
Abstract
Abstract
Objective:
To evaluate the acceptance of the single-knot running vesicourethral anastomosis in a worldwide survey, 10 years after its introduction.
Materials and Methods:
A survey composed of 13 multiple-choice questions was launched on the Internet. Urologists involved in minimally invasive surgery were invited to participate. Questions explored professional characteristics of the respondents, experience with the single-knot running vesicourethral anastomosis, complications (including technical, early, and late complications), and a general opinion on the technique.
Results:
The 391 urologists who participated in the survey worked in academic, private, and community settings. Live surgeries appear to have been the most important tool to teach the technique. The global experience gained with this technique is vast: in the last 10 years we calculated over 120,000 anastomoses were performed by our cohort of respondents. Overall, technical, early (mainly uncomplicated early leakage), and late complications (mainly anastomotic stricture) were observed in <2% of cases by the majority of surgeons in the survey. Most urologists in the survey seem to accept the technique as a commonly used procedure in urologic surgery.
Conclusions:
Today, in 2014, the single-knot running anastomosis technique appears to have been well accepted by the urologic community. However, research should continue always in order to explore and invent better surgical solutions for our patients.
Introduction
L
We therefore decided to evaluate our method and its application and feasibility in urologic surgery 10 years later. Hence, an Internet survey composed of 13 multiple-choice questions was launched to determine the current status of the single-knot running VUA, and urologists worldwide involved in minimally invasive surgery were invited to respond. The aim of the survey was to explore characteristics of the anastomosis, estimate the global experience achieved with this technique, and evaluate its complications. Given the obvious limitations of a survey and its subjective replies, the main purpose of this article must be considered the evaluation of the overall acceptance of this technique by the urologic community.
Materials and Methods
Between February 2013 and June 2013, an Internet survey was launched through the EAU Web platform and the da Vinci Web community. An e-mail was sent inviting urologists involved in laparoscopic and robotic-assisted urologic surgery to participate. The questionnaire was anonymous and composed of four main sections. These included professional characteristics of respondents, experience with the single-knot running VUA, complications (technical, early, and late), and finally one last question asking a general, thorough opinion on the technique. Questions are shown in the Appendix. For Questions 1–3 and 13, participants were allowed to give more than one answer. A database with all the answers was built, including cases in which only a partial answer to the survey was given. Descriptive statistics were used to summarize relevant variables of the survey.
To evaluate the global number of procedures performed yearly by the entire group of respondents, we considered the median number of annual procedures in the various ranges provided (1–30; 31–70; 71–120; 121–200; 201–250) and multiplied it by the number of answers for each range. These values were then added to calculate the total number of yearly procedures performed by the entire cohort of respondents. The same procedure was performed to calculate the total number of years of experience with the single-knot VUA. Finally, by multiplying (total procedures/year×the average years of performing the single-knot running VUA [i.e., total years of experience
Results
In total, 391 urologists participated in the study, and 384 (98%) completed all the questions in the survey. Full-length questions and results are shown in the Appendix. Overall, respondent were urologists working in an academic setting (37%) or in private (34%) or community (29%) scenarios. It appears that the technique has been learned mainly through live surgeries (49%), and, as expected, RALP is the most frequent procedure after which the single-knot running VUA is performed.
We calculated that, globally, the entire group of respondents performs 28,325 annual procedures for which the single-knot running technique is used to achieve the VUA (Table 1). As explained in Materials and Methods, by multiplying the total annual procedures by the average years of experience with the single-knot running VUA (total years of experience/number of respondents, 4.28 years), we estimated that in the last 10 years the entire group of respondents performed approximately 121,231 procedures applying the single-knot running technique (Table 1). This rough calculation represents the global experience that the entire cohort of respondents had while answering the survey.
Regarding complications, this survey found that technical (Fig. 1), early (Fig. 2), and late (Fig. 3) complications occur generally in <2% of cases in the experience of the majority of the urologists in this survey. Technical problems are encountered in fact by 54% of the respondents in less than 2% of their cases (Fig. 1). Regarding early complications, the most frequent is a noncomplicated early leakage (Fig. 2), whereas an anastomotic stricture remains the late complication most frequently reported (Fig. 3); nonetheless, both are observed in <2% in our survey. The majority of the respondents remove the urethral catheter between 5 and 10 days after surgery. Keep in mind that the answers of a survey naturally suffer from major biases, and as such these rates should be considered approximate; the intent of this section of this study was indeed to give an overall picture and not specific details of the technique's complication rate.
