
Abstract
Abstract
Gallbladder polyps are most commonly treated with cholecystectomy, which is associated with various complications. For benign disease, preserving the gallbladder is preferable. Since 1994, we have been exploring percutaneous polypectomy and have recently developed an improved new technique. This study reports a new endoscopic–laparoscopic (Endolap) technique for the removal of polyps and the preservation of the gallbladder. Nine Chinese mini-pigs were used to observe mucosal regeneration. Microwaves of 50–70 mA for 9 seconds were safe, and the gallbladder mucosa of pigs recovered to nearly normal 2 weeks later. In the clinical cases, 60 patients with gallbladder polyps were studied. With the patient under general anesthesia, each polyp stem was coagulated, and then the polyp was removed. All procedures were successful at between 60 and 135 minutes. The success rate was 93.33% (56/60). A retrospective analysis was conducted to assess the recovery of gallbladder function. All patients were followed up and symptom-free, without recurrence of the polyps; 3 months after the operation, the volume and contraction of the gallbladder recovered to preoperative levels. Thus the Endolap technique is reliable for removing benign gallbladder polyps and is applicable to a wider range of clinical situations than percutaneous polypectomy.
Introduction
G
Therefore, the first step in the treatment of gallbladder polyps is precise diagnosis. Recently, it was shown that an accurate diagnosis can be obtained with multidetector computed tomography combined with high-resolution ultrasonography, 6 although endoscopic biopsy remains the standard for obtaining a precise diagnosis.
With the realization of the importance of gallbladder function, many specialists are increasingly advocating for conservation of the gallbladder in the setting of benign lesions. In 1994, we proposed that if polyps were benign and gallbladder function was well preserved, there was no absolute indication for gallbladder removal. 7 In 2004, we reported our serial cases of percutaneous endoscopic polypectomy of the gallbladder. 8 The two procedures were safe, and there was no recurrence of polyps. Moreover, the follow-up showed good preservation of gallbladder function. However, these approaches are limited to some patients. 9 With the development of laparoscopic and endoscopic techniques, we have attempted to improve the operation. Compared with previous studies, we have improved the operation to a new endoscopic–laparoscopic (Endolap) technique.
Our latest data manifested an incentivizing result and suggested that the Endolap technique was more effective for managing gallbladder polyps. Combined with sufficient preoperative assessment and evaluation of gallbladder function, we performed Endolap polypectomy in 60 patients. This article describes our technique and its reliable results.
Patients and Methods
Surgical equipment
The instruments used in this study included a flexible coaxial bipolar microwave antenna (self-made), 7 a microwave generator (Nanjing Forsea Microwave Institutes, Nanjing, China), a laparoscope (Karl Storz, Tuttlingen Germany), a soft choledochoscope (Olympus, Tokyo, Japan), and a biopsy clamp for removal of the polyps.
Animal study
The animal study was proposed by the Jiangsu Province Animal Study Committee. Nine Chinese mini-pigs (average weight, 17 kg) were used to define the adequate settings for microwave coagulation on the gallbladder mucosa and to observe mucosal regeneration.
Patients
In the Department of General Surgery, Zhongda Hospital Southeast University, Nanjing, China, 60 patients (27 male, 33 female) underwent Endolap polypectomy between 2010 and 2013. The mean age of the patients was 39.3 years (range, 21–59 years). Twenty-one patients (33.3%) complained of right upper quadrant or epigastric discomfort, such as abdominal distension, indigestion, or dull pain. The other asymptomatic patients were detected incidentally during a health check. B-ultrasound showed that 48 patients had a single polyp and that 12 patients had two or more polyps. Meanwhile, 8 patients had concomitant disease: hypertension in 3 cases, coronary heart disease in 2 cases, and chronic colitis in 3 cases. There were 12 cases in which the patients' body mass index was >35 kg/m2.
All patients were required to meet the following criteria: (1) a strong desire to preserve their gallbladder; (2) between one and three polyps; (3) thickness of the gallbladder wall less than 0.3 mm; and (4) well-preserved gallbladder function, tested by ultrasound. 10 Gallbladder volume was calculated using the following formula: gallbladder volume (mL)=0.52×length×width×height (cm). The gallbladder function was evaluated by comparing the volume variation between fasting and 90 minutes after consuming a fatty meal: contraction=(fasting volume – postprandial volume)/fasting volume×100%. A volume contraction exceeding 30% was regarded as meeting the criterion.
