
Abstract
Abstract
Objectives:
The adoption of laparoscopy for the Whipple procedure remains limited in part by its technical difficulty. We sought to develop a superior, simpler pancreaticojejunostomy technique.
Materials and Methods:
We applied a running barbed suture (V-Loc™; Covidien, Mansfield, MA) to perform the pancreaticojejunostomy over a stent placed in the pancreatic duct and a small enterotomy in the jejunum. This technique was attempted in the last 19 of 37 patients presenting to two surgeons (M.A.M. and B.H.E.) for a laparoscopic Whipple procedure. Data were collected on operative time, pancreatic leak events, and related complications.
Results:
We successfully applied the modified technique in all 19 patients. Pancreatic leak occurred in 5% of patients with the modified technique (Grade A=0; Grade B=1; Grade C=0) and 11% with the standard technique (Grade A=1; Grade B=1; Grade C=0). All leaks were managed with external drainage. There were no leak-related complications. Mean operative time was shorter for the modified technique (mean, 367 minutes; range, 260–576 minutes) than the standard technique (mean, 440 minutes; range, 300–665 minutes).
Conclusions:
The use of a running barbed suture for laparoscopic pancreaticojejunostomy is a safe and efficient technique. Our operative times were decreased with this technique, and our outcomes were similar to other laparoscopic Whipple series.
Introduction
T
Materials and Methods
Patient selection
A laparoscopic Whipple procedure was performed in all patients presenting with no evidence of major vessel involvement to two surgeons (M.A.M. and B.H.E.) over a 2-year period (May 2010–May 2012). Of these patients, the first 18 were operated on using our standard laparoscopic surgical technique, and the last 19 were operated on using the barbed suturing technique.
Our standard laparoscopic surgical technique
The patient is positioned in the supine fashion with his or her arms extended. Initial abdominal access is obtained in the caudal aspect of the umbilicus using a Hassan technique under direct visualization. Once the abdomen is distended, a left subcostal 12-mm VersaStep™ (Covidien, Mansfield, MA) port is placed, followed by a 5-mm VersaStep port left of the umbilicus so that there are two working ports on the patient's left side. The right-sided abdominal ports are then placed by inserting a 5-mm port at the right subcostal region along the midclavicular line. Caudal to this port, two additional 12-mm ports are inserted so that there are two working ports on each side of the patient as well as a port for the retracting instrument to retract the duodenum and pylorus (Fig. 1). A 10-mm, 45° laparoscope is used for intraabdominal visualization.
