
Abstract
Abstract
Background:
To study the effects of low tidal volume with positive end-expiratory pressure (PEEP) on arterial blood gases of patients undergoing laparoscopic urologic surgeries.
Subjects and Methods:
Eighty-six laparoscopic urologic patients were enrolled in this study. Patients were randomized into two groups according to the ventilatory settings. In the conventional group (Group C) (n=43), the tidal volume was 10 mL/kg, and the PEEP was set at 0 cm of H2O. In the low tidal volume with PEEP group (Group LP), the tidal volume was 6 mL/kg, with PEEP of 5 cm of H2O. In both groups total minute volume was 6 L/kg. Peak and plateau airway pressure (PPEAK and PPLAT, respectively) and arterial blood gases were recorded before pneumoperitoneum (PNP) (T1) and the first and third hour (T3) after PNP induction and also after extubation in the intensive care unit. Additionally, heart rate, mean arterial pressure, and peripheral O2 saturation of hemoglobin were recorded.
Results:
Heart rate, PPEAK, and PPLAT values were similar in both groups. Partial arterial O2 pressure values measured postoperatively were significantly higher in Group LP, whereas those measured before PNP induction were similar (P=.014 and P=.056, respectively). Compared with the baseline, partial arterial CO2 pressure values measured at T1 and at T3 after PNP induction were significantly higher in Group C than in Group LP (P<.001). The pH values of Group C at T1 and at T3 postoperatively were significantly lower than the values of Group LP (P<.001). Extubation times were significantly lower in Group LP.
Conclusions:
The results of the present study suggest that low tidal volume with PEEP application may be a good alternative for preventing high CO2 levels and yielding better oxygenation and lower extubation times in patients undergoing prolonged laparoscopic urology.
Introduction
U
Several ventilatory strategies have been proposed to prevent intraoperative atelectasis and improve arterial oxygenation in laparoscopic surgeries. Protective ventilation refers to using low tidal volume, often in the range of 4–8 mL/kg of predicted body weight. In fact, 6 mL/kg is the normal physiologic tidal volume in humans. Many investigators have conducted several large randomized trials that have shown that the use of lower tidal volumes is associated with improved outcomes and a reduction in the incidence of ventilatory-induced lung injury.5,6 In addition to the reduction of tidal volume, increasing the level of positive end-expiratory pressure (PEEP) is now considered an integral part of protective ventilation. 7
Although there have been several studies investigating lung-protective ventilatory strategies in laparoscopic surgeries, none of them took longer laparoscopic procedures of urologic operations into consideration. Therefore, we aimed to investigate the effects of low tidal volume with PEEP on arterial blood gases intraoperatively in patients undergoing laparoscopic urologic surgeries.
Subjects and Methods
This study was approved by the Ethics Commitee of the Afyon Kocatepe University Medical Faculty, Afyon, Turkey, on August 6, 2012, with protocol number 147, and written informed consent was obtained from each patient. Eighty-six patients with American Society of Anesthesiologists physical status I–III, between 20 and 75 years of age, undergoing laparoscopic urologic procedures (radical nephrectomy, pyeloplasty, renal cyst decortications, and radical prostatectomy) were prospectively enrolled in this study. Patients with a history of severe cardiorespiratory disease, morbid obesity (body mass index [BMI] of >40 kg/m2), previous lung surgery, and pregnant women were excluded. Patients were randomized into either the conventional group (Group C) or the low tidal volume with PEEP group (Group LP) using a sealed envelope system. In Group C (n=43), ventilatory settings were as follows; tidal volume, 10 mL/kg; PEEP set at 0 cm of H2O. In Group LP (n=43), ventilator settings were as follows: tidal volume, 6 mL/kg; PEEP set at 5 cm of H2O. In both groups, total minute volume was 6 L/minute, the inspiratory to expiratory time ratio was 1:2, and the inspired oxygen fraction was 0.5 (balanced with air).
