
Abstract
Abstract
Introduction:
The objective of this study was to determine whether or not a navigation grid (NG) with a coordinate system overlaid on a laparoscopic display might allow attending surgeons to more easily and precisely direct their assistants' instruments to specific sites in a simulated laparoscopic field.
Materials and Methods:
In this randomized, crossover study, we evaluated the impact of the NG on an individual's performance in a target identification task. One hundred thirty pins served as targets in a standard laparoscopic box trainer. An instructor guided 30 naive subjects to locate five randomly selected targets each, either with verbal instructions alone or with verbal instructions supplemented by a localizing NG. The NG appeared on both the instructor's and the participants' monitors, but the randomly selected targets were visible only to the instructor. Each participant performed 10 trials alternating between with and without the NG. The outcome measure was the interval (in seconds) from when the laparoscopic instrument was first visible in the field to when the subject grasped the correct target with forceps.
Results:
The mean time to identify each selected target was significantly shorter with the NG (9.150±3.43 seconds) than without (12.53±4.89 seconds) (P<.0001). This effect was sustained throughout the learning curve.
Conclusions:
The use of the NG appears to improve efficiency in guiding an instrument to randomly identified targets within a laparoscopic field. The use of an NG may reduce the time required to move instruments to specific sites during surgery.
Introduction
E
Previous investigators have reported that trusting an assistant to accurately direct instruments and carry out instructions is essential to successful laparoscopic outcomes.5–7 For example, in a study of laparoscopic cholecystectomies, instructor-directed maneuvers were deemed critical in 25% of all spoken exchanges during the initial dissection phase, especially with regard to the positioning of instruments and the direction of tissue manipulation. 8 The difficulty of such tasks is exacerbated by the inherent nature of laparoscopic surgery that necessitates indirect observation and manipulation via a monitor.9–12
We hypothesize that a projected navigation grid (NG) that can be integrated into the surgical camera and superimposed on the video monitor image might allow attending surgeons to give more precise instructions to their assistants to more efficiently position and move laparoscopic instruments to a specific target.
Materials and Methods
In this randomized, crossover study, we evaluated the impact of the use of an NG (Karl Storz Endoscopy-America Inc., El Segundo, CA) on an individual's performance in a target identification task. The study was conducted at the Arizona Simulation Technology and Education Center at the College of Medicine, University of Arizona (Tucson, AZ), and was performed under the auspices of the Institutional Review Board of the University of Arizona and in compliance with its regulations and requirements.
Study participants
In total, 30 procedurally naive volunteers were entered into the study and completed an informed consent form. None of them had any previous experience of operating laparoscopic equipment. Each of the 30 participants received a scripted orientation of the laparoscopy equipment and a description of the target identification task. Characteristics of the participant population are outlined in Table 1. All participants were over 18 years of age.
Each participant performed a total of 10 trials with five randomly selected targets, alternating between moving to that target with and without the NG. To control for any learning curve effect, we randomized participants into two groups, according to whether they began with (n=13) or without (n=17) the grid, and allowed no practice trials.
Experimental design
The test bed for the target identification task consisted of 135 identical black pins (1/8 inch in diameter), embedded in a silicone base plate and placed in a laparoscopic box trainer. Evenly positioned, the pins created a multitude of identical targets with a density of 6.5 targets per square inch. The laparoscope's position was fixed so there would be no changes in the size of the displayed field. The instructor and each of the study participants had their own video monitor, positioned so that the participant could not see the instructor's display. Only the instructor could see which target had been randomly selected for each trial so the participant could rely only on the verbal instructions to navigate to the designated target.
For each participant, the five separate targets within the array were selected using a random number generator computer program. Each target was presented twice during the course of the 10 trials, once with the NG and once without. The five randomly selected targets were then randomized again for order of appearance in the 10 trials to minimize any learning effect. The NG consists of a 3×5 coordinate system projected through the camera onto the surgical display. The individual quadrants are designated by letter and number assignment (e.g., A1, B4, C2). The NG can be activated from the camera and adjusted to three sizes, making up 50%, 70% and 100% of the surgical display. For the sake of this study, we used the 70% mode only.
Participants were given a standard laparoscopic forceps instrument (Karl Storz Endoscopy-America, Inc.) with which to grasp and identify the correct target as instructed. All participants were told to start when ready by inserting the instrument into the box trainer. Timing for each trial began when the instrument was first introduced into the surgical field and ended when the participant had successfully grasped the designated target. The time from introduction of the laparoscopic instrument to grasping the designated target was the primary end point.