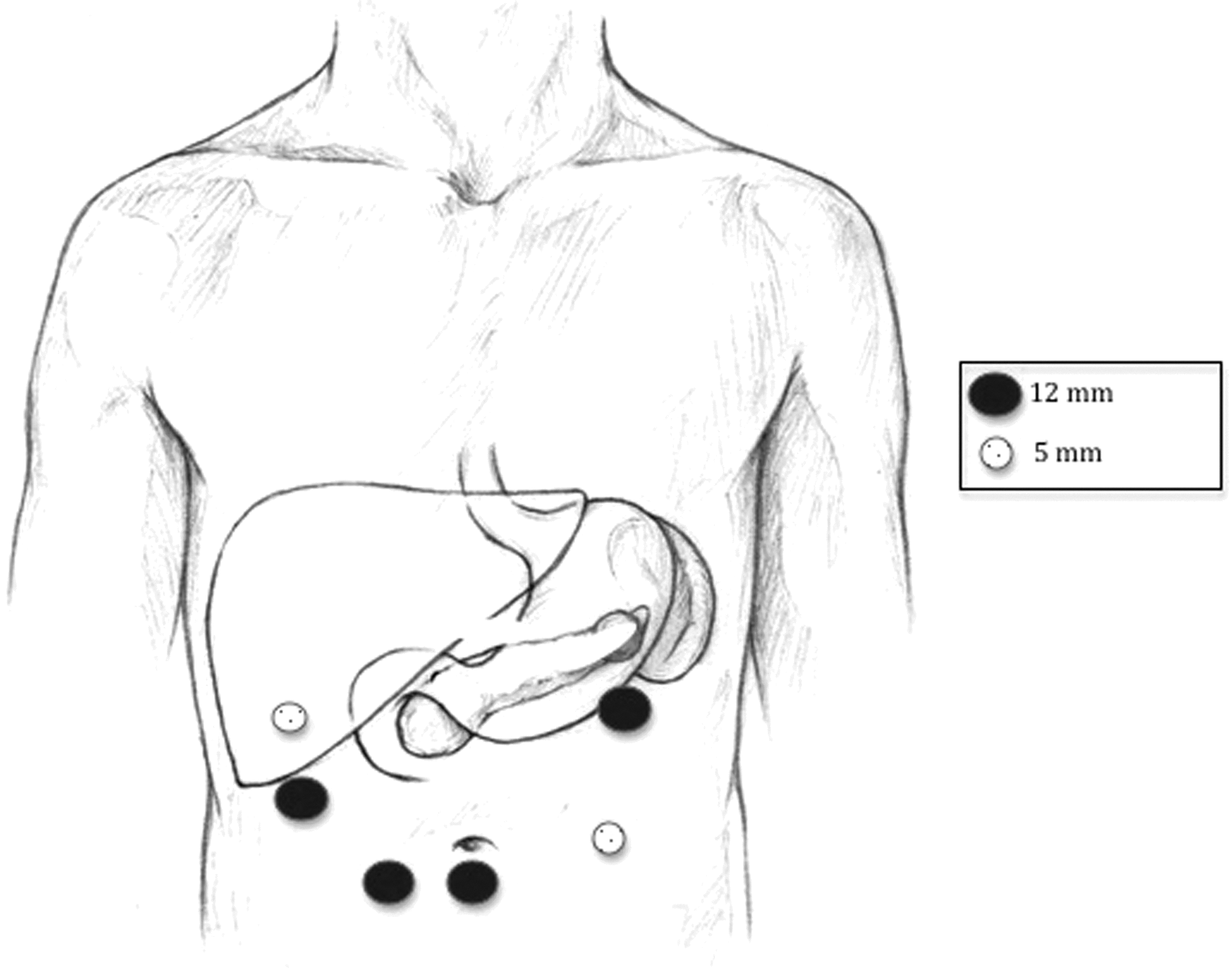
Trocar placement for the laparoscopic Whipple procedure. Following placement of a Hassan port below the umbilicus, a left subcostal 12-mm VersaStep (Covidien) port was placed, followed by a 5-mm VersaStep port in the right subcostal region along the midclavicular line. Inferior and medial to these ports, another three ports, including two 12-mm ports on the patient's right and a 5-mm port on the left, were inserted. The middle 12-mm port on the right side is for placement of the fan retractor for retraction of the duodenum and pylorus.
The abdomen is explored for evidence of metastases. When no metastatic lesions are identified, the procedure is continued. The lesser sac is approached through the gastrocolic ligament, which is widely opened. The hepatic flexure of the right colon is mobilized. The gastroduodenal artery is then skeletonized. Two 2-0 silk ties are placed proximal and distal on the gastroduodenal artery as well as one 10-mm clip on the proximal side, and the artery is divided with a sealing device. A cholecystectomy is then performed in the standard fashion.
The portal vein is then dissected from above the pancreas, and the superior mesenteric vein is dissected from below the pancreas. A tunnel behind the pancreatic neck is then easily achieved. The stomach is then divided just proximal to the pylorus with an Endo GIA (Covidien) stapling device with green loads (4.8 mm). The common bile duct is then identified and divided sharply.
The transverse mesocolon is then raised cephalad to identify the ligament of Treitz. At approximately 10–15 cm distal to the ligament of Treitz, the small bowel is divided using an Endo GIA stapling device with a white load (2.5 mm). The neck of the pancreas is transected using hook cautery. The small bowel mesentery is also divided. The ligament of Treitz is then mobilized.
The superior mesenteric artery is then identified, and the branches of the artery and vein going into the Whipple specimen are divided using clips and a sealing device. The Whipple specimen is then brought out using a 15-mm bag through the umbilicus.
