet recovered after treatment. The abdominal drainage was removed on postoperative day 4. All patients were discharged on postoperative day 7. The umbilical incision was obscured due to the folds around, which lead to a good cosmetic results. During the 3- to 7-month follow-up period, all the patients were in good condition. The scars were nearly invisible on the abdominal wall. There were no incisional hernia formation.
Conclusions: Transumbilical laparoscopic single-site surgery for duplex kidneys is safe, feasible, minimally invasive. It is can not only improve cosmetic results, also reduce the adverse psychological impact on children. It appears to be a valuable choice for the treatment of duplex kidneys in children.
Key words: umbilical plexus; laparoscopic single-site surgery; duplex kidneys; nephrectomy.
A CASE OF LAPAROSCOPIC VAGINECTOMY AND HYSTERECTOMY FOR CONGENITAL VAGINAL ATRESIA ASSOCIATED WITH PYOMETRA IN NEUROLOGICALLY IMPAIRED CHILDREN
Background: Laparoscopic vaginectomy and hysterectomy for pediatric no malignancies such as congenital vaginal atresia is rare, and this report presents the method used in this case.
Case Report: The patient is a 10-year-old girl with both mental and physical disabilities who underwent two operations previously at our hospital—laparoscopic Nissen fundoplication for GER at the age of 1 year old and the Cohen method for VUR of unilateral Kidney at 8 years old. A diagnosis of associate congenital vaginal atresia had been made in this patient at the operation of Nissen fundoplication and we had planned the radical operation for vaginal atresia prior to her first menstruation. However, she had pyometra and a drainage tube was inserted into the uterus at another hospital at the age of 9 years old. Although radical operation as the next step was necessary for her, we selected and performed not intestinal vaginoplasty but laparoscopic vaginectomy and hysterectomy, due to her neurological impairment, severe surgical stress of intestinal vaginoplasty, and predictable postoperative complications. Laparoscopic surgery was performed via 4 ports. Although intrapelvic adhesion was hard after inflammation, the bilateral ovaries could be preserved. Dissection of the one-third upper part of the vagina was most difficult in this procedure, so the uterus was divided and we checked the lumen for confirmation of the blind end of the vagina. The operation time was 5 h 30 min. There was no intraoperative complication and no conversion to open surgery.
THE CURATIVE EFFECT ANALYSIS OF PREOPERATIVE PERCUTANEOUS FISTULA IRRIGATION FOR TREATMENT OF INFECTION OF UPPER URINARY TRACT CALCULI
ABSTRACT WITHDRAWN
THE ROLE OF LAPAROSCOPIC PYELOPLASTY FOR PRIMARY REPAIR OF URETEROPELVIC JUNCTION OBSTRUCTION IN INFANTS UNDER 1 YEAR OF AGE
Purpose: Pediatric laparoscopic pyeloplasty to treat ureteropelvic junction obstruction has demonstrated successful rate similar to open pyeloplasty. However it's not clear if all age groups benefit from this procedure. We compare the outcome of laparoscopic pyeloplasty (LP) in infant under 1 year of age, with our pediatric group treated by LP.
Materials and Methods: From June 2005 to January 2012, 79 LP by trans-peritoneal approach were performed in 77 patients, 30 of them were infants under 1 year of age (39%). We retrospectively reviewed the records and the following information was recorded: body weight, age, sex, operative time, stents, length of hospitalization, length of follow up, successful rate, complications and reoperations.
Results: There were 79 LP in 77 patients divided into two groups: Group I (Infants under 1 year of age): 30 infants, and group II (more than 1 year-old): 47 patients.
In the group I (30): The mean age was 6.8 months (2–12) and the mean weight was 8 kg (3.5–12). LP was feasible in all cases with the use of stay sutures. In two cases JJ stent was unsucceful, in one case of them a peri-anastomotic drain was placed without complication in the postoperative period. The mean operative time was 110 min (80–150) and the mean hospital stay was 29 Hs.
In the Group II (49): The mean age was 69 months (13–150). The techniques used were: LP in 39 cases and in the last 10 cases when an aberrant crossing vessel was found, a vascular transposition and pexed of pelvic-ureteric junction without pyeloplasty was done. The procedure could not be completed by Laparoscopy in two patients at the beginning of the series. The mean operative time was 127 min (70–240) and the mean hospital stay was 2.4 days (1–12). There were immediate postoperative complications in 4 patients.
In the group I, the mean follow-up was 45 months. Two patients presented a recurrent PUJ obstruction and a redo laparoscopic procedure was done. In the group II, the mean follow-up was 51(12–120). Two patients presented a recurrent PUJ obstruction; one uretero-calicostomy and one balloon dilatations were done. In all cases decreased hydronephrosis, with improved PUJ drainage on isotope renography or sonography.
Conclusion: LP is effective procedure and safe in small infants and can be performed with outcomes comparable to that of open surgery.
OUR PATIENTS WITH VESICOURETERIC REFLUX AFTER DEFLUX INJECTION IN KOSOVA
Background: Vesicoureteral reflux (VUR) in children has been treated with subureteric deflux injection since 2009. This study analyzed the result of endoscopic treatment for vesicoureteric reflux. The aim of this study is to analyze the results of our short experience only 3 years.
Methods: Between 2009 and November 2012, 55 children underwent endoscopic subureteral injection of Deflux in 78 ureters. Two month postoperatively a voiding cystourethrogram (VCUG) was performed. This study examined the disappearance of VUR and urinary tract infection (UTI) as well as the quality of life during long-term follow-up.
Results: The study included 55 patients (40 females and 15 males) with 78 refluxing ureters. There were 22 refluxed ureters altogether and 33 children had a unilateral reflux (two duplicated systems). All patients were treated, from the age 6 months up to 12 yrs old. The mean age of patients was 5.2 years. There has been no complications, but with few recurrences. In 6 patients (16.6%) endoscopic treatment with deflux was done twice, while in three patients (8.5%) – 3 times, because of recurrence.
Conclusion: We recommend the use of endoscopic Deflux injection as the first line treatment for children with VUR. Endoscopic subureteral injection of Deflux is a minimally invasive method for VUR treatment in pediatric patients and is associated with low morbidity.
Key words: Deflux, pediatric urology.
INCIDENCE AND CHARACTERISTICS OF CONTRALATERAL MANIFESTATION IN CHILDREN WITH UNILATERAL INGUINAL HERNIA AFTER LAPAROSCOPIC COMPLETELY EXTRAPERITONEAL REPAIR
Background: Laparoscopic herniorrhaphy has been reported to have the advantages of technically simple, inspection of contralateral processus vaginalis (cPPV), and excellent cosmetic results. However, the indications for contralateral groin repair are still not clearly defined, and the incidence of metachronous contralateral inguinal hernia after this modality has not been well described.
Patients and Methods: A consecutive series of 1603 patients presenting with symptomatic unilateral inguinal hernias between July 1998 and December 2011 were included. This series included 784 boys and 819 girls with 936 right-sided and 667 left-sided indirect inguinal hernias. The patients' ages ranged from 1 to 358 months, with a median of 42 months. During laparoscopic completely extraperitoneal repair, the morphological appearances of the internal inguinal rings (IIRs) were characterized for both affected and asymptomatic side. The asymptomatic contralateral groin was carefully inspected and closed by a same technique with affected side if a cPPV was identified. With a median follow-up of 7.0 years (range 0.9–14.4), the characteristics of the children with contralateral inguinal hernia manifestation was documented.