The instructor guided the participants either with spoken instructions only or with spoken instructions supplemented by the localizing NG. Two experimental groups were created according to the type of verbal commands that the instructor could use to direct the subject to the designated target. In Group 1 (n=20), the instructor was limited to only four simple directional commands: namely, “up,” “down,” “left,” and “right.” When the grid was added, the instructor was allowed to use the coordinates of a specific quadrant (e.g., A5) as an additional directional cue. The instructor could also only use the same four simple directional commands to guide the participant to the target within that quadrant. In Group 2 (n=10), the instructor was not limited in any way as to what directional commands he was allowed to use to guide participants to the target. When the grid was added, the instructor could likewise use the coordinates along with any other verbal commands. Figures 1 and 2 depict the experimental setup.

Instructor's navigation grid with a marker on the designated target.

Experimental setup: the instructor in the foreground verbally guiding the assistant to a designated target using the surgical navigation grid.
The collected data from each group were analyzed statistically with paired repeated-measures t tests, using a P value of <.05 to indicate significance. Between-groups data were analyzed using unpaired t tests. The data are presented as mean±standard deviation values. This analysis was performed using the statistical software SPSS version 20.0 (SPSS, Chicago, IL).
Results
The use of the NG significantly decreased the time required from insertion to grasping the correct target regardless of the type of instructional commands used. In Group 1, the use of the NG produced a 27% reduction in mean task completion time of 9.15±3.43 seconds with the NG versus 12.53±4.89 seconds without the NG (P<.0001). Lifting the limitation on the type of instructional commands did not eliminate the benefit of the NG. In Group 2, use of the NG produced a 44% reduction in mean task completion time of 6.32±2.44 seconds with the NG versus 11.36±5.21 seconds without the NG (P<0.0001). In both groups this effect was sustained throughout the learning curve over the course of 10 trials (Fig. 3).
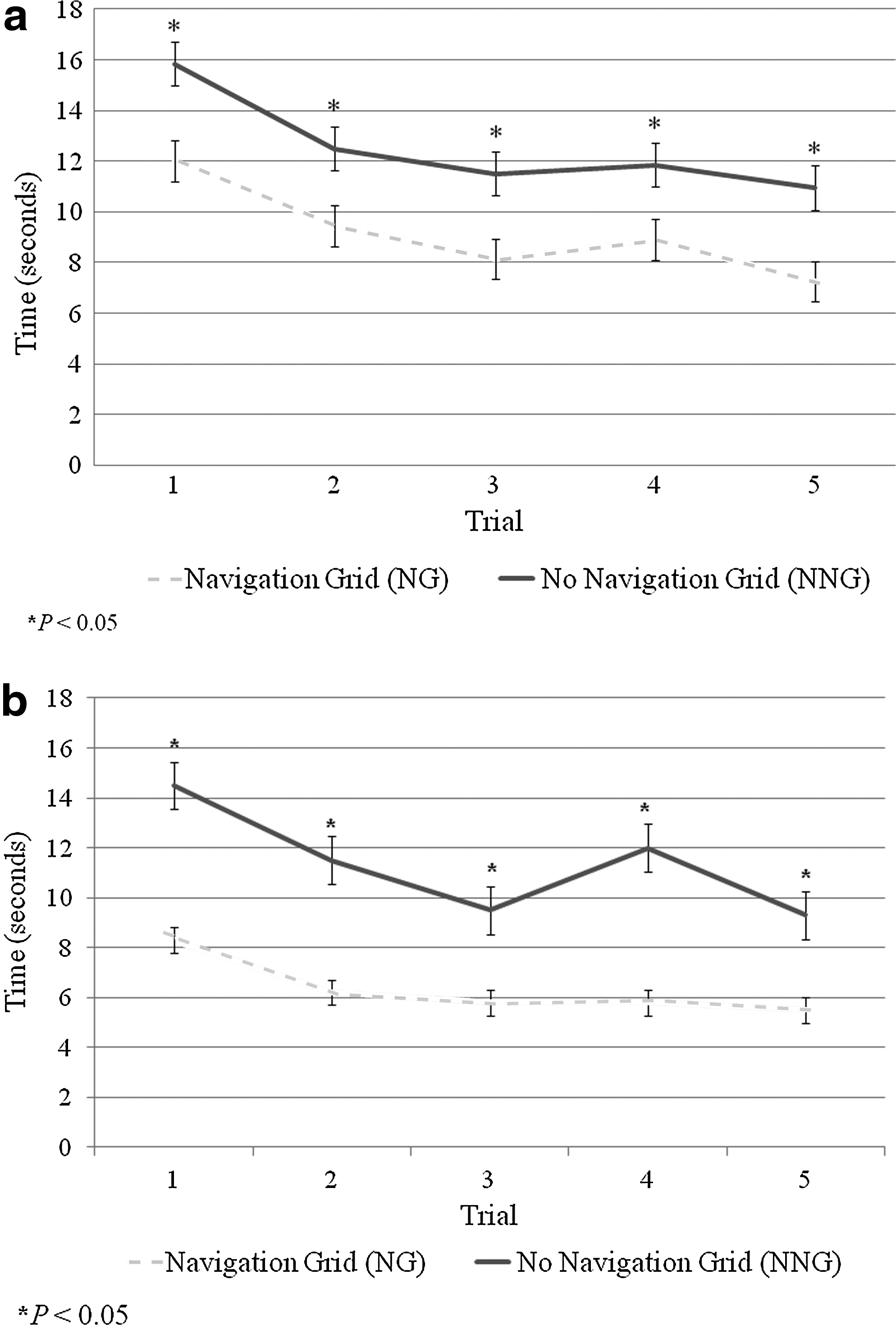
Learning curve for the navigation grid and no navigation grid scenarios:
There was no difference between Group 1 and Group 2 in the mean time required to locate a target without use of the NG (P=.1787). With use of the NG, participants in Group 2 were able to identify the target significantly faster than participants in Group 1 (P<.0001). We noted no significant difference in target identification time by gender, by education level, or by whether a participant started the trials with or without the NG.
