
Abstract
Abstract
Introduction:
Despite appendicitis being one of the most common surgical emergencies in the pediatric population, there is still a great deal of debate among pediatric surgeons regarding the workup and treatment.
Materials and Methods:
In an interactive Web symposium consisting of 130 pediatric surgeons from various regions of the world, questions about diagnosis and management of appendicitis were displayed on the screen. The audience was asked to respond to the poll questions. The questions asked to the participants pertained to an example case of a 12-year-old boy presenting to the emergency department with the classic history and exam for appendicitis.
Results:
The total number of respondents varied between 30 and 37, giving response rates of 23%–28%. Sixty-six percent of respondents would not order imaging. Thirty-one percent said that they would order ultrasound. No participant would order a computed tomography scan, whereas 5% would order some other form. Ninety-five percent of respondents said that they would treat the patient operatively. The majority (89%) of the participants felt comfortable waiting until morning to operate on the patient if the patient arrived at 11 p.m. Fifty-seven percent stated that they would use a three-port laparoscopic approach, and 38% would use a single port, whereas 5% would use an open surgical approach. The majority (34%) reported being able to visualize the appendix as the greatest benefit to using laparoscopy. Fifty-seven percent would give the patient one additional dose of antibiotics and then discharge him 24 hours later following treatment for acute, nonperforated appendicitis. Twenty percent of respondents would give no further antibiotics and would discharge the patient from the recovery room or soon after. Sixteen percent would not give any additional antibiotics and would discharge him 24 hours postoperatively, whereas 6% would give one additional dose of antibiotics and discharge him soon after.
Conclusions:
The use of virtual broadcasts affords a unique opportunity to surgeons around the world to share and learn from each other.
Introduction
A
With this broad base of treatment options and the controversy that follows, surgeons often look to what their colleagues are doing to help guide their decision processes. To accurately poll pediatric surgeons regarding their practice patterns, the cohort of surgeons should represent a wide geographic sampling rather than one location. To bring physicians from around the world together to contrast and compare the pros and cons of these various techniques is challenging. However, the advancement of Internet technologies has provided many opportunities for surgeons to quickly share ideas with their colleagues from all over the world. 2
The introduction of virtual broadcasts has helped to create a forum where surgeons from all across the world can come together to discuss controversial topics such as this one, without having to meet in one physical location. Physicians can now compare their techniques for diagnosis and management of various illness such as appendicitis in a way that provides opportunity for instant feedback, all while never leaving their own office. Here we take advantage of this unique forum to assess practice patterns relating to appendicitis from many geographic locations.
Materials and Methods
An interactive Web symposium was held by GlobalcastMD, which is an online platform that broadcasts internationally and allows viewers to interact with other physicians and presenters from around the world. During a broadcast in September 2013 discussing controversial topics such as the diagnosis and treatment of appendicitis, a survey was conducted by asking audience members to respond to a single response question that appeared on their computer screen at various intervals throughout the session.
Questions
Questions asked to the participants revolved around an example case of a 12-year-old boy presenting to the emergency department with the classic history and exam for appendicitis. Participants were then polled using single-response questions that periodically popped up on the viewer's screen throughout the session, asking them to provide a response. Participation in the polls was not a required portion of the session, so viewers were able to decline to respond without consequence. Responses were recorded and displayed back to the participants of the session in order to drive further conversation of the topic. Questions asked of the participants and total number of responses are displayed in Table 1.
CT, computed tomography.
Results
During the interactive online session 130 pediatric surgeons from around the world were polled to find their opinion on various aspects of the diagnosis and management of appendicitis in the pediatric population. The number of responses for each question varied from 30 to 37 responses, which gave response rates of 23%–28%. The questions were provided in response to clinical scenarios that were proposed, and the participants' responses were used to drive the conversation on the topic of appendicitis. A case of a 12-year-old boy presenting with the classic history and exam for appendicitis was presented.