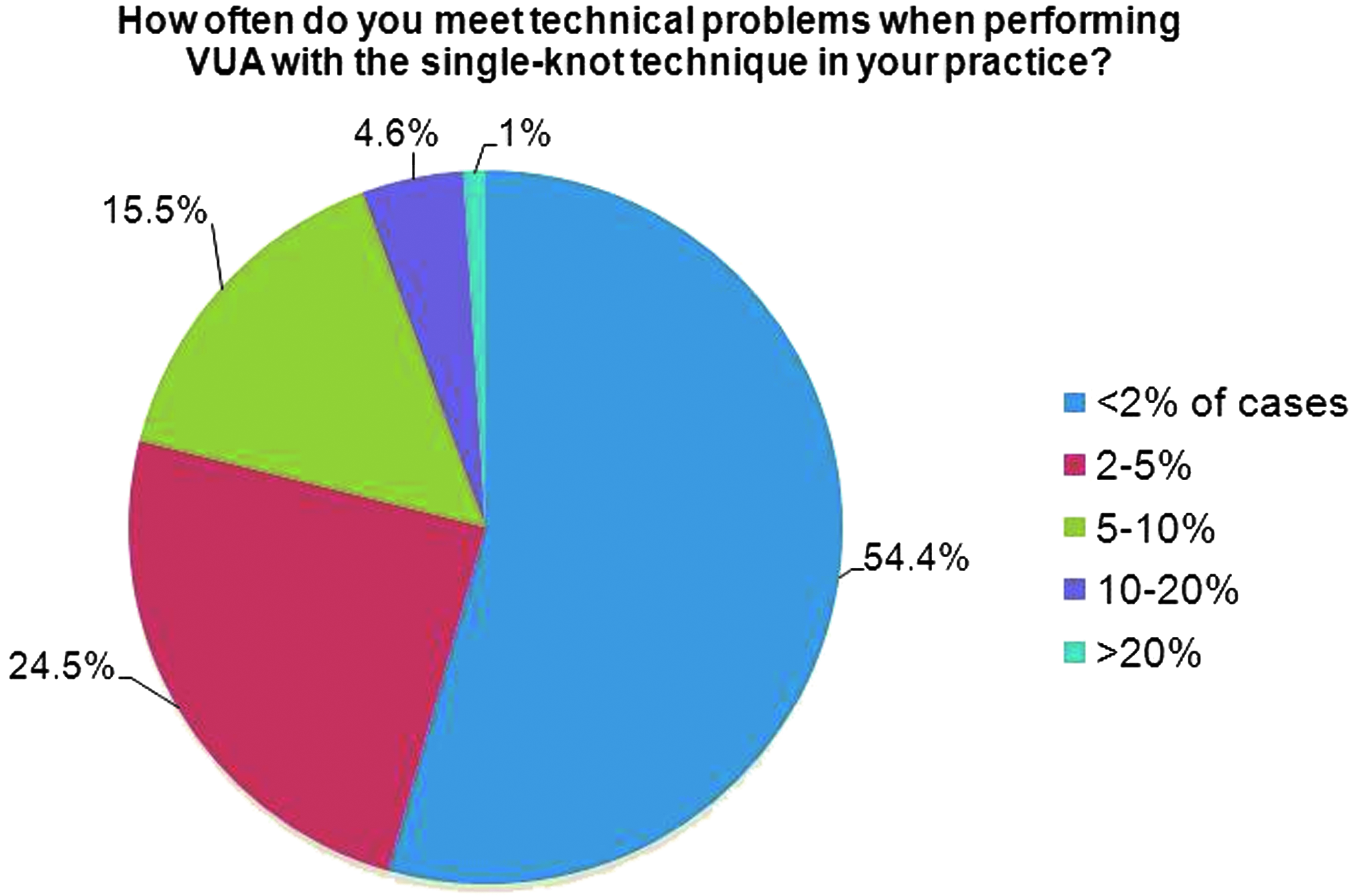
Technical complications after single-knot running vesicourethral anastomosis (VUA).