Discussion
Previous studies have shown that localization systems can be useful in laparoscopic surgery. Using a head-mounted infrared signal system with a passive marker on the surgical monitor, Jayaraman et al. 13 demonstrated a reduction in the time required for an instructor to guide an assistant to a designated target. This study used anatomic targets on a photograph and suggested that localization systems might be advantageous even in actual laparoscopic surgical fields—something our study did not address. The head-mounted system, however, did have several drawbacks. First, and most notable, is that the infrared marker required the instructor to maintain a focused gaze on the target displayed on the monitor until the assistant had identified it, and thus the target localization did not permit the surgeon to move his head freely. The second drawback of this infrared system was that it required both a special monitor and sensors and calibration for the infrared markers, thus adding a significant amount of surgical preparation time. Finally, it required the surgeon to wear a head-mounted apparatus throughout the case, something that can prove cumbersome.
In contrast, the NG used in our study does not require the instructor to make unnecessary head movements to guide a participant's instrument to a specific target. As a simple NG superimposed on the image displayed on the video monitor, it is in either “on” or “off” mode. The surgeon can activate the grid by a button, accessible in the sterile surgical field, on the top of the camera head. This feature eliminates the disadvantages of extraneous voice command systems and of separate foot activation switches reported by other investigators.12,14,15
The grid lines in our NG were faint enough not to interfere with the ability to visualize both targets and instruments in the surgical field while still allowing the number and letter designations of the grid coordinates to remain clearly visible. The coordinate system appears to reduce localizing time by permitting the assistant to move rapidly to a specific region where targets are located rather than having an instructor verbally direct the assistant through the surgical field and past irrelevant targets from the moment of entry into the surgical field. In Group 1, we attempted to isolate the effect of the NG by standardizing the verbal commands that an instructor was permitted to use. We realized that this method might provide an unfair advantage to the NG by limiting the verbal commands available to the instructor. Group 2 had no limitations on what verbal cues the instructor could use. Nonetheless, the benefit of the NG was maintained even in Group 2.
The NG does, however, have some drawbacks. It can be projected in its present configuration in only three sizes (100%, 70%, or 50% of the surgical monitor). Because the grid is integrated into the video camera, at higher grid magnifications the entire camera head would have to be moved in order to locate a target on the periphery of the surgical field. Moreover, the NG does not permit the instructor to zoom to scale, a feature that might have become useful at higher camera magnifications. Furthermore, even though the instructor was able to use the NG to designate a specific area of the surgical field where the selected target was located, it did not completely eliminate the use of simple verbal commands, especially with a large number of identical targets in each quadrant within the grid.
Nonetheless, the use of the NG—clearly superimposed on a simulated surgical field and easily viewed through the laparoscope—appears to reduce the amount of time it takes for an assistant to be directed to a specific target independent of whatever kinds of verbal cues are used by an instructor. Further investigations with the NG are planned to see if similar advantages are consistently seen when used by a surgeon and his or her assistant in an actual surgical laparoscopic field. We plan to evaluate whether the use of an NG can facilitate surgical coordination and reduce overall operative time.
Conclusions
The use of a projected NG with labeled coordinates significantly reduced the average amount of time it took for an assistant to find a target designated by an instructor. This advantage was sustained throughout the learning curve and persisted regardless of the type of additional verbal commands used by the instructor. Further studies are needed to confirm whether the advantages of an NG remain significant in actual laparoscopic procedures.
Footnotes
Acknowledgments
This research project, sponsored by an unrestricted educational grant by Karl Storz Endoscopy-America Inc. to the College of Medicine, University of Arizona, was completed at the Arizona Simulation Technology and Education Center, Tucson, AZ. A.J.H. was the Principal Investigator. This project has not previously been presented at a professional meeting.
Disclosure Statement
H.P. has a familial relationship with an employee of the sponsoring entity, Karl Storz Endoscopy-America Inc., which could potentially be perceived as a conflict of interest. All other investigators, including the Principal Investigator and senior author (A.J.H.), have no conflicts of interest or financial ties to disclose.