
Abstract
Abstract
Introduction:
Laparoscopic low anterior resection is commonly performed, but there is controversy about the optimal specimen extraction site. The purpose of the study was to evaluate the outcomes of two different specimen extraction sites.
Materials and Methods:
In this prospective study of total laparoscopic low anterior resection for rectal cancer, we compared the outcomes of specimen extraction from a right lower quadrant trocar site that is also used for a defunctioning ileostomy (21 patients) or a Pfannenstiel incision (25 patients).
Results:
The median visual analog pain score on postoperative Days 1 and 3 and meperidine requirement were significantly higher in the Pfannenstiel than in the ileostomy site group. Time to resumption of oral diet and hospital stay were significantly shorter in the ileostomy site than in the Pfannenstiel group. All four parastomal hernias were observed in the ileostomy site group.
Conclusions:
Use of the stoma site for specimen extraction in total laparoscopic low anterior resection for rectal cancer may minimize abdominal wall incisions, decrease postoperative recovery time, decrease pain level and analgesic requirement, and improve cosmesis. Although this procedure may increase the incidence of parastomal hernia, hernia repair may be performed during ileostomy takedown surgery, and the temporary stoma site (which also is the right lower quadrant trocar entry site) may be suggested as a proper specimen extraction site.
Introduction
L
During total laparoscopic rectal cancer surgery, the entire abdominal and pelvic dissection and the division of the distal rectum are performed laparoscopically. After an intracorporeal anastomosis is performed, a small abdominal incision is made that is sufficient for specimen extraction after reinsufflation of the abdomen. Although this surgical technique is performed commonly, there is controversy about the specimen extraction site that has the lowest frequency of postoperative hernia and wound infection. In total laparoscopic rectal surgery, a lower abdominal incision or the defunctioning ileostomy site usually may be preferred for this purpose.
The Pfannenstiel incision is associated with a low frequency of postoperative wound infection and incisional hernia in gynecologic procedures.6,7 For hand-access or specimen extraction sites in minimally invasive colorectal surgery, the Pfannenstiel incision may have fewer wound complications than other abdominal incisions. 8 However, the use of the Pfannenstiel incision includes an additional incision for specimen extraction in patients undergoing low anterior resection for rectal cancer with a defunctioning ileostomy.
The purpose of the present study of total laparoscopic low anterior resection for rectal cancer was to evaluate the advantages of extracting the specimen from the defunctioning ileostomy site compared with the Pfannenstiel incision.
Materials and Methods
Patients
This prospective study included 46 consecutive patients (age: mean, 67 years; range, 33–88 years) who had total laparoscopic low anterior resection with a defunctioning ileostomy at our hospital between May 2010 and October 2013. The study included only patients who had a specimen extraction site on the abdominal wall and completion of ileostomy closure. Patients were excluded because of prior abdominal surgery, conversion from laparoscopic to open surgery, or incomplete follow-up. The study was approved by the ethics committee of Baskent University, and written informed consent was provided by all patients.
The location of the tumor was measured at colonoscopy as the distance from the anal verge; tumors were located in the lower rectum (≤6 cm; 19 patients), middle third rectum (6.1–12 cm; 22 patients), and upper rectum (>12 cm; 5 patients). Based on preoperative staging, 16 patients had neoadjuvant radiochemotherapy.
Surgery
All laparoscopic low anterior resections were performed in our clinic with five trocars: one subumbilical port (10 mm) for the camera; two ports (12 mm) at the right lower quadrant and suprapubic midline; and two ports (5 mm) at the right and left upper quadrants (Fig. 1). The right lower quadrant port incision was placed medially, at the lateral edge of the rectus muscle, for use in specimen extraction and defunctioning ileostomy (Fig. 2).

Trocar entry sites for laparoscopic low anterior resection.