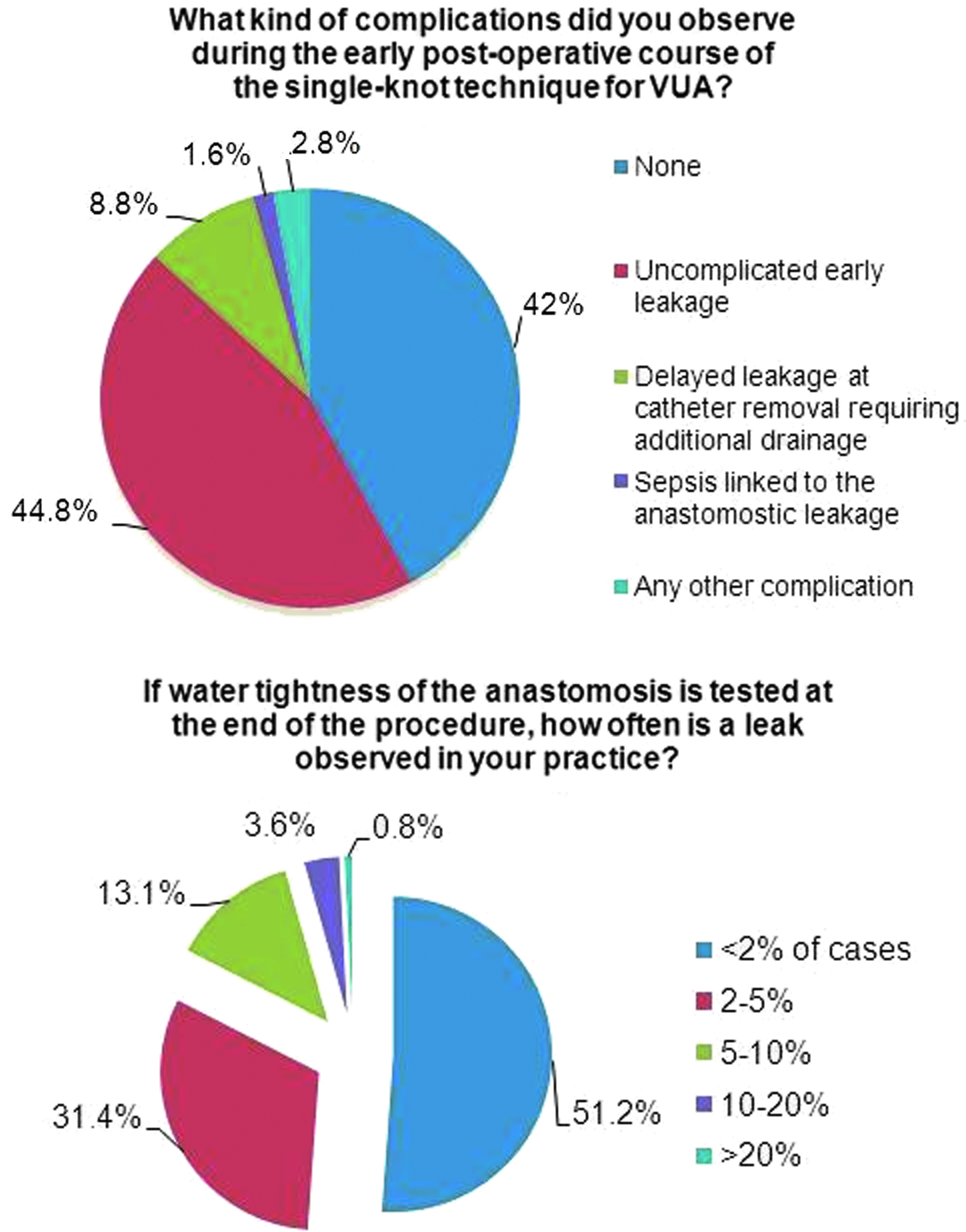
Early complications after single-knot running vesicourethral anastomosis (VUA).
