
Abstract
Abstract
Purpose:
To evaluate surgical outcomes of laparoscopic pyelolithotomy (LP) and percutaneous nephrolithotomy (PCNL) in managing multiple renal stones in various parts of the pelvocalyceal system.
Subjects and Methods:
From February 2004 to December 2011, 45 patients underwent LP, and 39 underwent PCNL for treatment of pelvic stone(s) with calyceal stone(s). Differences in demographics, perioperative data, and complications were compared between LP and PCNL patients. The primary end point in this study was the stone-free rate in a single session.
Results:
Stone-free rates were 91.1% and 64.1% in the LP and PCNL groups, respectively (P=.003). Mean operation time was longer in the LP group (P<.001). Mean change in hemoglobin level (P<.001) as well as postoperative analgesics usage (P=.022) was significantly better in the LP group. However, mean estimated blood loss (P=.112), mean change in creatinine level (P=.172) and estimated glomerular filtration rate (P=.395), and mean length of hospitalization (P=.842) were similar in both groups. The PCNL group had more overall complications.
Conclusions:
LP was safer and more effective than PCNL according to our study. Therefore, LP may be a feasible modality in managing multiple complex renal stones in various parts of the pelvocalyceal system.
Introduction
A
Recently several studies reported their experiences with the laparoscopic approach in properly selected patients with renal stones, and some of them demonstrated that laparoscopic pyelolithotomy (LP) is comparable to PCNL in terms of surgical outcomes for removing solitary renal pelvic stones.2–4 Despite such findings, however, many authors still assert that LP is merely an alternative modality for PCNL and that indications for LP should be restricted to single, large renal stones associated with ureteropelvic junction obstruction, extrarenal pelvis, or previous renal surgery.4,5
There have been efforts to improve surgical outcomes for complex renal stones, including multimodal minimally invasive techniques (PCNL combined with retrograde flexible ureteroscopy, retrograde flexible nephrolithotripsy, multiple access tracts during PCNL, etc.),6,7 but these modalities often resulted in unsatisfactory stone-free rates in the treatment of complex renal stones. Although a recent study did publish excellent results with LP for complex renal stones in a few cases, 8 there have been few comparative studies between LP and PCNL for multiple complex renal stones in a considerable number of cases.
We evaluated the surgical outcomes of LP and PCNL in patients with multiple renal stones in various parts of the pelvocalyceal system in a single session.
Patients and Methods
