
Abstract
Abstract
Objectives:
The aim of the study was to compare the long-term oncologic results of laparoscopic liver resection (LLR) versus open liver resection (OLR) for colorectal liver metastasis (CRLM) using a propensity score analysis.
Subjects and Methods:
This propensity score matching (PSM) study was based on a prospective database of a single tertiary-care center. Patients with primarily resectable CRLM were selected for a 1:1 PSM between LLR and OLR. Covariates for PSM estimation were age, gender, body mass index, American Society of Anesthesiologists score, primary tumor location, CRLM presentation, location, size, and number. Moreover, the year of surgery was included in the PSM model. Operative, postoperative, and survival rates were compared between groups.
Results:
From 2000 to 2013, in total, 339 liver resections for CRLM met the selection criteria. Among these, 52 LLR patients were matched with 52 OLR patients. The two surgical approaches showed similar postoperative morbidity and mortality rates. LLR was associated with significantly less blood loss, less frequent need for and shorter duration of pedicle clamping, faster recovery, and shorter hospital stay. Moreover, the overall 3- and 5-year survival rates were, respectively, 83% and 76% for LLR and 87% and 62% for OLR (P=.51). The 3- and 5-year disease-free survival rates were, respectively, 28% and 21% for LLR and 31% and 21% for OLR (P=.71).
Conclusions:
The LLR achieves similar oncological results to those of the standard open surgery for CRLM, with the additional benefit of significantly faster recovery.
Introduction
C
Hepatectomy for colorectal liver metastasis (CRLM) is the only chance of cure for patients with primarily resectable disease or after chemotherapy downstaging,8,9 with a 5-year survival rate ranging from 35% to 60%.10–13
Although open liver resection (OLR) remains the most widely used procedure for CRLM, laparoscopic liver resection (LLR) is recognized as being as safe as the open approach14–16 in stringently selected patients, providing even better perioperative results as demonstrated in some case series.17–19 However, further research on the most important issues associated with this setting (i.e., the oncological outcomes of LLR) is eagerly debated and awaited because the current evidence relies mostly on scarce and methodologically weak retrospective studies.14,17,18,20,21
Among the nonrandomized study designs, the propensity score matching (PSM) analysis is gaining increasing consensus in clinical trials, as it has been shown to provide an acceptable level of evidence to control selection bias and compare treatment groups. 22 The present study aimed to assess, in a single tertiary-care center, the long-term surgical and oncological outcomes of LLR compared with OLR performed for CRLM. The two operative techniques were compared using a PSM analysis.
Subjects and Methods
Patient selection
This single-center study relied on a prospectively maintained database implemented in 1989, including 58 (12%) cases of LLR out of a total of 483 hepatectomies performed for CRLM in our unit. All consecutive patients operated on from January 2000 to December 2013 were included in the selection process for the PSM, provided the following criteria were fulfilled: primarily resectable liver disease in a single procedure and absence of metastatic extrahepatic disease. Specifically, re-hepatectomies for recurrent liver metastases, combined colectomy or proctectomy, two-stage hepatectomy, and patients needing preoperative portal vein embolization were excluded.
All procedures were performed by four surgeons operating in pairs with expertise in both laparoscopic and open liver surgery. In all cases, the aim of surgical treatment was to achieve complete macroscopic resection of CRLM with a remnant liver volume to body weight ratio of ≥0.5%. 23 Major hepatectomy was defined as the resection of three or more liver segments 24 as described by Couinaud. 25 The techniques for open and laparoscopic resections have been previously described in detail.26–29 Intraoperative liver ultrasound was performed in all cases to confirm the number and size of the lesions, to define their relationship to the major intrahepatic vascular structures, and to look for occult liver metastases. Doppler ultrasound was repeated upon completion of resection to assess vessel patency in the liver remnant.
The study was approved by the Henri-Mondor Hospital Institutional Review Board and was conducted in accordance with the Helsinki Declaration for human research studies.