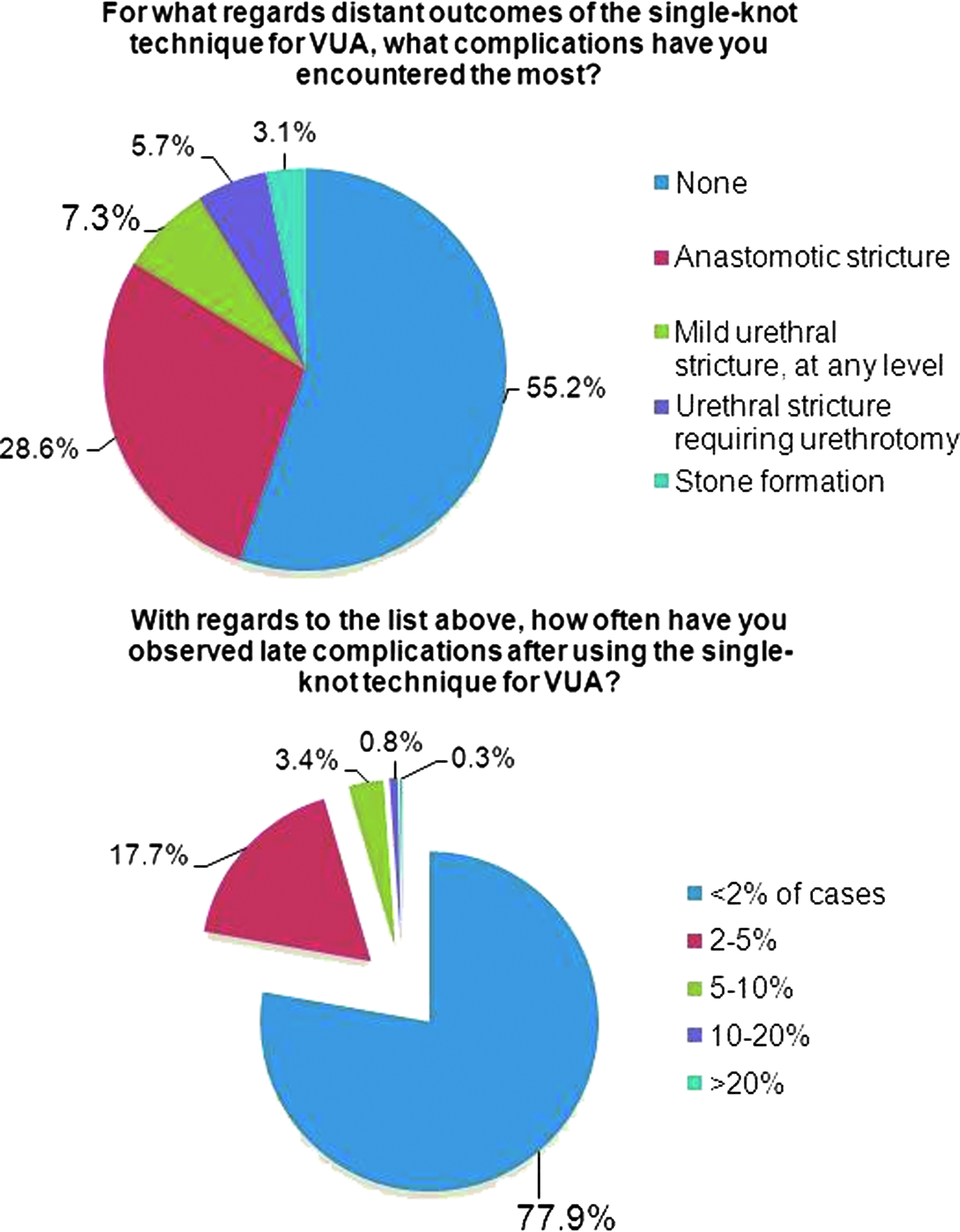
Late complications after single-knot running vesicourethral anastomosis (VUA).
According to the answers to Question 13, it appears that the single-knot running VUA has been accepted and is well considered by most surgeons participating in this study: 45% found this is a technique that “belongs to the commonly used procedures in urology.”
