
Abstract
Abstract
Sleeve gastrectomy is an effective and single stand-alone surgical procedure for the treatment of morbid obesity. One of the most frequent and serious complications of this procedure is staple-line leak. It can usually be treated with self-expandable stents. If this process results in failure and gastrocutaneous fistula occurs, a challenging period starts for the patient and the surgeon. We describe a new, relatively simple and quick endoscopic technique for closing a chronic gastrocutaneous fistula. A plug prepared with porcine acellular dermal matrix was used for this purpose. Gastrocutaneous fistula following an obesity surgery can be successfully treated endoscopically with this technique. This method can prevent the need for aggressive reconstructive surgery following a gastrocutaneous fistula and can prompt rapid improvement while decreasing the average hospital stay for this condition.
Introduction
L
In this study, we describe a new technique for the management of gastrocutaneous fistula that occurred after a failed endoscopic stent treatment for a leak in a patient on whom LSG had been performed.
Technique
The novel technique was first performed on a patient in order to close a gastrocutaneous fistula that had formed after an external drainage of a staple-line leakage from the stomach. A 43-year-old obese male patient was admitted to our bariatric surgery center at Ankara University Hospital (Ankara, Turkey). The patient was obese, with a body mass index of 36.8 kg/m2, and had comorbidities, including recently diagnosed type 2 diabetes. LSG was performed, and no leak was identified by an intraoperative leak test performed using blue dye and air insufflation. An upper gastrointestinal (UGI) series on postoperative Day 1 was also normal.
The patient was discharged on postoperative Day 4. Three days following his discharge, the patient was admitted to our clinic with intraabdominal sepsis. Abdominal computed tomography revealed a staple-line leak at the esophagogastric junction, as well as intraabdominal collections in the subhepatic, subdiaphragmatic, and pelvic regions (Fig. 1). We undertook laparoscopic re-exploration, but due to multiple adhesions and purulent collections, we were obliged to convert to laparotomy. We tried to repair the defect using 2-0 polypropylene suture, but the tissue was very fragile, and the defect could not be closed. We inserted the 22-Fr silicone drainage catheter in the left subdiaphragmatic region toward the esophagogastric junction to make a controlled fistula and replaced two closed suction drainage tubes in the other collection cavities. A partially covered self-expandable and retrievable metal stent (length, 80 mm; diameter, 18 mm; Choostent®; M.I. Tech, Seoul, Korea) was placed endoscopically on the following day.

Computed tomographic view of the fistula. The arrow indicates the fistula tract.
He was referred to a nutritionist and given a stent diet after a contrast study that confirmed an appropriate seal and no leakage. Two weeks later, the gastric contents were identified through the drainage tube, and following a UGI series, a massive leak around the esophagogastric junction was confirmed. The stent position was corrected. Oral intake was then prohibited, and supportive care in combination with total parenteral nutrition was maintained for 2 weeks. In order to facilitate the stent removal, a fully covered self-expandable metal stent (length, 100 mm; diameter, 20 mm; Hanarostent®; M.I. Tech) was placed endoscopically into the first stent. One week later, both stents were removed, and at this point the UGI series confirmed the presence of the massive leak.
About 6 weeks had passed since the operation, and we changed our treatment strategy in order to close the fistula.
We performed a UGI endoscopy with the patient under general anesthesia and exposed the fistula orifice. A guidewire (Anrei Medical, HZ Co. Ltd., Hangzhou, Zhejiang, China) was slid through the endoscope and guided through following the fistula tract in order to remove the 22-Fr silicone drainage catheter. We pulled the guide from the drainage catheter orifice, and the endoscope was then gently pulled out (Fig. 2). We prepared a fistula plug using Permacol™ (porcine acellular dermal matrix; Covidien, Mansfield, MA) mesh, and we tied 4/0 polyglactin 910 (Vicryl®; Ethicon, Cincinnati, OH) (70 cm) suture between the distal end of the plug and the mouth side of the guide (Fig. 3). When we gently pulled out the guide from the skin side, we simultaneously followed the plug with UGI endoscopy. We applied TISSEEL (Baxter, Vienna, Austria) via an endoscopic applicator (Fig. 3) into the fistula orifice, and then the plug was placed; the cap of the plug completely covered the orifice (Figs. 4 and 5). Then, the Vicryl was sutured on the skin at the fistula orifice for the purpose of immobilizing the plug.