PSM
Prematch baseline characteristics of all selected cases of LLR and OLR were compared by bivariate analysis to assess imbalances of covariates. PSM was performed to minimize selection bias in the control group. This method allowed for the comparison of treatment effects by accounting for the important known covariates predicting the selection of laparoscopy versus open surgery. Propensity scores were estimated using logistic regression.30,31 The regression model included the following covariates: age, gender, body mass index, American Society of Anesthesiologists score, primary tumor location, preoperative chemotherapy, synchronous or metachronous presentation of CRLM, and CRLM location (liver segment), number, and size. These covariates were chosen because they were available (1) for the decision to proceed for surgery and (2) for choosing the open versus the laparoscopic approach. Moreover, the year of surgery was included into the model in order to control for historical bias, which might be expected for studies that span over a long period of time.
An 1:1 “nearest neighbor” match paradigm was used: each LLR patient was matched with the OLR patient with the most similar estimated propensity score. After matching, the two groups were compared to control covariate balance and the similarity in baseline covariates between groups. Then, the two matched groups were compared with respect to the end points of the study.
Short- and long-term outcomes
The following variables were analyzed: patient demographics; CRC and CRLM characteristics; type of liver resection; perioperative and operative parameters, including operative time, rate of conversion, blood loss, and completeness of resection (taken from the operative reports); postoperative and oncological outcomes, including Clavien–Dindo classification of complications 32 ; morbidity; duration of hospital stay; tumor recurrence after resection; and long-term survival rates. Postoperative mortality and morbidity were defined as events occurring during the hospital stay or within 90 days after resection. Long-term outcomes included overall and disease-free 1-, 3-, and 5-year survival rates. Overall survival was measured from the date of liver resection to the date of death or latest follow-up. Recurrence-free survival was measured from the date of liver resection to the date of confirmed recurrence or death from any cause.
After liver resection, the patients were evaluated every 3 months for the first 3 postoperative years and every 6 months thereafter. Each follow-up visit included clinical assessment, total body computed tomography scan, and serum carcinoembryonic antigen measurement.
Statistical analysis
For bivariate two-sided comparisons between the LLR and the OLR groups, the chi-squared test or Fisher's exact test was used for categorical variables, and, according to the data distribution, the t test or Mann–Whitney U test was applied for continuous variables. Hence, continuous data were expressed as mean (standard deviation) values or medians and ranges (minimum to maximum). Overall and disease-free survival rates were analyzed using the Kaplan–Meier method. Survival curves were compared using the log rank (Mantel–Cox) test. The study was performed in an intention-to-treat basis (i.e., patients converted from laparoscopic to open resection were kept in the laparoscopic group for analysis). A P value of<.05 was considered to be statistically significant. Statistical analyses and PSM were performed with SPSS software (Statistical Package for Social Science, IBM SPSS Statistics, version 22 for Macintosh; IBM, Armonk, NY).
Results
Prematch study population
Over the total of 483 consecutive liver resections for liver metastases from CRC, 339 patients operated between 2000 and 2013 met the study inclusion criteria. Of these, 52 (15.3%) were LLR, and 287 (84.7%) were OLR. Baseline characteristics of the prematch groups are outlined in Table 1. There were considerable imbalances between the LLR and OLR groups in relation to the size of the largest CRLM nodule, the number of CRLM, and the proportion of synchronous or metachronous CRLM, which were significantly higher in the OLR group. Moreover, a trend toward a significant difference was observed for the rate of preoperative chemotherapy and additional biological therapy. The majority of the sample (59.6%) was operated in the period 2007–2013, without statistical difference between groups (33 patients [63.5%] for LLR and 169 patients [58.9%] for OLR; P=.64).
By Mann–Whitney U test.
By Fisher's exact test.
By chi-squared test.