Discussion
The quest for the application of laparoscopy to radical prostatectomy started in 1992, when Schuessler et al. 8 first (published in 1997) pioneered such an intervention; the procedure, however, was associated with long operative times and did not show major significant clinical advantages compared with the open approach. Several years after, in 2000, Guillonneau and Vallancien 9 reported their stepwise technique with operative times between 4 and 5 hours, in addition to reasonable oncologic and functional results. As such, laparoscopic prostatectomy began to be performed in centers of excellence worldwide; nonetheless, the procedure was and is complex, and, especially in the years prior to the vast distribution of the da Vinci® robotic system (Intuitive Surgical, Sunnyvale, CA), the learning curve was steep, requiring approximately 50 procedures. 10 Specifically, the VUA has always been a crucial, complicated, and time-consuming step,8,10 given the necessity of placing difficult stitches, mastering intracorporeal laparoscopic suturing, and finally the increasing fatigue to which the surgeon is exposed at the end of the procedure.
Therefore, in 2000, in our department, we introduced a single-knot running VUA, also known as the Van Velthoven anastomosis, and published its initial series in 2003. 2 This technique requires only one intracorporeal knot, it allows a water-tight approximation of the bladder neck to the urethra, and it is easily teachable. Now, after 10 years, we are critically evaluating its acceptance by the urologic surgical community. We have been satisfied with the feedback received, as 391 urologists worldwide, working in various clinical settings, took the survey. It appears that the single-knot VUA technique has been taught mainly through live surgeries (Question 1), and it is used principally in RALP (Question 3). Moreover, this technique appears to be associated with a low incidence of technical problems (Question 6) and a low rate of early (Questions 7 and 8) and late (Questions 11 and 12) complications. Clearly, one should bear in mind that a survey naturally suffers from important biases, and as such these rates should be considered approximate. This study finally suggests that, after 10 years, the single-knot VUA is used and accepted by many urologists involved in laparoscopic surgery (Question 13).
The results of this survey indicate that RALP is the surgical procedure in which the single-knot VUA is mostly applied. This reflects the current global trends of worldwide urologic minimally invasive surgical practice, as a consequence of the vast distribution of the da Vinci robotic system seen in recent years 1 and the reduction in number of prostate cancer cases treated by non–robotic-assisted laparoscopy. However, the single-knot technique is versatile and can be performed after different techniques of minimally invasive prostate surgery: Galfano et al. 11 recently presented their trans-Douglas approach to RALP, using an “inverted” (12 o'clock to 6 o'clock) single-knot running anastomosis. Coelho et al. 12 reported their technique of robotic simple prostatectomy with a modified Van Velthoven anastomosis. Moreover, the single-knot technique can be used whenever a urinary reservoir requires branching to the urethra, as in robotic-assisted radical cystectomy with neobladder reconstruction.
The global experience with the single-knot running VUA possessed by this group of respondents is solid: we roughly calculated that, in the last 10 years, in total, 121,231 procedures were performed by our respondents. This number, however, must be considered approximate. It appears that most surgeons have started using the single-knot technique between 3 to 7 years ago, with an average of 4.28 years (4 years 4 months) of experience, yet operators are continuing to learn and apply such technique in the last 3 years. Indeed, the Van Velthoven anastomosis is easy to teach, 2 and different in vivo and ex vivo models have been constructed to aid in this process.13,14 According to this survey, live surgeries have been the most useful method of teaching the technique; in the era of bioethics, where surgical societies are restraining the broadcast of live procedures, 15 this is a incentive in stimulating and supporting live surgeries.
In our survey we found a low rate of reported technical complications (54% of the respondents encountered technical complications in <2% of cases [Fig. 1]). To face some minor troubles that can, however, arise during the reconstructive phase of RALP, investigators have evaluated unidirectional and bidirectional barbed sutures to ameliorate and ease the surgeon's methodology while performing VUA.16–18 Tewari et al. 17 reported that using a V-Loc™ (Covidien plc, Dublin, Ireland), compared with a monofilament suture, reduces anastomotic time: however, given the difference was approximately 5 minutes; the clinical significance of such time saving is questionable. Moreover, Moran et al. 18 tested a bidirectional barbed suture (Quill™; Surgical Specialities Corp., Vancouver, BC, Canada) and found minimal differences in time and surgeon security score. Some surgeons may prefer barbed sutures, as they are self-cinching, do not require intracorporeal knot-tying, and can save time. Nonetheless, the method used most frequently remains the one described 10 years ago 2 : new materials, same technique.