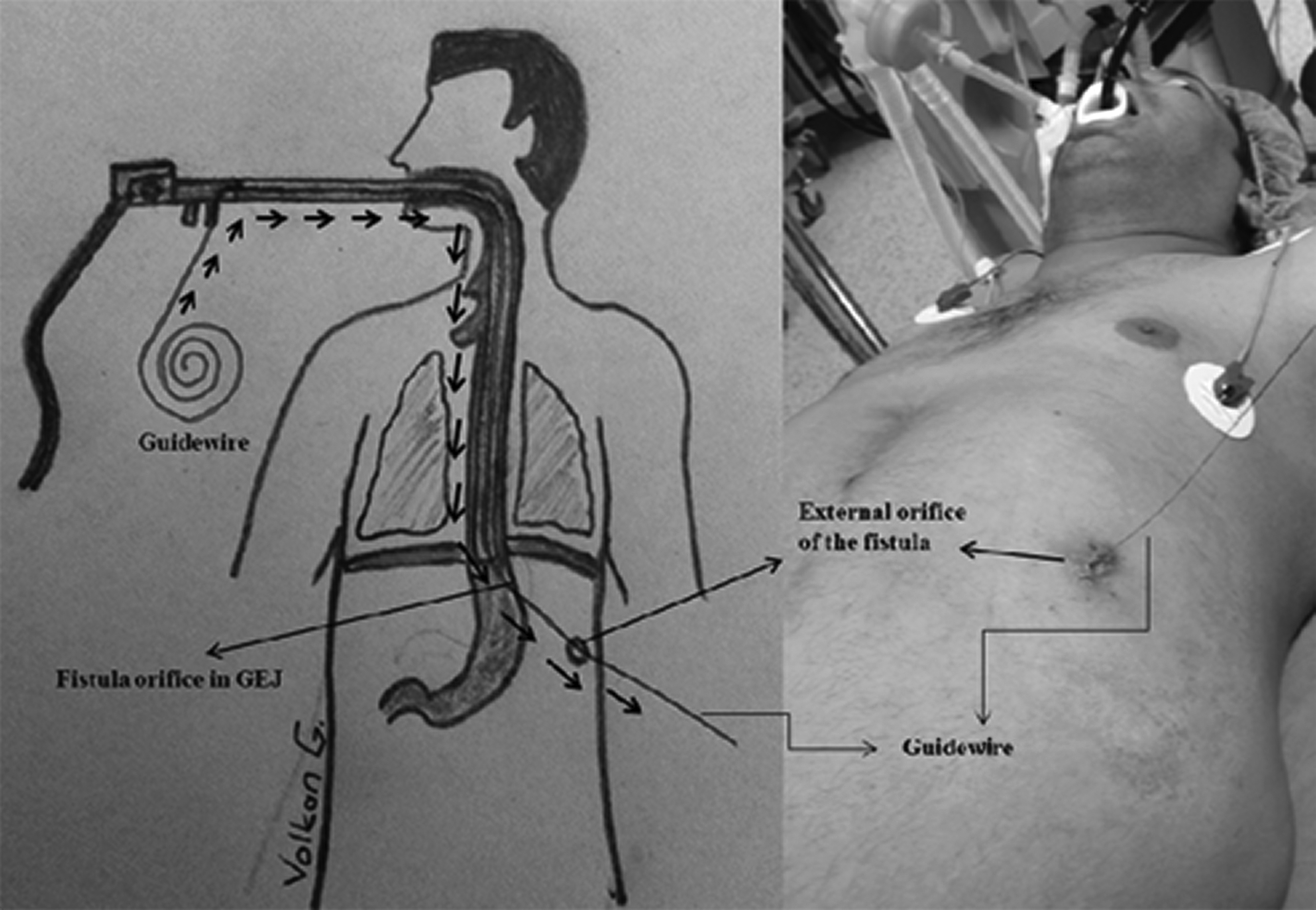
First step: the placement of a guidewire into the fistula tract. GEJ, gastroesophagus junction.