Results: Of 1603 children, 674 (42.0%) had positive cPPV findings with 353 (37.7%) in right-side hernia and 321 (48.1%) in left-side. Contralateral inguinal hernias developed in 9 patients involving 7 boys and 2 girls. Length after initial operation ranged from 2 days to 66 months with a median of 24 months. One patient had a history of incarceration due to metachronous contralateral inguinal hernia. The patients' age at second operation ranged from 21 months 120 months with a median of 47 months. Six were originally right-sided and three left-sided. During the second laparoscopic inspection, the morphological appearances of the IIRs were widely opened whereas all of them were diagnosed as negative cPPV at the initial operation. The incidence of contralateral hernia manifestation was 0.56%.
Conclusion: Laparoscopic inspection of the cPPV contributed to reduction in developing a contralateral metachronous inguinal hernia. The morphological appearances of extremely tiny IIRs or even flat groin can develop contralateral inguinal hernia.
OBSTRUCTED MEGAURETER: URETERAL REIMPLANTATION WITH EXTRACORPOREAL TAPERING OF THE URETER BY LAPAROSCOPIC EXTRAVESICAL TRANSPERITONEAL APPROACH
Purpose: To present a case report of laparoscopic ureteral reimplantation using extracorporeal ureteral tapering for management of Obstructed Megaureter (MGU).
Materials and Methods: One patient eighteen months old with Primary MGU underwent Laparoscopic Ureteral reimplantation with Extracorporeal tapering of the ureter. The ureter was dissected circumferentially down to the bladder. It was ligated close to the bladder and divided proximal to it. The free ureteral end was delivered out through the ipsilateral 3 mm port. The lower end was tailored over a JJ stent. Later the whole assembly was carefully replaced in the abdomen. A Lich-Gregoir type extravesical reimplantation was done.
Results: Operative time and hospital stay was 180 minutes and 3 days, respectively. No complications were noted intra-operatively. No urinary leakage occurred in early postoperative period. At 8 month follow up, we found no complications.
Conclusion: Laparoscopic ureteral reimplantation with extracorporeal tapering for Obstructed MGU is a safe procedure with results similar to open surgery.
LAPAROSCOPIC RESECTION OF URACHAL REMNANTS IS A SAFE AND EFFECTIVE ALTERNATIVE TO OPEN SURGERY IN CHILDREN
Purpose: An infected urachal remnant is an uncommon benign condition that commonly recurs and has the potential to become malignant. The open surgical approach for removing urachal remnants involves making a significantly large midline infraumbilical incision or a step-ladder hypogastric transverse incision. We reviewed our experience in laparoscopic excision of urachal remnants and reported the efficacy and outcomes of this procedure. The procedure was minimally invasive and allowed for complete excision of urachal remnants.
Patients and Methods: Five children with a median age of 35 months presented with urachal remnants between January 2010 and January 2012. The data and outcomes of all patients were retrospectively reviewed. Laparoscopic surgery was performed by using 3 ports including the umbilical port. In all 5 children, the urachal remnant was excised by performing electrocauterization from the umbilicus to the bladder dome, and the stump on the bladder was ligated with an endoloop suture. No drain was used during the procedure.
Results: All 5 operations were completed successfully. Median pneumoperitoneum time was 75 minutes. The boundary between the normal bladder wall and the urachal remnant was clearly identified using a laparoscope, and excision of the remnant could be performed. The muscle layer of the bladder wall could also be excised. One patient had large cystic lesions and required partial resection of the bladder. No intraoperative or postoperative complications were reported at a median follow-up of 16 months. Complete resection of the urachal remnant was confirmed by pathological evaluation. There have been no recurrences of symptoms. Laparoscopy showed a good cosmetic outcome.
Conclusions: Laparoscopy performed for resection of urachal remnants in children allows for better visualization of the anatomy and appears to be a safer, more effective, and more cosmetically beneficial alternative to open surgery.
COMPARATIVE EVALUATION OF THE RESULTS OF SURGICAL TREATMENT OF CRIPTORCHISM IN CHILDREN
Cryptorchism - one of the most common disorders of childhood for boys, which is accompanied by spermatopoietic and hormonal function disturbances of testes and requires early surgical correction. Orhipeksya, especially in case of abdominal form, is technically difficult and traumatic. In this regard, the endovideosurgery methods are increasingly used for correction of cryptorchism in recent decades.
The purpose of this study was a comparative evaluation the results of treatment of children with cryptorchism, operated by “open” and endovideosurgical ways. Since August 2007, 61 patients with various forms of cryptorchism have been treated in the urology department of National Research Center of Mother and Child Health.
Age of patients ranged from one year to 14 years. Endovideosurgery has been applied in the treatment of 43 patients (study group). The operation consisted of the following steps: diagnostic laparoscopy in order to clarify the level of retention, visual evaluation of the testis, its blood vessels and the fixing apparatus, the intersection Gunter`s cord, the mobilization of the vascular bundle and ductus defferens, forming a channel from the abdomen into the scrotum, bringing down the testis and fixation it in the scrotum.
The “open” brining down and fixation of the testis by Petrivalskij-Schumaker has been performed in 18 patients (control group).
For comparative assessment of body's postagressive response to laparoscopic and traditional types of operations for cryptorchism we studied: the state of simpaticoadrenalic system (in circadian excretion of adrenaline and noradrenaline) and several biochemical blood parameters, reflecting the functional state of the suprarenal glands and liver, the balance of carbohydrate and protein metabolism. To assess the state of the testis we conducted ultrasound and Doppler exams of gonads in the preoperative period, on the 3rd and 6 month of postoperative period. There were no complications in the immediate and late postoperative period.
The analysis of the comparative evaluation of body's postagressive response to laparoscopic and traditional operations has showed that laparoscopic surgery is less invasive, less traumatic, less durable surgical intervention, which is characterized to have more favorable postoperative period.
More expressive positive dynamics, concluded in the growth of gonads and the normalization of blood flow parameters while ultrasound and Doppler study, has been in patients undergone endovideosurgical interventions.
Thus, this study shows clear advantages of endovideosurgical treatment of cryptorchism in children and calls for their widespread introduction into clinical practice.
EXPERIENCE OF LAPAROSCOPIC PYELOPLASTY TREATMENTING NEONATAL SEVERE HYDRONEPHROSIS
Objective: The use of laparoscopy for pediatric pyeloplasty is increasing. We review our experience with our first 21 neonatal cases and describe the main technical points learned during this experience.
Methods: We retrospectively reviewed the charts of all patients who underwent laparoscopic pyeloplasties (LP) in neonates over a 3-year period (June 2009 to June 2012) at our institution. Patient demographics, operative details, hospital stay, outcomes, and complications were examined. Twenty-one neonateswere recruited in this study. Our case selection criteria: All were detected by prenatal ultrasound and renal pelvis anteroposterior diameter were more than 3 cm. At a week after birth, ECT showed that split function of hydronephrotic kidneys were lower than 30%.