Forty-two percent of surgeons in the survey did not report any significant complication in the early postoperative period after performing the VUA (Fig. 2). If there is one, the most common early complication is a urine leak. Although the results of a survey are naturally flawed by a possible major recall bias, different investigators using the single-knot running technique (or applying minor modifications) have reported similar results on their surgical series, with rates ranging from 0% to 7.5%,16,19,20 as in our survey. Average catheter retrieval time in our survey was 5–10 days in more than 80% of cases, with additional catheterization being required in <5% of cases. These findings are in line with data published by investigators using the single-knot running technique.19,21
Favorable results are also reported several months after the procedure (Fig. 3). Most of the surgeons interviewed (55%) reported no complications observed in the long-term follow-up. The complication worthy of notice, happening in <2% of cases according to our results, is an anastomotic stricture. Ouzaid et al. 22 evaluated 2115 patients who underwent minimally invasive prostatectomy with VUA performed according to the Van Velthoven technique; after a mean follow-up of 43 months, an anastomotic stricture was found in 1.4% of patients, with previous prostatic resection and external beam radiotherapy being the most significant risk factors. Most surgical series in which the single-knot method was used to perform VUA have reported similar stricture rates, ranging from 0% to 3%.16,19–21 Indeed, also, this item of the survey can be considered biased; however, the results of our survey appear to be well correlated with published data.
Since the beginning of laparoscopic prostatectomy, numerous methods have been proposed for VUA by centers of excellence worldwide. In the beginning, interrupted sutures had been tested by the first pioneers of this intervention.9,23 However, these techniques were complicated, and therefore running suture methods began to be explored. Hoznek et al. 24 in 2000 reported their method of performing a running VUA, which required three intracorporeal knots. Curto et al. 7 popularized the “Bordeaux technique,” a single running suture that starts at the 3 o'clock position and continues in a clockwise direction; this method has been modified by Emiliozzi et al. 6 to reduce the number of intracorporeal knots to only one and facilitate the throw of the posterior stitches. Menon et al. 25 readapted the Van Velthoven technique to robotic-assisted prostatectomy, with minimal modifications, and Meeks et al. 26 proposed the application of continuous tension to the suture to ameliorate mucosal approximation and guarantee a water-proof anastomosis. Recently, Simone et al. 5 proposed a single-knot running VUA technique that incorporates a posterior musculofascial reconstruction; the authors note the achievement of improved continence rates with this method compared with a pure Van Velthoven technique. However, in their control group no posterior musculofascial reconstruction was performed; the Van Velthoven technique does not exclude the configuration of a posterior reconstruction, which may ameliorate continence rates. 27
We must acknowledge limitations of the present study. A recall bias is inevitable when launching a survey; indeed, this is the major limitation of the study. Especially on the questions regarding complications (Questions 7–12), a subjective method such as a survey may determine a reduction of the rates reported. We acknowledge this limitation and believe that our results, especially on complications, are approximate and that as such they should be considered as an overall “picture” of this technique. Nonetheless, analyzing the data reported in peer-reviewed literature, these findings are similar to those reported by centers of excellence worldwide.16,19–22 Finally, the calculation of the total number of procedures performed by our cohort of respondent suffers from multiple biases, and, as specified, it must considered strictly speculative and with the objective of giving only an idea of the experience gained with the single-knot running VUA by the respondents to the survey. Finally, an insight on why some surgeons have either stopped performing or have never started using the single-knot running VUA is lacking in the present survey. Indeed, it would be interesting to explore the weak points of this procedure from the perspective of those who prefer other techniques.
Conclusions
Today, 10 years after its development and publication, the single-knot running technique is an accepted and commonly used procedure to perform VUA during laparoscopic and robotic-assisted urologic surgery. However, the answers to a survey remain subjective, and thus research should continue always in order to explore and invent better surgical solutions for our patients.
