
Abstract
Abstract
Background:
Laparoscopic distal pancreatectomy (LDP) is the most acceptable procedure in laparoscopic pancreatic surgery. Nevertheless, knowledge regarding patients at a high anesthetic risk during lengthy and technically demanding LDP is controversial. This study aims to assess the feasibility and safety of LDP in patients with high anesthetic risk.
Patients and Methods:
We conducted a prospective collection retrospective review of patients underwent LDP and open distal pancreatectomy (ODP) from January 2011 until December 2013. By the American Society of Anesthesiologists score, patients were divided into low- and high-risk patients. We compared the clinical, perioperative, and postoperative results in these patients.
Results:
The cohort included 77 patients: 20 underwent LDP, and 57 underwent ODP. There were 30 patients in the low-risk group and 47 patients in the high-risk group. In high-risk patients, LDP, compared with ODP, presented a shorter operating time (mean, 220.8±101.1 minutes versus 299.4±124.3 minutes; P=.038), less blood loss (409.3±569.9 mL versus 1083.1±1583.0 mL; P=.039), higher rate of spleen preservation (73.3% versus 43.8%, P=.037), and shorter length of postoperative hospital stay (LOS) (9.5±3.0 days versus 15.7±9.4 days; P=.044).
Conclusions:
In conclusion, LDP provides early recovery and better cosmetic appearance. In high anesthetic risk patients, LDP shows less operative time, less perioperative blood loss, a higher rate of spleen preservation, slighter complication, and shorter LOS, which might explain why LDP is a feasible and effective procedure.
Introduction
C
Although literature had been published to advise the effect of laparoscopic surgery and advocate its benefits, 6 there were still some contraindication of laparoscopic surgery. High anesthetic risk had been presumed to be a relative contraindication of laparoscopic surgery related to the prolonged pneumoperitoneum and increasing abdominal pressure, which induced further cardiopulmonary decompensation. 7 Based on combined improvements in anesthetic techniques and the increasing experience of surgical teams, findings of the feasibility and safety of laparoscopic surgery in several aspects were published in high anesthetic risk patients. 8 Nevertheless, knowledge regarding the response of patients at a high anesthetic risk during lengthy and technically demanding LDP is scarce.
The aim of this study is to assess the feasibility and safety of LDP in patients with high anesthetic risk.
Patients and Methods
Data collection
We conducted a prospective data collection and retrospective review of all patients who underwent pancreatic surgery from January 2011 until December 2013 at Chang Gung Memorial Hospital, Linkou, Taiwan. The study was approved by the Internal Review Board of Chang Gung Memorial Hospital. During this study period, we performed LDP and open distal pancreatectomy (ODP) concurrently. Demographic data, the American Society of Anesthesiologists (ASA) score, medical, operative, and postoperative characteristics, and information regarding complications were recorded into a computerized database prospectively. We conducted a retrospective review of patients underwent LDP and ODP in this time.
By the ASA score, patients were divided into two groups: low-risk group patients whose ASA scores were I–II and high-risk group patients whose ASA scores were III–IV. The age, gender, the ASA score, operative procedure, perioperative blood loss, operative time, spleen preservation or not, the occurrence of postoperative pancreatic fistula (POPF), and the complication grading by the Clavien–Dindo classification were collected. We also retrieved the length of postoperative hospital stay (LOS) and final prognosis.
We excluded the patients who underwent resection of multiple organs that included resection of the pancreas. We only included patients who underwent concomitant minor surgery such as cholecystectomy into this cohort, but the operative time was recorded only for distal pancreatectomy. Patients who had had past pancreatic or splenic surgery were excluded from this cohort.
Procedure
Caudal approach technique: an easy and safe laparoscopic distal pancreatectomy method
During the operation, the patient was placed in a supine position under general anesthesia, and a nasogastric tube and a Foley tube were inserted. One 12-mm subumbilical incision was made, and pneumoperitoneum was created to 10 mm Hg. One 12-mm port was inserted in the incision, followed by one 30° rigid 10-mm videoscope. The peritoneal cavity was fully explored, and all potentially interfering adhesions were lysed. Two 12-mm ports were set both at the midclavicular line at the level about the umbilicus, and another two 5-mm ports were set at the bilateral subcostal margin (Fig. 1). Then, the patient was placed in the reverse Trendelenberg position, which allows exploring the peritoneal cavity, and all potentially interfering adhesions were lysed.