From February 2004 to December 2011, 45 consecutive patients underwent LP, and 39 underwent PCNL as first-line treatment for multiple renal stones in various parts of the pelvocalyceal system (sum of the maximal diameter of pelvic and calyceal stones, ≥20 mm). Patients with solitary kidneys, previous abdominal surgery, malignancy, or coagulopathy were excluded from this study. The operation method was based on anatomical features of the kidney. LP was mainly preferred in patients with impacted pelvic stones with extrarenal or dilated pelvis (Fig. 1). Clinical data from eligible patients were retrieved from medical records and retrospectively reviewed after approval (protocol number 06-2011-110) by the Institutional Review Board of our institution.
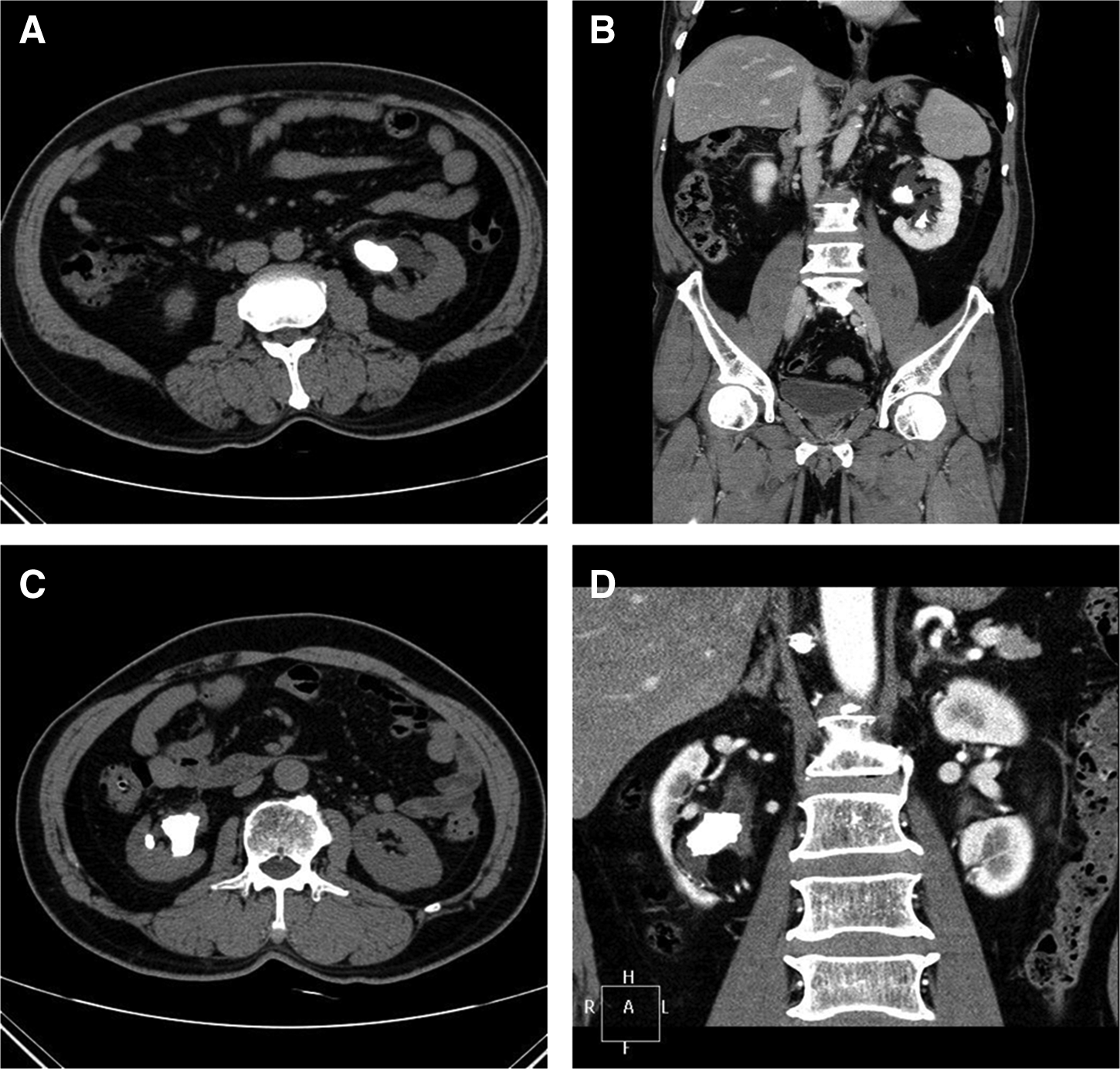
Preoperative computed tomography scans of pelvic stones with extrarenal and dilated pelvis:
Preoperative plain X-rays of the kidney-ureter-bladder (KUB) region were taken with non-enhanced computed tomography (CT) and/or intravenous urograms (IVUs) for all patients. Stone size was defined as the sum of the renal stones' maximal diameters (in mm), which were radiologically evaluated. Demographic parameters and peri- and postoperative surgical outcomes were compared between the LP and PCNL groups. Demographic parameters included age, gender, body mass index, type of surgery (LP or PCNL), and stone characteristics (laterality, size, number, and location). Preoperative laboratory tests included serum hemoglobin and creatinine levels, coagulation panel, urinalysis, and urine culture.
LP technique
All procedures were performed via the transperitoneal route. Patients were placed in the flank position under general anesthesia. After formation of the peumoperitoneum using a Veress needle, the primary port of the camera was placed 2 cm below the umbilicus and lateral margin of the rectus muscle. A 12-mm port for dissection at the anterior axillary line of the umbilicus level and a 5-mm port 7–8 cm cephalad to the primary port were placed under laparoscopic view. The renal pelvis was fully exposed and incised vertically using a number 11 blade, and the pelvic stone was then retrieved using grasping forceps. The entire collecting system was explored through one of the instrument ports using a flexible nephroscope, and calyceal stones were retrieved using a stone basket. We did not use intraoperative fluoroscopy routinely. The retrieved stones were collected in a hand-made rubber basket and pulled out. A ureteral stent was inserted over the guide wire through the pyelotomy site. The pelvis was closed using interrupted sutures using 4/0 polyglycolic acid, and a Jackson–Pratt drain was placed through the 5-mm port and left in the perinephric area.
PCNL technique
Before the surgery, the access tract was applied by the radiologist on the day before the operation. After the patient was placed under general anesthesia, ureteral stenting was indwelled in the lithotomy position, and the patient then was turned to the prone position. Tract dilation was performed with a high-pressure balloon dilator. The stone burden was fragmented with a pneumatic lithotriptor, and stone fragments were retrieved using grasping forceps under a nephroscope. A ureteral stent was inserted through the nephrostomy site using a guide wire. A 24 French nephrostomy tube was placed, and a fluoroscopic nephrostomogram was done to evaluate the stone-free status.
