
Abstract
Abstract
Purpose:
We present a procedure of suturing the transversus abdominis muscular arch to the ileopubic tract laparoscopically in order to repair recurrent unilateral pediatric inguinal hernia (PIH).
Patients and Methods:
Twenty-five children with recurrent unilateral PIH were treated during a 5-year period in a tertiary academic center. All cases were subjected to laparoscopic hernia repair and discharged the next morning. Sutures were placed from the muscular arch to the ileopubic tract, avoiding the spermatic vessels and duct, in an interrupted manner using 2/0–3/0 polypropylene (Prolene®; Ethicon, Somerville, NJ) or polyglactin 910 (Vicryl®; Ethicon) sutures. In 4 cases, a rectangular purse-string–like suture was added to narrow the internal ring defect. Operative findings and postoperative results and complications were assessed. The patients were followed up for a period that ranged between 6 and 60 months.
Results:
There were 23 boys and 2 girls. Operative age ranged between 18 months and 15 years. Three or four sutures were placed in each case. In 4 cases, an additional rectangular purse-string–like suture was added. Operative time ranged between 35 and 70 minutes, and there was no conversion. Mild scrotal edema was reported in 4 cases and port-site infection in 2 cases; all cases were treated conservatively. One case of recurrence among boys was reported, but there was no case of testicular atrophy. Cosmetic outcomes were excellent.
Conclusions:
Laparoscopic interrupted muscular arch repair is a feasible and safe technique in the reconstruction of the inguinal canal in recurrent unilateral PIH. Larger studies and long-term follow-up are needed to support our encouraging results.
Introduction
L
The advantages of the laparoscopic approach include the following: a procedure that clarifies the diagnosis and treats both sides in one session; any open contralateral patent processus vaginalis (CPPV) can be detected during laparoscopy and closed immediately; the trocar position is the same for both sides; the cord structures have excellent visualization; and they can be guarded well during the procedure. Rare forms of hernia such as direct, femoral, or combined hernias are easily diagnosed and identified. Also, a negative diagnosis, or absent hernia, is more easily documented. In cases of recurrent hernia, recurrences are easy to identify laparoscopically, the cord structures remain untouched, and this avoids the risk of ischemic damage to the testis or injury to the vas, especially when dissecting in scar tissue. Operating time and recurrence rate are comparable with those of the open procedure, and cosmesis is excellent; there are nearly invisible scars.7,8 This lends the laparoscopic technique to the repair of any recurrence, whether from previous open or laparoscopic surgery.1,7,12,14,15
Many laparoscopic techniques have been used in PIH, including purse-string closure at the level of the internal ring 7 or with adding a lateral peritoneal incision to reduce mechanical tension to the suture, 16 assisted laparoscopic ligation of the internal ring like subcutaneous endoscopically assisted ligation, 17 use of the Reverdin needle,9,18 sac resection only, 10 or sac disconnection and internal ring purse-string closure.19,20 Herniotomy is not suitable for a large PIH with a wide internal ring.20–22
The causes of recurrence include the presence of an undetected direct hernia, failure to ligate the hernia sac high enough at the internal inguinal ring, tension at the closure of the internal opening, a large hernia, a broken purse-string thread, and the presence of skip areas, especially over the vas and spermatic vessels.1,11–13 The descriptive laparoscopic anatomy of this area reveals the "dangerous eye," which is the area formed by the transversus arch and the ileopubic tract and which surrounds the deep inguinal ring. 23 Passing from origin to insertion, the transversus arches over the external iliac vessels to insert onto the pectineal ligament. Those fibers that form the arching, muscular lower border of the transversus abdominis arch over the position of the deep inguinal ring. The transversus abdominis arch is a useful entity for the repair of inguinal hernia.23,24 The ileopubic tract is an aponeurotic band that extends laterally to the iliacus and psoas fascia up to the anterior superior iliac spine and passes medially to form the lower border of the internal ring and the anterior margin of the femoral sheath to end at the pectineal ligament. 25 It consists of more than aponeurotic fibers of the transverses abdominis and transversalis fascia; extraperitoneal connective tissue also contributes to the formation of the ileopubic tract, increasing the brightness of light reflection from the laparoscope.23–26 The principle of open suturing the musculoaponeurotic arch to the ileopubic tract is used in the repair of a groin hernia among adults using mesh as an ileopubic repair.27,28
The aim of this work is to present a procedure of suturing the transversus abdominis musculoaponeurotic arch to the ileopubic tract laparoscopically in children in order to repair recurrent unilateral inguinal hernia as a novel approach.