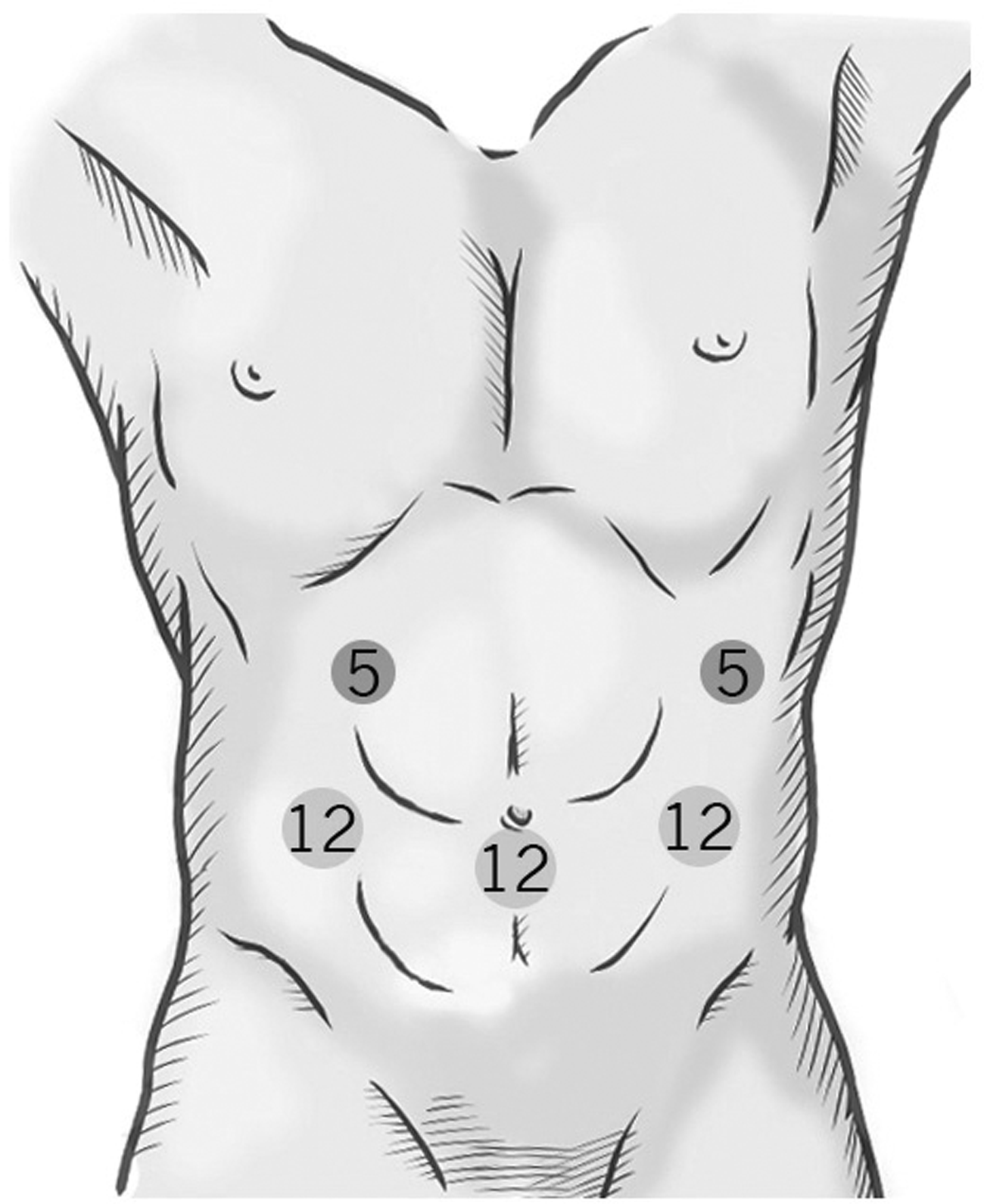
The insertion sites of trocars. 5, 5-mm; 12, 12-mm.