On arrival in the operating room, patients were monitored (Datex-Ohmeda Avance®; GE Healthcare, Helsinki, Finland) with continuous electrocardiography, pulse oximetry, capnography, central venous pressure, and invasive blood pressure. A standardized anesthetic technique was used in both groups. Patients were premedicated with 0.1 mg/kg of midazolam 1 hour before induction of anesthesia, which was induced with propofol (1–2 mg/kg), fentanyl (1–2 μg/kg), and rocuronium (0.6 mg/kg) and maintained with desflurane, rocuronium, and fentanyl. Mean arterial pressure and central venous pressure were measured via a radial artery catheter and jugular central venous catheter, respectively, in all patients. The magnitudes of PPEAK and PPLAT were obtained directly from the ventilator and were recorded before PNP induction (T1) and at the first and third hour after PNP induction (T2 and T3, respectively). Arterial blood gases also were analyzed at T1, T2, and T3. Additionally, hemodynamic parameters such as heart rate and peripheral O2 saturation of hemoglobin were recorded. If partial arterial CO2 pressure (PaCO2) increased in either study group above 60 mm Hg, the ventilation rate was increased while the tidal volume maintained constant. After completion of surgery, all patients were transported to the anesthesia intensive care unit (ICU). Arterial blood gases also were analyzed after extubation (T4) in the ICU. Operation times, extubation times (times between admission to ICU and extubation) of the patients were also recorded.
Laparoscopic procedures were performed either by the transperitoneal or by the retroperitoneal approach. Patients were placed in the Trendelenburg position. Peritoneal access was created by the Hasson technique during transperitoneal approaches. PNP was adjusted to 14 mm Hg intraabdominal pressure. Like in transperitoneal access, during retroperitoneal approaches, the Hasson method was performed, and retroperitoneal space was created by retroperitoneal balloon dilatators.
Statistical analyses were performed using SPSS software (SPSS version 18; SPSS, Inc., Chicago, IL). Descriptive analyses were evaluated as the mean and standard deviation for normally distributed variables, whereas non-normally distributed variables were evaluated as the median and minimum–maximum. The Mann–Whitney U test was used to compare continuous variables, and the chi-squared test was used to compare categorical variables. The Wilcoxon signed-rank test was used to compare preoperative and postoperative variables. A P value of <.05 was considered to indicate a statistically significant difference.
Results
Among the 86 patients initially enrolled, 81 patients completed the study; 5 patients in Group C were excluded because of severe hypercapnia. PNP was interrupted in these patients until the PaCO2 values were improved. No other surgical complications were recorded. Therefore we evaluated 38 patients in Group C and 43 patients in Group LP.
Patient and operation characteristics are presented in Table 1, and no significant difference was seen among them, except for extubation times between the groups. Extubation times were significantly shorter in Group LP (P<.01) (Table 1).
Data are mean±standard deviation values. There were no significant differences between the groups with respect to demographic and operation characteristics.
P<.05 indicates a significant difference.
BMI, body mass index; Group C, conventional group; Group LP, low tidal volume with positive end-expiratory pressure group.
The hemodynamic data of patients are shown in Table 2. Significant differences were detected in mean arterial pressure and peripheral O2 saturation values of patients between the groups. Heart rate, PPEAK, and PPLAT values were similar in both groups. Partial arterial O2 pressure (PaO2) values measured before PNP and postoperatively were higher in Group LP; however, the difference did not reach significance before PNP induction (P=.014 and P=.056, respectively) (Table 2).
Data are mean±standard deviation values.
P<.05 indicates a significant difference.
bpm, beats per minute; Group C, conventional group; Group LP, low tidal volume with positive end-expiratory pressure group; MAP, mean arterial pressure; PaO2, partial arterial O2 pressure; PNP, pneumoperitoneum; PPEAK, peak airway pressure; PPLAT, plateau airway pressure; SpO2, peripheral O2 saturation of hemoglobin.