Patients and Methods
Twenty-five consecutive children with recurrent unilateral PIH who presented to the Department of Pediatric Surgery, Tanta University Hospital, Tanta, Egypt, over a 5-year period (from December 2008 until November 2013) were included in this study. The ethical research committee of our institution approved the study design. A detailed informed consent was obtained from each patient's guardian.
Exclusion criteria included nonrecurrent hernia, irreducible bilateral hernia cases as a primary diagnosis, and bilateral recurrent inguinal hernia.
No special preoperative measures were required for laparoscopic hernia repair in children. All patients received general anesthesia with endotracheal intubation or a laryngeal mask. In all patients, we had adopted the open technique to establish pneumoperitoneum. Intraabdominal gas pressure ranging from 8 to 12 mm Hg has been found to be sufficient for the procedure using a 5-mm 30° scope. All cases were subjected to laparoscopic exploration first, followed by laparoscopic hernia repair, and were discharged the next morning by the same group. The diagnostic exploratory laparoscopy was first done, with both inguinal regions being inspected from within the abdomen to confirm the clinical preoperative diagnosis and to detect any CPPV or other rare defects as described earlier by our group.12,21 Cases that showed nontouch of the hernia sac with a small internal ring diameter around 2–3 cm were treated laparoscopically by purse-string suture after sac disconnection; these represented another study and were excluded from the current study because herniotomy alone with sac removal only is not suitable for wide defects.19–21 If the diameter of CPPV is less than 5 mm or the length is less than 1 cm, no intervention is done as it is considered laparoscopically negative for CPPV. 12
After circumferential sac disconnection, as seen in Figure 1a–d, sutures were placed from the transversus musculoaponeurotic arch to the ileopubic tract in an oblique manner away from the triangle of doom, avoiding the spermatic vessels and duct by interrupted sutures using 3/0 or 2/0 polypropylene (Prolene®; Ethicon, Somerville, NJ) or polyglactin 910 (Vicryl®; Ethicon) sutures according to age and space, as seen in Figure 1e–h. The first suture should be passed lateral to the gonadal and iliac vessels. The knot is tied either intracorporeally or extracorporeally, according to the surgeon's preference. In some cases, when the medial gap of the defect is wider than the 5-mm instrument passing lateral to the vas, a purse-string–like suture is added in a rectangular manner to narrow the defect at the internal ring area provided that the tip of the 5-mm instrument is passable after knotting. The needle is removed transabdominally as introduced. There is no need to approximate the peritoneum in most cases as this could tear during knot-tying. This allows the peritoneal scar tissue to close the gapped area. Air tightness is assessed at the end of the repair by inspecting the scrotum without decreasing the pneumoperitoneum pressure or by external abdominal indentation. Patients are transferred to their wards and receive medical treatment in the form of the second dose of intravenous first-generation cephalosporin, with the first one having been given at the time of induction, and a nonsteroidal anti-inflammatory suppository was used for postoperative analgesia during the first 48 hours following the procedure as needed. Oral fluids were started when bowel sounds were audible. All patients were discharged the next morning.
