
Abstract
Abstract
Objective:
The aim of this study was to clarify the role of thoracoscopic plication for diaphragmatic eventration after surgery for congenital heart disease (CHD) in children.
Patients and Methods:
We retrospectively reviewed the medical charts of pediatric patients who had undergone thoracoscopic plication of diaphragmatic eventration after surgery for CHD between 2008 and 2013 at our department.
Results:
Five patients were identified during the study period. The median age and body weight of the patients were 7.6 months and 6.6 kg, respectively. The associated CHDs were pulmonary artery atresia in 3 patients, truncus arteriosus in 1 patient, and double-outlet right ventricle in 1 patient. Four patients needed preoperative mechanical respiratory support. At operation, all the patients received CO2 insufflation (4 mm Hg), and single-lung ventilation was attempted in 3 patients using a bronchial blocker. A sufficient operative field was maintained by CO2 insufflation in all the patients regardless of single-lung ventilation. The procedure was not converted to open operation in any patient. Postoperative extubation was performed in the operating room in 1 patient, on the day of operation in 2 patients, and on postoperative Days 1 and 2 in 2 patients. Air embolism was not observed in any of the patients. Diaphragmatic eventration did not recur in any of the patients after thoracoscopic plication.
Conclusions:
Thoracoscopic plication is a safe and effective procedure for pediatric diaphragmatic eventration after surgery for CHD. Considering the sufficient operative field maintained by CO2 insufflation, single-lung ventilation using a bronchial blocker would be unnecessary for this procedure. With its safety and good outcome, early thoracoscopic plication is a good treatment option for pediatric patients with symptomatic diaphragmatic eventration after surgery for CHD.
Introduction
D
Diaphragmatic plication has been traditionally performed via open thoracotomy. With advances in endosurgery, several reports have been published on thoracoscopic diaphragmatic plication in adults 9 and children.10–13 Because it involves minimal injury on the thoracic wall, thoracoscopic diaphragmatic plication was advocated as a safe procedure with less morbidity and quick recovery in children. 11 Thoracoscopic diaphragmatic plication was also performed in neonates. 14
Theoretically, the advantages of thoracoscopic plication can be applied in pediatric patients who develop diaphragmatic eventration after cardiac surgery for CHD. However, the perioperative safety of thoracoscopic surgery for such patients is a source of possible concern. The aim of the present study was to clarify the role of thoracoscopic plication in the recovery of children with diaphragmatic eventration after surgery for CHD.
Patients and Methods
Patients
All pediatric patients who had undergone thoracoscopic plication of diaphragmatic eventration after surgery for CHD between 2008 and 2013 were included in the study. Preoperative and postoperative clinical data were retrospectively collected from a chart review.
Surgical procedure
Under general anesthesia, the patients were placed in the lateral position. CO2 insufflation (4 mm Hg) was applied for lung collapse in all the cases. Single-lung ventilation by a commercially available bronchial blocker was also performed in some cases. Generally, the optical port (5 mm) was placed in the fourth intercostal space on the middle axillary line, and two working ports (4 mm) were placed in the fourth intercostal space on the anterior axillary line and in the fourth or fifth intercostal space on the posterior axillary line. The position of the port was adjusted for each patient, and an extra working port was used in some early cases. After grasping and pulling using forceps, the eventrated diaphragm collapsed owing to intrathoracic pressure due to the CO2 insufflation, which indicated no adhesion to the diaphragm in the abdominal cavity (Fig. 1). The redundant diaphragm was plicated using running sutures (3-0 Ti-Cron™; Covidien, Mansfield, MA) with extracorporeal knots. Intrathoracic CO2 was removed at the end of procedure, and a chest tube was not used.