The first step is dividing the gastrocolic ligament for visualization of the pancreas. The dissection is continued to the short gastric vessels, which should be preserved. This procedure allows complete exposure of the pancreas. The second step is mobilizing the pancreas. We divided the posterior peritoneum at the inferior border of the pancreas near the superior mesenteric vein, at the junction of the pancreatic neck and body, and dissection was performed along the avascular plane (Fig. 2A). We continued to divide the peritoneum laterally toward the pancreatic tail and to make the pancreas as free as possible. Next, we opened the peritoneum along the superior border of the pancreas to prepare for tunneling. Then we mobilized and lifted the pancreas from the superior mesenteric vein and splenic vein (SPV) (Fig. 2B). After totally detaching the pancreas from the SPV and superior mesenteric vein, we taped the pancreatic neck and performed intraoperative ultrasonography to determine the tumor location and to design the resection line (Fig. 2C).
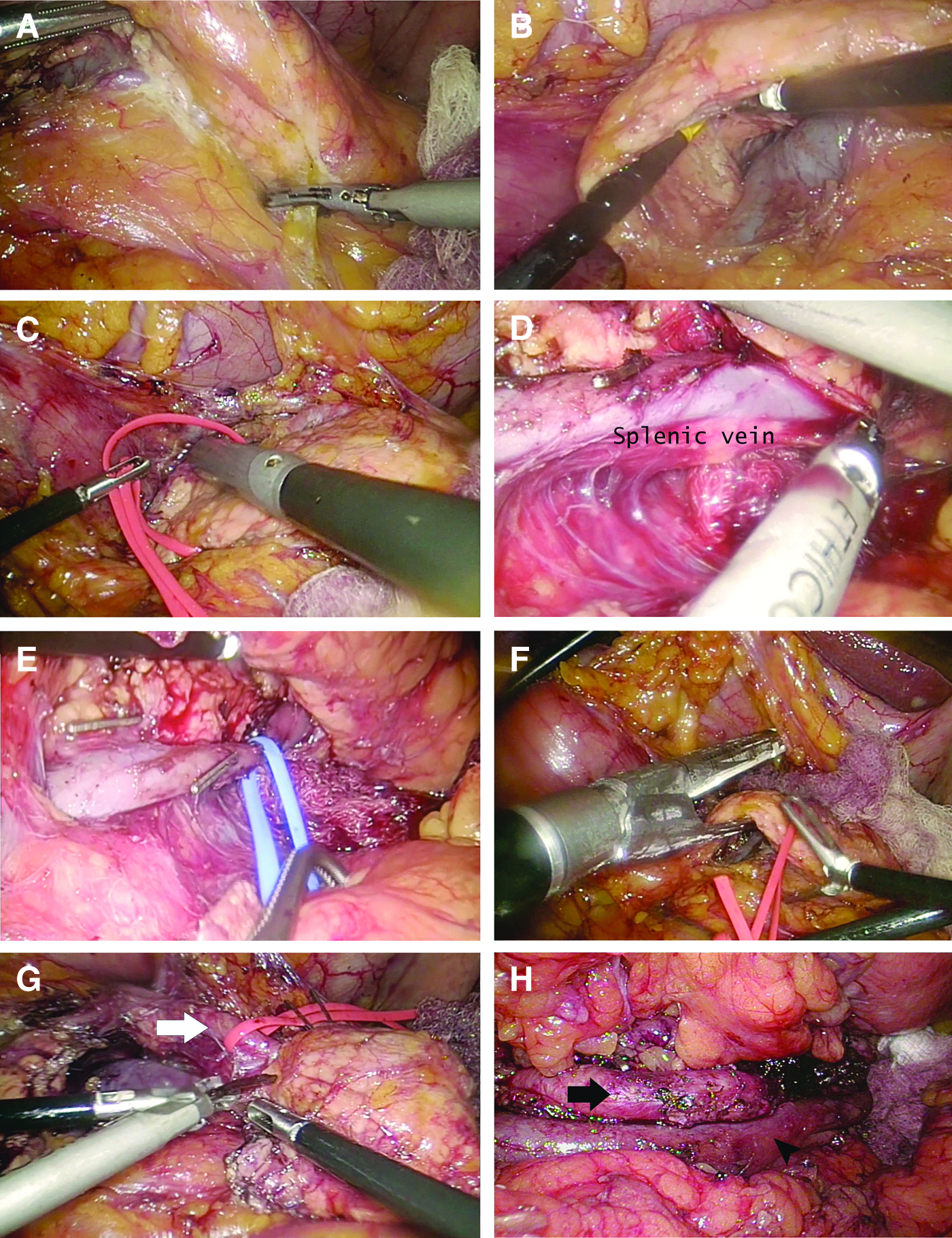
After the pancreatic mobilization, we usually isolate the SPV from the posterior wall of the pancreas. Wide mobilization and rotation of the dorsal surface of the pancreatic body in the cranial direction enable the SPV to be easily identified at the posterior wall of the pancreas. Usually, the SPV is embedded in the sulcus of the pancreatic parenchyma, finally becoming exposed at the pancreatic tail (Fig. 2D). The dorsal pancreatic fascia can longitudinally be opened with the ultrasonic device, and then the SPV can be released from the pancreas. One tape was circled around the SPV, and then proper dissection toward the pancreatic tail was performed. With traction on the SPV, tiny branches to the pancreas were carefully clipped and divided (Fig. 2E).
We usually use the stapler to transect the pancreas at the designed resection line (Fig. 2F). With inferior traction on the pancreatic body and tail, Toldt's fusion fascia was dissected at the superior edge of the splenic artery (SPA). The tape encircling the SPA was drawn out from the posterior surface of the pancreas in the ventral and cranial directions (Fig. 2G). Thus, retraction and cranial traction of the SPA were very useful when dissecting between the SPA and pancreatic parenchyma. With inferior traction and