
Abstract
Abstract
Background:
The aim of this study was to compare the perioperative and long-term oncologic outcomes of laparoscopic liver resection (LLR) and open liver resection (OLR) for single hepatocellular carcinoma (HCC) in case-controlled patient groups using the propensity score.
Patients and Methods:
Between January 2005 and February 2013, 292 patients underwent surgical resection for HCC. Of these, 202 patients who underwent surgical resection for initial treatment for a single mass were enrolled. These patients were divided into two groups according to the method of operation: the Lap group (patients who underwent LLR) and the Open group (patients who underwent OLR). To correct different demographic and clinical factors in the two groups, propensity score matching was used at a 1:1 ratio, and, finally, 102 patients were enrolled in this study, 51 patients in each group. Preoperative characteristics, perioperative results, and long-term results were retrospectively analyzed based on the prospectively recorded database.
Results:
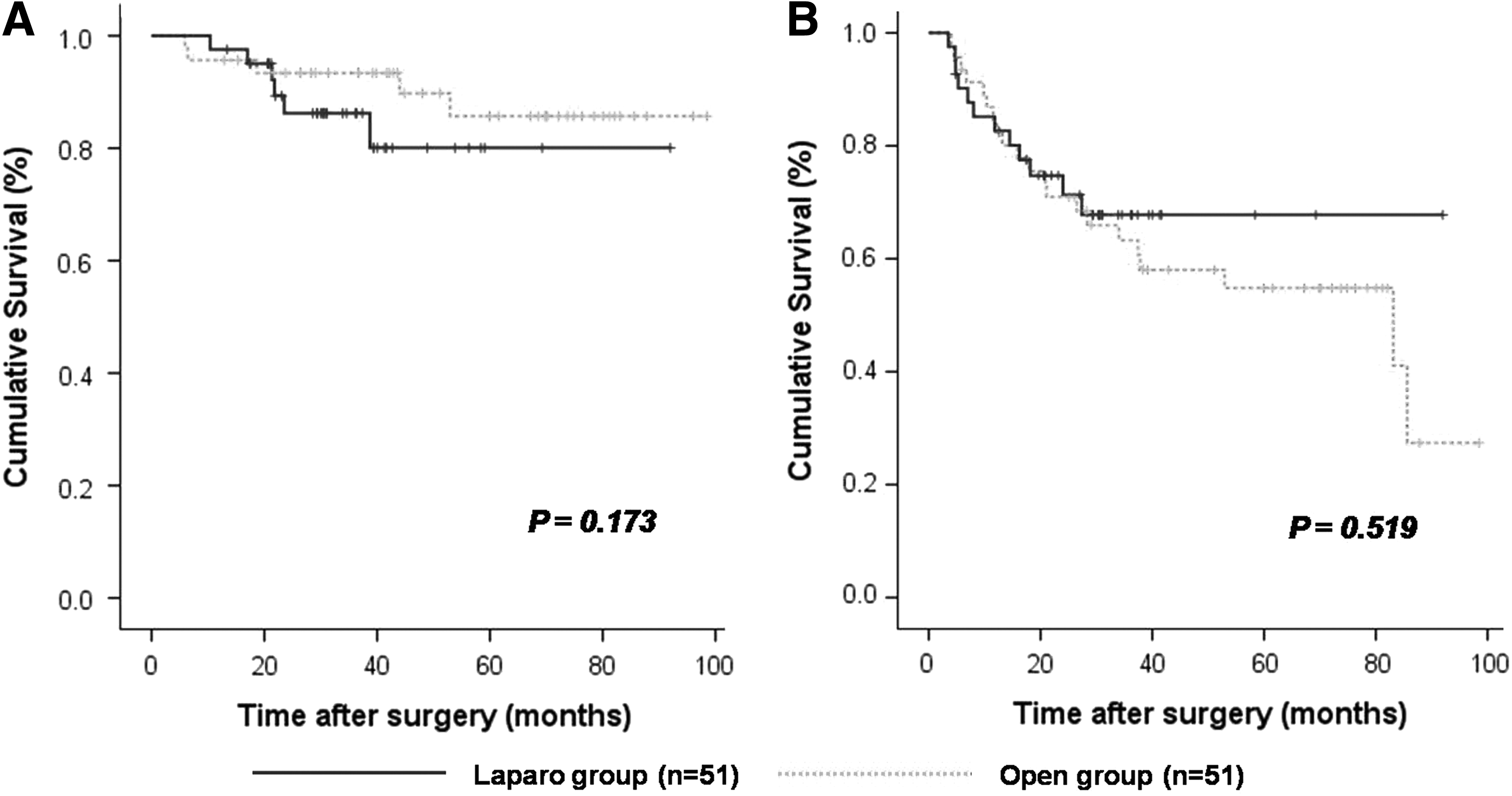
Preoperative baseline variables were well balanced in both groups. There were no differences of extent of surgery and rate of anatomical resection between the two groups. With the exception of a shorter postoperative hospital stay in the Lap group than that of the Open group (8.2 days versus 12.3 days; P=.004), there were no significant differences in perioperative, pathological, and long-term outcomes. The 5-year overall survival rates were 80.1% in the Lap group and 85.7% in the Open group, respectively (P=.173). The 5-year disease-free survival rates were 67.8% in the Lap group and 54.8% in the Open group, respectively (P=.519).