Operative procedures
Endolap polypectomy of the gallbladder was performed with the patient under general anesthesia. Patients were placed in the reverse Trendelenburg position, and the operating table was tilted upward to the right. After pneumoperitoneum was achieved, a 10-mm trocar was inserted through the umbilicus, and then the 30° laparoscope was introduced to inspect the peritoneal cavity adhesions and the appearance of the gallbladder. Then, a 10-mm trocar and two 5-mm trocars were placed on the right subcostal, the left subcostal, and the right midclavicular line lateral to the umbilicus, respectively (Fig. 1A). A piece of dry gauze was placed around the gallbladder. A 5-mm incision was made on the gallbladder fundus with the electronic hook, and bile was withdrawn (Fig. 1B). The gallbladder lumen was irrigated with saline; meanwhile, the soft choledochoscope was introduced to inspect the inner wall through the right subcostal trocar (Fig. 1C).

The first part of the operation procedure.
Through the soft choledochoscope, the bipolar flexible microwave thermal antenna was inserted into the gallbladder. For pedunculated polyps, the polyp stem was coagulated directly (Fig. 2A); for sessile polyps, coagulation was performed along the basement of the polyps, along with simultaneous irrigation with nephrine saline (1:1000 dilution). Then, each polyp was removed using a biopsy clamp for histological examination (Fig. 2B). The gallbladder was rinsed once again, and the choledochoscope was placed to ensure reflux from the opening site of the cystic duct. After the patency of the cystic duct, a lack of bleeding, and no residual polyps were confirmed, the incision on the gallbladder fundus was sutured using an absorbable 4/0 polyglactin 910 (Vicryl™ Plus; Ethicon, Somerville, NJ) (Fig. 2C). 