rolling of the pancreatic body and tail and superior traction on the vessel tapes, the SPA and SPV were completely isolated from the pancreatic parenchyma (Fig. 2H). Then the pancreas resection was completed. The specimen was extracted through the umbilical incision, which was extended to 2 cm in length under the protection of a ring protector. Finally, the pancreatic stump was enforced by suture, and then tissue glue was applied at the pancreatic stump and splenic hilum.
Alternative method for spleen preservation: Warshaw's technique. 9
When the tumor encased the SPV or SPA, we performed resection of the SPV, the SPA, or both vessels. The splenic vessels may be divided simultaneously during pancreatic transection using a stapler. After ligation of splenic vessels, we preserve the short gastric and left gastroepiploic vessels to maintain the blood supply of the spleen.
Statistical analysis
Pearson's chi-squared test and Fisher's exact test were used as appropriate to compare categorical variables. Quantitative variables were compared by Student's t test. Statistical analysis was done with SPSS version 20.0 for the Mac (SPSS Inc., Chicago, IL). A value of P<.05 was considered statistically significance.
Results
Study population
The cohort included 77 patients: 20 in the LDP group and 57 in the ODP group (Table 1). The mean age was 57.5 years for the LDP group and 49.7 years for the ODP group (P=.058). The ASA scores of patients in the LDP and ODP groups were comparable (P=.433). The overall operating time was significantly shorter in the LDP group than in the ODP group (mean, 225.3±112.5 minutes versus 286.4±116.2 minutes; P=.045). The blood loss was less in the LDP group than in the ODP group (382.5±566.8 mL versus 750.2±1262.4 mL; P=.213). The rate of spleen preservation was significantly higher in the LDP group than in the ODP group (75% versus 42.1%; P=.011). The POPF rate was comparable in both groups (40.0% versus 40.4%; P=.437). There were nine postoperative complications in the LDP group, and there were 26 patients with complications in the ODP group (P=.470). The average LOS was 9.4±2.9 days for the LDP group, which was shorter than the 13.1±7.8 days for the ODP group (P=.044). There was no perioperative 30-day mortality in the LDP group, whereas 1 patient died beause of profound sepsis within 30 days after the operation in the ODP group.