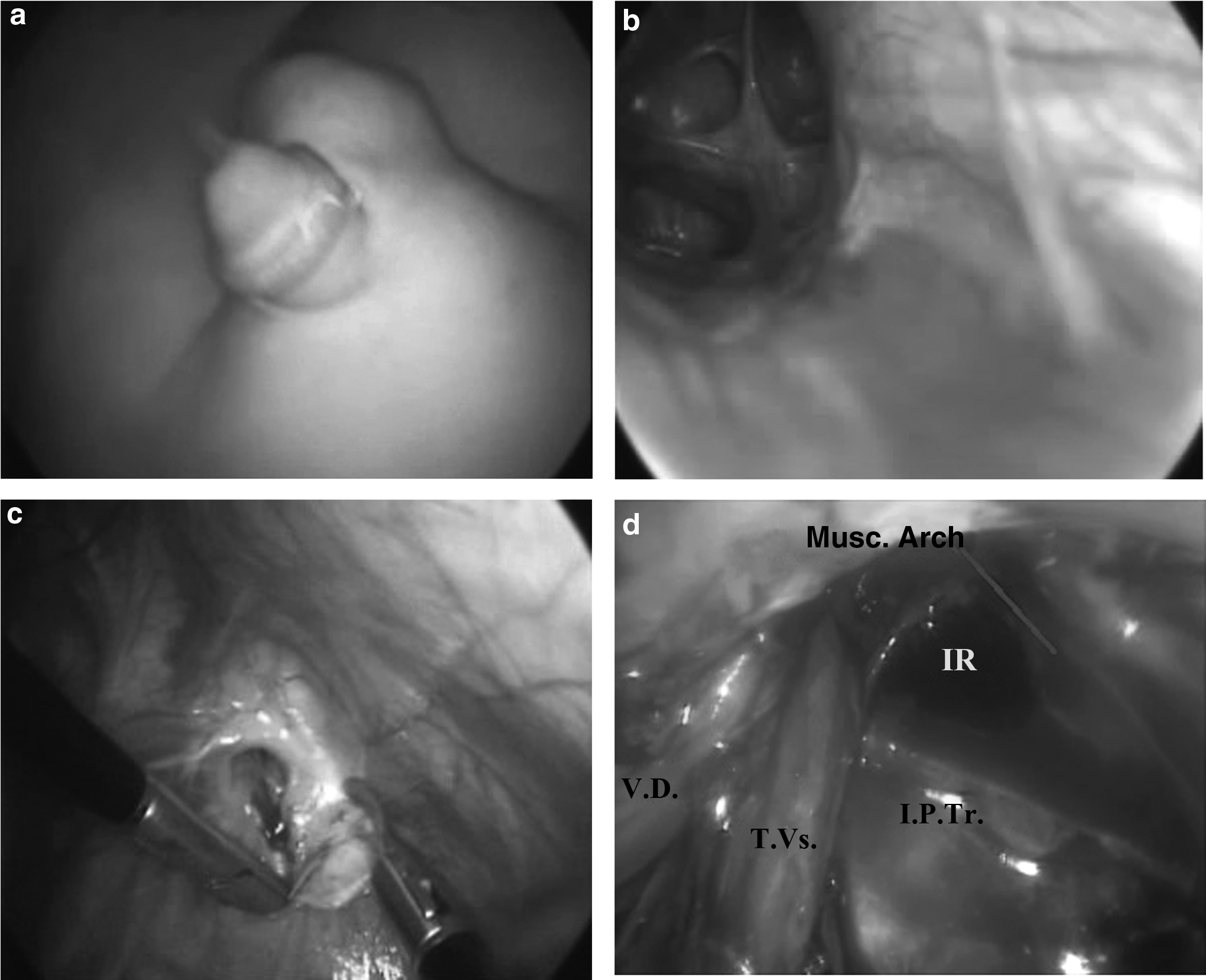
Operative photographs for two cases of right pediatric inguinal hernia. Case A:
Operative findings and postoperative results and complications were assessed and reported during the follow-up period, which ranged between 6 and 60 months with a mean of 24.2 months. Follow-up protocol included outpatient visits at 1 week and 1, 3, and 6 months postoperatively and then by phone call every 6 months thereafter until 3 years, and an outpatient clinic visit was arranged when needed.