A postoperative X-ray of the KUB region was immediately performed to evaluate the initial stone-free state. Thereafter, we performed CT or IVU to identify residual fragments and delayed excretion at 3 months after surgery. The primary end point in this study was the stone-free rate of a single session, which was defined as having no evidence of residual stones or when clinically insignificant residual fragment was observed on CT or IVU at 3 months postoperatively. Clinically insignificant residual fragment was defined as residual fragments <4 mm, asymptomatic, nonobstructive, noninfectious, and associated with sterile urine. 9
To compare surgical outcomes, we evaluated operation time, estimated blood loss, changes in hemoglobin, serum creatinine, and estimated glomerular filtration rate levels, analgesics usage, length of hospitalization, stone-free rates, and complications.
Clinical parameters were presented as mean±standard deviation values. Continuous variables were assessed with an independent t test, and categorical variables were analyzed with the chi-squared test. All P values were two-sided, and P<.05 was considered statistically significant. All statistical analyses were performed using the statistical software SPSS version 14.0 (IBM, Armonk, NY).
Results
Table 1 compares demographics and perioperative data. Differences in patient characteristics such as age, gender, and body mass index were statistically insignificant between the LP and PCNL groups. The LP group had a slightly higher number of stones (4.36±4.43 versus 2.97±1.97; P=.076). However, mean stone size, which was calculated using the sum of the renal stones' maximal diameters, showed no significant difference between the two groups (49.3±30.3 versus 46.3±16.5 mm; P=.574). Distribution of stones in the pelvocalyceal system was more diverse in the PCNL group (P=.002).
BMI, body mass index; eGFR, enhanced glomerular filtration rate; ESWL, extracorporeal shock wave lithotripsy; F, female; LP, laparoscopic pyelolithotomy; M, male; PCNL, percutaneous nephrolithotomy; URS, ureterorenoscopy.
Mean operation times were significantly longer in the LP group than in the PCNL group (163.7±78.2 versus 110.0±54.6 minutes; P<.001). However, the LP group had a significantly smaller mean change in hemoglobin level (–0.66±1.28 versus −1.92±1.77 g/dL; P<.001) and less postoperative analgesics usage (22/45 [48.9%] versus 29/39 [74.4%]; P=.022) compared with the PCNL group. Moreover, the LP group had more favorable results in terms of mean estimated blood loss (47.7±108.9 versus 121.3±265.6 mL; P=.112), mean change in creatinine (–0.04±0.17 versus 0.02±0.23 mg/dL; P=.172), and estimated glomerular filtration rate (2.49±13.47 versus −0.19±15.26 mL/minute/1.73 m2; P=.395) levels, but the differences were not significant. Difference in mean duration of hospital stay was also not significant (4.64±3.34 versus 4.76±1.60 days; P=.842). Stone-free rates in a single session were significantly greater in the LP group (91.1% versus 64.1%; P=.003).
Table 2 presents postoperative complications. There were more overall complications in the PCNL group than in the LP group. Twenty-two patients (48.9%) in the LP group and 29 (74.4%) in the PCNL group took analgesics postoperatively because of pain. Five (11.1%) in the LP group and 8 (20.5%) in the PCNL group had fever and required antipyretics. Most complications were Grade I. One patient in the LP group had hypertension and thus required an antihypertensive drug, and 4 in the PCNL group received blood transfusions (Grade II). One patient in the LP group required percutaneous drainage because of perirenal urine collection. Grade IIIa complications occurred in 4 patients in the PCNL group: 1 patient had perirenal hematoma, 1 had urine leakage through the nephrostomy site, and 2 had complications associated with the double J stent. Neither group had complications of Grade IIIb or higher.
LP, laparoscopic pyelolithotomy; PCNL, percutaneous nephrolithotomy; PSVT, paroxysmal supraventricular tachycardia.
Discussion
Since the laparoscopic approach for urinary stones was first described more than 20 years ago, 8 many subsequent series of LP have been reported. Because LP requires more skill, is more invasive and less cosmetic, and requires longer operation time and longer convalescence as compared with PCNL, 4 LP has not been welcomed much by urologists. As a result, LP is currently considered an alternative modality for PCNL, which is the treatment of choice for most renal stones.
Although only small numbers of cases are available, there have been some studies that reported encouraging results from LP for single renal stones in the early 2000s. These studies concluded that PCNL and LP provide comparable results in the management of pelvic stones.2,3 However, these studies only focused on managing solitary pelvic stones. Studies comparing PCNL and LP for multiple complex renal stones have not yet to be done in much detail. A recent study reported a 100% stone-free rate from LP for multiple renal stones in different poles in 4 patients. 8 Lee et al. 10 also stated that LP is an feasible modality for managing multiple renal stones. To our knowledge, our study is the largest-scale study to demonstrate the effectiveness and safety of LP for PCNL in the management of multiple complex renal stones.