Results: All successful underwent laparoscopic dismembered pyeloplasty, no converion to open surgery or add Trocar, no intraoperative complications. The mean operation time was 75 min, and blood loss was less than 10 ml, the mean postoperative hospital stay was 9 d. All patients have been followed up for 6 to 36 months with ultrasound and ECT. All the thickness of renal parenchyma increased, renal pelvis anteroposterior diameter were significantly reduced, the scar is not obvious, and 8 kidneys appeared almost normal renal pelvis shape.
Conclusion: Laparoscopic neonatal pyeloplasty was safe and feasible and worth for spreading. But operator need to perfect himself in laparoscopic suture technology, and then gradually transit from older children to neonates.
INITIAL SINGLE INSTITUTION'S EXPERIENCE WITH LAPAROSCOPIC NEPHRECTOMY AS A SUITABLE THERAPY FOR WILMS TUMOUR IN CHILDREN
Purpose: Although laparoscopic surgery in children is widely performed, the value of laparoscopic nephrectomy (LN) for the surgical treatment of Wilms tumour is still controversially discussed. Only few centers in the world perform this procedure. We report initial experience of a single center.
Methods: In a retrospective study, we analyzed the clinical records of 16 patients who underwent LN or open nephrectomy (ON) for Wilms Tumour (WT) on Pediatric Surgery Department University of Catania, Italy, between 2008 and 2012.
Results: WT was treated in 50% by LN and in 50% by ON; there was no conversion from LN-to-ON. Comparing LN with ON in both patient groups, we found no significant difference in the overall intraoperative complications as intraabdominal rupture, spillage or bleeding. The duration of surgery was similar. However, in both patient groups, the postoprerative period was uneventful. In contrast to patients treated by ON, patients treated by LN needed significantly less analgesic and the hospitalization time was shorter with LN, while the outcome in term of recurrence or staging after 1 year follow-up was the same in both patients groups.
Conclusions: Although limited number of cases, our data suggest that LN could be an effective choice for the surgical treatment of Wilms tumour. Of course more studies and guidelines are requires to reserve this procedure only to meticulous patient selection.
LAPAROSCOPIC EXCISION OF AN RETROPERITONEAL CYSTIC LYMPHANGIOMA LOCATED IN RIGHT ADRENAL REGION
Background and Aim: Lymphangiomas can be seen anywhere in the abdomen, however, cystic lymphangiomas located in adrenal region were rarely reported. We present a laparoscopicaly excised retroperitonel cystic lymphangioma located in right adrenal region, whole dissection and excision of the cyst was carried out with Ligasure device.
Case Report: 5-year-old boy was admitted to our clinic with abdominal pain lasting for six months. Abdominal US revealed lobulated cystic mass, 3.5×4 cm in size, at suprarenal region. Laboratory results were as follows; NSE; 31.2 μg/l, HVA: 2.28 mg/24 h, VMA: 1.26 mg/24 h. MRI evaluation of the cyst resulted with simple adrenal cyst/lymphangioma?? diagnoses. Laparoscopic exploration and excision of the mass was planned. Case was placed in left semi-lateral (45°) position. Excision of the cyst was accomplished with one 10-mm umblical video-port, and three 5-mm working ports inserted trough; epigastrium, halfway between epigastrium and umblicus in midline, and right lateral position to the umblicus on the right midclaviculer line. Epigastric port was used for liver retraction, and remaining two ports were used as working ports. Ligasure was used to open the peritoneum, dissection and excision of the cyst. He was fed on the 1st postoperative day and discharged home on 2nd postoperative day without any problem. Even the follow-up period is short as 7 months, there is no cyst recurrence detected with US so far.
Conclusion: Retroperitoneal cystic lymphangiomas located in adrenal region are rarely reported in literature. Although our laparoscopy experience was intermediate at that time, we found laparoscopic excision of such cyst is safe and effective with the help of LigaSure device due to its easy application and controlled sealing features. In addition, laparoscopy gave us better visualisation of the operative field and adrenal region, and allowed us to complete the operation in reasonable time as expected.
LAPAROSCOPIC EXTRAVESICAL APPENDICOVESICOSTOMY–MITROFANOFF PROCEDURE IN A PATIENT WITH V-P SHUNT AND EXTENSIVE INTRAABDOMINAL ADHESION
Introduction: Several techniques for continent catheterizable appendicovesicostomy as Mitrofanoff procedure (MP) were described in the literature. Laparoscopic MP with extravesical approach could be performed even in an abdomen with adhesions.
Video Presentation: This video presents a laparoscopic extravesical appendicovesicostomy-MP in a 7-year-old male patient with V-P shunt and extensive intraabdominal adhesion. Tips and tricks on creation of working space, preparation of bladder wall and appendix, appendicovesical anastomosis and tunnel formation were shown. The patient was discharged in the 3rd postoperative day and could perform catheterization with no problem in the last 13 months.
Conclusion: Intraabdominal extravesical laparoscopic MP could be performed with careful dissection and preparation of appendix and bladder wall in patients with previous intraabdominal operation and adhesions. In patients with V-P shunt, a special care should be given not to contaminate the peritoneal cavity.
GUBERNACULAR SPARING LAPAROSCOPIC-ASSISTED FOWLER-STEPHENS PROCEDURE IN INTRAABDOMINAL TESTIS
Introduction: A meticulous attention should be paid to preserve collaterals of testis in single or two staged Fowler-Stephens procedure (FSP).
Video Presentation: This video presents a 6-year-old patient having gubernacular sparing laparoscopic-assisted staged FSP for an intraabdominal testis. The patient had a left peeping testis which was tethered on the internal inguinal ring. Following the first stage of FSP; 4 months later, laparoscopic dissection and preparation of peritoneum on the lateral side of the ductus deferens with guberneculum sparing was performed. The second stage was completed with inguinal dissection and orchidopexy. Physical examination and ultrasound of the testis in the 6th postoperative month did not show any abnormality.
Conclusion: In non-palpable testis, if FSP is needed, a special attention should be paid to save the vascular collaterals of ductus deferens, cremester and scrotal arteries and veins. By gubernacular sparing laparoscopic-assisted FSP, collaterals, especially branches of cremesteric and scrotal arteries and veins could be preserved. The orchidopexy procedure could be accomplished by using gubernaculum associated natural track of testis.
RETROPERITONEAL LAPAROSCOPIC MANAGEMENT AND OUTCOMES OF UPPER-POLE NEPHROURETERECTOMY FOR DUPLEX KIDNEY ANOMALIES IN CHILDREN
Purpose: The standard treatment for a duplex kidney with poorly functioning upper pole moiety is ipsilateral upper pole heminephrectomy. This procedure is usually performed by open surgery, but with recent developments in techniques of uro-laparoscopy, it can be done with it, safely. In this study we evaluated the results and safety of laparoscopic heminephrectomy in our consecutive cases.
Materials and Methods: From May 2010 to May 2012, fourteen unilateral laparoscopic heminephrectomy were performed in our department. Median age at surgery was 35.4 months (7 month to 11 years). A retroperitoneoscopic approach was used in all patients in lateral retroperitoneal (LRP). Patients' characteristics, presenting symptoms, operative time, and blood loss, complications were all collected retrospectively. Using pre-operative ultrasonography, intravenous pyelography (IVP) and delayed enhanced three-dimensional CT scanning, unilateral upper pole hydronephrosis was detected in all cases. By DTPA isotope scan hypofunctioning of ipsilateral moieties was detected in all cases. Follow up included routine ultrasound, and DTPA was performed in the event of abnormalities in ultrasound or postoperative course.