Compared with the baseline, PaCO2 values measured at T2 and T3 were significantly higher in Group C than in Group LP (Fig. 1) (P<.001). Also, there was a significant difference in terms of PaCO2 measured postoperatively between the groups (P<.05).
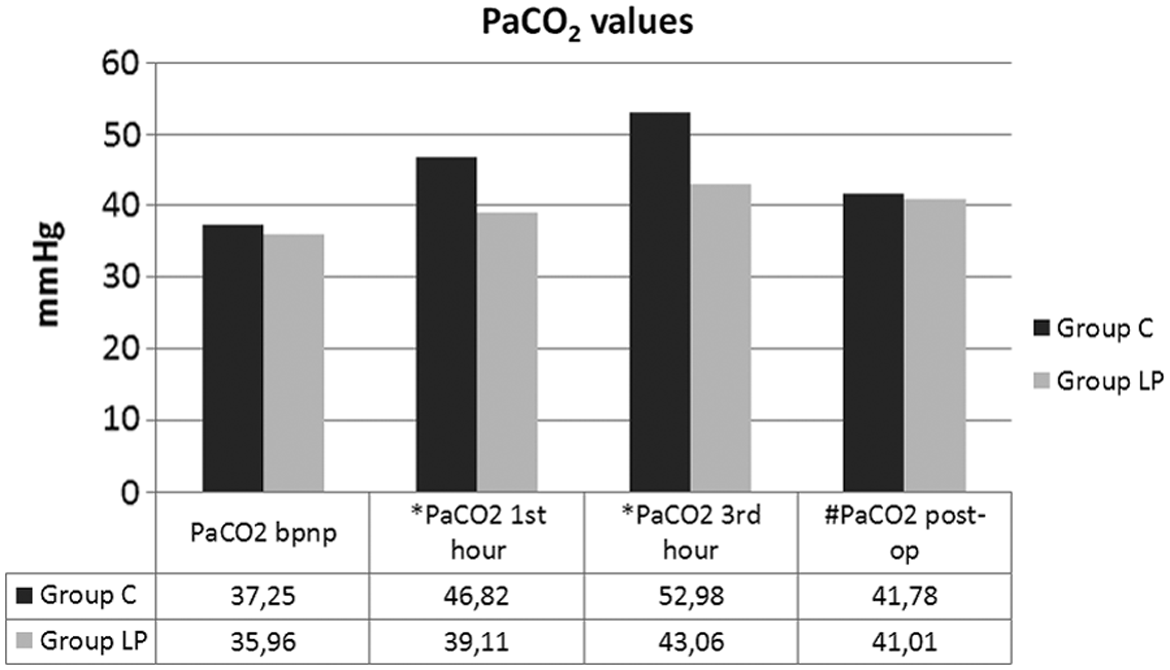
Measurement of partial arterial CO2 pressure (PaCO2) values relative to the operation. bpnp, before pneumoperitoneum; Group C, conventional group; Group LP, low tidal volume with positive end-expiratory pressure group; post-op, postoperatively. *P<.001, #P<.05.
The pH values measured at T1 (before PNP), T2 and T3 (after PNP induction), and T4 (postoperatively) were significantly lower in Group C (Table 3) (P<.001). However, HCO3− values were similar in the two groups.
Data are mean±standard deviation values.
P<.001 indicates a significant difference.
Group C, conventional group; Group LP, low tidal volume with positive end-expiratory pressure group; PNP, pneumoperitoneum.