The reconstruction is then initiated starting with the pancreaticojejunostomy. The small bowel is passed through the ligament of Treitz to perform an end-to-side pancreaticojejunostomy. The jejunum is placed next to the cut end of the pancreas in a tension-free fashion. For the standard (comparison) technique, the end-to-side pancreaticojejunostomy is performed in a standard hand-sewn fashion with invagination of the pancreatic duct into a 0.5–1.5 cm enterotomy in the side of the proximal jejunum. A back layer of running 3-0 silk running stitches is placed. A running 3-0 polyglactin 910 (Vicryl®; Ethicon, Somerville, NJ) suture is used for the duct to mucosa anastomosis. An anterior layer of 3-0 silk running stitches is then placed. This is consistent with techniques described elsewhere in the literature for laparoscopic pancreaticojejunostomy.8,9
Pancreaticojejunostomy using a barbing suture over a stent technique
The pancreaticojejunostomy is created by sewing the back layer using a running 4-0 barbing suture (V-Loc™; Covidien) in a running fashion (Fig. 2). A small (2–3-mm) enterotomy is made in the jejunum so that the enterotomy approximates the pancreatic duct. A pediatric feeding tube is placed from the pancreatic duct into the jejunum with an equal portion of the stent placed in each. The size of the stent is determined by the pancreatic duct size (we most commonly used a 5-French). A single-layered running anastamosis is then performed using a barbed suture on the anterior side (Fig. 3). The two ends are then tied down, completing the pancreaticojejunostomy.
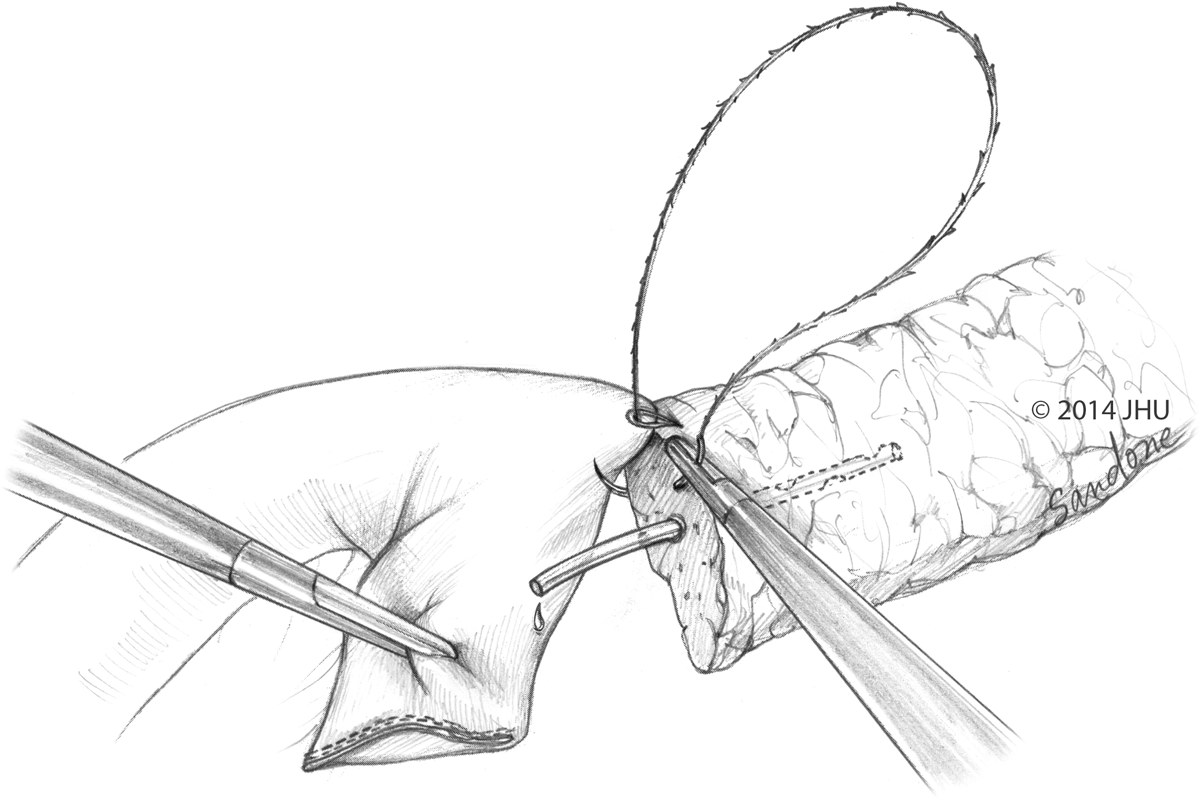
Sewing of the back layer of the pancreaticojejunostomy using a running 4-0 barbing suture. The pediatric feeding tube is in the pancreatic duct.