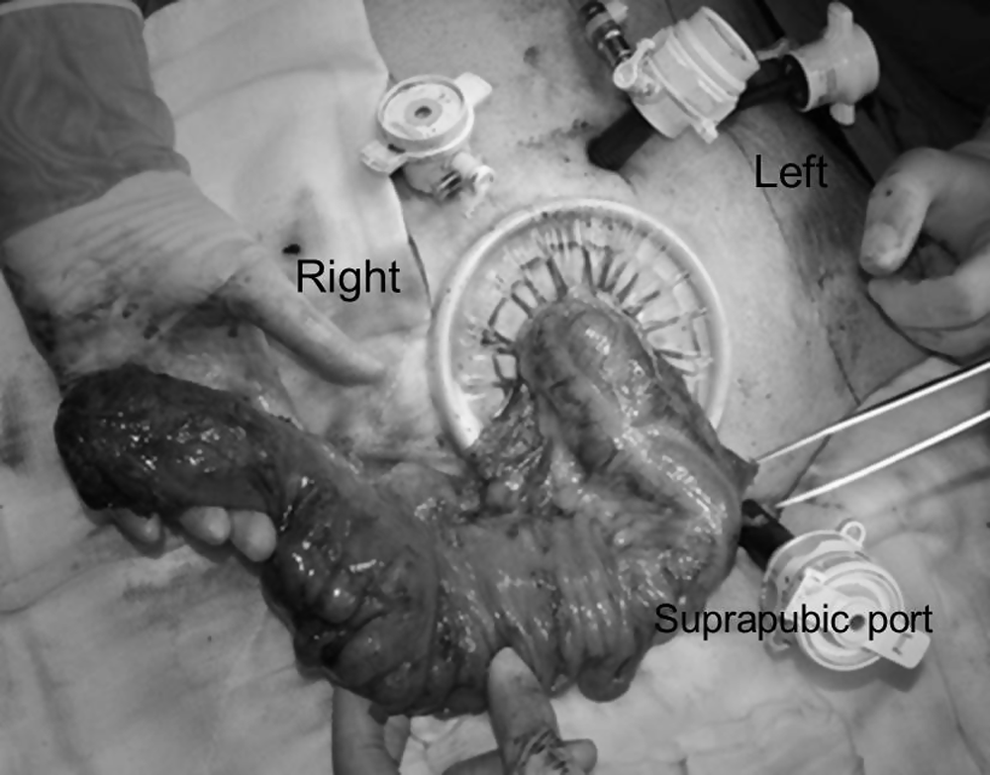
Specimen extraction from the right lower quadrant trocar site.
After the sigmoid colon was exposed, the inferior mesenteric pedicle was identified and ligated. The splenic flexure was then mobilized, and the transverse colon was separated from the pancreas so that the colon could be mobilized up to the middle colic artery in all cases. Total mesorectal excision was accomplished for tumors located in the lower and middle third of the rectum; for tumors located in the upper third, a partial mesorectal excision was performed with a 5-cm distal resection margin from the tumor. The rectum was divided laparoscopically using linear staplers, and anastomosis was performed with intracorporeal double-cross staplers. For very low rectal tumors (7 patients), pelvic dissection was completed from the transanal approach, and a hand-sewn anastomosis was performed. Specimens were extracted from the extended right lower quadrant or suprapubic ports. When the right lower quadrant was the preferred specimen extraction site, the skin incision and underlying oblique fascia (trocar entry hole) were extended, and the rectus muscle was retracted medially. After extraction of the specimen, the peritoneum and fascia were partially closed, leaving a two-finger aperture to accommodate the ileostomy (Fig. 3). When the specimen was extracted from a Pfannenstiel incision, the rectus muscle was split in the midline after the extension of the suprapubic port and anterior rectus sheath incisions, and the peritoneum was opened vertically; in these cases, the right lower quadrant trocar site was used only to remove the ileostomy. Nonabsorbable sutures were used for fascia closure at both extraction sites.
