
Abstract
Abstract
Purpose:
Robot-assisted radical cystectomy (RARC) was first introduced in 2003. Although there have been modifications to the surgical techniques over the years, in every published RARC series the surgical robot is invariably docked between the patient's legs. We evaluated the use of a side-docking approach in RARC.
Patients and Methods:
Ten RARCs using a side-docking technique were performed at a single institute between February 2013 and February 2014. The patients' clinical notes and operative findings were reviewed. The results were compared with results from RARCs using the conventional central-docking method from our historical cohort.
Results:
There were no significant arm collisions in the side-docking RARC procedures. The perineum was readily accessible in all cases that used the side-docking method. A simultaneous urethrectomy was performed in 1 case with a side-docking approach. The median operative times were 417.5 minutes (range, 345–515 minutes) and 405.0 minutes (range, 330–500 minutes) in the central-docking and side-docking groups, respectively. There were no statistically significant differences in operation time, transfusion rate, complication rate, or hospital stay between the two groups.
Conclusions:
A side-docking approach in RARC provides better perineal access with the advantage of allowing simultaneous urethrectomy and transvaginal retrieval of the specimen without compromising the dexterity and precision of the robotic surgical system.
Introduction
R
Patients and Methods
Patient characteristics
Between February 2013 and February 2014, 10 consecutive patients underwent RARC for bladder cancer. Informed consent was obtained before the procedures. The four-arm robotic surgical system (da Vinci S) was used in all of the cases.
Surgical technique
The patient is placed in a steep Trendelenburg in low lithotomy position. Excessive abduction of the legs is avoided. Six trocars are used (Fig. 1). The camera port is inserted 3 cm above the umbilicus. Two 8-mm robot ports are located 8 cm away from the camera port at the umbilical level. One additional 8-mm robot port is inserted over the right lower quadrant 3 cm above and medial to the anterior superior iliac spine. A 12-mm assistant port is placed over the left lower quadrant to facilitate the insertion of needles and laparoscopic staplers. Another 5-mm assistant port is placed over the upper abdomen between the camera port and left robot arm. The patient cart is docked to the right side of the patient at a slight angle (<20°) to the long axis of the patient (Fig. 2). The robotic arms are docked starting from arm #3 on the right. The number sign of arm #3 should face medially to prevent collision between arms #3 and #2 (Fig. 2). The docking of the robot arms continues from right to left (#2→camera→#1). The alignment of the “sweet spot” on the camera arm may not be necessary in some cases. Maximum spacing and adequate movement between the robot arms should be ensured after cannula stabilization. The assistant sits comfortably on the left side of the patient (Fig. 3). A second assistant may sit between the patient's legs if perineal manipulation or a simultaneous urethrectomy is required (Fig. 4).