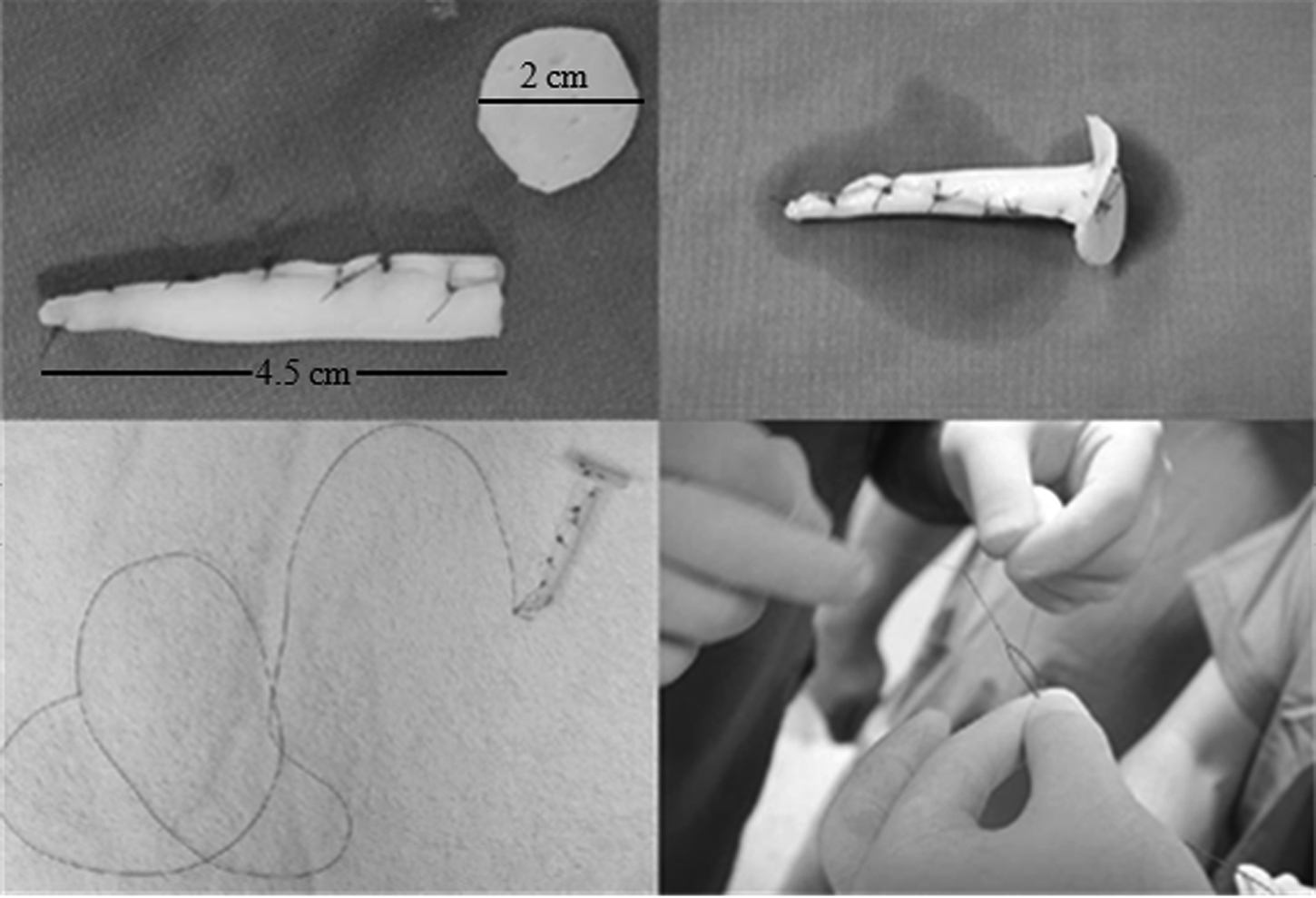
Second step: the preparation of a fistula plug from Permacol mesh.