Results: Mean operative time was 163±80 minutes. no patients required open conversion. 2 patients (%) developed a postoperative urinoma. The mean blood loss was 25 ml and no children required perioperative blood transfusion. No major intra-operative or early complications were identified. Mean hospital stay was 6.1 days. On mean follow-up of 16 months no disturbing symptoms or episodes of urinary tract infections (UTIs) were detected. No atrophic kidney was detected.
Conclusion: Laparoscopic partial nephrectomy in children is safe, associated with decreased morbidity and shorter hospitalization. Perfect renal pedicles vascular system manipulation is important for the preservation of renal function post-operatively. Long term follow-up is necessary to study long term outcomes.
EXPERIENCE WITH LAPAROSCOPY IN NONPALPABLE TESTIS
Objective: The aim of this study was to investigate the feasibility and benefits of diagnosis and interventional laparoscopy in those pediatric patients with nonpalpable testes (NPT).
Patients and Methods: Between 2004 and 2012, 325 patients with NPT (mean age 52.46 months, range12 months to 16 years) were treated. 352 testes were evaluated.
Results: According to the laparoscopic findings 4 groups of testes were identified: vanishing testis (n=250), low abdominal testis (<2 cm to the internal ring) (n=37), high abdominal testis (>2 cm to the internal ring) (n=34) and intersex patients (n=4). Of the first group, 58 testes (two bilateral) had blind-ending spermatic cord and vessels. Two atrophic testes in the abdomen underwent laparoscopic assisted orchidectomy. For those with spermatic cord and vessels beyond the internal ring (193 testes), inguinal exploration was performed and testicular remnants were removed. Histologic evidence confirmed excision of testicular tissue in 11 cases (12 specimens). 48 testes of the second group had a one-stage laparoscopic orchidopexy. 3 testes in the 3rd group had a single-stage Fowler-Stephens (F-S) orchidopexy and 43 testes had a staged F-S procedure (with 6 to 12 months intervals between the two stages). There was no evidence of testicular atrophy in all but one testis in the exploration of F-S stage 2 procedure and it was removed during the procedure. In the 4th group, gonadal biopsy was performed. Three patients were diagnosed as true hermaphrodite, the testis was on one side and ovary was on the other side in two cases, both patients underwent ovariectomy. Ovotestes were confirmed by histology on both sides in another case. One patient was diagnosed as mixed gonadal dysgenesis with testis on one side and streak gonad on the other side and underwent dissection of the streak gonad. The follow-up period was between 6 months and 8 years, and one testicular atrophy was noted in single-stage F-S procedure, three more testicular atrophies were noted after F-S stage 2 and two testicular atrophies were noted after one-stage laparoscopic orchidopexy. All testes were seen to be located in the bottom of the scrotum, with the exception of four testes that had retracted to the neck of the scrotum. Seven patients were identified as having persistent mullerian duct syndrome (PMDS) and all the ductal structures were removed with hysterectomy.
Conclusion: Laparoscopy decreases the number of laparotomies in NPT, allows a single-stage procedure in low abdominal testis, and facilitates clip ligation of the testicular artery in high abdominal testis. Laparoscopy also provides diagnostic and therapeutic options for vanishing testis and intersex patients. Our data also show that the laparoscopic gonadal biopsy remains the only way to obtain morphologic gonadal structure and to establish a final diagnosis in doubtful cases. Magnification and easy access to the pelvic cavity allow removal of gonads or ductal structures with the advantages of minimally invasive procedure.
DOUBLE PELVIC HITCH METHOD FOR LAPAROSCOPIC REDUCTION PYELOPLASTY WITH USE OF CHOLANGIOGRAM FORCEPS FOR DOUBLE J STENT INSERTION: TWO VERY USEFUL AND TIME SAVING TRICKS
Aim: The main constraints in paediatric laparoscopy pyeloplasty is the small size abdomen and the presence of distended bowel which does not deflates even with preoperative bowel preparation. We present a double hitch method for paediatric laparoscopic pyeloplasty, which helps the surgeon to circumvent this problem along with an easy and quick method of inserting double j stent both saving significant amount of operative time.
Patients & Methods: All patients diagnosed to have pelvi ureteric junction obstruction after a standard protocol of imaging by Ultrasound, nuclear scan and were included. They were given a single rectal enema an evening before surgery. The procedure was done by one optical and 2 working ports. The pelvis once identified, if required, is first decompressed and then hitched at the superior angle by a trans abdominal suture, similarly the lower angle of distended pelvis was made to elevate by either looping the UPJ by another abdominal hitch or by hitching the lower angle of pelvis. In this way the entire distended pelvis was raised above the surrounding viscera following which reduction pyeloplasty was performed with great ease. The video also demonstrates the use of a cholangiogram forceps for introduction of double j stent which is extremely easy and quick method of doing so as it has a 5fr channel along its length.
Results: Total of 25 patients and renal units (6 females, 15 left) were operated by the given method. The mean age was 13 months range (7 mth-36 mth). There was no preoperative preparation required. All the cases were accomplished by using 2 working ports only and no retraction port was required. There was no conversion to open.
Conclusion: Hitching the dilated pelvis at both superior and inferior angles aides the surgeon for pelvic reconstruction without the surrounding colon and small bowel coming in view. This method avoids the need of placing an additional retracting port. This technique helps us to attempt pelvic reconstruction even in smaller infants with small abdominal volume. The use of cholangiogram forcep is a quick time saving method of inserting trans-anastomotic double j stent.
LAPAROSCOPIC URETEROCISTOPLASTY WITH MITROFANOFF SYSTEM
Even though the enterocisplasty is the gold standard to increase the capacity of neurogenic bladder, it has an elevated morbidity. So the use of dilative ureter could be a good alternative for this purpose and for the Mitrofanoff system.
Four pediatric patients with neurogenic bladder, pop off phenomenon and renal ipsilateral atrophy were submitted to cistoplasty with dilative refluxing ureter. First nephrectomy with preservation of total ureter was made. The middle and distal portion of detubularized ureter were anastomosed to the widely opened detrusor. The proximal portion was introduced through a submucosal tunnel created in the vesical dome and was taken out through the umbilicus. The average time for the surgery was 4 hours and there were no complications. The tracing of the patients were of 2 to 4 years and the increment of bladder obtained was of the 75% of the capacity according to their age with compliance that varied between 15 a 20 cc/cm H20. There was no leaking of urine by the stoma betwen 4 hours cateterization.
The introduction of increased bladder with dilated ureter in the early 90's was promising. Theoretically there wouldn't be better tissue for bladder augmentation. It eliminates electrolyte abnormalities, the production of mucus and intestinal tract interruption when compared with the enterocystoplasty. It also has an internal hedge of urothelium, smooth muscle elasticity and has the characteristic that potentially would preserve the ability of bladder emptying. The postoperative follow-up has proven beneficial therapeutic impact, comparable to that obtained with the open technique, both adaptability (compliance) and bladder capacity of the patient, with the benefit of minimally invasive.