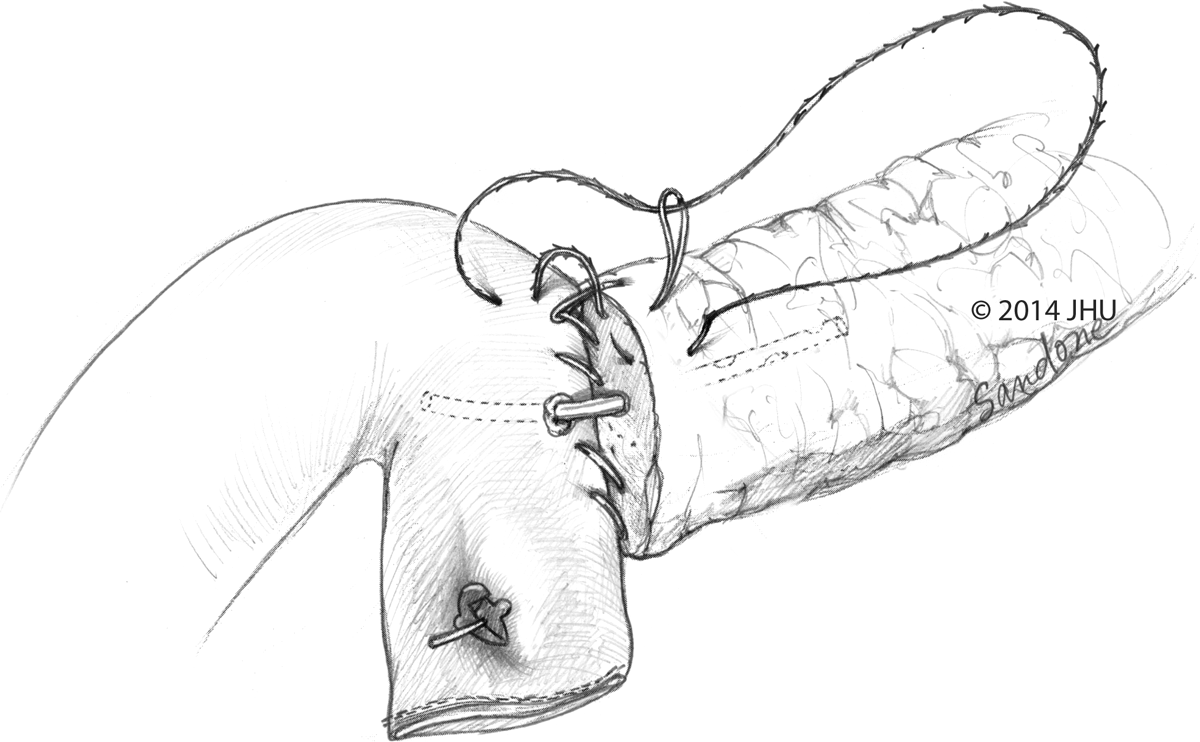
Jejunal enterotomy with placement of the pediatric feeding tube into the jejunum and performance of the anterior layer of the pancreaticojejunal anastamosis using a running 4-0 barbing suture.
The hepaticojejunostomy is then performed with placement of a single layer using 4-0 Vicryl sutures (Fig. 4). The gastrojejunostomy is then performed in an antecolic retrogastric side-to-side fashion using the stapled technique (3.5-mm staples, 60-mm Endo GIA stapler). The resulting defect on the right side of the anastomosis is then closed with interrupted sutures. Jackson–Pratt drains are then placed with at least one drain adjacent to the pancreaticojejunostomy. All 12-mm port sites are closed at the level of the fascia with a Carter–Thomason suture passer (CooperSurgical, Trumbull, CT), and the last 12-mm port site at the umbilicus is closed with a series of interrupted #1 polyglyconate (Maxon™; Covidien) and 0 Vicryl interrupted sutures. The skin is closed with 4-0 Biosyn™ (Covidien).