ASA, American Society of Anesthesiologists; BMI, body mass index; CEA, carcinoembryonic antigen; CRC, colorectal cancer; CRLM, colorectal liver metastasis; LLR, laparoscopic liver resection; OLR, open liver resection.
Postmatching baseline characteristics
By using PSM, the 52 LLR patients were matched with 52 OLR patients (Fig. 1). The balance of covariates was assessed for accuracy of the model. No covariate had a standardized mean difference of >0.25 between the two groups. The average absolute standardized difference of the mean propensity score was 0.22 in the prematched samples and 0.019 in the postmatched sample. The ratio of the variance in the two groups was 0.9.30,33,34 The baseline characteristics of the matched LLR and OLR groups are summarized in Table 2. There were no significant differences in baseline parameters included in the logistic regression between the LLR and OLR groups. There were also no significant differences between groups concerning the number of patients receiving postoperative chemotherapy (51.9% in the LLR group versus 61.5% in the OLR group; P=.43). In each group, 19 patients (36.5%) were operated between 2000 and 2007; the remaining 33 patients (63.5%) were operated between 2007 and 2013 (P=1).
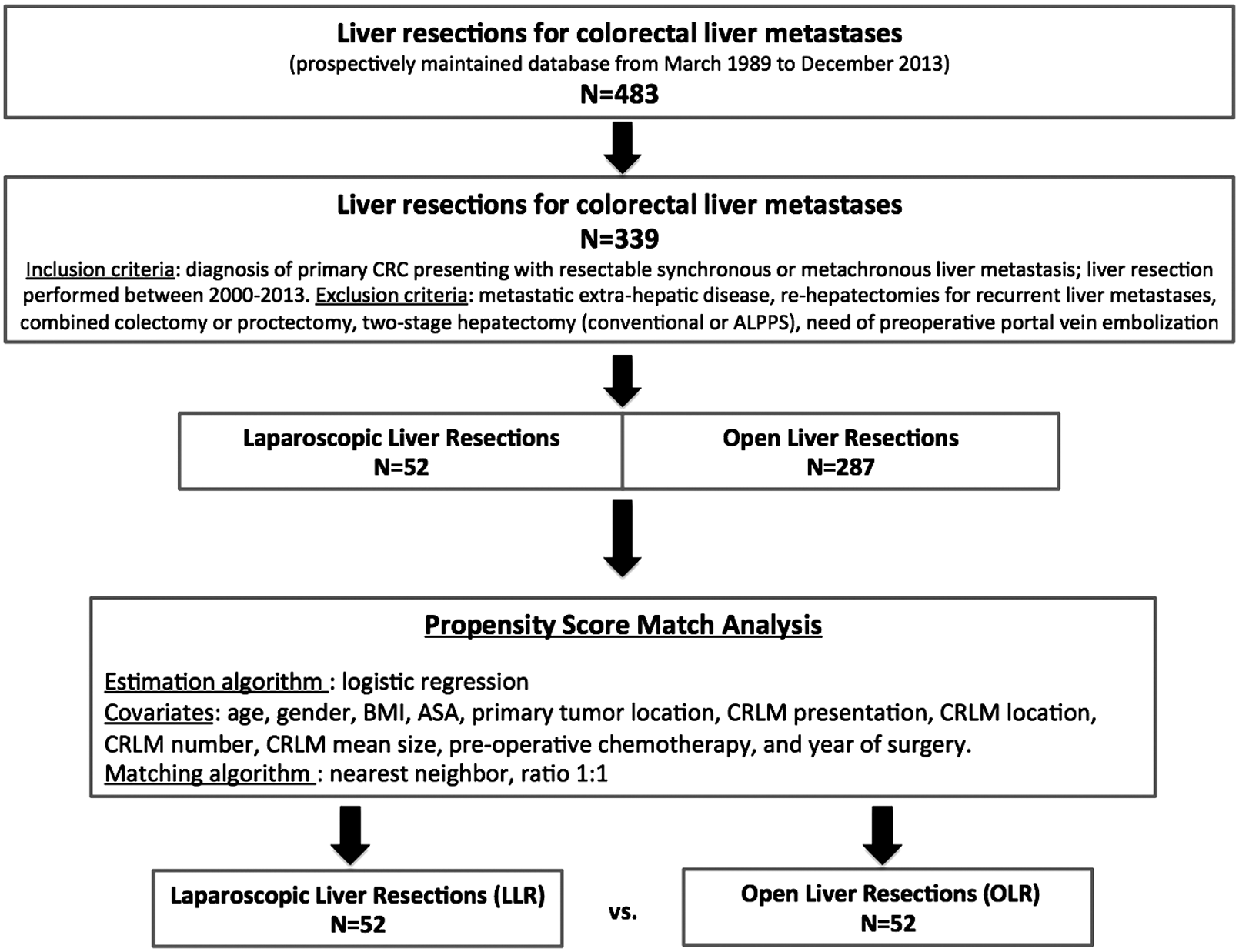
Study design frame, patient selection, and propensity score matching. ALPPS, associating liver partition and portal vein ligation for staged hepatectomy; ASA, American Society of Anesthesiologists; BMI, body mass index; CRC, colorectal cancer; CRLM, colorectal liver metastasis.
By Mann–Whitney U test.
By Fisher's exact test.
By chi-squared test.
ASA, American Society of Anesthesiologists; BMI, body mass index; CEA, carcinoembryonic antigen; CRC, colorectal cancer; CRLM, colorectal liver metastasis; LLR, laparoscopic liver resection; OLR, open liver resection.
Operative and postoperative variables