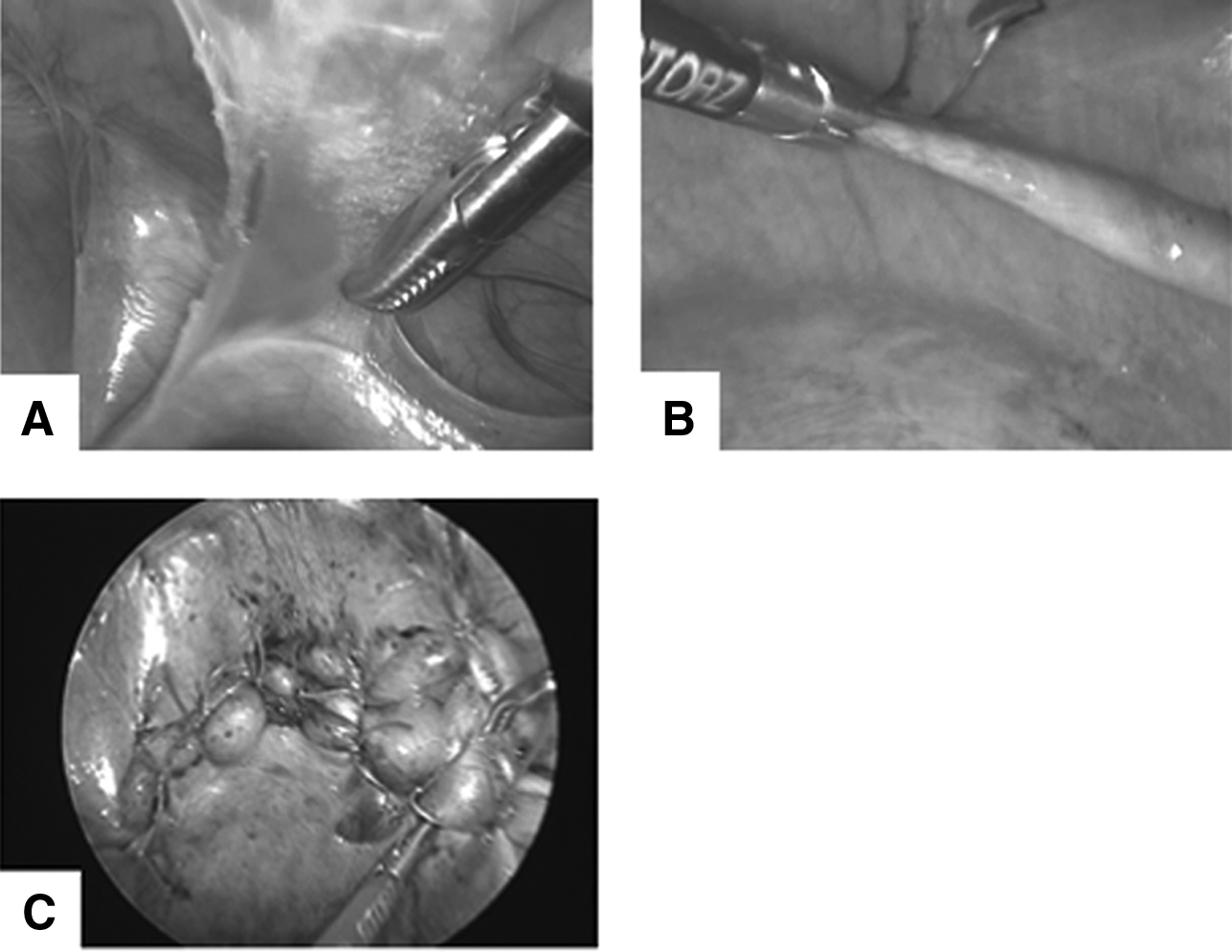
Thoracoscopic view (Case 5).
Data notation and ethics
Numerical data were expressed as median (range), if not indicated otherwise. This study was approved by the institutional ethical committee.
Results
During the study period, 5 patients (4 boys and 1 girl) who had undergone thoracoscopic plication of diaphragmatic eventration after surgery for CHD were included in the study (Table 1). No open or laparoscopic plication was performed for diaphragmatic eventration during the study period. The median age and body weight at thoracoscopic plication were 7.6 months (1.8–17.9 months) and 6.6 kg (3.0–7.1 kg), respectively. All the patients had left-sided diaphragmatic eventration. The associated CHDs were pulmonary artery atresia in 3 patients and truncus arteriosus and double-outlet right ventricle in 1 patient each. The previous operations for CHDs were the Glenn operation in 3 patients, complete repair for truncus arteriosus in 1 patient, and right ventricle to pulmonary artery shunt in 1 patient. Two patients had a history of ipsilateral thoracotomy for Blalock–Taussig shunt. Three patients had a right-to-left shunt at the time of thoracoscopic plication.