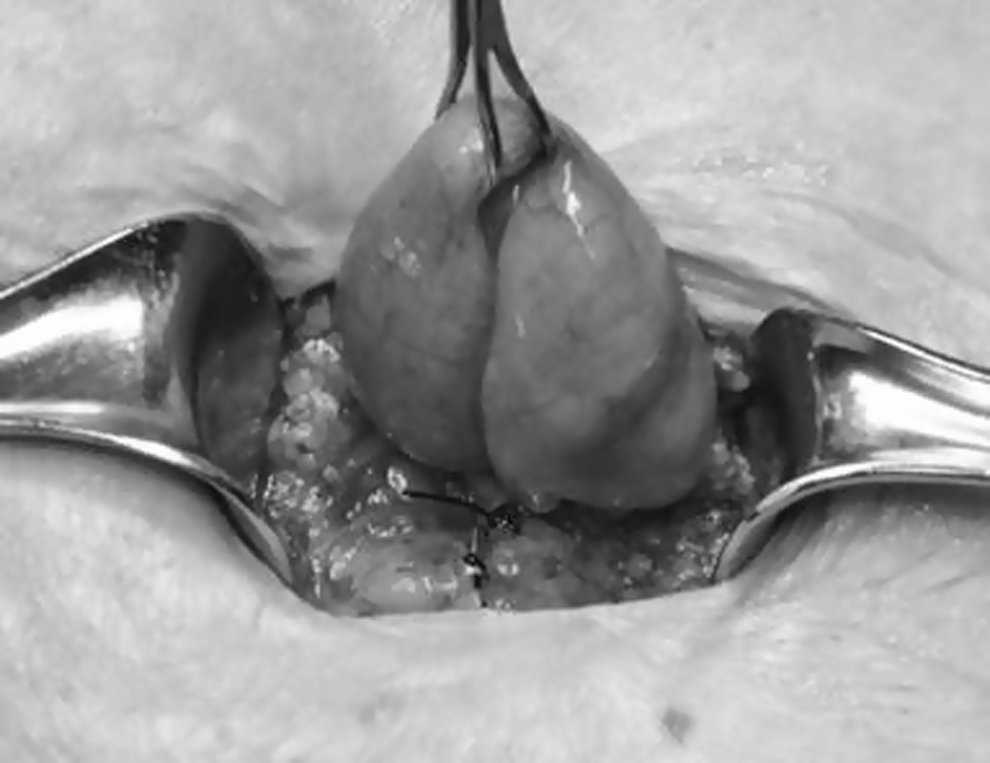
Ileostomy and closure. The ileostomy was made after extraction of the specimen, and the peritoneum and fascia were partially closed.
Although this was a prospective study, it was not possible to allocate the patients randomly to the study groups because for some patients the extraction site had to be chosen during the surgery. In 1 patient who had laparoscopic linear cutting stapler failure, a conventional stapler was inserted through a Pfannenstiel incision, and this incision subsequently was used for specimen extraction. In 3 patients, after the intracorporeal anastomosis was performed, the specimens were extracted from the Pfannenstiel incision because the surgeon was uncertain about the security of the anastomosis.
Evaluation
Patients were categorized into two groups according to the specimen extraction site: right lower quadrant trocar site (which also was the site of the ileostomy) (21 patients) or Pfannenstiel incision site (25 patients). Clinical parameters were recorded prospectively including demographic characteristics, operating time, length of extraction site incision, American Society of Anesthesiologists physical status classification, cancer stage, neoadjuvant or adjuvant therapy, postoperative pain scores, analgesic requirement, length of hospital stay, time to resumption of oral diet, postoperative complications, postoperative hernia development, and length of follow-up. Postoperative pain scores were assessed with a visual analog scale (from 0=no pain to 10=worst pain imaginable) at Days 1 and 3 after surgery. Analgesic requirement was evaluated by calculating the total dose of meperidine given after surgery from the patient-controlled analgesia device until the end of postoperative Day 2. Wound infection was defined by inflammatory signs or drainage at the specimen extraction site requiring antibiotic treatment or wound opening. Prolonged postoperative ileus was defined as absence of flatus by postoperative Day 4, with or without intolerance to oral intake. Parastomal hernia was defined as an abnormal protrusion of the contents of the abdominal cavity through the abdominal wall defect that was created during ileostomy takeout procedure (Fig. 4). Parastomal hernia was diagnosed with physical examination, radiographic imaging studies performed for any reason, and intraoperative findings during the ileostomy takedown surgery. All clinical parameters and outcomes were compared between the study groups.

Right lateral view of a standing patient with a parastomal hernia. This hernia developed where the specimen was extracted from the ileostomy site.
Gastrointestinal continuity was restored by ileostomy takedown surgery after 6–12 weeks, except patients who received adjuvant therapy had ileostomy reversal delayed until the completion of treatment. The mean interval between the initial operation and ileostomy reversal was 174 days (range, 49–357 days).
Statistical analysis
Data analysis was performed with statistical software (IBM SPSS Statistics for Windows, version 20.0; IBM Corp., Armonk, NY). Conformity of variables to normal distribution was examined with the Kolmogorov–Smirnov test, and Levene's test was used for equality of homogeneity of variances. Differences in categorical variables between groups were analyzed using the chi-squared test and Fisher's exact test, and quantitative variables and independent groups were compared with the Mann–Whitney test and the t test. Statistical significance was defined by P≤.05.