Intraoperatively, no significant difference between the two groups was observed for the type of liver resection (P=.94) or operative time (P=.27) (Table 3). Conversely, the LLR group was associated with significantly less frequent pedicle clamping (12/52 [23.1%] versus 32/52 [61.5%] cases; P=.0001). When the pedicle was clamped, the median total ischemia time was 20 minutes (range, 5–45 minutes) for LLR and 35 minutes (10–90 minutes) for OLR (P=.002). In addition, the estimated blood loss (200 versus 300 mL; P=.001) and the need for transfusion (3 versus 11 cases; P=.041) were significantly lower in the LLR than in the OLR group (Table 3). In the LLR group, three (5.8%) conversions to laparotomy occurred in 1 case each for the following reasons: portal vein injury during right hepatectomy, massive hemorrhage during wedge resection of segment 4, and hemodynamic instability upon induction of pneumoperiteneum. The postoperative course of these 3 patients was uneventful.
By chi-squared test.
The mixed hepatectomies were as follows: wedge resection of segment I+segmentectomy of III; and wedge resection of segment V+segmentectomy of III.
By Mann-Whitney U test.
By Fisher's exact test.
Significant difference.
LLR, laparoscopic liver resection; OLR, open liver resection.
Overall 90-day mortality and morbidity rates were 1.9% (2 patients) and 19.2% (20 patients), respectively, with no difference observed between the two groups (P=.49 and P=.62, respectively). As shown in Table 3, the median time to flatus and hospital stay were 2 (range, 1–4) days and 6 (range, 2–13) days for the LLR group, versus 3 (range, 1–5) days and 9 (range, 3–25) days for the OLR group. These two parameters were significantly shorter for the LLR group (P=.006 and P=.0001, respectively).
Specimen analysis
The two groups were similar in terms of specimen weight (P=.68) and status of underlying liver parenchyma (P=.47) (Table 3). More importantly, R0 resection was achieved in 43/52 cases (82.7%) in the LLR group and in 46/52 cases (88.5%) in the OLR group (P=.57).