Results
Twenty-five cases presenting with unilateral recurrent PIH are included in this study.
Operative age ranged between 18 months and 15 years, with a mean of 51 months, at the time of surgery. Our study included 23 boys and 2 girls, with 12 cases presenting in the first year after a previous repair. The former repair was by the open technique in 22 cases and by laparoscopy in 3 cases. Thirteen cases presented with right-sided recurrent PIH with no case associated with CPPV on laparoscopic exploration, compared with 12 left-sided cases with one associated CPPV on laparoscopic exploration. This contralateral side was managed by laparoscopic herniotomy and excluded from the study group as the diameter of the internal ring was around 1 cm.
Thus, the total number of recurrent hernias subjected to this technique was 25 cases following exploration, where three to four sutures were placed in each case. In 4 cases, an additional rectangular purse-string–like suture was added to narrow the internal ring defect medially as described in Patients and Methods. Three cases showed some adhesions, being omentum in two occasions, which were cleaved laparoscopically. Operative time ranged between 35 and 70 minutes in the studied cases, with a mean of 51.1 minutes. All operations were completed laparoscopically without conversion. No intraoperative complications in the form of vas or vessel injury were reported.
Postoperative pain lasted for a period that ranged between 6 and 24 hours (mean, 13.9 hours) according to analgesic need. Two cases developed wound infection in the umbilical port site and were treated conservatively. Mild scrotal edema was reported in 4 boys that subsided in the first postoperative week under conservative treatment. One case of recurrence among boys was reported 3 months postoperatively, and no case of testicular atrophy or hydrocele was reported in the follow-up period. Cosmetic outcomes were excellent.
Twenty of the 25 patients complied with the clinical 1-year follow-up (80%) without sequelae except the single case of recurrence (4%).
Discussion
Inguinal hernia repair is one of the most frequently performed operative procedures in children. The traditional surgical approach requires an open revision of the inguinal canal and dissection of the hernia sac from the spermatic cord. 25 However, the open approach does have associated disadvantages as well, including inability to evaluate the contralateral internal ring and a reported recurrence rate of 1%–3%.1,5,6 Furthermore, the open repair can be challenging in certain cases such as recurrent hernias, incarceration, hernias in premature infants, and obese adolescent patients. Hence, recurrent hernia is one of the justifications to use laparoscopy.18,26
Patkowski et al. 29 reported three recurrences among their series, where hernia recurrence in their series was noted only in boys older than 1.5 years. The main cause of recurrence in PIH is the remaining preformed sac in open cases.30,31 This holds true with many transcutaneous techniques where the medial part of the peritoneum overlying the vas and vessels is left without repair as reported.29,32,33 This transcutaneous closure with intact peritoneum was the technique used in two out of the three recurrences in our present series after laparoscopic hernia. Even more in older boys, recurrences are increased following laparoscopy, as the retained area of peritoneal sac is large or the suture material gave away with an intact preformed sac as reported in an experimental rabbit model 34 and humans. 35 Kelly et al. 34 proved that by suture removal, 60% of the Vicryl ligations had failed significantly, and no Vicryl suture material was identified during necropsies in their experimental work.