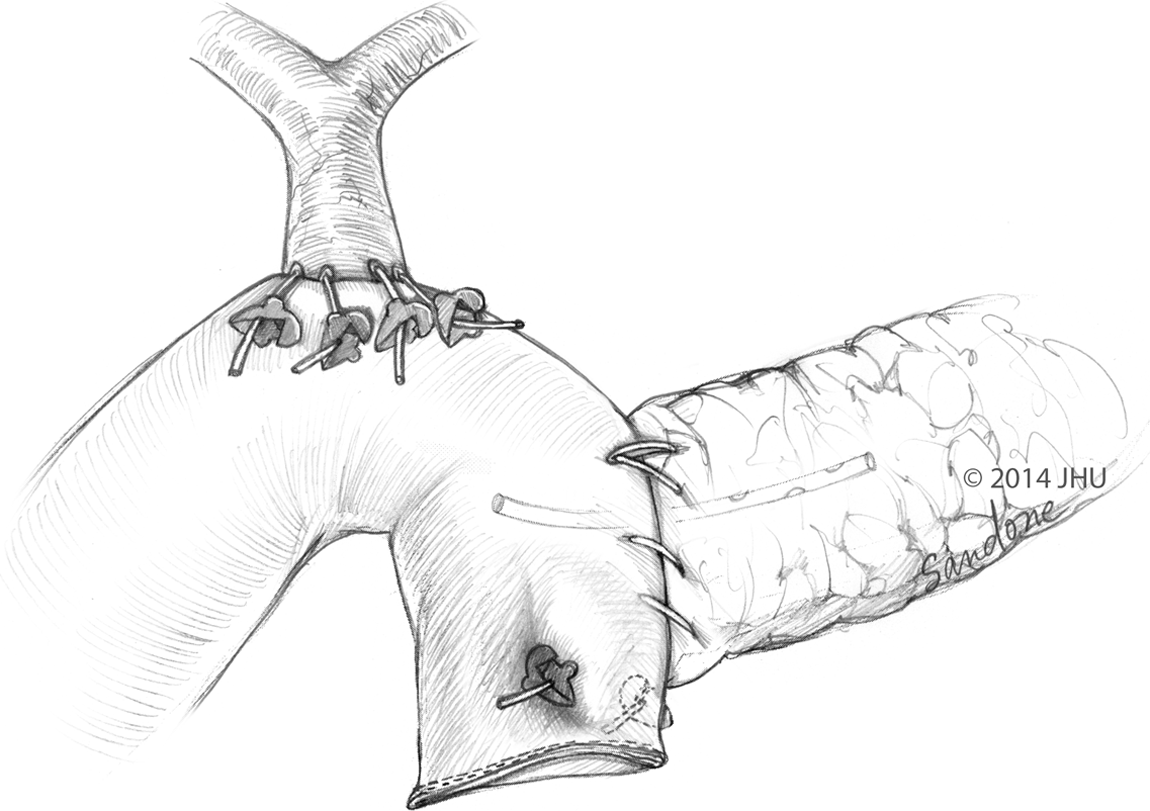
Completed pancreaticojejunostomy and hepaticojejunostomy using the modified technique.
For safety, for all of our advanced laparoscopic pancreas procedures, a #10 blade scalpel and Mayo scissors are always kept on the Mayo stand in case a rapid conversion to open is necessary. We also make sure that no pop-off stitches are used as these can easily pop off inadvertently while in the insufflated field.
Data collection and analysis
We retrospectively collected data on pancreatic leak and operative time for patients who underwent the standard and modified techniques. The data were compared using t-test analysis, and significance was set at a P value of <.05.
Results
In total, 37 laparoscopic Whipple procedures were performed. Eighteen of these were performed using the standard pancreaticojejunostomy technique, and 19 were performed using the barbing technique. Patient characteristics are given in Table 1.
GIST, gastrointestinal stromal tumor; IPMN, intraductal papillary mucinous neoplasm; PJ, pancreaticojejunostomy.