Results
There was no difference between the two groups in age, sex, American Society of Anesthesiologists score, body mass index, albumin level, tobacco use, diabetes mellitus, distance from the anal verge to the lowest margin of the tumor, and neoadjuvant chemoradiotherapy (Table 1). Evaluation of early postoperative outcomes showed that the median visual analog scale score on postoperative Days 1 and 3 and mean meperidine requirement were significantly higher in the Pfannenstiel than in the ileostomy site group (Table 2). Prolonged postoperative ileus (3 in the Pfannenstiel group, 1 in the ileostomy site group), resolved with nonoperative treatment (Table 2). Superficial wound infections involving the skin and/or subcutaneous tissue were observed in 4 patients in the Pfannenstiel group, and these minor infections were treated with local wound care without antibiotics. Time to resumption of oral diet and hospital stay were significantly shorter in the ileostomy site than in the Pfannenstiel group (Table 2). The Tumor-Node-Metastasis (TNM) stages and frequency of adjuvant chemoradiotherapy were similar between the two groups (Table 2).
Data are reported as number, mean±standard deviation, or number (%), as indicated, for a total of 46 patients.
ASA, American Society of Anesthesiologists; NS, difference not significant (P>.05).
Data are reported as number, mean±standard deviation, or number (%), as indicated, for a total of 46 patients.
NS, difference not significant (P>.05); TNM, Tumor-Node-Metastasis; VAS, visual analog scale.
All four parastomal hernias were observed in the ileostomy site group and were classified (by the European Hernia Society Classification of Parastomal Hernias 9 ) as type 1 (3 patients) and type 3 (1 patient); these parastomal hernias were repaired at postoperative months 7, 9, 10, and 11 with using an onlay nonabsorbable prosthetic mesh during the ileostomy reversal surgery, after the completion of adjuvant treatment. All patients in both groups were followed up at a mean of 400 days after ileostomy reversal, and there was no significant difference in incidence of incisional hernia between the two groups (Table 2).
Discussion
Total laparoscopic rectal cancer surgery is gaining recognition with increased experience in minimally invasive colorectal surgery. This method is associated with reduced abdominal wall trauma, decreased postoperative pain, improved cosmesis, and shorter recovery period than open surgery. The total laparoscopic approach has the advantage of better visualization of the mesorectum, nearby nerves, and other vital structures during deep pelvic dissection because of the magnification of the laparoscope, compared with laparoscopic-assisted surgery.10,11 Although an abdominal incision is needed to remove the specimen from the peritoneal cavity during total laparoscopic surgery, the incision is smaller than the laparoscopic-assisted or hand-assisted laparoscopic surgery incisions.
There are several options in laparoscopic colorectal surgery for the specimen extraction site including midline, left or right lower oblique, and Pfannenstiel incisions, depending on the surgeon's preference, port sites, and surgical technique. 12 The Pfannenstiel incision is used frequently to extract the specimen and has advantages, including the following: (1) one of the 12-mm ports usually is inserted from the suprapubic region to facilitate low-level rectum stapling, and this port site can easily be converted to a Pfannenstiel incision; (2) this incision also can be used for completion of the low pelvic dissection and extracorporeal anastomosis; and (3) the reported frequencies of wound infection and hernia are low. Recent retrospective studies have shown significantly lower incidence of wound disruption, infection, and incisional hernia after laparoscopic cancer surgery when a Pfannenstiel incision is used.8,13 The Pfannenstiel incision usually is the preferred specimen extraction site in our clinic. In 1 of the patients in the present report, this incision was used to perform the anastomosis with a surgical stapler, preventing the conversion to open surgery from the laparoscopic technique.
The level of the anastomosis that is below the peritoneal reflection in rectal cancer surgery carries a higher risk of anastomotic leakage. The reported incidence of leakage varies from 2.6% to 26.2%. 14 A defunctioning ileostomy has been recommended for routine fecal diversion and may decrease the incidence of anastomotic leakage requiring surgical intervention. However, some authors have suggested a more selective approach and recommended stoma formation when there is concern about the safety of the anastomosis because of difficult surgery, incomplete doughnuts, or positive air leakage test. 14
In our clinic, we routinely perform a defunctioning loop ileostomy in rectal cancer surgery, when the anastomosis is at the level of the pelvic floor or below, for patients who received neoadjuvant therapy or when there is doubt about an unsafe anastomosis. For patients who have planned stoma creation during laparoscopic colorectal surgery, the stoma site also can be used for specimen extraction.15–17 However, in laparoscopic low anterior resection, complete mobilization of the splenic flexure and additional proximal dissection are required to safely extract the specimen from the right ileostomy incision. Although this may not be necessary and may be time consuming in some cases, it has the advantage of providing a tension-free anastomosis. In addition, when there is doubt about insufficient blood supply at the distal end of the proximal colon after resection, the surgeon can perform additional colon excision.