Age, weight, and height at the time of the thoracoscopic diaphragmatic plication.
Ventilation support by nasal directional positive airway pressure.
CHD, congenital heart disease; DORV, double-outlet right ventricle; F, female; M, male; PA, pulmonary artery atresia; RV-PA, from the right ventricle to the pulmonary artery; TA, truncus arteriosus.
All the patients received oxygen supplementation, and 4 patients needed mechanical respiratory support (ventilator in 2 and nasal-directional positive airway pressure in 2 patients) before thoracoscopic plication (Table 1). The median interval between the previous CHD surgery and thoracoscopic plication was 56 days (15–169 days). The patient with the longest interval (169 days) was independent of mechanical ventilation. The indication for thoracoscopic diaphragmatic plication was difficulty in weaning from mechanical respiratory support in 4 patients and recurrent and persistent respiratory infection in 1 patient.
During thoracoscopic diaphragmatic plication, single-lung ventilation was attempted using a bronchial blocker in 3 of the 5 patients, and all 5 patients received CO2 insufflation (4 mm Hg) for ipsilateral lung collapse. A sufficient operative field was maintained with CO2 insufflation in all the patients, regardless of single-lung ventilation. The procedure was not converted to open operation in any patient (Fig. 1). The median operative time was 140 minutes (92–169 minutes). In 1 patient, the dislodgement of the bronchial blocker just before the operation resulted in severe respiratory and circulatory failures; the patient needed intraoperative nitric oxide inhalation and also underwent thoracoscopic diaphragmatic plication after stabilization. Although the patients had mild intraoperative acidosis (pH 7.29 [7.22–7.39]) and hypercapnia (51 mm Hg [44.5–67 mm Hg]), their intraoperative lactate levels were almost within the reference range (11 mg/dL [3–19 mg/dL]; reference range, 4.5–18 mg/dL), suggesting sufficient peripheral tissue oxygenation.
Postoperative extubation was performed at the operation room in 1 patient, on the day of the operation in 2 patients, and on postoperative Days 1 and 2 in 2 patients. One patient experienced minor pneumothorax and pleural effusion, which resolved spontaneously without drainage. Air embolism was not observed in any of the patients. One patient died of heart failure 15 months after thoracoscopic plication. No recurrence of diaphragmatic eventration was experienced in this series.
Discussion
To the best of our knowledge, this is the first study that focuses on thoracoscopic diaphragmatic plication using a minimally invasive technique for pediatric patients with diaphragmatic eventration after cardiac surgery for CHD. A few cases of thoracoscopic plication have been reported in some case series of diaphragmatic eventration due to various causes, including congenital phrenic nerve palsy, birth injury, and after cardiac or thoracic surgery.10,12
As expected, good short- and long-term outcomes such as early extubation have been observed in patients with diaphragmatic eventration after cardiac surgery for CHD who had preoperative dependence on mechanical ventilator support, minimal complications, and no recurrence. Less impairment of respiratory muscular function and immediate improvement of vital capacity induce early extubation after thoracoscopic diaphragmatic plication.10–12,15
For applying thoracoscopic surgery for patients who had undergone cardiac surgery for CHD, the following concerns should be addressed: intrathoracic adhesions after cardiac or thoracic surgery, circulatory and respiratory instability during operation due to CHD, and air embolization caused by a right-to-left shunt. In our series, 2 of the 5 patients had a history of ipsilateral thoracotomy for a Blalock–Taussig shunt. The moderate intrathoracic adhesions in these patients needed dissection. However, as all the operations were accomplished successfully without open conversion, intrathoracic adhesion after cardiac or thoracic surgery for CHD seemed no reason for avoiding thoracoscopic diaphragmatic plication. Although mild acidosis and hypercapnia were observed in the patients, sufficient peripheral tissue oxygenation, indicated by a normal lactate level and an intraoperative circulatory status such as blood pressure and heart rate, was maintained during the thoracoscopic operation. Early recovery from thoracoscopic surgery also suggests that pediatric patients with CHD can tolerate thoracoscopic diaphragmatic plication. Although 3 patients had a right-to-left shunt and all the procedures were conducted with CO2 insufflation, we experienced no air embolism after thoracoscopic plication. The low insufflation pressure (4 mm Hg) and minimal dissection through the thoracoscopic plication may be the reason for the absence of embolism.