PNEUMOCYSTOSCOPIC COHEN URETERIC REIMPLANTATION: REPORT OF 10 CASES
ABSTRACT WITHDRAWN
TEN YEAR EXPERIENCE OF LAPAROSCOPIC REPAIR OF PEDIATRIC HYDROCELE AND THE LONG-TERM FOLLOW-UP RESULTS
Purpose: To assess the efficacy and safety of laparoscopic repair for pediatric hydroceles and its long-term follow-up results.
Methods: We performed this procedure to 284 patients from 2002 to 2011 using our specially designed curved awl. The patent internal ring was enclosed and fixed under laparoscopy and fluid within the patent processus vaginalis was emptied by percutaneous needle aspiration.
Results: The median operation time was 16 minutes. Fifty-seven contralateral open internal rings were diagnosed during laparoscopic exploration and closed at the same time. During our 10-year follow up only four kids had recurrence of moderate amount of fluid accumulation 1–3 months after the surgery and 3 of them spontaneously resolved during the out-patient follow-ups. Only one of them was treated by percutaneous needle aspiration successfully. No abdominal viscera injury happened.
Conclusions: Laparoscopic hydrocele repair proved to be applicable and effective with satisfactory long-term results according to our experience.
Key Words: Pediatric Hydrocele Laparoscopy Follow-up.
ANALYSIS OF 8 CASES OF PEDIATRIC LAPAROSCOPIC PYELOPLASTY UNDERGOING RETROPERITONEAL ACCESS
Objective: To explore the minimal invasive approach using laparoscope for pelvic ureteral junction obstruction in children.
Methods: Eight cases of pediatric laparoscopic pyeloplasty (LP) undergoing retroperitoneal access were identified, including 5 boys and 3 girls. Median age was 14 months old (range 6–96). Median operative time was 239 minutes (range 182–297). Three 5-mm conventional ports were placed. Two 5-mm laparoscopic instruments and a 30-degree 5-mm camera were used for Anderson-Hynes pyeloplasty. Laparoscopy by retroperitoneal access for the treatment of pelvic ureteral junction obstruction was performed through the incision at right paracolic gutter. A F4.7 or F3 pigtail stent was introduced through one of the instrument ports. A drain was placed next to the anastomosis by retroperitoneal access.
Results: All procedures were performed without additional trocars. There were no open conversions. There were no intraoperative complications. The operating time was 224 min (range: 175–310), the intraoperative blood loss was little, the postoperative intestinal function recovery time was 8 hours (range: 4–24). Median follow-up was 19 months (range 12–26). Follow-up renal ultrasound evaluation has demonstrated improved hydronephrosis in all patients. No reoperative pyeloplasty was performed.
Conclusion: Pediatric laparoscopic pyeloplasty is accepted widely. LP was performed undergoing retroperitoneal access in our unit, and the drain is placed by retroperitoneal access. This procedure minimizes intraperitoneal organs effects of operation. Pediatric laparoscopic pyeloplasty undergoing retroperitoneal access is available as a minimal invasive approach to treat pelvic ureteral junction obstruction in children.
LONG-TERM FOLLOW-UP RESULTS OF SINGLE STAGE FOWLER-STEPHENS ORCHIOPEXY FOR INTRA-ABDOMINAL TESTES
Objective: To compare long-term follow-up results of single stage laparoscopic Fowler-Stephens orchiopexy for intra-abdominal testes with traditional open Fowler-Stephens orchiopexy.
Methods: Respectively analyzed the postoperative follow-up materials of 55 patients (64 testes) who underwent their first surgery for intra-abdominal testes between March 1993 and January 2012 in West China Hospital of Sichuan University. Between March 1993 and April 2003, traditional open Fowler-Stephens orchiopexy was performed on 15 patients (16 testes) which aged from 11 months to 14 years old (median 4.1 years old). Between May 2003 and January 2012, laparoscopic Fowler-Stephens orchiopexy was performed on 40 patients (50 testes) which aged from 6 months to 14 years old (median 3.2 years old). All the patients have regular follow-up through outpatient department from 10 months to 9 years old (median 2.8 years old). Testicular position, testicular size and testicular texture was be estimated by physical examination and testicular echo, testicular volume and testicular blood supply was be estimated by ultrasound.
Results: All patients had no significant perioperative complication. All testes were down into the scrotum after operation without retraction. 5 testes were atrophic after traditional open Fowler-Stephens orchiopexy in 5 patients, the incidence was 31.25%. While 3 testes were atrophic after laparoscopic Fowler-Stephens orchiopexy in 3 patients, the incidence was 6.25%. The rest testes were normal on testicular texture and echo, also had increased testicular volume and good testicular blood supply.
Conclusion: Laparoscopic technique has significant advantages in the diagnosis and treatment of intra-abdominal testes, according to the position of testes and the tension of spermatic cord. single stage laparoscopic Fowler-Stephens orchiopexy has a lower atrophic rate compared with traditional open Fowler-Stephens orchiopexy because of retaining a large peritoneal around vas deferens and epididymis and avoiding the damage of them. If the surgeon is proficient at laparoscopic surgery, laparoscopic Fowler-Stephens orchiopexy is optimum selection for treating intra-abdominal testes.
SINGLE INCISION LAPAROSCOPIC NEPHRECTOMY AND HEMINEPHROURETERECTOMY USING STANDARD INSTRUMENTS VERSUS CONVENTIONAL LAPAROSCOPY IN CHILDREN WITH CONGENITAL NON-FUNCTIONING KIDNEYS
Introduction: Nephrectomy(N) or heminephroureterectomy(Hn) by single incision laparoscopic surgery(SILS) have been previously reported in children. Most of the reports on SILS describe a technique using a combination of single port device, reticulating and standard instruments which incur extra costs in instruments. Others have adopted the approach of using standard laparoscopic setup with reusable trocars and straight 3- and 5-mm instruments to perform SILS in children. Data comparing SILS with conventional laparoscopy (CL) in children undergoing nephrectomy or heminephroureterectomy remains scarce in pediatric literature.
Methods: Consecutive children who underwent nephrectomy or heminephroureterectomy by SILS using standard instruments for congenital non-functioning kidneys or moieties of duplex system from 2009 to 2012 were retrospectively compared with a matched cohort of children who underwent CL in the same center.
Results: A total of 30 children, aged 14 months to 9 years, were recruited for the study. 12 children in the SILS group (n=8; Hn=4; N:Hn=2:1) were compared with a matched cohort of 18 children in CL (n=12;Hn=6) of same N-to-Hn ratio. There was no difference between the two groups in the age, body weight, gender proportion, laterality of pathology, postoperative analgesic requirement and hospital stay. In the SILS group, one case of Hn required conversion to open because of difficult dissection. The remaining 29 children had their surgery completed successfully by either CL or SILS without additional port placement. There was no intraoperative complications in both groups and none of the patients required blood transfusion intraoperatively. Nephrectomy by SILS took longer operative time than CL (156±45 vs 99±35 mins). There was one wound infection in the CL group while no postoperative complication or access site hernia was noted in SILS group.
Conclusions: SILS using standard instruments is comparable to CL in its effectiveness and safety in performing nephrectomy and heminephroureterectomy in children for congenital benign conditions. SILS has the potential advantage of better cosmesis, which has yet to be proven, but at the cost of longer operative time.