11 In the first 20 patients, full-thickness closure of the incision was performed. In the latter 40 patients, we improved to close the incision with a double suture: the mucous membrane and then the muscular layer as well as the serous membrane. After no active bleeding or bile leakage was identified, the gauze was removed, and the operative field was irrigated repeatedly. No drainage was placed. The trocars were removed, and the ports were closed with stitches. The patients usually resumed eating after 24 hours of postoperative fasting.
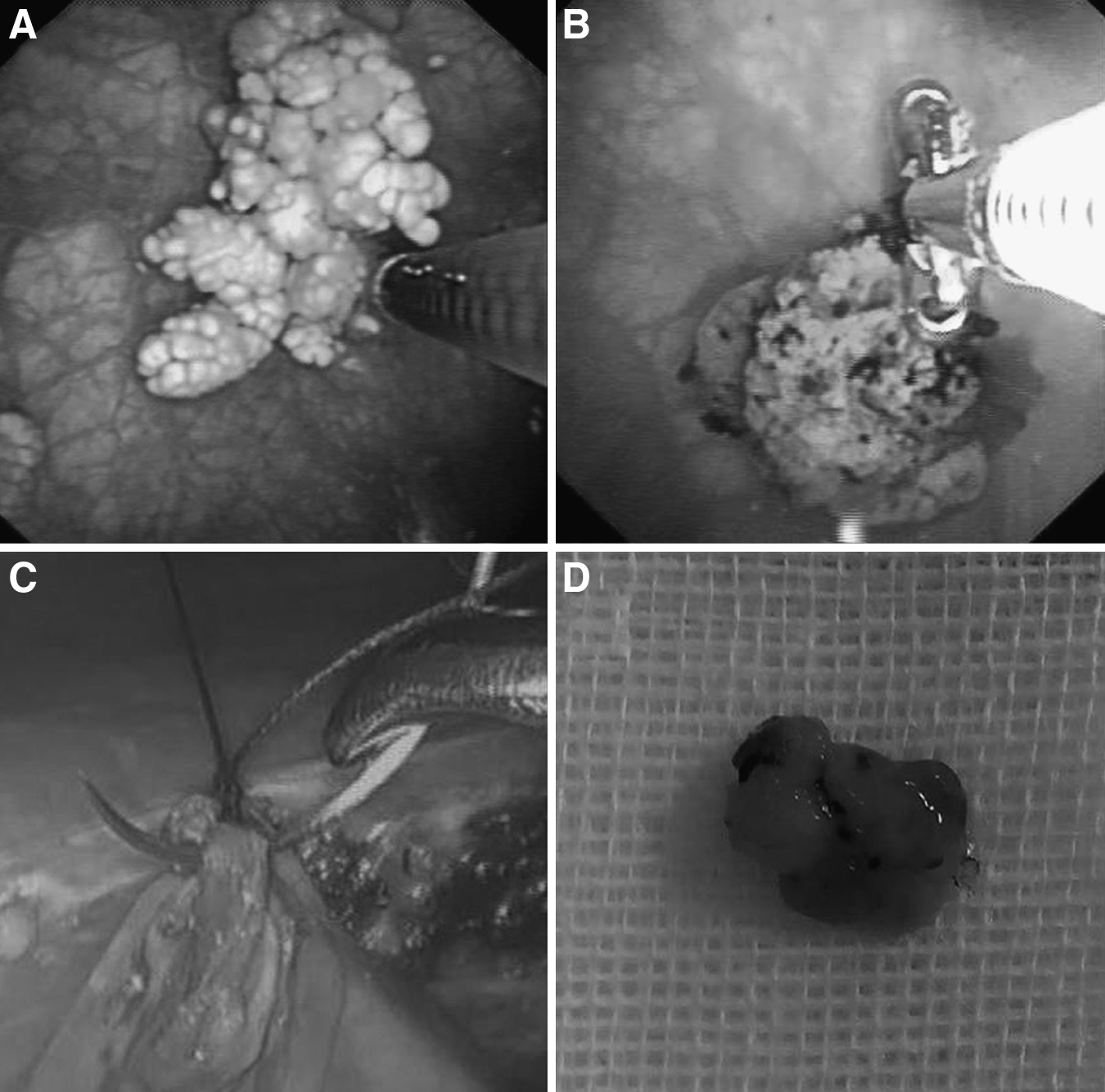
The second part of the operation procedure.
Follow-up
The follow-up of patients included assessment for clinical symptoms, polyp recurrence, and the gallbladder-emptying function. The latter was assessed by measuring the length, width, and height of the gallbladder before and after a fatty meal at 1, 3, and 6 months after the operation. Subsequently, we inspected the gallbladder every 6 months. A volume reduction of more than 30% was considered satisfactory emptying function. The other parameters included gallbladder appearance, wall thickness, and bile echo.
Statistical analysis
All data were given as mean±standard deviation. SPSS software (SPSS, Inc., Chicago, IL) was used to draw the linear graph.
Results
The security of the microwave
Microwaves generated at 50–70 mA for 9 seconds produced effective mucosa coagulation. The gallbladder mucosa of pigs was coagulated using the coaxial bipolar microwave antenna (Fig. 3B). Then, 1 week later, the gallbladder epithelial cells started to regenerate on the surface of the coagulated mucosa (Fig. 3C); 2 weeks later, the gallbladder mucosa was almost normal (Fig. 3D). All images suggested that the gallbladder mucosa is self-healing and can recover to normal after injury. Thus, endoscopic polypectomy using microwave coagulation was feasible in patients.
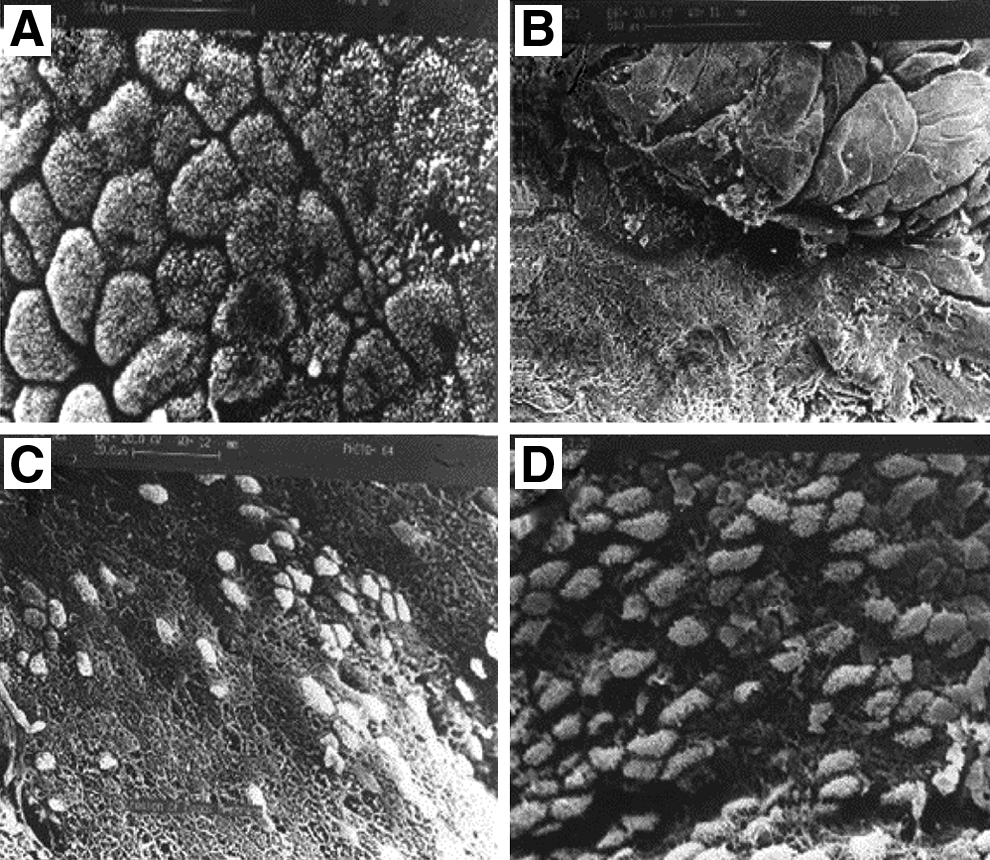
Electron micrographs show the healing procedure of the pig gallbladder mucosa coagulated with the coaxial bipolar microwave antenna.