The optimal management of diaphragmatic eventration due to phrenic nerve palsy after cardiac surgery in children remains controversial. Two different options—namely, conservative observation with ventilation support if necessary and thoracoscopic diaphragmatic plication—are usually considered for these patients. 16 Conservative observation is based on the possibility of spontaneous recovery from phrenic nerve palsy and is preferred for patients with mild symptoms. Meanwhile, diaphragmatic plication is preferred for patients with severe symptoms and children younger than 1 year. 16 However, the appropriate timing of the operation remains controversial. Some authors recommend performing the operation immediately after the diagnosis of diaphragmatic palsy is made, whereas others first recommend preoperative observation 1–6 weeks after the diagnosis.16,17 In patients who had undergone univentricular repair with the Fontan operation, early diaphragmatic plication reduced the risk of morbidity.18,19 Considering the safety, efficacy, and invasiveness of thoracoscopic diaphragmatic plication demonstrated in this study, early surgical intervention using a minimally invasive technique would be optimal for pediatric patients who develop diaphragmatic palsy after cardiac surgery.
Several technical details need to be considered in pediatric thoracoscopic diaphragmatic plication. Although Hines 12 preferred video-assisted plication using four ports, others selected thoracoscopic plication under CO2 insufflation.10,11,13–15,20 The advantages of CO2 insufflation include the following: a larger operative field obtained with the positive pressure in the thoracic cavity; complete plication of the diaphragm with CO2 insufflation, indicating no adhesion of the diaphragm to the abdomen; and the small number of port incisions (three ports in our series) in the thoracic wall. Some authors applied a relatively high insufflation pressure (6–8 mm Hg).10,11,15 However, our study showed that a low CO2 insufflation pressure of 4 mm Hg was enough for conducting thoracoscopic diaphragmatic plication and could be tolerated by the infants or children younger than 2 years who developed diaphragmatic eventration after cardiac surgery for CHD.
Another technical consideration is the usage of single-lung ventilation with a bronchial blocker. Both the application 14 and avoidance10,12 of single-lung ventilation have been reported in the literature. In 3 patients in the present study, single-lung ventilation was applied using a bronchial blocker, and 1 of the patients experienced severe preoperative respiratory and circulatory failures caused by the dislodgement of the blocker. Considering this harmful event and the fact that a sufficient operative field was maintained without single-lung ventilation, single-lung ventilation would not be necessary for children with thoracoscopic diaphragmatic eventration, especially in infants in whom it is difficult to perform single-lung ventilation.
The limitations of the study include the small number of patients, its retrospective design, and the lack of a control group. As all the diaphragmatic plication procedures during the study period were performed thoracoscopically at our department, we could not apply a proper control group in this study. Despite these limitations, our study demonstrated that thoracoscopic plication is a safe and effective treatment option in pediatric patients who develop diaphragmatic eventration after cardiac surgery for CHD. Considering the good results, designing a randomized controlled trial of open or thoracoscopic diaphragmatic plication might be difficult for such patients.
In conclusion, this is the first study to evaluate the role of thoracoscopic plication in the recovery of pediatric patients with diaphragmatic eventration after cardiac surgery for CHD and to demonstrate that thoracoscopic plication is a safe and effective procedure with low morbidity in such patients. Considering the sufficient operative field maintained by CO2 insufflation with a low pressure of 4 mm Hg and the possible serious complication of single-lung ventilation, single-lung ventilation using a bronchial blocker would be unnecessary for this procedure. With its safety and good outcome, early thoracoscopic plication is a good treatment option for pediatric patients who develop symptomatic diaphragmatic eventration after surgery for CHD.
Footnotes
Disclosure Statement
No competing financial interests exist.