Would you order imaging?
Figure 1 shows the results of whether or not participants would order imaging for this particular case. Sixty-six percent of respondents said that they would not do imaging. However, 31% said that they would do ultrasound. No participants said that they would order a computed tomography scan, and 5% stated that they would do some other form.
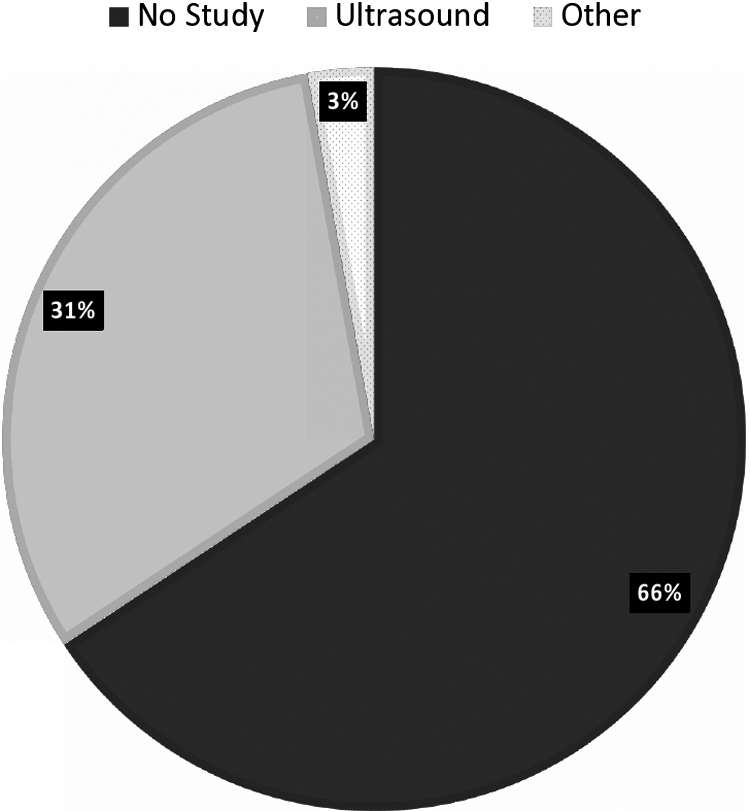
Would you order imaging? (n=35).
Treat nonoperatively
Ninety-five percent of respondents said that they would treat this patient operatively. However, 5% stated that they would treat this patient nonoperatively. These results are shown in Figure 2.
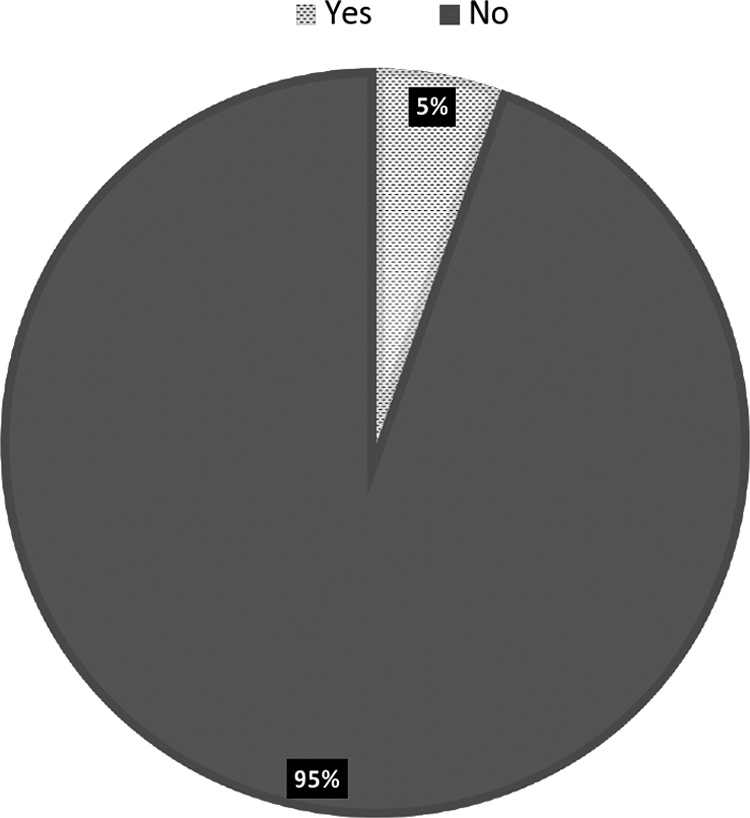
Would you manage nonoperatively? (n=37).