Discussion
Laparoscopy has been considered as the best approach for many surgical procedures. Decreased postoperative complications and consequently early recovery to a normal level of activity have enabled laparoscopic surgery to become common in various surgical specialities such as urologic procedures. Although all the conventional complications and concerns associated with laparoscopy are applicable to urologic procedures, two unique problems also are identified. First, the urogenital system is mainly retroperitoneal space, and its communications with the thorax and subcutaneous tissue may be exposed to the insufflated CO2. Subcutaneous emphysema occurs frequently in these patients and may extend all the way up to the neck and head.1,8 This complication should be kept in mind before extubation of these patients. Second, the procedures tend to be lengthy, resulting in sufficient absorption of CO2 in the circulation to cause marked acidosis. 8 Because of the significant increases in intraabdominal pressure and intrathoracic pressure as a result of insufflated CO2, a steep Trendelenburg position, and lengthy procedures, general anesthesia is the method of the choice. 1 To the best of our knowledge, there is no study comparing the effectiveness of conventional and low tidal ventilatory strategies for laparoscopic urologic procedures in the literature. The main findings of this study were as follows: (1) Compared with the baseline, PaCO2 values measured at 1 and 3 hours after PNP and postoperatively were lower in patients in whom low tidal with PEEP ventilation was performed. (2) PaO2 values measured postoperatively were significantly higher in Group LP (P=.014).
Laparoscopy procedures require PNP, and prolonged PNP in patients undergoing general anesthesia may cause a continuous decrease in arterial oxygenation due to compressive atelectasis, particularly in gravity-dependent regions of the lungs.9,10 Also, there is clear evidence from animal and human data that mechanical ventilation can induce and exacerbate lung injury, and thus the current standard of care is the use of a lung-protective ventilation strategy in patients suffering from acute lung injury or adult respiratory distress syndrome. 11
Protective ventilation refers to the use of low tidal volume, often in the range of 4–8 mL/kg of predicted body weight. Many investigators have conducted several large randomized trials that have shown the use of lower tidal volume is associated with improved outcomes and a reduction in the incidence of ventilatory-induced lung injury.5,6 However, evidence also exists that mechanical ventilation can be injurious to the lung and organ systems in patients without acute lung injury or adult respiratory distress syndrome. Determann et al. 12 recently performed a randomized trial comparing the conventional rate of 10 mL/kg with a rate of 6 mL/kg in 152 critically ill patients; they measured cytokine levels in bronchoalveolar lavage fluid and plasma and observed the development of acute lung injury/adult respiratory distress syndrome, duration of ventilation, and overall mortality. In their study more patients developed lung injury in the conventional group (13.5% versus 2.6%), and plasma interleukin-6 levels were more pronounced in the low tidal volume group. 12 A trial by Lee et al. 13 in a surgical ICU randomized 103 patients to 12 mL/kg versus 6 mL/kg; they documented a reduction in pulmonary infections, a trend toward a reduced ICU length of stay, and reduced duration of intubation in the group with lower tidal volume. In our study we compared the conventional rate of 10 mL/kg with 6 mL/kg (Group LP) in laparoscopic urologic patients. We documented better oxygenation in Group LP postoperatively.