Whole mobilization of the splenic flexure is technically more demanding when tension is observed on a completed anastomosis. In laparoscopic colorectal surgery, choosing the specimen extraction site is a special challenge because of a desire to reduce the number and size of the incisions and to maintain the postoperative benefits of the laparoscopic procedure. In the present study, our intention was not to create an additional abdominal incision other than the trocar entry sites by removing the specimen from the right lower quadrant trocar site, which also was used for ileostomy take out.
The feasibility of left-sided ileostomy at the specimen extraction site in laparoscopic-assisted low anterior resection for rectal cancer was assessed previously. 15 Although the specimen was extracted from a left ileostomy site in a group of patients, a separate left lower quadrant incision was used for that purpose in another patient group that had right-sided ileostomy. 15 Despite the additional abdominal incision in the left lower quadrant for patients with right-sided ileostomy, there was no difference between groups in recovery data, including time to resumption of regular diet and length of hospital stay, but pain status was not evaluated. 15 In the present study, narcotic analgesia requirement and pain levels were higher in the Pfannenstiel group, possibly because of the presence of two separate incisions. In the ileostomy site group, there was only onr abdominal incision, less bowel manipulation, and less analgesic requirement, and these factors may shorten the gastrointestinal recovery period with earlier regular oral intake and decreased hospital stay (Table 2). Although the frequency of prolonged postoperative ileus was also higher in the Pfannenstiel group, the difference was not statistically significant (Table 2).
Parastomal hernia is the most frequent problem and may be an inevitable consequence of stoma formation.18,19 A higher frequency of hernia may be associated with stomas formed lateral to, instead of through, the rectus abdominis, and this risk may be reduced by properly placing the stoma through the rectus muscle. However, the available data do not support the opinion that the location of the stoma through or lateral to the rectus abdominis affects hernia formation. 20 Parastomal hernia formation may be affected by diseases (high body mass index, diabetes mellitus, ulcerative colitis, increased intraabdominal pressure, postoperative sepsis, corticosteroid use, or malignancy), patient factors (age, smoking status, or malnutrition), and technical factors (stoma location or aperture size). The frequency of parastomal hernia after loop ileostomy is 0%–6.2% at a median of 3 months and 9% at a median of 4 months.20,21 In a prospective study, the prevalence of parastomal hernia was 22% for ileostomies (in which 59% were loop ileostomies) after a median of 14 months between stoma formation and assessment. 22 The variation between studies in frequency of parastomal hernia after loop ileostomy may depend on differences in follow-up until the ileostomy takedown procedure.
In the present prospective study, there was a 9% frequency of parastomal hernia at a mean of 6 months, comparable to previous studies (Table 2). All four parastomal hernias were observed in the ileostomy site group. The only difference in surgical technique between the groups was the length of the right lower quadrant fascia incision. In both groups, the trocar entry site at the lateral border of the right rectus abdominis muscle was used for stoma takeout. However, in the ileostomy site group, the oblique fascia incision was extended (mean, 6.7 cm), to facilitate specimen extraction without disrupting the integrity of the specimen, and sutured by leaving a two-finger aperture for ileostomy, which may explain the occurrence of parastomal hernias only in this group.
At long-term follow-up, another complication was the development of an incisional hernia at the temporary stoma site after ileostomy takedown (Table 2). The frequency of this complication may be 31%–48%.23,24 Therefore, all four parastomal hernias were repaired with the extraperitoneal onlay prosthetic mesh technique during the ileostomy closure surgery, and a polypropylene mesh was used, which we believe is safe and economic. Although the risk factors for hernia development were similar in both groups, further study is required with more patients for multivariate analysis of parameters that may have a negative effect on wound healing.
In summary, use of the stoma site for specimen extraction in total laparoscopic low anterior resection for rectal cancer may prevent an additional abdominal wall incision, decrease postoperative recovery time, decrease pain level and analgesic requirement, and improve cosmesis. Although this procedure may increase the incidence of parastomal hernia, further study is needed to evaluate this problem with larger patient groups. Furthermore, hernia repair may be performed during ileostomy takedown surgery, and the temporary stoma site (which also is the right lower quadrant trocar entry site) may be used as the specimen extraction site.
Footnotes
Disclosure Statement
No competing financial interests exist.