How would you manage at 11 p.m.?
In terms of urgency of treatment, Figure 3 shows that 89% of participants would feel comfortable waiting until morning to operate on this patient. Elven percent of participants, however, said that they would operate immediately.
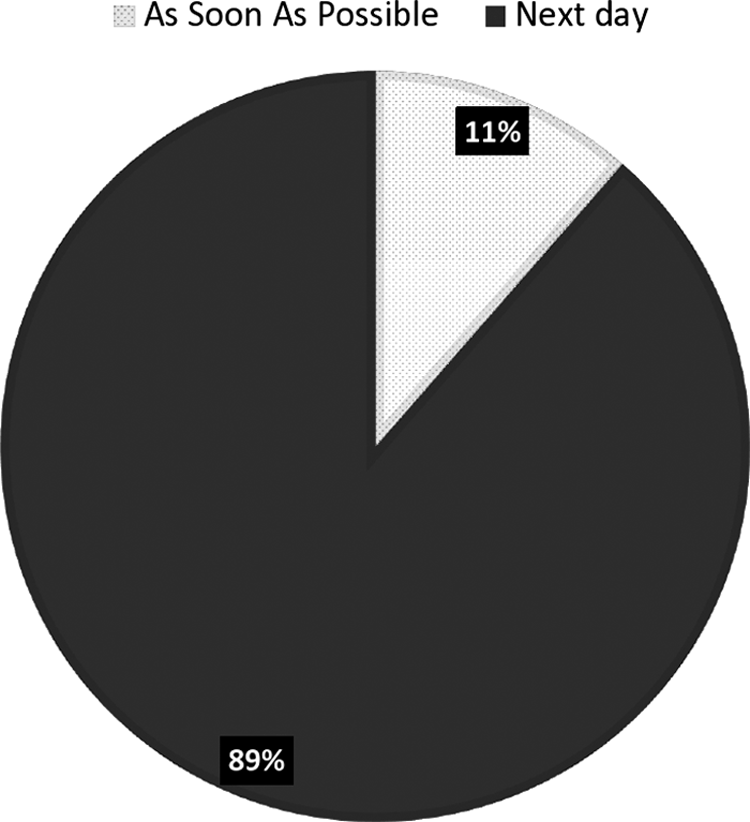
How would you manage a patient presenting at 11 p.m.? (n=35).
What surgical approach would you use?
Discussing the various techniques for appendectomy, Figure 4 shows that 57% of respondents stated that they would use a three-port laparoscopic approach for treating this patient. Thirty-eight percent of those surveyed said they would use a single port with incision through the umbilicus, whereas 5% said that they would use an open surgical approach.