Operative procedures
The operation procedures were successful, and the mean operation time was 1.5 hours (60–135 minutes). Neither massive bleeding nor perforation occurred. The patients fasted on the first day after the operation and were usually discharged 2 days later. There were 4 cases involving failure to preserve the gallbladder, including diffuse cholesterosis in 3 cases and massive adhesions around the gallbladder in 1 case; laparoscopic cholecystectomy was performed in one session. These cases were excluded from the study.
Follow-up
A long-term follow-up for a mean of 1.5 years (range, 0.5–2.5 years) was carried out in 56 cases, and the follow-up rate was 100%. The results showed that all patients were symptom free. Polyps did not recur. The volume and contractility of the gallbladder based on ultrasonography were found to be well preserved. Different closures for the gallbladder fundus incision slightly interfered with the volume and the contractility of the gallbladder (Fig. 4). The volume and contractility were decreased at 1 month after the operation and elevated at 3 and 6 months after the operation.
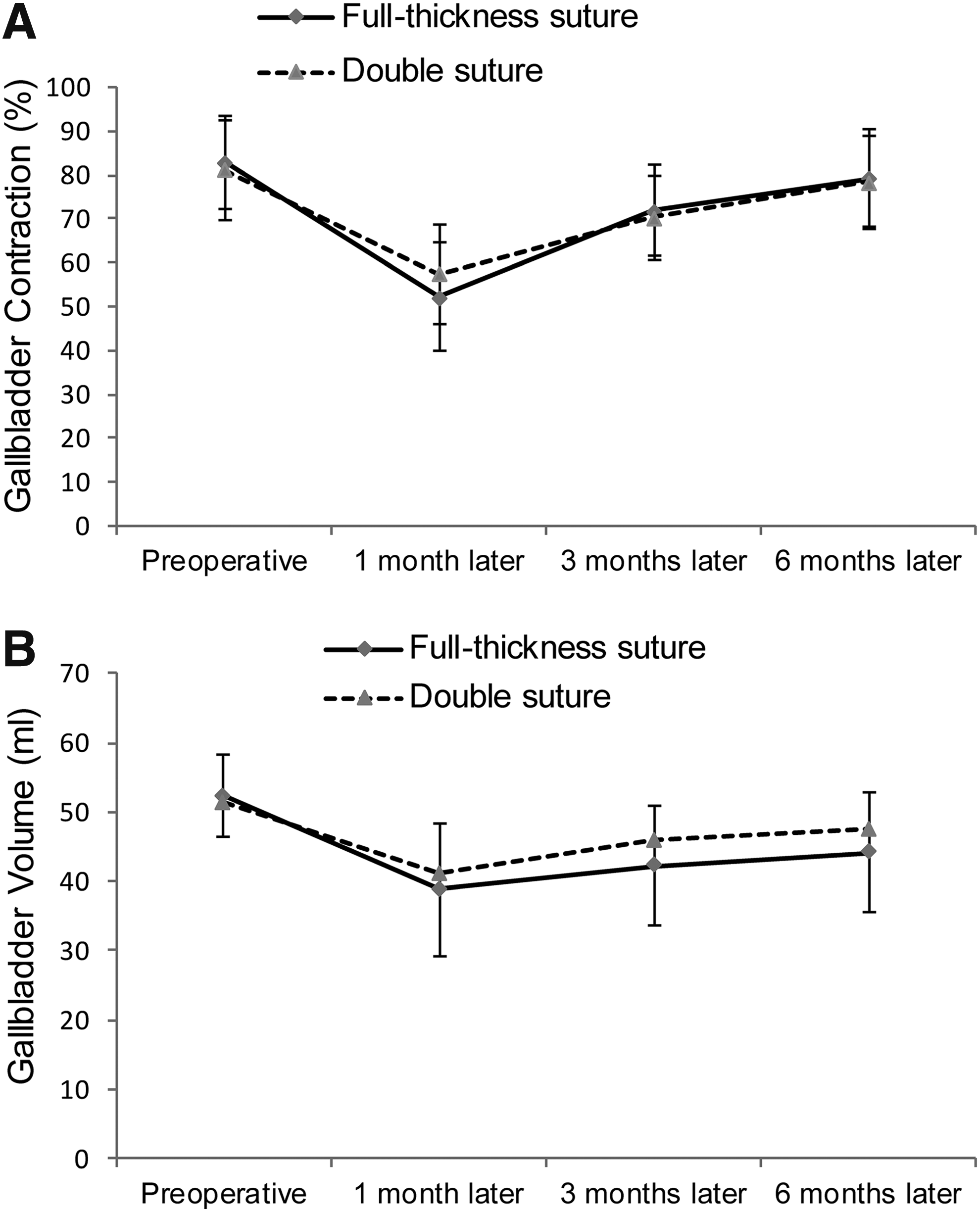
The contraction and volume of the gallbladder followed up 1, 3, and 6 months after the procedures.
Discussion
The incidence of the gallbladder polyps is high in East Asian countries. Most gallbladder polyps histologically are cholesterol polyps, whereas the minority of the polyps include inflammatory polyps, adenomyomatosis, adenomas, and others. 12 In our study, cholesterol polyps accounted for 91.07% (51/56) of the polyps detected, and the gallbladder function in these cases was good. The gallbladder is a vital organ of the human body, and its function includes not only the storage, concentration, and excretion of bile during feeding, but also the regulation of intrahepatic and extrahepatic bile duct pressure. There are also important secretion and immune functions. Based on the importance of gallbladder function, it is very necessary to select a more suitable operation for benign polyps. For this reason, we first developed a percutaneous endoscopic polypectomy technique in 1994. 7 Our past data in 2004 showed a progressive result that 78.8% of the operative patients were followed up over 5.5 years on average, and 95% of the cases had a good gallbladder function without gallstone formation and polyp recurrence. 8 Our present study also demonstrated that polypectomy of the gallbladder polyps is a reliable and effective procedure. 13