Trocar placement. The assistant used the 12-mm trocars on the left side for the insertion of stapling devices and needles. Robot arm #3 is placed over the right lower quadrant.
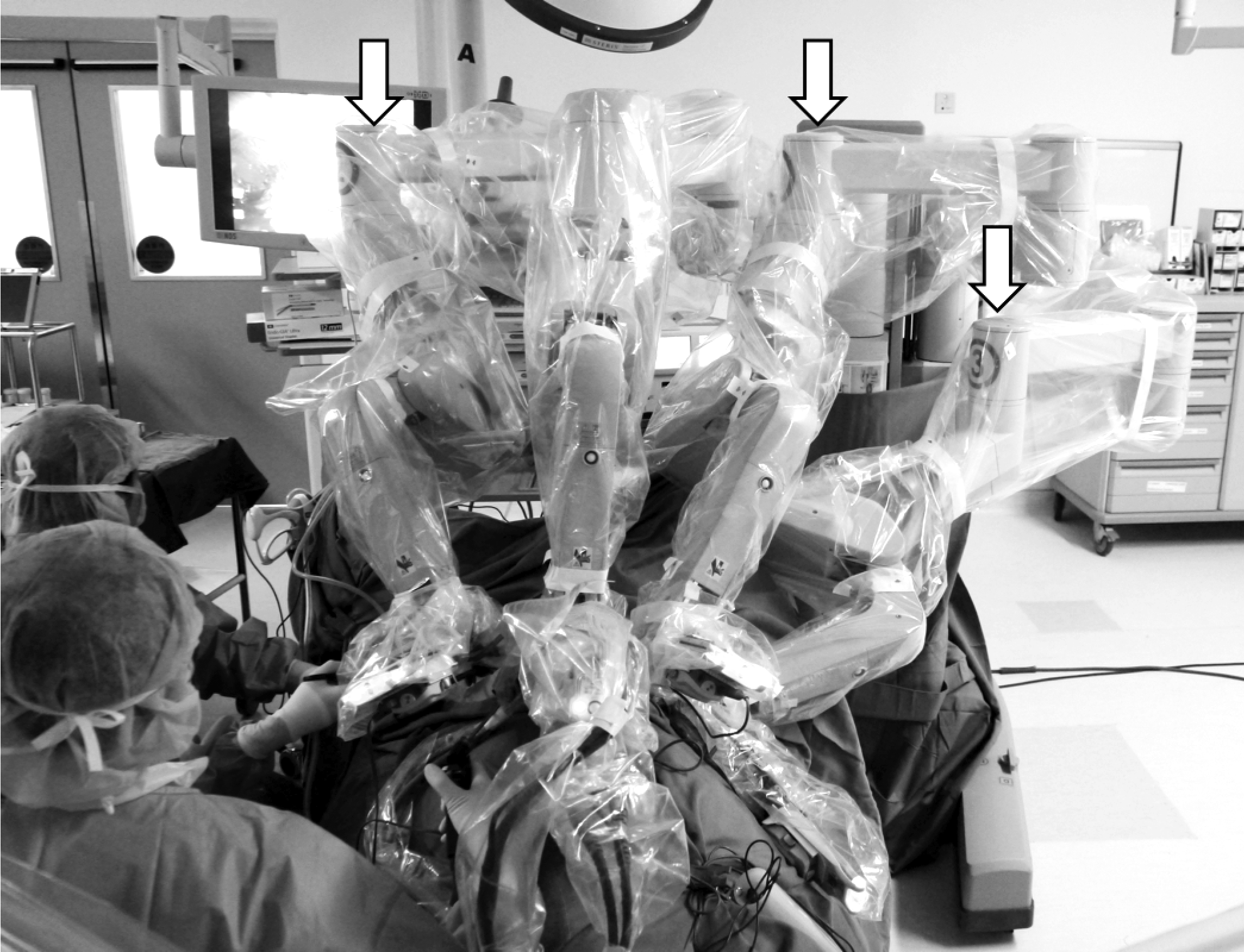
Position of robot arm #3. Note the slight angle of the central column relative to the operating table. The arrows indicate that the number signs of robot arms should face sideways as shown.

The operating theater setting. The patient's head is on the right.

Simultaneous radical cystectomy and urethrectomy.
RARC is then performed as described by Guru et al. 3 A bilateral extended pelvic lymphadenectomy is performed after the completion of radical cystectomy. The caudal placement of the camera and working ports facilitates the dissection of lymph node up to aortic bifurcations. 4 Urinary diversion can be performed either extracorporeally through a small incision or totally intracorporeally. Arm #3 is used for bowel retraction and manipulation, and there is no limitation on its movement. This is essential especially for intracorporeal ileal conduit or neobladder reconstruction. The transection of the ileum and small bowel anastomosis are completed with 60-mm laparoscopic staplers via the 12-mm assistant port on the left.
Statistical analysis
Descriptive statistics were used to characterize the demographics. The data comparisons were performed using the Mann–Whitney U test for continuous variables and Fisher's exact test for categorical variables. P<.05 was considered statistically significant. The SPSS software package (version 20.0; SPSS, Inc., Chicago, IL) was used for all of the calculations.
Results
Between February 2013 and February 2014, 10 consecutive patients underwent a side-docking RARC. The results were compared with our historical cohort of 10 patients who had undergone RARC using the conventional central-docking approach between November 2011 and January 2013. The demographic data of both groups are shown in Table 1. One case in the side-docking group and 1 case in the central-docking group needed open conversion because of dense adhesion due to a previous nephrouretectomy and clinical stage T4 disease, respectively. There was one orthotopic neobladder in each group, and both operations were performed through a mini-laparotomy wound.
No significant collision between robot arms was observed in either the central- or side-docking groups. The median operative time was 417.5 minutes (range, 345–515 minutes) and 405.0 minutes (range, 330–500 minutes) for the central-docking and side-docking techniques, respectively (Table 2). Two cases in the central-docking and 5 cases in the side-docking groups had total intracorporeal ileal conduit reconstruction. One patient in the side-docking group had a simultaneous urethrectomy at the time of radical cystectomy (Fig. 4). There were 5 (50%) patients in the central-docking group and 3 (30%) patients in the side-docking group who required transfusions. There were no statistically significant differences in operation time, transfusion rate, and length of hospital stay between the two groups. There was one major complication (Clavien Grade III) in the side-docking group due to adhesive intestinal obstruction within 3 months after radical cystectomy. No major complication was observed in the central-docking group. Skin, nerve, and musculoskeletal injuries were not observed in either group.