ASA, American Society of Anesthesiologists; HLOS, hospital length of stay; LDP, laparoscopic distal pancreatectomy; ODP, open distal pancreatectomy; SD, standard deviation.
Low anesthetic risk patients
In low-risk patients, the mean age was older in the LDP group than in the ODP group (60.6±17.0 years versus 47.5±15.7 years; P=.104). However, there was no significant difference in perioperative blood loss, operative time, rate of spleen preservation, and incidence of POPF or complication between the two groups. The LOS was comparable in both groups (Table 2).
HLOS, hospital length of stay; LDP, laparoscopic distal pancreatectomy; ODP, open distal pancreatectomy; SD, standard deviation.
High anesthetic risk patients
In high-risk patients, the overall operating time was slightly shorter in the LDP group than in the ODP group (mean, 220.8±101.1 minutes versus 299.4±124.3 minutes; P=.038). The blood loss was less in the LDP group than in the ODP group (409.3±569.9 mL versus 1083.1±1583.0 mL; P=.039). The rate of spleen preservation was higher in the LDP group than in the ODP group (73.3% versus 43.8%; P=.037). The POPF rate was comparable in both groups (40.0% versus 43.8%; P=1.000). There were seven postoperative complications in the LDP group, and there were 17 patients with complications in the ODP group (P=.680). The average LOS was 9.5±3.0 days for the LDP group, which was shorter than the 15.7±9.4 days for the ODP group (P=.044) (Table 3).
HLOS, hospital length of stay; LDP, laparoscopic distal pancreatectomy; ODP, open distal pancreatectomy; SD, standard deviation.
Discussion
In all patients in this study, LDP provided less blood loss, higher spleen preservation, and a shorter LOS than ODP. These results had been proved by previous series focused on comparing ODP and LDP.10,11 Moreover, we recognized the benefits of LDP in patients with high anesthetic risk. In low-risk patients, the benefits of LDP were not significant. However, in high-risk patients, LDP provided less blood loss (409.3±569.9 mL versus 1083.1±1583.0 mL; P=.039), a shorter operative time (220.8±101.1 minutes versus 299.4±124.3 minutes; P=.038), higher spleen preservation (73.3% versus 43.8%; P=.037), and a significantly short LOS (9.5±3.0 days versus 15.7±9.4 days; P=.044).
The caudal approach provided a unique surgical view that allows surgeons to approach vessels first that are difficult in conventional open surgery. In open surgery, it is difficult to access the SPV unless widely dissecting the peritoneal attachment around the pancreas and spleen. However, by the caudal approach, surgeons can approach the SPA and SPV with limited dissection in the early phase of surgery. Simple assessment of vessels and easy vascular control decrease the blood loss.12,13 The magnified view under the videoscope helps surgeons to recognize and to ligate small branches from the splenic vessels meticulously. For all of these reasons, the blood loss was significantly less in LDP than in ODP as previous reports presented.14,15 Furthermore, the improvement of technology such as usage of energy devices, a high-resolution videoscope, and an auto-inflation–suction system can create a clean and bloodless surgical field. The combination of both the clean surgical field and less dissecting range can shorten the operative time in LDP. For high-risk patients, the shorter operative time and the diminished blood loss were both factors to decrease the perioperative risk and to prevent physical decompensating.
Splenic preservation is another challenge when performing distal pancreatectomy. By experience, there were two major methods to achieve spleen preservation. The first method is preservation of splenic vessels from pancreatic parenchyma and just ligation of the penetrating vessels into the pancreas. 16 The second method is the method of Warshaw, 9 which preserves the short gastric and left gastroepiploic vessels with resection of the SPA, SPV, or both. Owing to the magnified view under the scope, the pancreatic structure and vessels can be identified clearly. The splenic vessels can be dissected from the pancreatic parenchyma precisely without injury to these vessels, even short gastric vessels. That can explain why higher splenic preservation was achieved in LDP than in ODP, as was stated by other authors.11,15 With spleen preservation, which may reduce the infection with some bacteria and maintain immune efficiency, the incidence of complications may be reduced.17,18 That might be a reason why the LOS in LDP is shorter than in ODP.