In addition to the reduction of tidal volume, increasing the level of PEEP is now considered an integral part of protective ventilation. Lower tidal volume might lead to atelectasis, especially if PEEP is low or not used at all. Sufficient PEEP must be used to minimize atelectasis and to maintain oxygenation. 14 Choi et al. 15 found that in patients with normal lungs undergoing prolonged abdominal operations, the use of smaller tidal volumes (6 mL/kg) with PEEP prevented increases in levels of procoagulant factors in bronchoalveolar lavage fluid indicative of lung injury that were associated with larger tidal volumes (12 mL/kg) with the absence of PEEP. In another study comparing conventional and protective ventilation in critically ill patients without lung injury, Pinheiro de Oliveria et al. 16 randomized patients to ventilation with either 10–12 mL/kg or 6–8 mL/kg of predicted body weight; in both groups a PEEP of 5 cm of H2O was applied. At 12 hours postventilation, levels of inflammatory markers (tumor necrosis factor and interleukin-8) in bronchoalveolar lavage fluid were significantly higher in the larger tidal volume group. In a recent study, Lee et al. 17 investigated the optimal level of PEEP to maintain adequate arterial oxygenation and hemodynamics, and they found that a PEEP of 7 cm of H2O was associated with greater improvement of PaO2 without causing excessive PPEAK. Talab et al. 18 showed that PEEP values of 10 cm of H2O applied after recruitment vital capacity maneuvers was more effective than zero end-expiratory pressure or PEEP of 5 cm of H2O for prevention of postoperative atelectasis and was associated with better oxygenation in obese patients undergoing laparoscopic surgery. In contrast, Azab et al. 19 concluded that PEEP (5 cm of H2O) prevents deoxygenation during PNP and leads to a lower atelectasis score on computed tomography scan. In obese patients with a BMI of >30 kg/m2 who had lower functional residual capacity, PEEP of 5 cm of H2O may not be enough to reopen collapsed alveoli after induction of anesthesia. Our study used nonobese patients with a BMI of <40 kg/m2; except for 1 patient with a BMI of 40 kg/m2, the other patients had a BMI<31 kg/m2 in this study. We used a PEEP of 5 cm of H2O, and we found better oxygenation postoperatively in the low tidal volume with PEEP group; airway PPEAK values were not seen above 21 cm of H2O, and PPLAT values were lower than 17 cm of H2O as well, in each group.
Physicians' additional concerns for hypercapnia and acidosis have led to barriers in implanting protective ventilation. 20 Permissive hypercapnia should be tolerated in patients undergoing protective ventilation, although to what degree is still unclear. And, also due to the reduction in tidal volume and subsequent minute ventilation, CO2 levels are often elevated in these patients. To avoid severe respiratory acidosis (pH<7.20), the respiratory rate needs to be increased, often up to 30 breaths/min. 21 We kept a high rate of respiration at the beginning of the study in Group LP in anticipation of high CO2 levels because of low tidal volume and urologic cases' predisposition to acidemia. We also increased the respiration rates when the PaCO2 values were over 60 mm Hg in Group C. If we could still not reduce PaCO2 values, we had to stop PNP until the PaCO2 values improved. We had severe acidemia that improved by interrupting the surgery for 5 patients in Group C. But, we did not have to intervene because of PaCO2 values in Group LP during the study. Besides, we found that PaCO2 values were higher and pH values were lower in Group C significantly. Using high respiratory rates decreases the expiratory times, and this may lead to less time for the patient to exhale. When the expiratory time is insufficient to completely exhale, inadequate emptying between breaths causes hyperinflation. This is called dynamic hyperinflation, a common problem in patients with status asthmaticus. Dynamic hyperinflation creates intrinsic PEEP and elevates PPLAT, which can lead to cardiovascular collapse and barotraumas. Adjustment of ventilator settings while maintaining a PPLAT of <30 cm of H2O, shortening inspiratory time, increasing expiratory time, decreasing tidal volume, and decreasing respiratory rates may help in decreasing air trapping. 22 In this study, patients with respiratory diseases such as asthma were excluded. Severe PPLAT values, which constitute the best assessment of hyperinflation, 23 were not seen in either group (mean PPLAT values were <17 cm of H2O) in our study. Additionally, we did not change the inspiration/expiration time ratio in either group.
In the present study, patients were transferred to the ICU at the end of the surgery, and they were extubated when appropriate conditions (hemodynamic stability with no significant arrhythmia, patient awake and responding to commands, and adequate respiratory parameters [inspired oxygen fraction <45%, PEEP <7.5 cm of H2O, respiratory rate >10 breaths/minute, and minute ventilation >100 mL/kg/minute]) were supplied. Extubation times were significantly lower in Group LP.
In conclusion, the results of the present study suggest that low tidal volume with PEEP application may be a good alternative for preventing high CO2 levels and yields better oxygenation and lower extubation times in patients undergoing prolonged laparoscopic urologic surgeries.
Footnotes
Disclosure Statement
No competing financial interests exist.