SD, standard deviation.
Discussion
Laparoscopic radical cystectomy and RARC have become popular in recent years. The advantages of such minimally invasive approaches include less blood loss, a lower transfusion rate, early recovery of bowel function, reduced use of analgesic, and a short hospital stay.4–7 The short-term and long-term oncological outcomes are comparable with those of ORC. With enhanced freedom of movement, a robotic surgical system makes intracorporeal reconstruction possible. Ease of suturing and an excellent view of the surgical field are the main advantages of RARC over the conventional laparoscopic approach. The technique of RARC has been well described in the literature.2,3,8 Patients are positioned in low lithotomy, with the robot cart placed between the patients' legs. However, in this configuration the central column of the robot restricts full access to the perineum. It makes manipulation of the vagina or rectum difficult. In the case of a urothelial tumor involving the urethra, urethrectomy can only be performed after undocking the robot before or after urinary diversion.
Side-docking techniques have been reported in robot-assisted hysterectomies and other gynecological procedures.9,10 This configuration facilitates uterine manipulation and the retrieval of specimens through the vagina. In lower anterior resection, docking the surgical robot over the side of the patient allows full access to the upper abdomen and pelvis. 11 Splenic flexure mobilization and total mesorectal excision can then be performed without the need to reposition the robot. These techniques have been recently applied to prostatectomy 12 and other urologic pelvic surgeries. 13 Uffort and Jensen 12 reported that in radical prostatectomy the side-docking technique reduced setup time and benefitted patients with limited hip abduction. The advantages are pronounced, especially in procedures involving complex reconstructions (e.g., ureteric re-implantation, bladder augmentation, and partial cystectomy). Simultaneous cystoscopy, ureteric catheterization, and uterine manipulation facilitate the procedures.
The access to the perineum is important in an RARC. Our technique allows surgeons to perform RARC with efficiency and unlimited perineal access. In the conventional central-docking method, a urethrectomy can only be performed after completion of the cystectomy and intracorporeal reconstruction. Extra operative time is needed. In the side-docking approach, a cystectomy can be performed en bloc with the urethra. Total intracorporeal reconstruction is possible without interruption, while the second assistant is closing the perineal wound. This will significantly reduce the length of the operation. In a female cystectomy with anterior exenteration, the assistant can sit comfortably between the patient's legs for the retrieval of a specimen through the vagina. The extreme abduction of the hip joints in the conventional central-docking method may potentially cause neural damage from stretching of the sciatic and obturator nerves or from compression on the femoral nerve. The smaller abduction angle used in the side-docking technique avoids over-abduction of the hips, which in turn reduces the chance of such nerve injuries, especially in patients with lower limb contracture.
Collisions between robot arms are the main concern in the side-docking technique. Before starting the procedure, the surgical team should check that each arm is set at the proper working distance and that the arms are not compressing the patient. Particular attention should be paid to setting up robot arm #3. Arm #3 should be pushed toward the column with the number sign facing the left lateral. This modified positioning avoids awkward movements of the robot arm and maximizes the range of movement. It is different from the central-docking configuration in which all of the robot arms should be extended outward with the number facing the patient's head anteriorly.
If robot arm #3 is coming from the left, the robot trocar will need to be inserted through a 15-mm assistant port over the left iliac fossa. It is alternately used by the robot for retraction and bowel transection with an endoscopic stapler. 14 We docked the robot on the right side of the patient with robot arm #3 placed on the right lower quadrant. The 12-mm assistant port was located over the left lower quadrant to facilitate passing needles and stapling the intestine without needing to swap with the robotic trocar.
Radical cystectomy is a procedure that is associated with a high perioperative complication rate. The published postoperative complication rates are as high as 70%. 15 Leow et al. 16 recently reviewed data from over 36,000 patients and reported that the major complication rates of ORC and RARC were about 17.0% and 19.8%, respectively. In our current series, the overall rate of high-grade complication was about 5%. There was one Clavien Grade III complication in the side-docking group. The complication was not directly related to the robot positioning.
The present study is limited by its small sample size. Another shortcoming of this study is the short surgical and oncologic follow-up period. Long-term complications, including ureteric stricture and intestinal obstruction, may occur in a delayed manner. A randomized controlled trial with long-term follow-up may prove the value of side-docking RARC.
Conclusions
The side-docking technique is an excellent alternative to conventional positioning in robot-assisted pelvic procedures. It may become the new standard positioning for RARC, especially in patients who need a urethrectomy or anterior exenteration. This technique is efficient and provides better access to the perineum without compromising the dexterity and precision of the robotic surgical system.
Footnotes
Disclosure Statement
No competing financial interests exist.