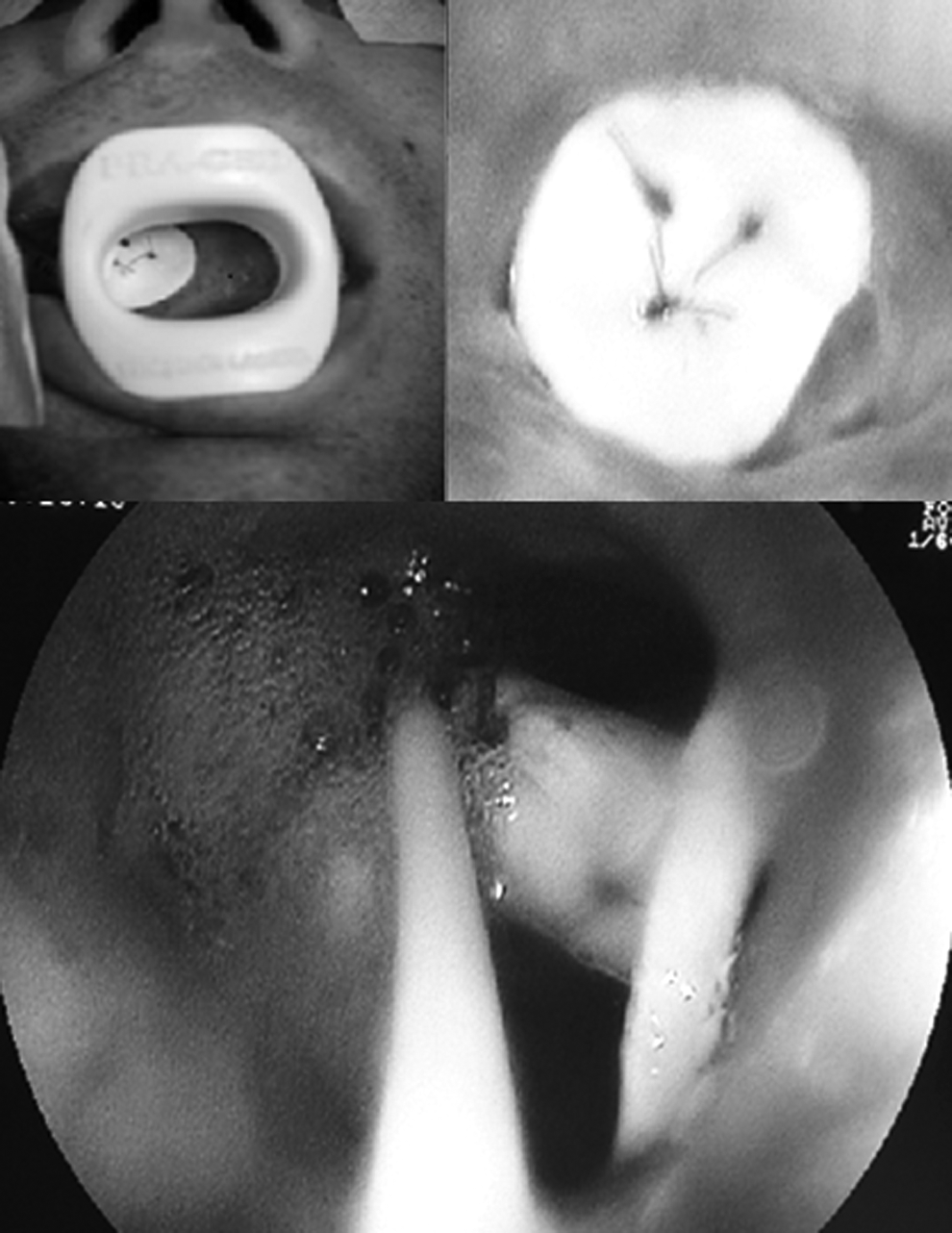
Third step: endoscopic viewing of the placement of a plug using fibrin glue.