Footnotes
Disclosure Statement
No competing financial interests exist.
Appendix: Single-Knot Running Vesicourethral Anastomosis Questionnaire
| a) Textbook, original paper | 15.1% (59) |
| b) Internet-edited material (video, pod-cast) | 13.0% (51) |
| c) Live surgery workshop | 49.1% (192) |
| d) Congress poster or presentation | 9% (35) |
| e) Other | 30.2% (118) |
| a) Solo, private clinic environment | 7.2% (26) |
| b) Solo, community-based environment | 5.1% (20) |
| c) Team, private | 26.6% (104) |
| d) Team, community | 24.3% (95) |
| e) Academic | 36.8% (144) |
| a) At the end of a laparoscopic prostatectomy | 29.4% (113) |
| b) At the end of a robotically assisted prostatectomy | 79.2% (304) |
| c) At the end of a laparoscopic radical cystectomy, branching an extracorporeally made reservoir to the urethra | 6.8% (26) |
| d) Same as above, in a robotic-assisted environment | 11.2% (43) |
| e) At the end of a laparoscopic cystectomy with orthotopic bladder replacement performed intracorporeally (possible robotic) | 7.8% (30) |
| a) Less than 1 year | 7.9% (31) |
| b) 1–3 years | 25.4% (99) |
| c) 3–5 years | 29.5% (115) |
| d) 5–7 years | 26.2% (102) |
| e) 8–10 years | 11% (43) |
| a) Less than 30 | 27.2% (106) |
| b) 30–70 | 33.2% (129) |
| c) 70–120 | 23.4% (91) |
| d) 120–200 | 10% (39) |
| e) >200 | 6.2% (24) |
| a) In less than 2% of cases | 54.4% (211) |
| b) 2%–5% | 24.5% (95) |
| c) 5%–10% | 15.5% (60) |
| d) 10%–20% | 4.6% (18) |
| e) More than 20% | 1% (4) |
| a) In less than 2% of cases | 51.2% (199) |
| b) 2%–5% | 31.4% (122) |
| c) 5%–10% | 13.1% (51) |
| d) 10%–20% | 3.6% (14) |
| e) More than 20% | 0.8% (3) |
| a) None | 42% (162) |
| b) Early leakage, noncomplicated | 44.8% (173) |
| c) Delayed leakage at catheter removal, requiring additional drainage | 8.8% (34) |
| d) Sepsis linked to anastomotic leakage | 1.6% (6) |
| e) Other | 2.8% (11) |
| a) After less than 3 days | 0.3% (1) |
| b) After 3–5 days | 7% (27) |
| c) After 5–7 days | 40.5% (156) |
| d) After 7–10 days | 41.6% (160) |
| e) After more than 10 days | 10.6% (41) |
| a) In less than 2% of cases | 46% (178) |
| b) 2%–5% | 35.1% (136) |
| c) 5%–10% | 15.5% (60) |
| d) 10%–20% | 3.1% (12) |
| e) More than 20% | 0.3% (1) |
| a) Anastomotic stricture | 28.6% (110) |
| b) Mild urethral stricture, at any level | 7.3% (28) |
| c) Stone formation | 3.1% (12) |
| d) Urethral stricture requiring internal urethrotomy | 5.7% (22) |
| e) None of the above | 55.2% (212) |
| a) In less than 2% of cases | 77.9% (299) |
| b) 2%–5% | 17.7% (68) |
| c) 5%–10% | 3.4% (13) |
| d) 10%–20% | 0.8% (3) |
| e) More than 20% | 0.3% (1) |
| a) A good technique for beginners, which becomes optional afterwards (learning curve) | 15.9% (61) |
| b) A technique adopted on the long term in my own practice, a personal preference without any impact on my colleagues | 15.9% (61) |
| c) A technique which has transformed my daily practice and belongs to the commonly based procedures in urology | 45.3% (174) |
| d) A technique which has enabled urologists to master the minimally invasive approach to laparoscopic prostatectomy | 37.8% (145) |
| e) None of the above | 4.2% (16) |