THE EXPERIENCES OF RETROPERITONEAL LAPAROSCOPIC NEPHRECTOMY IN CHILDREN WITH UNILATERAL RENAL DYSPLASIA
ABSTRACT WITHDRAWN
LAPAROSCOPIC TRANSVESICAL URETERAL REIMPLANTAION FOR VESICO-URETERIC REFLUX WITH AND WITHOUT PRIOR DEFLUX(R) INJECTION: EARLY EXPERIENCE
Background: Injection of dextranomer/hyaluronic acid has been the treatment of vesico-ureteric reflux (VUR) in recents years. A proportion of these patients still require reimplantation when the injections are not successful. Laparoscopic transvesical ureteral reimplantaion (LTUR) is an alternative to reimplant the ureters. It is technically demanding but has the benefit of less pain and without an unsightly scar. We report our experience with this technique with patients injected with dextranomer/hyaluronic acid.
Methods: This is a retrospective review of patients with primary VUR from 2005–2012. Patients with Laparoscopic Transvescial Ureteral Reimplantation were included. All operations were performed via three 5 mm transvescial ports. Bladder dome was anchored to the abdominal wall during operation. Ureter was mobilized transvescially and then sutured to contralateral side of the trigone via a submucosal tunnel. Demographics and clinical outcome were analysed with SPSS 20.0.
Results: 11 patients were included in this study. 9 of them were female and the 2 were male. 5 of them had bilateral ureteral involvement and a total of 16 ureteral units were operated. The indications for operation were urinary tract infection or persistent VUR. 3 of them had previous injection of dextranomer/hyaluronic acid. The mean age at operation was 6.82±1.99 yrs (range 5–12 yrs). The mean preoperative grading was 4.00±0.82 (range 2–5) with a mean operative time of 221.26±42.12 mins (range 175–298 mins). One of them had residual grade 1 disease. The complete disease resolution rate was 93.8%. 2 of them need conversion and both of them had injection of dextranomer/hyaluronic acid before the ureteral reimplantation where no conversion in patients with no previous injection of dextranomer/hyaluronic acid. The mean follow-up time was 35.82±29.45 months (range 3–84 months).
Conclusion: High complete disease resolution rate was demonstrated in patients with Laparoscopic Transvescial Ureteral Reimplantation in this study. With the advantages of minimally invasive surgery, this technique should be advocated in patients' with primary VUR. However, high conversion rate was noted in patients with previous injection of dextranomer/hyaluronic acid. Alternative operative options may be considered in this group of patients.
LAPAROSCOPIC ASSISTED PYELOPLASTY IN NEONATES
Background and Aim: Pediatric urologic operations that can now be regularly performed using the minimally invasive surgery (MIS). One of the procedures is laparoscopic dismembered pyeloplasty (LP) for hydronefrotic kidney with ureteropelvic junction (UPJ) obstruction. LP is very difficult for neonates and small infant. Laparoscopic assisted pyeloplasty (LAP) is an innovative alternative MIS. In this study, we want to present our experiences with LAP in neonates.
Materials and Methods: Between December 2008 and August 2012, 35 neonates underwent LAP. The neonates (23 male, 12 female) were in the age range of 5 days to 30 days (mean 21 days). The UPJ obstructions were left sided in 22 cases (63%), right sided in 11 (31%) and bilateral in 2 (6%). All of the patients were detected to have UPJ obstruction during the antenatal evaluation. Using a 3/4 mm camera and two 3 mm working ports, UPJ was mobilized by a transperitoneal laparoscopic technique. The UPJ was brought out through a tiny flank incision and a standard dismembered pyeloplasty was performed and a double J stent replaced.
Results: Mean operative time was 65 minutes (range, 50–75 minutes). Incision was smaller than 1,5 cm in all, and the average postoperative hospital stay was 3 days (range, 2–6 days). Follow-up ranging from 4 to 44 months showed reduction in hydronephrosis and improvement in renal function of all the operated units.
Conclusion: We concluded that laparoscopic assisted pyeloplasty is recommended especially in neonates and small babies where laparoscopic pyeloplasty is difficult.
SCROTAL HYDROCELES NOT ASSOCIATED WITH PATENT PROCESSUS VAGINALIS IN CHILDREN
Background: Regarding a scrotal hydrocele in a boy older than 4 months of age, it is considered that the hydrocele represents peritoneal fluid entering the scrotal portion of the patent processus vaginalis (PPV), which indicates an alternative manifestation of indirect inguinal hernia (IIH), and the ligation of the PPV at the internal inguinal ring (IIR) is the appropriate treatment. In fact, our series of more than 300 children with hydrocele who underwent repair under laparoscopy, all had PPV and were cured without recurrence after closure of the PPV. On the other hand, we have experienced postoperative large scrotal hydrocele on rare occasions, appearing after closure of the PPV in boys with IIH or hydrocele, in spite of complete occlusion of the IIR. We found the instances that may explain the cause of this rare occurrence.
Materials: From May 1998 to March 2012, we experienced large scrotal hydroceles not associated with PPV in six boys (2 right, 1 left, 3 bilateral) among the 352 children who underwent laparoscopic repair for hydroceles. Ages ranged from 7 months to 15 years with a median of 12 years. Three of them had had cut-down repair for hydrocele with PPV, one had had laparoscopic repair for bilateral IIH prior to the definitive surgery, and the remaining two boys had their operations for the first time.
Results: In four boys, who had had repair for their IIH or hydrocele, laparoscopic inspection at the definitive surgery revealed completely closed IIRs. Two boys with hydrocele, whose operation was the primary one, were found to have large hydroceles bulging into the peritoneal cavity without PPV. All of them were treated with subtotal removal of the tunica vaginalis, instead of any surgical intervention to the IIR, with no recurrence of the hydrocele. Pathological studies of the removed sacks revealed marked thickness with chronic inflammation and lymphectasis.
Conclusions: The complete occlusion of the PPV does not always prevent the recurrence of hydrocele due to alternative pathogenesis. Pathological findings of the specimen suggested any disturbance in lymph flow of the testicular system. In these cases, the subtotal removal of the sac is the choice of treatment, and direct operative approach to the IIR or the neck of the sac must be avoided, because of provable risk to induce the disturbance of lymph drainage.
OPTIMUM SELECTION AND EFFICACY ANALYSIS OF SURGICAL APPROACHES FOR CRYPTORCHIDISM
ABSTRACT WITHDRAWN
LAPAROSCOPY FOR PERSISTENT MULLERIAN DUCT SYNDROME IN CHILDREN
Purpose: To evaluate the effectivness of laparoscopy for the diagnosis and treatment of Persistent Mullerian Duct Syndrome (PMDS) in children.
Patients and Methods: The medical records of children with PMDS who underwent laparoscopic procedures were reviewed retrospectively at the last 5 years.
Results: The mean age of patients were 7.4 (R:1-16) years and they were presented to our center after operations. The patients' identifications are summarized in the Table.
Persistent mullerian ducts were removed at all except patient number 5, who had severe adhesions in between ductus deferens and mullerian structures secondary secondary to past inguinal exploration.