Conclusions:
LLR for HCC is safe, and long-term oncologic outcomes in selected patients were comparable to those who underwent OLR.
Introduction
R
Most patients with hepatocellular carcinoma (HCC) have chronic liver disease, including liver cirrhosis, and it makes LLR a more difficult and dangerous procedure. However, several perioperative benefits of LLR for cirrhotic patients, such as less pain, less bleeding, and shorter hospital stay, have been reported.14–18 However, the oncologic results of LLR for HCC still remain a matter of debate. Although several articles have been published showing results of LLR comparable to those of open liver resection (OLR) for HCC,14,16–19 most of them had selection bias, more feasible location (segment 2, 3, 4, or 5), less severe cirrhosis, and frequent minor resection for laparoscopic resection.16–18 That would mean that advantages of LLR would be weakened without adjusting for these biases. Therefore, a well-matched study is needed for proving long-term oncologic safety, as well as technical safety, of LLR for HCC.19–21 Propensity score matching is a useful method to reduce selection bias in the nonrandomized observational study. 22 It offers investigators the ability to balance treated groups across all putative risk factors and allows them overcome the selection biases.
The purpose of this study was to compare the perioperative and long-term oncologic outcomes of LLR and OLR for single HCC in groups of well-matched patients using propensity score matching.
Patients and Methods
Study population and study design
To determine operative methods and extent of resection, all patients with HCC were evaluated by preoperative assessment of liver function (chemistry, Child–Pugh classification, and indocyanine green retention rate at 15 minutes [ICG-R15]) and dynamic computed tomography scan. In selected patients, contrast-enhanced magnetic resonance imaging was performed. These preoperative assessments and intraoperative ultrasonography delineated the location and multiplicity of the tumors and their anatomical relation with the major vascular structure. There were no standard criteria for selection of laparoscopic or open resection. LLR was applied to patients with Child–Pugh Class A cirrhosis, without invasion or close to the main portal pedicle or major hepatic veins. The relative indication for LLR was peripherally located small lesions. However, tumor location or size alone was not a contraindication. A tumor located close to major vasculature or biliary structures was not an indication for the laparoscopic procedure. Nonanatomical liver resection was usually performed for patients with peripherally located tumors. Sectionectomy or hemihepatectomy was considered when the tumor was deeply located and remaining liver function was expected to be adequate.
Between January 2005 and February 2013, 292 patients underwent surgical resection for HCC. Among these patients, LLR was performed in 72 patients. Those patients with previous treatment for HCC (hepatic resection, percutaneous radiofrequency ablation, or transarterial chemoembolization), noncurative resection, presence of portal vein thrombus, ruptured HCC, and multiple HCC were excluded in this study. In addition, 5 cases of conversion to open surgery (3 cases due to bleeding and 2 cases due to exposed tumor margin) were excluded. The remaining 202 patients were enrolled for this study, and these patients were divided into two groups according to the method of operation: the Lap group (n=52; laparoscopic resection) and the Open group (n=150; open resection). To correct for different demographic and clinical factors in the two groups, propensity score matching was used at a 1:1 ratio, and, finally, 102 patients were enrolled in this study, 51 patients in each group (Fig. 1).