Ponsky et al. 31 reported that there is no argument against the fact that the laparoscopic technique grants the unequivocal opportunity for the surgeon to directly visualize the internal inguinal ring without dissection of the abdominal wall. A very important factor for durability of inguinal hernia repair likely involves some component of trauma to the peritoneum. This certainly occurs during the open repair, where the sac is transected after ligation. In fact, it has been reported that the actual sac ligation may not be needed during repair, rather, just the sac transection. 36 However, based on the available literature, it appears that the laparoscopic approach to inguinal hernia repair in children is safe and effective with recurrence rates comparable to those for the open repair in primary cases.37,38
In our opinion, to repair recurrent inguinal hernia we need a sound technique to achieve good outcome. To our knowledge, the laparoscopic suturing of the transversus abdominis musculoaponeurotic arch to the ileopubic tract in order to repair recurrent unilateral inguinal hernia in children has not been described before. It was described previously in adult open groin hernia mesh repair with efficient results.27,28 Our hypothesis is that in recurrent hernia, usually the ring is large and age is older, so simple closure without disconnection is unfair when compared with the open technique. Chan et al. 11 and our group 22 concluded that some additional repair can avoid this problem in large hernias to minimize recurrences, especially when there is tension at the closure of the internal ring. To strengthen the wide or weak defect in recurrent cases, use the laparoscopic suturing of the transversus abdominis musculoaponeurotic arch to the ileopubic tract in order to repair a recurrent unilateral inguinal hernia in a child to overcome the above-mentioned problem as a novel laparoscopic approach. This is not needed in smaller defects, as hernia sac dissection is enough with very low recurrence as reported by Shehata et al. 21 and Boo et al. 39 Our technical point of sac disconnection with interrupted muscular arch sutures is to create a strong repair with muscle support. To validate the technique, we have to follow the golden steps of open repair here in the laparoscopic repair by complete sac disconnection and muscle repair as proved in large hernias or recurrent cases as indicated in former studies by our group.20–22 Hence our technique provided the solution for large defects as it adds muscle support. 22 Also, at the same time the basic step in the gold standard open hernia repair of sac excision is used here in the form of complete sac disconnection.10,22,36
Most laparoscopic reports present hernias with a small internal ring compared with recurrent cases with larger defect size due to a wide ring or older age.30,35,40 In accordance with this, we highlight the problem of large and recurrent defects considering that recurrence in the pediatric age group is very low, ranging between 0.7% and 1.8%1,29,41; hence the number of patients in this study is considerable. Technically, care should be taken to apply sutures lateral to the vascular structures at the triangle of doom, and this is achieved by scope magnification as an advantage of laparoscopy, plus the experience of surgeons to alleviate the worries of injuries to the posterior wall of the canal in former reports.25,29 This is feasible with experience without the need of hydrodissection as reported earlier.13,29,35,42
We reported a mean pain duration of 13.9 hours. This is comparable to a former report of mean postoperative pain of 11.2 hours with herniotomy alone without muscular sutures. 21 Because there are no extra doses of analgesics needed compared with our former protocol or more pain duration, we can prove no extra pain than other types of repair. Minor complications are treated conservatively as scrotal edema or port-site infection. We reported 1 case of recurrence (4%) among this group of recurrent cases in a mean follow-up period of 2 years, which is comparable to other reports, 1 considering that we include large hernias and recurrent cases. This may be attributed to suture failure or a large defect that is planned for open mesh hernioplasty. Treef and Schier 15 reported comparable results of a 3% recurrence rate of 32 children out of 1071 cases, even though they included mainly smaller ring sizes. They reported medial or lateral recurrence to the single suture they were using or suture breakdown; hence we can provide an answer to minimize recurrence by complete sac disconnection and multiple interrupted muscular arch repair as we described to overcome the remains of the sac, large defects, and weak muscle, as well as suture breakdown, as predisposing causes of recurrence as reported earlier.15,29,32–35
Conclusions
To our knowledge, this is the first report using the muscular arch repair by suturing the transversus abdominis musculoaponeurotic arch to the ileopubic tract in an interrupted manner to treat recurrent PIH laparoscopically. This procedure is helpful in the functional reconstruction of the inguinal canal in recurrent cases of unilateral PIH. Laparoscopic inguinal herniorraphy by this technique is feasible and safe. Consequently, there is a lower risk of injury to the spermatic duct or vessels than with the conventional herniorraphy by working in a virgin area with the use of scope magnification. Larger studies and long-term follow-up are needed to support our initial encouraging results.
Footnotes
Disclosure Statement
No competing financial interests exist.