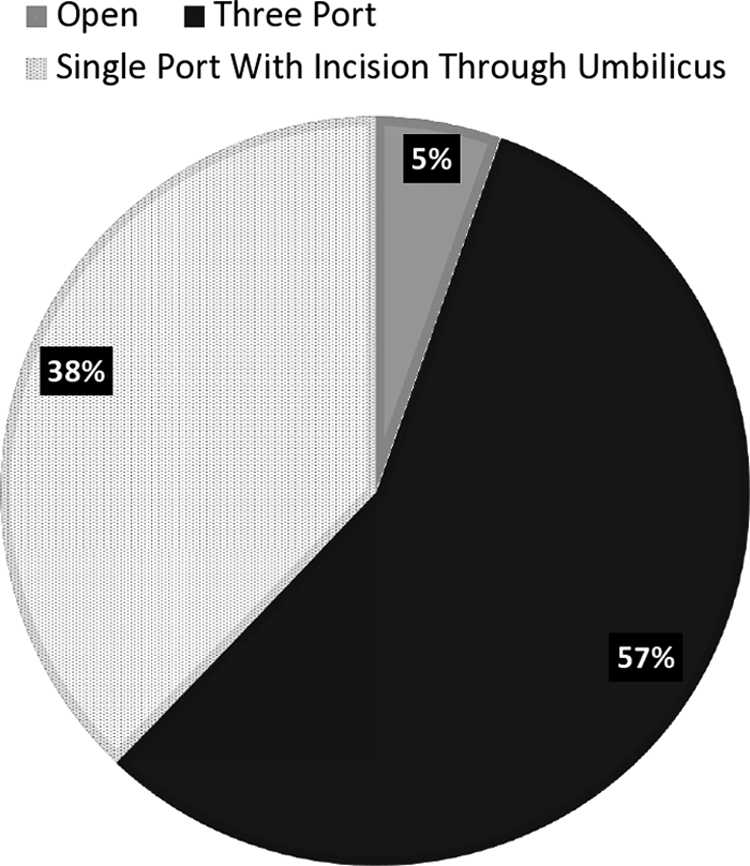
What surgical approach would you use? (n=37).
Benefits of laparoscopic procedure
Figure 5 shows what participants felt were the greatest benefits to using a laparoscopic procedure. The majority of participants (34%) said they could see the appendix wherever it was. Nineteen percent of participants said the biggest benefit was that it was faster in most cases, whereas 16% of respondents agreed that the decreased incidence of small bowel obstruction and cosmesis were the biggest benefits, and 15% stated decreased wound infection as the largest benefit to the laparoscopic procedure.
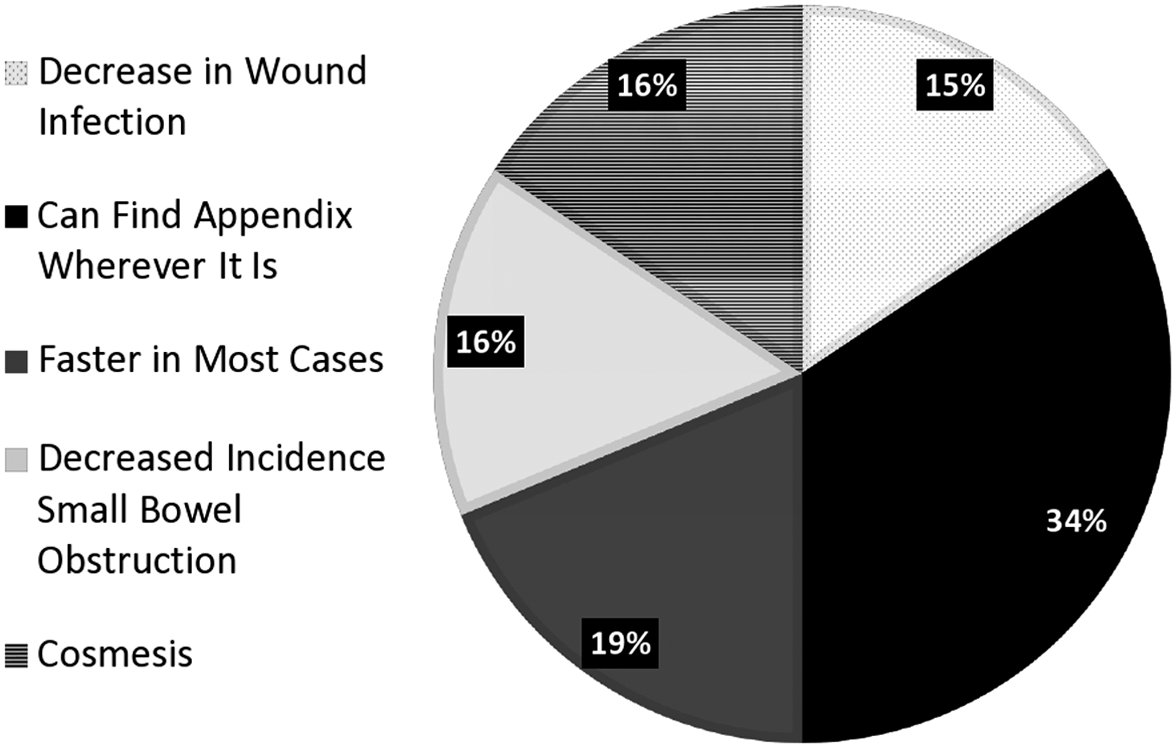
The biggest advantage to the laparoscopic procedure (n=32).