Of 10 testes, 2 had no testis secondary to inguinal orchidopexy at another center, 2 underwent inguinal orchidopexy, 6 underwent lapararoscopic orchidopexy in our center (One case two stage).
Conclusion: Surgical treatment of PMDS is challanging and there is no standart approach. In our series, laparoscopy was found as usefull both diagnostic and therapatic tools in managemet of PMDS but relation of Mullerien structures is important and defines success of surgery.
Purpose: Presentation of transvesicoscopic revision of ureteric stenosis following transtrigonal ureteroneocyctostomy.
Patients and Methods: Two male patients developed postoperative ureteric stricture after excison of left paraurethral diverticula and transtrigonal ureteroneocystostomy which was done by open surgery in one case and transvesicoscopically in the other. Following failed attempts of other treatment modalities shuch as percutaneous nephrostomy and/or cystoscopy and balloon dilatation, surgical repair was decided. Transvesicoscopic excision of stenotic part of the distal ureter and re-ureteroneocystostomy procedure was done in both case successfully. The cases are event-free on the post-operative 8th and 10th months.
Conclusion: Transvesicoscopic surgery could be used for treatment of ureteric stenosis secondary to previous surgery in children as an alternative to open surgery.
LAPAROSCOPIC TRANSPERITONEAL HEMINEPHRECTOMY FOR DUPLEX KIDNEY ABOVE AND BELOW ONE YEAR OF AGE: FEASIBILITY AND LONG-TERM RESULTS
Purpose: Evaluation of feasibility, safety and outcome of laparoscopic heminephrectomy for duplex kidneys in children above and below the age of 12 months.
Methods: The surgical technique included division of the parenchyma via Ligasure® and amputation of the ureter as low as possible. A follow-up study was performed. Patient records were analyzed retrospectively for perioperative parameters and early postoperative complications. Long-term outcome was assessed during follow-up visits in clinic and a final telephone interview. Outcome was compared between the groups: group 1 (G1): age <12 months, group 2 (G2): >12 months. Fisher's exact test and t-test were used for statistical analysis and p<0.05 was considered significant.
Results: Between 7/2004 and 9/2012, a total of 22 laparoscopic transperitoneal heminephrectomies (21 upper pole and 1 lower pole) were performed in 20 patients (2 bilateral cases) (G1: 12 cases, G2: 10 cases). Median age at surgery was 7.6 (3–11) months in G1 and 37 (15–128) months in G2. Average operative time was 162 (81–220) min in G1 and 210 (90–265) min in G2 (p=0.035). All procedures were completed laparoscopically. Early postoperative complications included one urinoma in G1 which was surgically revised. No further surgical procedures were necessary in any other patients. Median postoperative hospital stay was 3 days (G1: 3.5 days; G2: 3.0 days). During long-term follow-up (median 64 months) there were no complications except febrile urinary tract infections, which occurred in both groups (G1: 1/12 (patient with additional posterior urethral valves), G2: 2/10) (p=0.57). None of the patients underwent uretero-cysto-neostomy.
Conclusion: Laparoscopic heminephrectomy for duplex kidneys is safe and feasible even in small infants. Long-term results are excellent irrespective of patient age.
LAPAROSCOPIC SURGERY IN SEXUAL DIFFERENTIATION DISORDERS
Aim: To share the experiences of laparoscopic surgery which provides excellent visualization of internal genital organs, tissue sampling for histopathological evaluation and application of definitive surgery in the management of sexual differentiation disorder.
Patients and Methods: The records of patients who were diagnosed as sexual differentiation disorders between January 2005 and June 2012 were retrospectively evaluated. Data about genetic gender, preferred gender, diagnosis and procedure were evaluated and among these, data of patients who were undergone laparoscopic surgery were collected.
Results: Laparoscopy was used in diagnosis and treatment of fifteen children with sexual differentiation disorders and five of the patients were reared as male and ten of them were reared as female (Ten children with 46XY, four children with 46XX, one child 45X0). The children were diagnosed as congenital adrenal hyperplasia (n=6), complete androgen resistance syndrome (n=3), partial androgen resistance syndrome (n=3), complete gonadal dysgenesis (n=2) and mixed gonadal dysgenesis (n=1). Mean age was 13 (range 4 months-17 years). Hysterosalphingectomy was performed to six of the children, colovaginoplasty to six, gonadal biopsy to three (total abdominal hysterectomy and bilateral salphingooopherectomy to one of them and gonadectomy to other) and gonadectomy to three children. There were no operative or postoperative complications except vaginal stenosis in one of the patients. Surgical results were satisfactory regarding both function and cosmesis.
Conclusion: Laparoscopic surgery should be treatment of choice in patients with sexual differentiation disorders since it provides excellent visualization of internal genital organs, biopsy can be safely and easily performed for histopathological diagnosis and it causes minimal morbidity and excellent cosmesis.
LAPAROSCOPIC BILATERAL PHEOCHROMACYTOMA EXCISION
A fifteen-year-old boy with the symptoms of excessive sweating, polydipsia, polyuria and hypertension was diagnosed as bilateral pheochromacytoma. Laparoscopic bilateral tumoral excision was performed. The patient had no problem in the follow-ups. The aim is to emphasize the feasibility of laparoscopy in malignant tumoral lesions even in bilateral cases by demonstrating the surgical details with this HD video presentation.
LAPAROSCOPIC BILATERAL URETERONEOCYSTOSTOMY
Two-year-old girl who had recurrent urinary tract infection was diagnosed as bilateral grade V vesicoureteral reflux. Laparoscopic bilateral extravesical ureteroneocystostomy was performed. Operating time was 90 minutes. There was no intraoperative or postoperative complication. The aim is to present the feasibility of laparoscopic bilateral ureteroneocystostomy by showing technical details of this surgery.
LAPAROSCOPIC COLOVAGINOPLASTY IN SEXUAL DIFFERENTIATION DISORDERS
Aim: To evaluate the feasibility and results of laparoscopic colovaginoplasty in vaginal reconstruction.
Patients and Methods: The records of patients with sexual differentiation disorders who were diagnosed and treated in pediatric surgery were retrospectively evaluated. Diagnosis of diseases, operating time, period of hospital stay, presence of intraoperative or postoperative complications, cosmetic results were determined.
Results: The mean age of children with sexual differentiation disorders (complete androgen resistance syndrome (n=3) and partial androgen resistance syndrome (n=3)) who were undergone laparoscopic colovaginoplasty was 15 (11–17 years). Median of operating time was 150 minutes (120–300 minutes). Median of hospital stay was 6 days (4–6 days). There was no intra-operative complication. There was no postoperative complication except one patient with vaginal stenosis who was treated with series of vaginal dilatations.
Conclusion: Laparoscopic colovaginoplasty should be treatment of choice in vaginal reconstruction with low complication rates and excellent cosmetic results. Prospective evaluation of sexual functions will fortify the present data.