Overall and disease-free survival rates
The mean follow-up was 58.6±44.4 months (range, 8–171 months) for the LLR group and 54.1±43.4 months (range, 7–172 months) for the OLR group (P=.73). No patient was lost in the follow-up. Similar overall survival rates were observed for the two groups at 1, 3, and 5 years: 96.1%, 80.7%, and 73.1% for the LLR group, respectively, and 97.6%, 87.5%, and 62.5% for the OLR group, respectively (P=.51) (Fig. 2). The 1-, 3-, and 5-year disease-free survival rates were 75%, 28.8%, and 21.1% for the LLR group, respectively, and 61.5%, 30.7%, and 21.1% for the OLR group, respectively (P=.71) (Fig. 3 and Table 4). Twenty-three patients (44.2%) in the LLR group and 20 patients (40%) in the OLR group showed disease recurrence during the follow-up (P=.69). The majority of tumor recurrence involved the liver only (18/23 for LLR and 16/20 for OLR). The recurrent CRLM occurred within a median time interval after liver resection of 13 months (range, 3–62 months) for the LLR group and 11 months (range, 3–47 months) for the OLR group (P=.75).
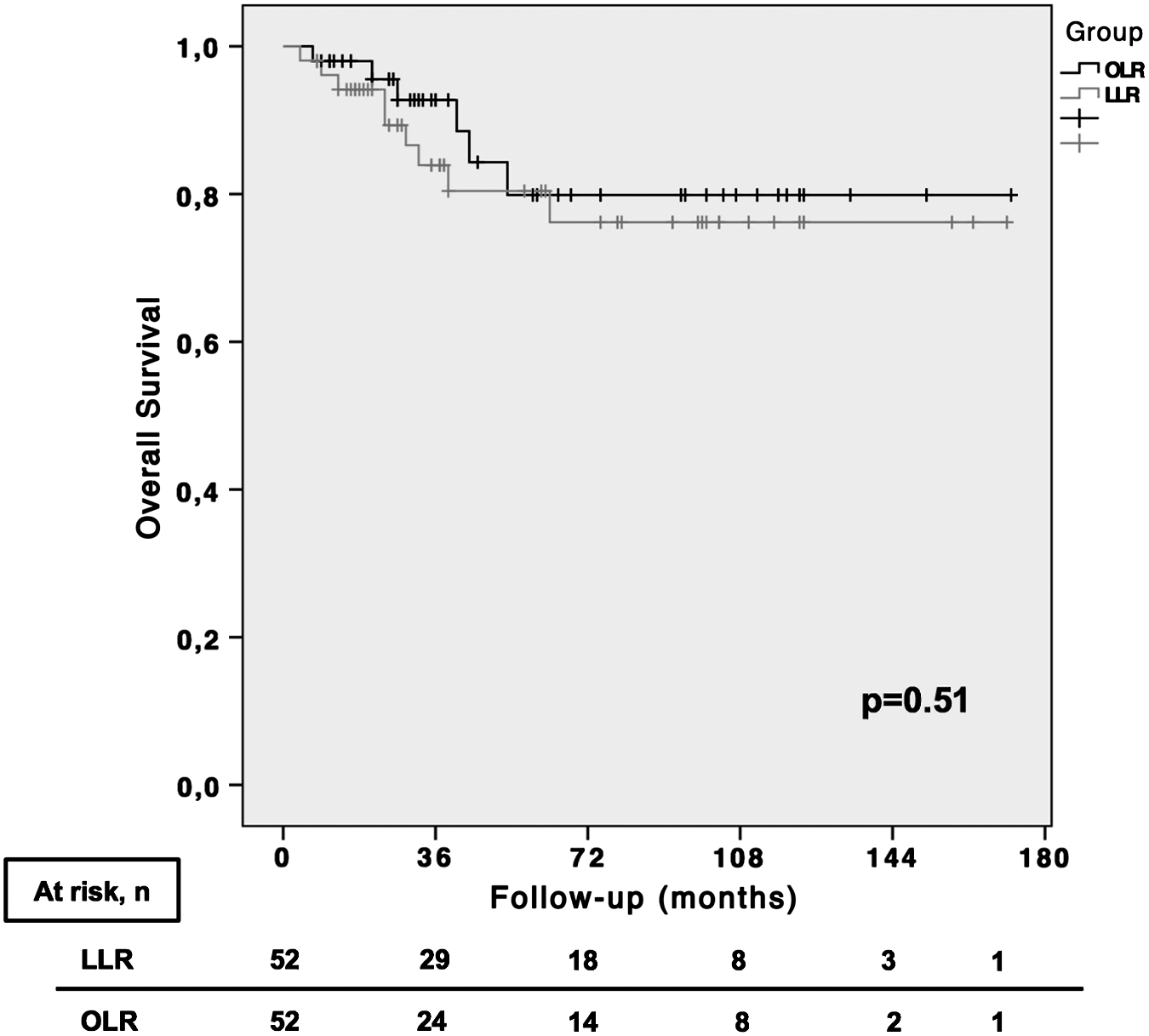
Overall survival of the laparoscopic (LLR) and open (OLR) liver resection groups.