The incidence of POPF was previously around 9%–50%,11,19 and the incidence of POPF was 40.3% in this study. The POPF formation was similar in LDP and ODP. After transection of the pancreas, the pancreatic stump was sutured to enhance the security. Furthermore, we used fibrin glue, whether in LDP or ODP, at the stump, dissected fossa, and splenic hilum to prevent POPF. The incidence was still high in both groups. However, most of our patients had mid-POPF and recovered smoothly. Only 2 patients in the ODP group suffered from severe abscess and sepsis.
In the low-risk group, the surgical complication and recovery were similar between the LDP and ODP groups. For relative healthy patients, the recovery from surgery seemed quick, and it was not obviously different which procedure they had had. However, in high-risk patients, the different procedures make the postoperative recovery significantly different. Because of decreased blood loss and the shortened operative time, recovery of the high-risk patients was better in LDP. Furthermore, higher spleen preservation in LDP maintains the immunity. All of these benefits gave the high-risk patients a shorter LOS with LDP. Although the complication rates were comparable between LDP and ODP in high-risk patients, the grade of complication was slightly less in the LDP group15,20 (Table 3). Among the high-risk patients, there was only 1 patient (14.3%) with a complication more than grade III in LDP; however, more than half of the patients (52.9%) had a complication more than grade III in ODP. This result indicated that LDP not only offered minimal invasion and less trauma, but also diminished the severity in the presence of complications. 15
Also, LDP provided additional advantages over ODP because of less trauma and postoperative pain. Shortening the length of the incision decreased the possibility of not only incisional hernia, but also surgical wound infection. 21 Minimally invasive surgery helps patients recover ambulation and pulmonary toilette smoothly, thus decreasing the possibility of pulmonary atelectasis and venous thromboembolic events.
The hesitations about laparoscopic surgery in the high-risk patients were related to the pneumoperitoneum and increasing abdominal pressure. Intraabdominal pressure increases in both systemic vascular resistance and central venous pressure, together with decreased cardiac output. This can be detrimental for patients whose cardiac function is compromised. 7 Furthermore, insufflation of the abdomen can produce a vagal response to peritoneal distension, causing bradyarrhythmias, whereas CO2 can induce rhythmic disturbances because of cardiac irritability.22,23 Therefore, laparoscopic surgery had been relatively contraindicated in the high-risk patients. That prolonging the surgical time with high intraabdominal pressures typically increases CO2 absorption is another consideration in the hesitations about laparoscopic surgery in risky patients. To reduce the effect of pneumoperitoneum and high intraabdominal pressures, we intermittently deflate and release the pneumoperitoneum to minimize its side effects.14,19 Moreover, in this series, we found a decreased operative time in LDP compared with ODP; therefore, surgical time might not be considered a risk factor of LDP. No patients experienced an expectable anesthetic event during operation. All high-risk patients can tolerate the pneumoperitoneum and intraabdominal pressures, and none of these anesthetic problems required conversion to open surgery in this study. Arteaga González et al. 8 found that laparoscopic surgery may be safe and feasible in high-risk patients, and here we add further evidence that LDP is feasible and effective in high anesthetic risk patients.
Although this study demonstrated the benefits of LDP in high anesthetic risk patients, there were still some deficits in this study. First, the study is a retrospective study; the selective and recall bias cannot be avoided because of the study nature. Although the patients' demographic distribution was similar in both groups, the bias still cannot be completely prevented. Another cause is the limited number of patients, which decreased the statistical power. Our findings should be confirmed in future prospective, randomized controlled trials that compare LDP and ODP for increasing number of patients having benign disease of the pancreas.
In conclusion, LDP provides early recovery and better cosmetic appearance than ODP. In low anesthetic risk patients, the benefits of LDP are not significant. However, in high anesthetic risk patients, LDP shows less operative time, less perioperative blood loss, a higher rate of spleen preservation, slighter complications, and a shorter LOS, thus suggesting that LDP is a feasible and effective procedure.
Footnotes
Disclosure Statement
No competing financial interests exist.