As a minimally invasive technique, percutaneous cholecystoscopy can facilitate the correct diagnosis through endoscopy and adequate biopsy using a coaxial bipolar microwave antenna for the removal of polyps and preservation of the gallbladder with satisfactory results. Since 1994, we have explored percutaneous endoscopic polypectomy for gallbladder polyps. Because of the physical limitations of the hard choledochoscope, the entire gallbladder lumen and gallbladder mucosa were difficult to clearly inspect. With the development of the soft choledochoscope, which we used instead of the hard choledochoscope, this problem was solved, and better outcomes were obtained. In 2004, 8 we published our improved procedure and follow-up results. However, in some patients who are obese or whose gallbladder is situated in an abnormal position, percutaneous procedures cannot be performed.
As the laparoscopic technique has become popular, we have modified the laparoscope by combining with a choledochoscope technique, which can be performed for nearly all patients. All procedures were uneventful with an operating time between 60 and 135 minutes, except for 4 patients who were not suitable for gallbladder preservation. In this series, there were 12 patients with a body mass index of >35 kg/m2, and their gallbladder fundus was not situated in the subcostal region; as a result, percutaneous cholecystoscopic procedures could not be performed.
Although obesity is associated with a higher incidence of gallbladder disease with increasing body mass index, 14 percutaneous endoscopic polypectomy is inappropriate in obese patients. Moreover, the higher the index, the greater the difficulty of performing any type of cholecystectomy becomes. Some studies have reported that a body mass index exceeding 30 kg/m2 increases the difficulty of the operation and that a body mass index exceeding 35 kg/m2 increases not only the wound infection rate but also the conversion rate, possibly because of the abnormal anatomy and the difficult separation of the structures, especially in Calot's triangle. 15 The Endolap technique avoids these risks, enables the gallbladder fundus to be manipulated in situ, and also has wider indications for gallbladder manipulation. All followed-up patients were symptom-free and without recurrence of polyps. Their gallbladder function recovered to the normal level 3 months after the operation. In contrast to the new technique, percutaneous endoscopic polypectomy can be a basic technique for training residents.