Postoperative antibiotics
Fifty-seven percent of respondents stated that they would give the patient one additional dose of antibiotics and then discharge hi 24 hours later following treatment for acute, nonperforated appendicitis. Twenty percent of participants said that they would give no further antibiotics and would discharge the patient from the recovery room or soon after. Also, 16% of participants said they would not give any additional antibiotics and would discharge him 24 hours postoperatively, and 6% said that they would give one additional dose of antibiotics and discharge him soon after. These results are illustrated in Figure 6.

How many doses of postoperative antibiotics (antibx)? (n=30).
Return to full activity
In Figure 7 it is shown that 33% of participants would allow the patient to return to full activity 2 weeks following surgery. Twenty percent said that they would allow it after 1 week. Seventeen percent of respondents said that they would allow the patient to return to full activity either in 3 or 4 weeks, and 13% said it would be okay whenever the patient desired.
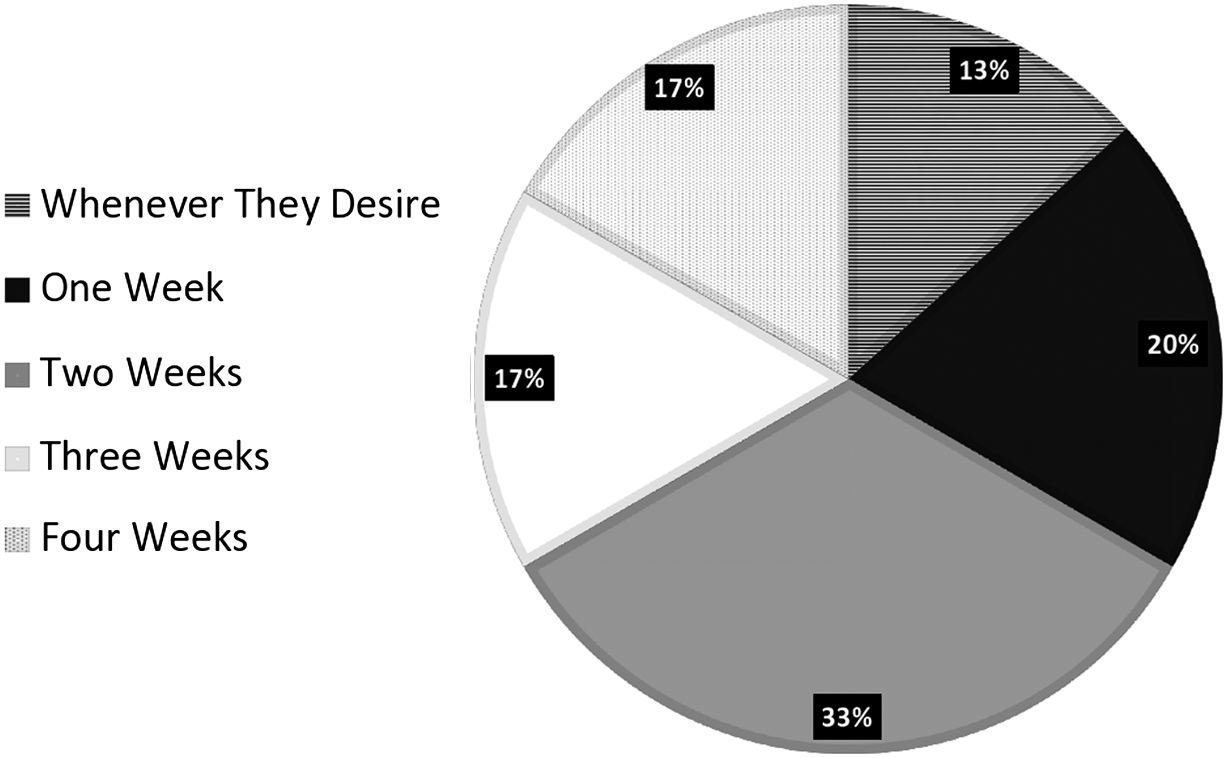
When can the patient return to full activity? (n=30).
Discussion
Appendicitis is one of the most common conditions requiring urgent treatment among the pediatric population. 1 Despite this fact, there is no consensus among physicians as to the proper way to diagnose, treat, and manage appendicitis. Because of this, there is wide variability in practice. Although there is a vast pool of literature relating to the management of appendicitis, data are often conflicting. For example, a study by Di Cesare et al. 1 concluded that clinical assessment should be the primary tool used to diagnose appendicitis and that only in inconclusive cases is imaging necessary. However, Poortman et al. 3 performed a study in which all potential appendicitis patients underwent imaging and found it to be very effective.
There are several surgical methods used to treat appendicitis. A Cochrane study that compared laparoscopic with open appendectomy concluded the laparoscopic technique to be superior, although the investigators admitted that some of these benefits are of little clinical significance. 