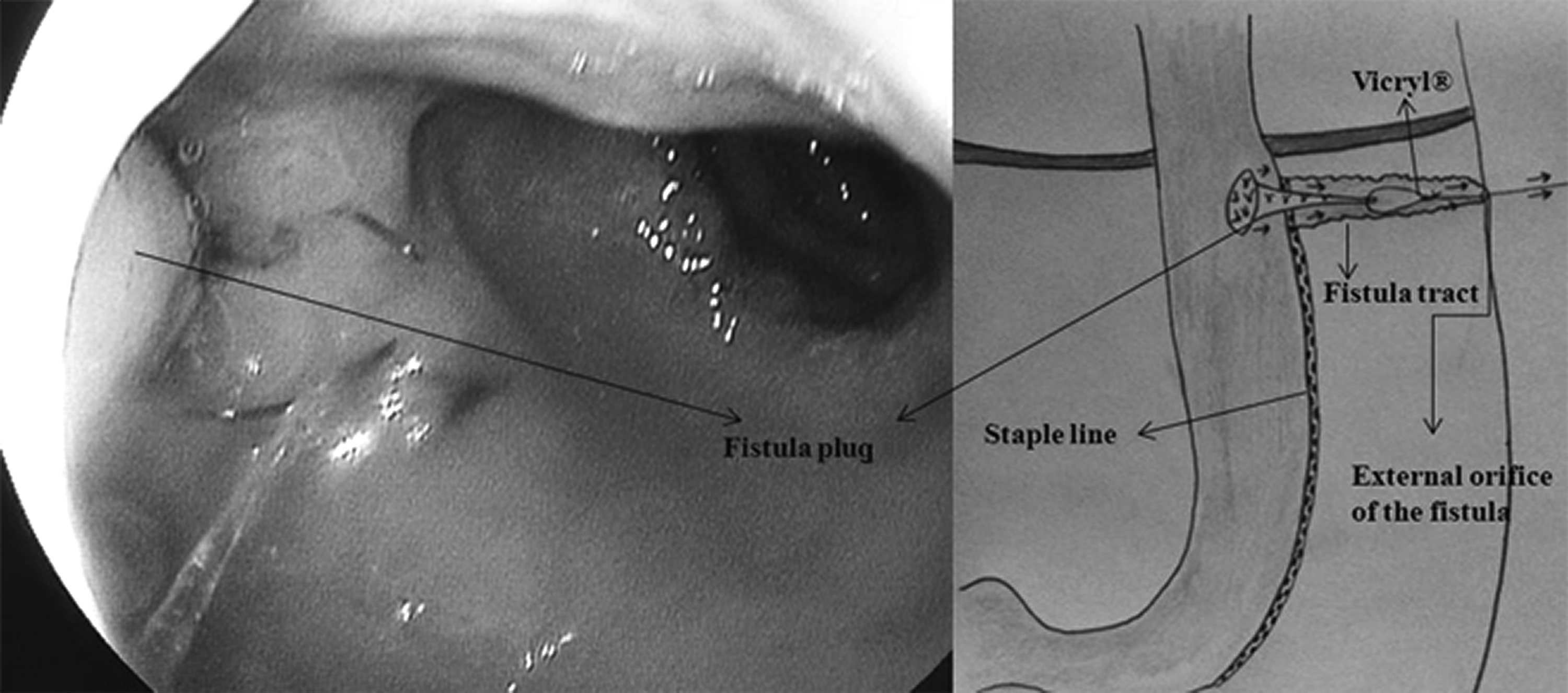
The final appearance of the plug application.