Currently, controversy in the management of asymptomatic patients with gallbladder polyps still exists. Therapeutic decision-making is usually correlated with the polyp size and shape. 2 Based on the literature, for the following findings, cholecystectomy was recommended: (1) polyps of 10 mm or more in diameter; (2) sessile polyps associated with stones in patients older than 50 years; and (3) symptomatic polyps. However, the diagnostic criteria for cholecystectomy remain a challenge. In this study, polyps larger than 10 mm were present in 11 cases, but only 2 cases were adenomas. In our patients, most of the polyps were detected on routine examination, and patients were usually given unclear information about the polyps, which always caused them to be afraid of malignancy of the polyps and to suffer some mental stress. In 1994, we reported one adenoma treated with percutaneous polypectomy. 7 To date, no recurrence or malignancy has occurred. To the best of our knowledge, if polyps are benign and the gallbladder function is normal, polypectomy with gallbladder preservation should be considered. However, we recommend cholecystectomy for the following cases: more than three polyps of the gallbladder, adenomyomatosis of the gallbladder, intramural gallstones, or more than three gallbladder stones. If stones were discovered by chance and there were fewer than three, we recommend removal of the polyps and stones and subsequent preservation of the gallbladder.
Gallbladder volume is an important parameter of gallbladder function. The size of a stab incision in the gallbladder fundus and the closure method could affect gallbladder function. In this study, the incision on the fundus was less than 1 cm, and double-layer sutures (mucous to mucous, seromuscular to seromuscular) influenced the gallbladder volume and contractility to a lesser extent. In the full-thickness suture group, the volume and contractility of the gallbladder at 1 and 3 months after the operation seem to be lower than those of the double-layer suture group. This observation implies that sophisticated laparoscopic suture skills are needed for gallbladder preservation. In addition, absorbable sutures are recommended, and the tissue should not be stitched extensively.
How to handle a polyp in the gallbladder is another topic we must address. Unlike polyps in the colon or stomach, polyps on the gallbladder wall are usually pedunculated or sessile. Radiofrequency is not an adequate thermal coagulator. As described in our previous study, 7 we have developed a coaxial bipolar microwave antenna that provides sufficient coagulation on the stalk or base of the polyps without perforation or bleeding. The prevention of mucosal bleeding using nephrine saline (1:1000 dilution) irrigation of the gallbladder lumen resulted in a clear view of the gallbladder cavity; thus, polyp coagulation with a microwave probe and removal with a soft forceps can be safely performed. Our animal study also demonstrated that appropriate settings of the microwave energy induced the mucosa to recover to normal 2 weeks after the operation. This reversible damage to the gallbladder wall ensures that gallbladder functioning is preserved after the procedure. We further believe that thermal injury to the polyp's stalk or basement was able to prevent polyp recurrence in the same location.
Intraoperative endoscopy is a necessary supplement to avoid missing polyps or stones. The flexible choledochoscope is another powerful tool because it can be conveniently adjusted to different angles and can explore any site of the gallbladder inner surface. 16 Initially, the choledochoscope should be attached to the gallbladder neck where small stones could be located, and then it should be moved gradually to the gallbladder incision where it should be bent as far as possible, until no other gallbladder disease is observed.
Polyp recurrence and the preservation of gallbladder function are the major problems affecting this procedure. However, the absorption and excretory function of the gallbladder should also be further studied. 17 Although contractions were observed, the correlation between the contractions and Cajal-like cells, a type of dynamic cells that stimulates gallbladder motivation, has not been studied. 18 The development of a single-incisional laparoscopic technique or robotic surgery would be a revolutionary advancement in the technology for gallbladder preservation.
In conclusion, the Endolap technique we presented here is a safe and feasible procedure. It not only avoids the risk of the complications associated with cholecystectomy but also preserves gallbladder function to the maximum extent possible. However, to the best of our knowledge, currently, the procedure should be limited to benign polyps of the gallbladder. Although no polyp recurrences were detected and gallbladder function was not compromised based on the short follow-up in most cases, the indications for this technique should be determined based on evidence. We suggest that this procedure could be an alternative treatment for patients with benign gallbladder polyps.
Footnotes
Disclosure Statement
No competing financial interests exist.