LAPAROSCOPIC PYELOPLASTY FOR SECONDARY URETEROPELVIC JUNCTION OBSTRUCTION IN CHILDREN
ABSTRACT WITHDRAWN
ANALYSIS OF OUTCOMES USING DEXTRANOMER-HYALURONIC ACID (DHA) INJECTIONS FOR THE TREATMENT OF MACE OR MITROFANOFF INCONTINENE AS WELL AS BLADDER NECK INCONTINENCE FOLLOWING CONTINENT UROLOGICAL RECONSTRUCTION PROCEDURES
ABSTRACT WITHDRAWN
THE TREATMENT OF URINARY STONES IN CHILDREN: OUR EXPERIENCE IN ENDOSCOPIC LASER TREATMENT
ABSTRACT WITHDRAWN
ENDOSCOPIC TREATMENT WITH HYALURONIC ACID IN DEXTRANOMER AND VESICOURETERAL REFLUX ALSO COMPLICATED BY HIGH-GRADE DOUBLE URINARY DISTRICT
Introduction: Since June 2010, we entered into our treatment protocol of vesico - ureteral reflux, endoscopic treatment in all children over the years of life or even the smaller ones in the event of poor compliance in the management of antibiotic prophylaxis.
Materials and Methods: Over the last 24 months, in our structure, we have treated endoscopically with dextranomer and hyaluronic acid reflux 32 patients with high-grade (IV - V) with or without double urinary district. Twenty-two patients had reflux of high degree and the remaining ten had double urinary district for a total of 54 units refluxing. Twelve patients had reflux nephropathy. The treatment consisted of the injection endoscopic, below the ureteral meatus, dextranomer and hyaluronic acid, by needle drive, lifting the bladder mucosa with the needle itself, so as to favor the detachment and thus the elongation of the junction uretero - bladder and the creation of an appropriate niche for the wheal of organic material - compatible (Technique Nicola Capozza). The molecule of dextranomer combined with hyaluronic acid ensures a good biocompatibility, good tissue tolerance, a valid duration in time, does not tend to migrate from the injection site, optimal ease of use, excellent success rate. The radiological check were performed at least four months after injection to avoid false successes, using traditional cystography, nuclear cystography and ultimately through the ultrasound dynamic (before and after emptying the bladder).
Results: In twenty-four patients (16 with high degree and 8 with double urinary district) there has been the healing of reflux, in 16 of these children, it was necessary to proceed more endoscopic treatments (maximum of three).
Conclusions: The use of endoscopic treatment of vesicoureteral reflux - ureteral, in our experience, is pushed even, in extreme cases, in fact just recently allowed us to obtain good results with minimal invasiveness, without creating discomfort for the child and his family, avoiding the surgery that has most certainly impact the psychological, physical, and subjects the child to a greater stress. Besides all this, we have reduced the time course of administration of antibiotic prophylaxis. Lately, after injection, prescribe the antibiotic for five days, followed by administration up to control only cranberry.
LAPAROSCOPIC TREATMENT OF VARICOCELE WITH AND WITHOUT LYMPH SAVINGS: OUR EXPERIENCE
Introduction: Over the past three years we have subjected to laparoscopic treatment of all cases of varicocele requiring treatment. We display the results of the technique with and without saving the lymphatic vessels.
Materials and Methods: From 31 October 2009 to 31 October 2012 we treated laparoscopically 38 boys aged between 10 and 21 years with an average of 16 years. In agreement with the international guidelines, the indications for intervention have been the degree of varicocele and/or the presence of clinical signs or alterations ultrasound of the testis. Our philosophy has always been, however, to try to intervene closest possible at the end of pubertal development, as we have seen that this leads to a marked reduction in the recurrence of the disease. Of all the 38 cases operated, 25 had a grade III varicocele, the remaining 13 had a grade II. Testicular ultrasound abnormalities were present in 12 patients. Clinical signs were manifested by 8 guys and they were: sense of weight, discomfort when sitting, pain that is accentuated by standing for a long time. In 10 cases there were problems related to relational aesthetic problems caused by the presence of varicocele. The technique used was that of traditional laparoscopic, using three trocars, the umbilical 12 mm., one of 5 mm. in the right iliac quadrant and another 5 mm. sovrapubic. The induction of pneumoperitoneum has been practiced by Verres needle. We approached the spermatic plexus through a tiny opening in the posterior parietal peritoneum. Initially we practiced tying the spermatic plexus in its entirety without saving the lymphatic vessels in 22 patients. Recently, we performed ligation of the spermatic vein only with saving the lymphatic vessels in the remaining 16 cases. We performed ligation of the vessels always using four metal clips, two on each side of the complex, so we always cut the spermatic plexus.
Results: We had no recurrence of varicocele with both techniques. The incomplete emptying of the spermatic vein occurred in 20 cases. Indrocele in 4 cases which is then resolved spontaneously in 6–12 mesi. In all symptomatic cases there was complete disappearance of the symptoms. We did not notice any difference in quality and results between the two techniques, one with binding in its entirety spermatic plexus and the saving of the lymphatic vessels. We think that the laparoscopic treatment is the best approach to varicocele and give results safer than other techniques used for the treatment of this pathology.
A TECHNICAL INNOVATION IN RETROPERITONEOSCOPIC DISMEMBERED PYELOPLASTY IN THE PRESENCE OF LOWER POLE CROSSING VESSELS
Aims and Objectives: Traditionally during a dismembered pyeloplasty, in the presence of lower pole crossing vessels, the pelviureteric anastomosis is made anterior to the crossing vessels to prevent recurrent obstruction. As an increasing number of children undergo laparoscopic procedures we report a technique, which allows this same manoeuvre to be achieved during a retroperitoneoscopic pyeloplasty.
Materials and Methods: This technique has been performed at our institution by a single surgeon for several cases of pelviureteric junction obstruction secondary to lower pole crossing vessels.
Reconstructive technique: Following standard retroperitoneal dissection for pyeloplasty a stay suture is placed on the ureter distal to the site of obstruction and the ureter is divided proximal to the stay suture. A longer length stay suture is placed on the renal pelvis and the pelvis divided distal to the stay suture in the usual manner to excise the pelviureteric junction. The long stay suture is then passed anterior to the crossing vessels thus taking the pelvis anterior to the vessels. A stay suture is placed through the medial aspect of both pelvis and ureter and is sutured to the psoas muscle. This retains the pelvis anterior to the vessels, approximates the ureter and renal pelvis and brings the site of anasomosis distal to the vessels thus improving vision. Anastomosis of the ureter to pelvis can then proceed in the usual manner anterior to the crossing vessels.
Results: This technique proceeded well in all patients with no increase in complications or operative time. The intra-operative and post-operative course was similar to that of patients undergoing retroperitoneoscopic pyeloplasty for intrinsic pelviureteric junction obstruction.
Conclusion: With the aim of improved cosmesis and reduced post-operative pain many children now undergo a laparoscopic rather than an open pyeloplasty and this is performed either by the transperitoneal or retroperitoneal route. Anastomosis of the ureter and pelvis anterior to lower pole crossing vessels is easily accomplished via open and transperitoneal routes however it is more challenging during retroperitoneoscopic pyeloplasty due to the position of the instruments posterior to the renal pelvis. Completing the pyeloplasty retroperitoneally however offers advantages in terms of the potential sequelae of urinary leak and the reduced risk of post-operative ileus and adhesions.
We therefore recommend this described technique as it enables a dismembered retroperitoneoscopic pyeloplasty with anterior placement of the anastomosis to be achieved in the presence of lower pole crossing vessels. The long-term outcome needs further evaluation.