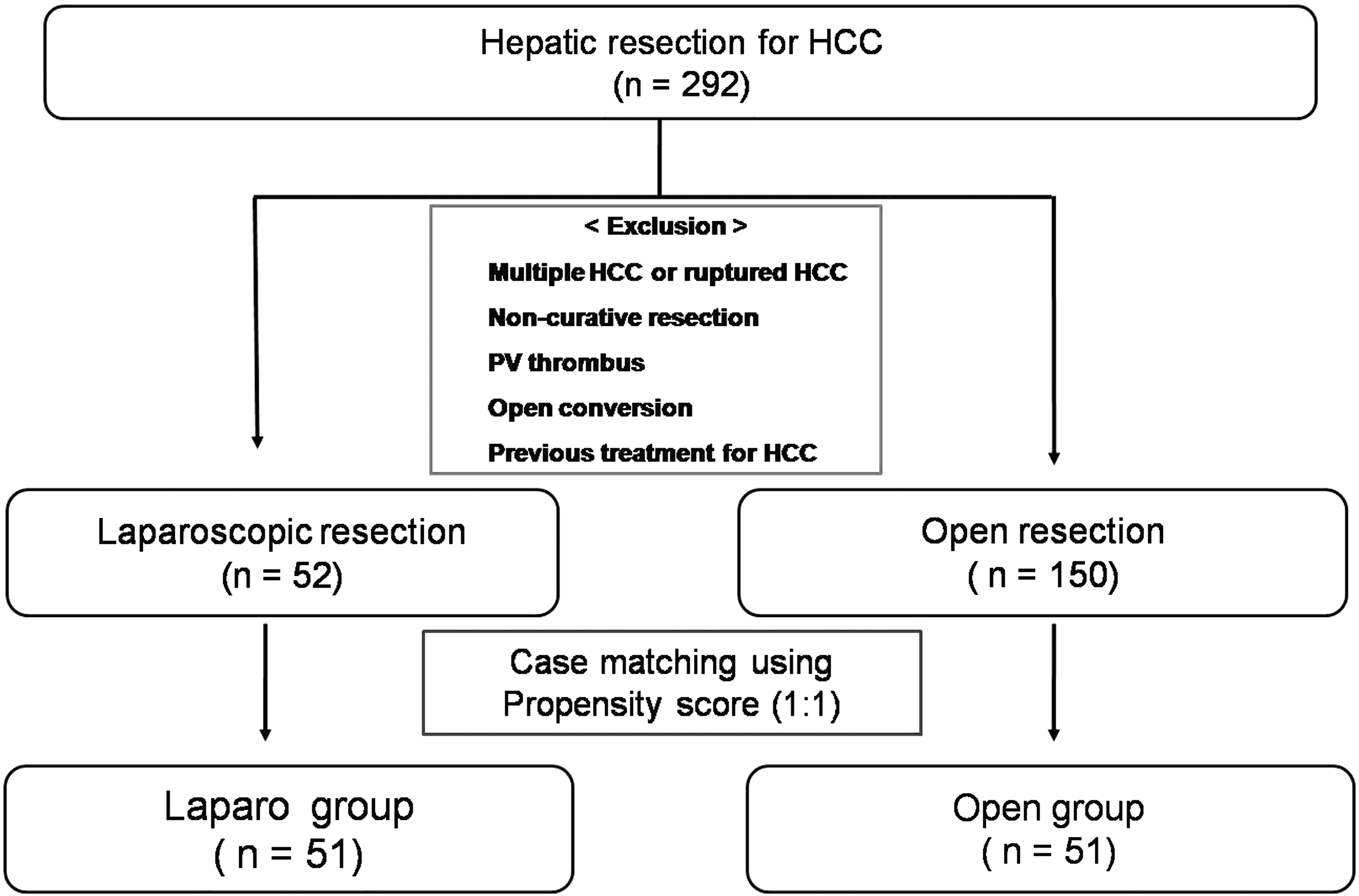
Study design and population. HCC, hepatocellular carcinoma; PV, portal vein.
This study protocol was reviewed and approved by the Institutional Review Board at Keimyung University Dongsan Medical Center (Daegu, Republic of Korea).
Operative procedure
The operative techniques for OLR in our institution have been described elsewhere. 23
Laparoscopic procedures were performed by the total laparoscopic approach. The patient was placed supine in the reverse Trendelenberg position, with or without the lower limbs apart. When tumorectomy of segment 7 or 8 was performed, the patient kept with 45°–60° of right decubitus position contralaterally. Usually, three to five ports (5–12 mm) were used, and the intraabdominal pressure was maintained below 12 mm Hg. A 30° telescope was used, and the liver was examined by direct vision. As necessary, intraoperative ultrasonography (model PLF-308P; Toshiba Corp., Tokyo, Japan) confirmed the location of the lesions and identified their relationship with the intrahepatic vascular structures. In the case of hemihepatectomy or sectionectomy, the portal pedicles were dissected and divided outside or inside the parenchyma during transection with a Hem-o-lok® clip (Weck Teleflex Medical, Research Triangle Park, NC) or linear stapler according to the size. The Pringle maneuver was applied as necessary, with an endovascular clamp. Transection of the superficial parenchyma was performed with a Harmonic Scalpel® (Ethicon Endo-Surgery, Cincinnati, OH) or LigaSure™ (Tyco Healthcare, Princeton, NJ), and the deeper portion of the parenchyma was dissected using a laparoscopic Cavitron ultrasonic surgical aspirator (Valleylab Inc., Boulder, CO). After completion of the hepatic transection, fibrin glue sealant (Greenplast®; Green Cross Corp., Seoul, Republic of Korea) was sprayed on the raw cut surface. The resected specimen was placed in a vinyl bag and extracted through an incision that was created by extending the wound at the umbilicus or additional minilaparotomy.