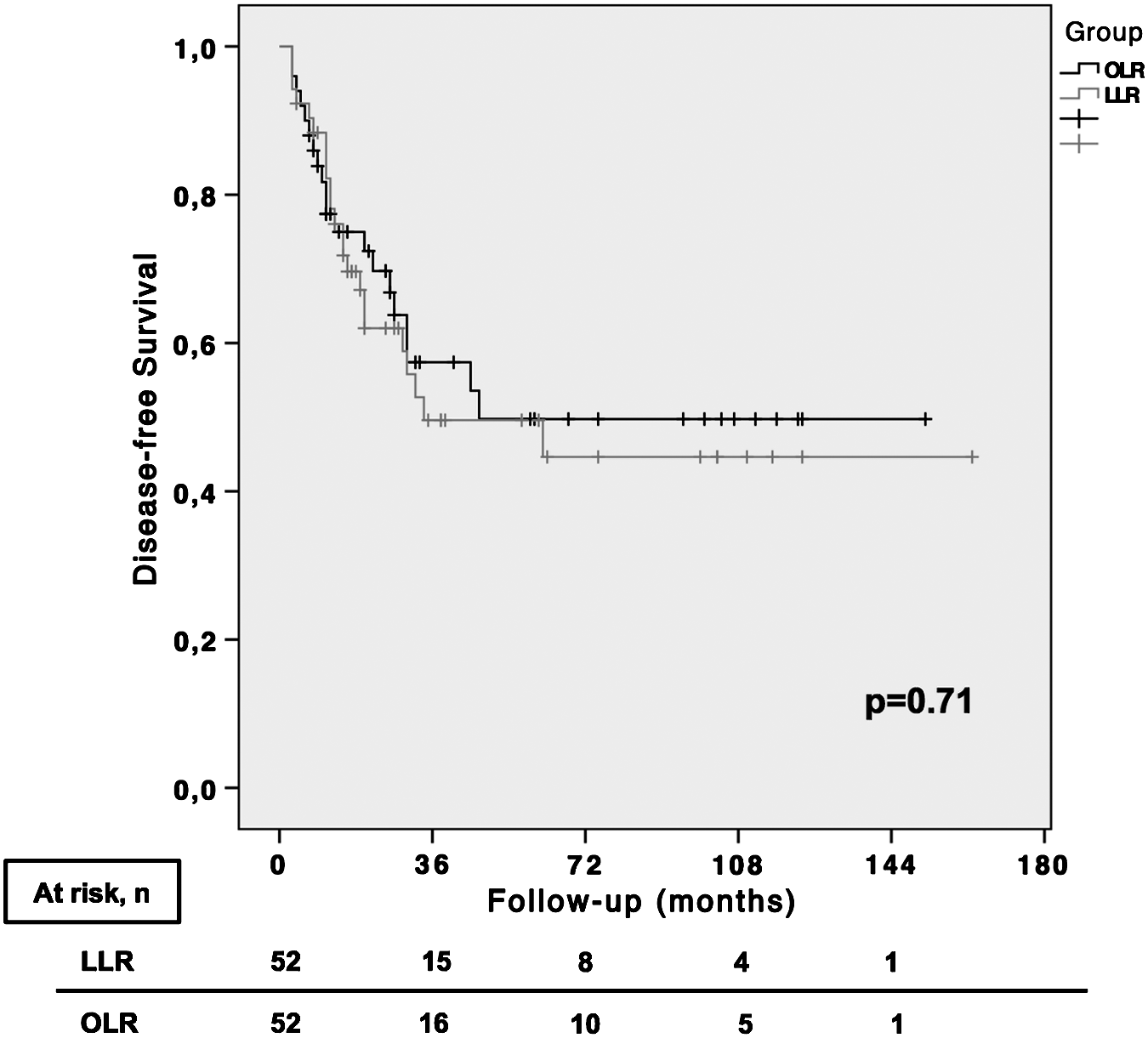
Disease-free survival of the laparoscopic (LLR) and open (OLR) liver resection groups.
All are retrospective, matched case-control studies, except for Cannon et al. 35 (2012) and the present one, which used propensity score matching analysis. All studies, except Castaing et al. 17 (2009), are single-center.
LLR, laparoscopic liver resection; NS, nonsignificant, as reported in the original articles; OLR, open liver resection.
Discussion
This study compared by using PSM analysis the laparoscopic and open approach for CRLM resection. 22 The main result of the present study is the demonstration that LLR and OLR have similar long-term overall and disease-free survival rates. Additionally, the two surgical approaches are associated with similar postoperative morbidity and mortality. Nevertheless, the analysis of perioperative outcomes shows that the laparoscopic approach could be performed with significantly faster recovery and shorter hospital stay.
Previous studies have already observed comparable overall and disease-free survival rates between LLR and OLR (as summarized in Table 4).17,18,20,21,35,36 However, these results come mainly from retrospective comparative studies with limited sample sizes and inherent limitations related to the significant risk of selection22,37 and reporting bias. 38 The PSM used in the present study has allowed for the treated groups to be balanced across the major putative risk factors and known confounders that may influence the selection of the surgical approach. 39
Of note is a recent meta-epidemiological study comparing treatment effect estimates between nonrandomized studies with propensity score adjustment and randomized controlled trials (RCTs) that was performed by Lonjon et al., 22 scoping a broad range of unselected clinical questions in surgery. They found no statistically significant difference in the treatment effect between the two study designs.
Furthermore, although RCTs are the gold standard for therapeutic evaluation, they remain hardly applicable for surgical interventions and large populations. Nonrandomized studies may thus be useful by providing information on treatment effectiveness in a more representative context (i.e., a real-world setting).22,40 No RCTs have been published on surgical approaches for CRLM. A search at the URL www.clinicaltrials.gov using the terms “laparoscopy,” “liver resection,” “open resection,” and “colorectal liver metastases” revealed two RCTs registered in 2012 and 2013: the Oslo-CoMet (NCT01516710) and ALIVE (NCT01720966) studies. Only the Oslo-CoMet study appears to be recruiting patients. Therefore, whether the studies ever reach completion, their long-term results will not be available before 2020. In this perspective, nonrandomized studies with PSM design might be considered the best level of evidence available, especially if based on a prospectively maintained database and carried out with an intention-to-treat analysis.