Perioperative complications occurred in 22% of patients (8/23). Pancreatic leak occurred in 5% (1/19) of patients who underwent the modified technique (Grade A fistula=0; Grade B fistula=1; Grade C fistula=0) and 11% (2/18) of patients who underwent the standard technique (Grade A fistula=1; Grade B fistula=1; Grade C fistula=0). All pancreatic leaks were managed with external drainage: one with placement of a percutaneous drain and two with leaving the operative Jackson–Pratt drains in place. There were no further pancreas leak-related complications. Bile leak occurred in 11% (2/19) of patients who underwent the modified technique (Grade A=1, Grade B=1) and 11% (2/18) of patients who underwent the standard technique (Grade A fistula=1; Grade B fistula=1; Grade C fistula=0). These were also managed with external drainage alone. Delayed gastric emptying occurred in 5% (1/19) patients who underwent the modified technique, which was managed with nasogastric tube decompression alone. It occurred in 6% (1/18) patients who underwent the standard technique, which was managed with esophagogastroduodenoscopy and gastrojejunal dilatation. The 90-day mortality was 3% (1/37). A patient who underwent the modified technique developed a closed-loop bowel obstruction managed by emergency exploration, which was complicated by subsequent hepatic artery bleeding, atrial fibrillation, and acute respiratory distress syndrome. Care was withdrawn, and the patient died 68 days after the initial operation.
Mean operative time was 367 minutes (range, 260–576 minutes) for the modified technique and 440 minutes (range, 300–665 minutes) for the standard technique. The operative times were shorter using the modified technique.
Discussion
The Whipple operation is one of the most morbid elective operations in the field of general surgery, with a complication rate of up to 65%.10–12 In addition to its complication profile, the majority of patients having the operation for cancer do not survive to 3 years. Laparoscopy for distal pancreas resection has been shown in multiple studies to result in decreased rates of surgical-site infection, incisional hernia, and postoperative pain, decreased time to return to normal activity, and improved cosmesis compared with the open technique.2–7 The same benefits of laparoscopy have been demonstrated in patients undergoing the Whipple procedure. Kendrick et al. 13 reported that the laparoscopic Whipple procedure was associated with no superficial surgical-site infections and a reduced length of stay compared with the open procedure. Additionally, for those patients who undergo postoperative chemotherapy, including many pancreas cancer patients, the improved recovery can facilitate adjuvant therapy. Overall, the laparoscopic Whipple procedure can offer patients several advantages over an open Whipple operation.
However, adoption of the laparoscopic Whipple procedure has been limited by the technical challenges of the procedure, with one of the most challenging aspects being the pancreaticojejunostomy. We report a technique that is safe, quick, and feasible. The described technique has some unique advantages. The barbing suture creates close tissue approximation. Simply pulling the suture through the tissue creates an appropriate amount of coiling tension to avoid excessive laxity or tension on the suture line. This allows the visualization of the tension required and maintains the desired tension without cracking or traumatizing the pancreas. Second, the closure over the pancreatic duct stent allows for precise approximation, allowing a controlled fistula tract to be created between the pancreas and bowel, without traumatizing the pancreas duct. Third, the technique can be performed rapidly, decreasing the operative time.
Our series had a pancreatic fistula profile similar to that of open Whipple series.10–12 Our findings are consistent with those of other investigators who reported that the pancreatic leak rate is the same for both laparoscopic and open Whipple procedures.14–20 In our series, there was no difference in pancreatic fistula rate between the standard and modified techniques. Our operative times were shorter using the modified technique compared with the standard technique, and they were similar to those previously reported in the literature for laparoscopic Whipple procedures.14–20
This study has some important limitations. First, our sample size does not allow us to interpolate a true rate of events, only an early observation. Second, the learning curve we encountered in the early experience may explain the difference in operative times. Finally, we did not consider all surgical outcomes in this study, only the feasibility and safety of the novel technique.
In this series, we found that by changing our technique, we were able to decrease operative times with no change in pancreatic fistula rates. With the optimal pancreas and laparoscopic surgery skills, laparoscopic pancreaticojejunostomy can be performed safely.
Footnotes
Disclosure Statement
No competing financial interests exist.