Managing complex renal stones, which were defined as multiple stones, staghorn stones, and calyceal diverticular stones, remains challenging. 8 Stone-free rates for PCNL through single access tracts (defined by residual stones <4 mm in diameter on X-ray of the KUB region, CT, or ultrasonography) for branched stones and multiple stones were 55.5% and 94.1%, respectively. 11 Stone-free rates (defined by two or fewer stones and ≤2 mm in diameter) for PCNL were 79% for access through the lower calyceal tract and 87% through the upper pole for complex inferior calyceal stones. 12 Singla et al. 13 reported a 70.7% stone-free rate in multiple-tract PCNL for staghorn stones. In contrast, stone-free rates of 88%–100% were indicated for LP for single renal stones,2,3,14 with good results for multiple or staghorn stones in a small number of cases. 8 In our study, results of the LP group were superior to those of the PCNL group in the management of a vast number of multiple complex renal stones in various parts of the pelvocalyceal system (91.1% versus 64.1%, respectively). The fact that the stone-free rates of the PCNL group in this study were lower than those previously reported in other studies is reasonable because this study was originally designed to compare the results of a single session treatment for complex renal stones. In addition, we did not include results from multiple-tract PCNL or additional treatments such as sandwich treatment.
Although PCNL has had good surgical results, complete removal for multiple stones in various parts of the pelvocalyceal system may be impossible through a single access tract because of the specific anatomical structure of the collecting system. 12 Multiple access tracts are necessary to assess the entire collecting system with PCNL. Previous reports demonstrated that PCNL required multiple access tracts in 20%–58% of cases,14–16 which increased the risk of renal parenchymal injury, bleeding, and postoperative discomfort.17,18 In addition, although the supracostal approach is considered the most effective, this mode of access has an increased risk for intrathoracic complications.15,19,20 Other approaches, including upper or interpolar access, may be more challenging because of the angular limitation of the calyces and ribs. 7 In our study, LP enabled us to easily explore nearly the entire collecting system using a flexible nephroscope through one of the ports.
In the present study, all of the patients who underwent LP had an extrarenal or a dilated pelvis (Fig. 1). A large pyelotomy is necessary to retrieve stones ≥1 cm in diameter. Although the intrarenal pelvis could be fully dissected, it is very difficult to repair the large pyelotomy site technically with a narrow working space after a removal of renal stones. Therefore, we believe that LP cannot be a feasible modality for renal stones with intrarenal pelvis, in particular. We also preferred LP mainly to PCNL to avoid a renal parenchymal injury and chose a minimal invasive laparoscopic approach instead of an open surgery.
Some authors have claimed that the major limitations of LP are that it is laparoscopically difficult to dissect the inflamed renal pelvis, retrieve calyceal stones, and apply intracorporeal sutures in a pelvis. 4 It is indeed technically difficult to dissect pelvises with inflammation or adhesions due to stones. In cases of extrarenal or sufficiently dilated pelvises, however, the pelvises not only provide anatomical landmarks, but also facilitate dissection. Here, we used a flexible nephroscope to overcome difficulties in retrieving calyceal stones, as flexible nephroscopes enable easier approach and assessment of the entire pelvocalyceal system. Of course, the fact that another monitoring system is needed when using flexible nephroscopes is somewhat cumbersome, but the advantages of flexible nephroscopy are well worth the small inconvenience. With regard to technical difficulties associated with intracorporeal suturing, only sufficient experience with the laparoscopic procedure can help overcome them. Edematous pelvises with inflammation can be sewn without injury using the sliding knot technique and mucosa-to-mucosa sutures, which hasten rapid healing of the pyelotomy site and decrease the occurrence of extrarenal urine leakage.
A previous review article published overall complication rates during or after PCNL of up to 83%, including fever (21.0%–32.1%), transfusion (11.2%–17.5%), extravasation (7.2%), sepsis (0.3%–4.7%), colonic (0.2%–0.8%) or pleural (0.0%–3.1%) injury, and perioperative mortality (0.3%–0.78%). 21 In our study, most of the complications were Grade I in both groups. Two patients in the LP group and 8 patients in the PCNL group experienced Grade II or IIIa complications. There were no complications of Grade IIIb or higher. However, overall complication rates in the PCNL group were higher than in the LP group. Accordingly, LP could be considered a more feasible modality than PCNL with respect to safety.
Limitations of our study include the fact that data were nonrandomized and collected retrospectively. The number of cases analyzed was relatively small. However, our study is significant in that the surgical procedures were standardized. In addition, considering the general paucity of complex renal stone patients, our study included the largest number of cases compared with other comparative studies on surgical outcomes between LP and PCNL for multiple complex renal stones in different calyces.
The findings of our study demonstrate that LP seems to be more effective and safer than PCNL. Therefore, we suggest that LP could be considered a useful modality for patients with multiple complex renal stones in various parts of the pelvocalyceal system, which are hard to retrieve completely using PCNL in a single session. Further large-scale, prospective, and randomized controlled studies will be required to deduce long-term outcomes.
Footnotes
Disclosure Statement
No competing financial interests exist.