After 2 days from the application of this method, the UGI series was normal, and no leak was identified. The patient was discharged and received a stent diet for 15 days. The 15-, 30-, and 60-day controls were normal with the patient having no complaints.
Discussion
The major complications of sleeve gastrectomy are leakage, hemorrhage, and abscess formation, of which the most dreaded is the staple-line leak because it can rapidly lead to septic conditions (localized or diffuse peritonitis). Thus, it is a potentially life-threatening surgical emergency that can be associated with high morbidity and mortality. This condition must be recognized early and managed immediately. Extreme suspicion is very important for early diagnosis; furthermore, tachycardia, feelings of unhappiness, and discomfort also may alert the surgeon in the early postoperative period.
The treatment of an intraabdominal leak is dependent on the size of the leak and the clinical status of the patient. Generally, a small-size leak from the gastrojejunal anastomosis in the biliopancreatic diversion or Roux-en-Y gastric bypass can be successfully treated with conservative treatment, including drains, parenteral nutrition, and antibiotics. Surgical intervention may be inevitable under the circumstances of a large leak or of a small one with worsening clinical status. Surgical repair, diversion, and placement of a feeding jejunostomy for enteral nutrition or of a new drain for effective drainage are among the possible treatment modalities. 10
On the other hand, leaks that take place after sleeve gastrectomy, especially in the superior aspect of the staple line, are more challenging for clinicians and patients due to high intragastric pressure caused by the intact pylorus. These kinds of leaks, with the exception of microleaks, cannot generally be treated conservatively. If the leak is diagnosed early (<7 days postoperatively) and the drain is still present, control of sepsis, adjuvant routine antibiotics, and total parenteral nutrition are immediately begun. If the diagnosis is delayed, clinical status is very important for determining the treatment method.
Although well-contained collections in a stable nonseptic patient can be managed by radiologic drainage, surgical drainage of any abscess/collection is mandatory in a septic patient. After efficient drainage is provided, some interventions are usually needed. As a surgical option, oversewing with or without omental patches frequently results in failure due to excessive inflammatory tissue. So, removing partially or fully covered self-expanding metal stents, endoscopic metallic clips, and endoscopic sealing glue and/or use of more invasive techniques such as feeding jejunostomy, jejunal serosal patch repair, gastrojejunal anastomosis, Roux-limb placement, and total gastrectomy can be mandatory.11–16
Although stent treatment for leaks is a first option in our clinic, we are well aware that the effectiveness of self-expandable stents is not 100%. We choose partially covered metallic stents due to their creation of high granulation and minimal sliding. In this case, the stent was placed endoscopically, using fluoroscopy as a guide with a guidewire-assisted deployment, and then we waited for 3 weeks for sufficient granulation. If the stent can be endoscopically removed, we do not need a second stent, but if excessive granulation occurs and the stent cannot be endoscopically removed, we insert a fully covered stent that is 2 mm wider than the original into the primary stent, and we wait 1 more week for easy removal of the first stent. In case of failure of the endoscopic endoluminal placement of stents, various endoluminal clips can alternatively be used, but regarding this option, there are limited and conflicting results in the literature.17,18 When gastrocutaneous fistula develops, a definitive surgical approach including gastrojejunal anstomosis, Roux-limb placement, or total gastrectomy is generally recommended in the literature.13,16
In this study, we described a new, relatively simple, and quick technique for closing a chronic gastrocutaneous fistula. This technique can prevent the need for aggressive reconstructive surgery following a gastrocutaneous fistula and can yield rapid improvement while decreasing the average hospital stay for this condition.
Footnotes
Acknowledgments
The authors wish to extend a sincere thank you to the staff members of the Endoscopy Unit at Ankara University for their assistance in completing this project.
Disclosure Statement
No competing financial interests exist.