In the present study, the propensity score on which the groups were matched was calculated including the factors that are accounted as bias in the selection of the surgical approach as well as parameters known to potentially influence the clinical outcomes and prognosis.9,41,42 The matched LLR and OLR groups showed similar postoperative and long-term outcomes in terms of morbidity and mortality rates. The good oncologic results observed in both groups may be related to multiple factors. With respect to the completeness of resection (R stage), the different type of liver resection has not influenced the achieved rates of R0 margins, which were similar in the LLR and OLR groups. However, compared with OLR, LLR was associated with a significantly less frequent need for pedicle clamping, yielding lower rates of ischemia/reperfusion injury, less blood loss, and lower need for transfusion. Although it is still under debate whether these perioperative parameters are predictive factors on the oncologic outcome,24,43–45 the laparoscopic approach enabled their achievement. Again, the methodology used in this study reinforces what was at least partly reported in the literature.14,36,46,47
Another factor known to potentially influence the long-term oncologic outcome is the use of neoadjuvant chemotherapy.48–51 Although the therapeutic protocols in the case of CRLM have not yet been standardized, neoadjuvant chemotherapy is considered the current standard.42,50,52 In the present study, the majority of the patients received preoperative chemotherapy (i.e., Folfox, Xelox, Folfiri), in a similar proportion between the LLR and OLR groups. Patients who did not receive neoadjuvant chemotherapy were usually those with single metachronous CRLM.51,52 Moreover, patients included in the present study were treated between 2000 and 2013; the point could be raised that over this time interval the chemotherapic protocols and recommendations have been modified. For this reason, the year of surgery was included in the PSM model in order to balance the two groups over the different therapeutic protocols that have been observed during the years. Because of the balance between groups, the influence of chemotherapy on the oncologic results might be limited.
During the past decades, the indications of laparoscopy for liver resection have continued to expand, paralleling the widespread application of the minimally invasive hepatobiliary surgery implemented by the development of novel surgical devices. In this scenario, the stringent selection of patients remains crucial to the success of liver resections. Nevertheless, our experience suggests that criteria such as tumor location in superior and posterior liver segments, tumor size greater than 5 cm, and proximity to major hepatic structures should no longer be considered as absolute contraindications for the application of laparoscopy. 26 Rather, the surgical approach should be chosen on a patient-by-patient basis according to the individual risk, while the operation should be planned in order to spare hepatic parenchyma to leave sufficient remnant functional liver and to anticipate the potential need for re-hepatectomy. 53 Moreover, vascular clamping with subsequent ischemia/reperfusion injury should be used keeping in mind to balance the hemorrhage with its short- and long-term prognostic impacts. 43 Considering the good long-term survival and the postoperative advantages of LLR, it appears evident that in the future the effort will be to increase the number of patients operated on by laparoscopy, adapting the liver resection to the disease and not to the surgeon's skills. However, as stressed by several studies concerning laparoscopy in CRLM treatment,18,47 the surgeon's experience and the specific training in minimally invasive hepatobiliary surgery may represent an important issue that is equally related to the instrumental equipment available and the volume of patients in each single surgical center.
The present study has strengths related to its relatively large sample of patients operated on by laparoscopy within the same surgical unit and monitored over a long follow-up period. Moreover, potential selection bias inherent to the evaluation of the surgical approach and historical bias related to the study period were controlled by the use of PSM. With regard to external validity of the study, it is important to highlight that all liver resections were performed by experienced attending surgeons. 54 Thus, the present results cannot be generalized to centers with minor surgeon and/or institutional experience in complex hepatobiliary and minimally invasive surgery. Keeping this in mind, the present study confirms that laparoscopy should be considered a valuable alternative to open surgery and may become the “gold standard” for selected patients as expertise in liver laparoscopy increases further. 55
In conclusion, in the subset of selected patients operated on by LLR and OLR, the present results demonstrate that LLR for primarily resectable CRLM provides oncologic long-term outcomes that are fully comparable to those of the open approach. Although the two surgical approaches have similar short-term results, laparoscopy is associated with a faster recovery.
Footnotes
Acknowledgments
The authors would like to thank Maria Clotilde Carra, PhD, for her valuable support in statistical analysis and manuscript preparation.
Disclosure Statement
No competing financial interests exist.