Follow-up and diagnosis of recurrence
The routine follow-up program consisted of physical examination, computed tomography, and laboratory tests, including levels of alpha-fetoprotein and protein induced by vitamin K absence/antagonist-II, every 3 months for the first 2 years and then every 6 months for the next 3 years, which then was done annually for patients who had neither recurrence nor metastasis.
Clinical analysis
Preoperative demographic factors, perioperative results, and long-term oncologic results were analyzed retrospectively based on the prospectively recorded database. Postoperative morbidity was graded by Clavien–Dindo classification. 24
Statistical analysis
With the propensity scoring method, 1:1 matching from the primarily enrolled 202 patients was done. Propensity scores were generated with the baseline characteristics, including age, sex, body mass index, underlying liver disease, presence of liver cirrhosis, ICG-R15, extent of resection (hemihepatectomy, sectionectomy and segmentectomy, or tumorectomy), and location and size of the tumor. The matching method was used for comparison. The logistic regression model of the propensity score for the two groups and the above covariates was appropriately based on the assessment of Hosmer–Lemeshow goodness of fit (P=.472). 25
All the continuous values were expressed as mean±standard deviation values, and categorical data were expressed as number or frequency (%). Statistical analysis was performed using an independent-samples t test for continuous parameters and Pearson's chi-squared test or Fisher's exact test (when expected cell frequencies were less than 5) for categorical parameters. Survival rates were estimated using the Kaplan–Meier method and compared using the log-rank test. The differences were considered significant at a P value of <.05.
All the statistical analyses were performed using Statistical Package for Social Science for Windows™ release 20.0 (SPSS Inc., Chicago, IL) and R version 2.12.1.
Results
Demographic and preoperative data
The patient population consisted of 26 women and 76 men, with a mean age of 57.7 years (range, 32–81 years). All preoperative baseline variables, including body mass index, alpha-fetoprotein, ICG-R15, underlying liver disease, laboratory findings, and tumor location, were well balanced in both groups (Table 1).
AFP, alpha-fetoprotein; ASA, American Society of Anesthesiologists physical status classification system; BMI, body mass index; ICG-R15, indocyanine green retention rate at 15 minutes; INR, international normalized ratio; Lap group, laparoscopic group; mAU, milli–arbitrary units; PIVKA-II, protein induced by vitamin K absence/antagonist-II.
Perioperative outcomes
Table 2 summarizes perioperative outcomes. There were no differences of extent of surgery and rate of anatomical resection between the two groups. Mean ischemic time, estimated bleeding amount, rate of transfusion, operative time, and postoperative complication were similar between the two groups. However, the postoperative hospital stay period was significantly shorter in the Lap group than in the Open group (8.2 days versus 12.3 days; P=.004). There was no in-hospital mortality in either group.
Lap group, laparoscopic group; S, segment.
Histopathologic results
Table 3 summarizes histopathological outcomes. Mean tumor size was 2.7±1.3 (range, 0.8–9.5 cm), and the surgical margin was cleared in all patients. Most of the tumors were <5 cm in size; however, for 3 patients in each group, the tumor size were >5 cm. The maximal tumor diameter in the Lap group was 9.5 cm, and that in the Open group was 7.8 cm. All pathological parameters, including presence of cirrhosis, mean tumor size, mean resection margin, differentiation, and rates of microvascular invasion, were not different between the two groups.
Lap group, laparoscopic group.
Long-term oncologic outcomes
The mean follow-up period was 38.6 months (range, 10–92 months) for the Lap group and 52.3 months (range, 6–98 months) for the Open group. In the Lap group, 12 patients had recurrences, and 6 (50%) of them were dead because of cancer recurrence. In the Open group, 21 patients had recurrences, and 5 of them were dead. The pattern of recurrence (intrahepatic/extrahepatic) was similar between the two groups. Among patients with recurrence, extrahepatic metastases occurred in 2 patients (16.7%) of the Lap group and 5 patients (23.8%) of the Open group. The 5-year overall survival rates were 80.1% in the Lap group and 85.7% in the Open group. The 5-year disease-free survival rates were 67.8% in the Lap group and 54.8% in the Open group. The overall survival and disease-free survival rates were similar between the two groups (Fig. 2).