4 There is also controversy in whether to treat operatively or not. In a study by Armstrong et al., 5 10 out of 12 patients were successful in two treatment groups either receiving surgery or not. On the other hand, a study compared nonoperative antibiotic therapy with surgical appendectomy and found that although nonoperative treatment was associated with fewer complications, it is not as effective because of the high recurrence rate. 6 Timing of the operation is also a controversial topic. A study by Yardeni et al. 7 found that delaying appendectomy did not affect operating time, perforation rate, or complications. However, Ditillo et al. 8 concluded in their study that delaying appendectomy increases the development of advanced pathology as well as postoperative complications.
Because of the conflicting literature and views in treatment and management of appendicitis, many physicians often turn to their colleagues to identify an appropriate course of action. Web-based symposiums, such as GlobalCastMD, allow for physicians to come together virtually to review various treatment preferences with colleagues from around the world. The results of the polls in this study showed the variance in practice pertaining to treatment of appendicitis. The bringing-together of these ideas can allow for physicians to justify their preference based on a majority from across the world or, if desired, to adjust their treatment methods. Conducting similar symposiums on other controversial topics would allow for physicians to communicate in a way that could lead to a more unified approach to the treatment of several highly debated conditions. Given that our study is limited in the number of respondents per question, further studies could be conducted to identify how often forums such as this lead to a change in practice style by physicians.
Conclusions
Although appendicitis is commonly seen among the pediatric population, workup and treatment of the condition are highly varied among physicians around the world. The use of online symposiums is an effective way to bring physicians together to discuss the various methods that they prefer to treat the condition. Virtual broadcasting can be used in the future to allow physicians from across the globe to share their thoughts and practice strategies about any condition or disease with the aims of improving medical treatment for patients everywhere.
Footnotes
Disclosure Statement
T.A.P. is an owner of GlobalcastMD.