Discussion
Although LLR is technically demanding, it has been applied to more difficult procedures, and the limitation of laparoscopic hepatectomy has been overcome. In the present study, in about 20% of the Lap group, tumors were located in segments 7 and 8 and in 3 patients, and tumor sizes were >5 cm (maximal size was 9.5 cm). Tumor location or size alone would not be a limitation for the laparoscopic approach, and LLR should be considered based on the combined factors of tumor size, tumor location, severity of cirrhosis, and experience of the surgeon. However, still the best indications for LLR for HCC are tumor diameter of <5 cm, a single nodule, and peripheral lesion (segments 2–6). 11 As previously mentioned, although many reports showed oncologic safety of LLR,14,16–19 most of them had limited numbers of patients and selection bias of tumor size or location. Major resection and anatomical resection for large mass tend to be performed by open resection. Therefore, a randomized controlled study of laparoscopic versus open resection for HCC is still absent. We used the propensity score matching method, which was designed to balance the baseline covariates between groups. In the absence of a randomized controlled study of laparoscopic versus open resection for HCC, this method would be desirable for a comparative study showing the oncologic safety of LLR.
The present study focused on the oncologic safety of laparoscopic hepatectomy for HCC. Therefore, unlike previous case-matched studies, tumor factors that could affect long-term outcomes regardless of procedure types (laparoscopic or open approach) were excluded. Although laparoscopic hepatectomy can be applied to patients with multiple tumors, 5 the long-term outcome would be determined not by type of procedure (laparoscopic or open approach) but by tumor factor, because the occurrence of multiple or intrahepatic metastases is a definite poor prognostic factor. 26 Previous treatment such as radiofrequency ablation or transarterial chemoembolization also could become a confounding factor. Open conversion cases were excluded because these cases were too vague to classify as either Lap or Open group.
Therefore, only those patients who underwent surgical resection for initial treatment of a single mass were included in this study. With these conditions, the pattern of recurrence and the long-term outcomes were not different. This means that LLR for HCC has oncologic safety comparable to that of OLR. Moreover, although demographic characteristics were similar, the postoperative hospital stay was shorter in the Lap group. Although we excluded 5 cases of open conversion, the amount of bleeding was not different between the two groups when we included these patients in the Lap group (data was not shown).
In other studies, not only shorter hospital stay but also less blood loss and shorter operative time were reported as benefits of the laparoscopic procedure.14,16,17,20,21 Therefore, LLR for HCC is superior to open resection in selected conditions considering the better perioperative results. There are additional oncologic benefits in the long-term aspect. The lesser degree of postoperative adhesion compared with the open procedure would make it easier in the approach for subsequent surgery, repeated resection, or salvage transplantation in the case of recurrent HCC. 27 These potential oncologic benefits can make the laparoscopic approach be more desirable for HCC than the open approach.
However, our study has a few limitations. Although at baseline the patient groups were well balanced, this was a retrospective and nonrandomized study. In addition, propensity score matching itself has limitations. Although previous reports adjusted baseline characteristics with the propensity score, the laparoscopic approach was still preferred in small and better locations, and minor resection was the predominant procedure. Although a few experienced centers have reported good results of a laparoscopic major resection or resection of a posterosuperiorly located tumor, they are technically demanding procedures. In major LLR, the operation time was longer,28,29 and the conversion rate was high, >10%.29,30 Although there are a few reports of laparoscopic anatomical monosegmentectomy, it still remains a challenging procedure.31,32 Therefore, good results in previous case-matching studies may be due to highly selected candidates for LLR. Perioperative and oncologic safety for HCC located in the posterosuperior region or requiring major resection is still controversial, and the results of these studies apply only to the selected patients, not to general HCC cases. Although our case-controlled study was well balanced and the LLR for HCC with well-compensated liver cirrhosis was feasible and safe, our study also could not overcome these limitations, as most of the cases were minor resections. Therefore, a further well-designed and prospective study is needed.
In conclusion, LLR for HCC is safe, and long-term oncologic outcomes were comparable to those of OLR in selected patients. Based on the present results, a well-designed prospective study will be needed to affirm the validity of LLR for HCC.
Footnotes
Acknowledgments
This research was supported by a research grant from an annex research institute (the Medical Genetics Institute) of Keimyung University in 2011.
Disclosure Statement
No competing financial interests exist.