
Abstract
Abstract
Background:
Although laparoscopic surgery is now extensively used, laparoscopic middle pancreatectomy (LMP) has rarely been described.
Study Design and Methods:
A 45-year-old woman was diagnosed with branch duct intraductal papillary mucinous neoplasia (IPMN) at the pancreatic neck, which was discovered after numerous attacks of acute pancreatitis. LMP was decided on for treatment.
Results:
The patient underwent pure LMP with right to left dissection and one-layer pancreatogastric anastomosis. Surgery lasted 160 minutes, with 20 mL of blood loss. A frozen section showed negative margins on both sides. The postoperative course was uneventful with 15 days in the hospital. Histology confirmed the diagnosis of branch duct IPMN with moderate dysplasia and negative margins. The patient is symptom free 6 months after surgery.
Conclusions:
Our results and the data in the literature suggest that the laparoscopic approach is indicated for middle pancreatectomy because there are no technical or oncological contraindications and the outcome is similar to that with the open approach.
Introduction
W
Patient and Methods
Surgical technique
Our surgical technique has already been described in detail. 16 The patient is placed in the supine position with the legs spread apart and the right arm along the body. Trocar placements and surgical team position are illustrated in Figure 1. Harmonic™ shears (Ethicon Endo-Surgery, Issy les Moulineuax, France) and a bipolar coagulation device are needed. Once exploration is complete, the gastrocolic ligament is divided, and the stomach is charged with tape and tracked by the epigastric trocar. The inferior pancreatic border is freed to allow identification of the mesentericoportal vein and facilitate handling of the pancreas. The superior pancreatic border is freed, and lymphadenectomy of the hepatic artery and the celiac trunk is performed for lymph node picking and to facilitate identification of vessels. Once the borders of the pancreas have been clearly identified, the pancreas is easy to control at the neck and is sectioned with a stapler or more rarely with the Harmonic shears. If possible, elective ligation of the main pancreatic duct can be performed. The pancreas is freed from the splenic vessels and then sectioned to the left of the lesion. Although the lesion can be located by laparoscopic ultrasound, it should be mentioned that anatomical structures, such as the gastroduodenal artery on the right and the first curve of the splenic artery on the left, are important landmarks for small lesions. One-layer pancreatogastric (PG) anastomosis is performed. Omentoplasty with the great omentum can be performed to cover the dissected vessels (preventing bleeding) and to separate the two potential PF sites and facilitate postoperative management. Sites of potential PF are drained with two tubular drains and exteriorized through the lateral abdominal wall.
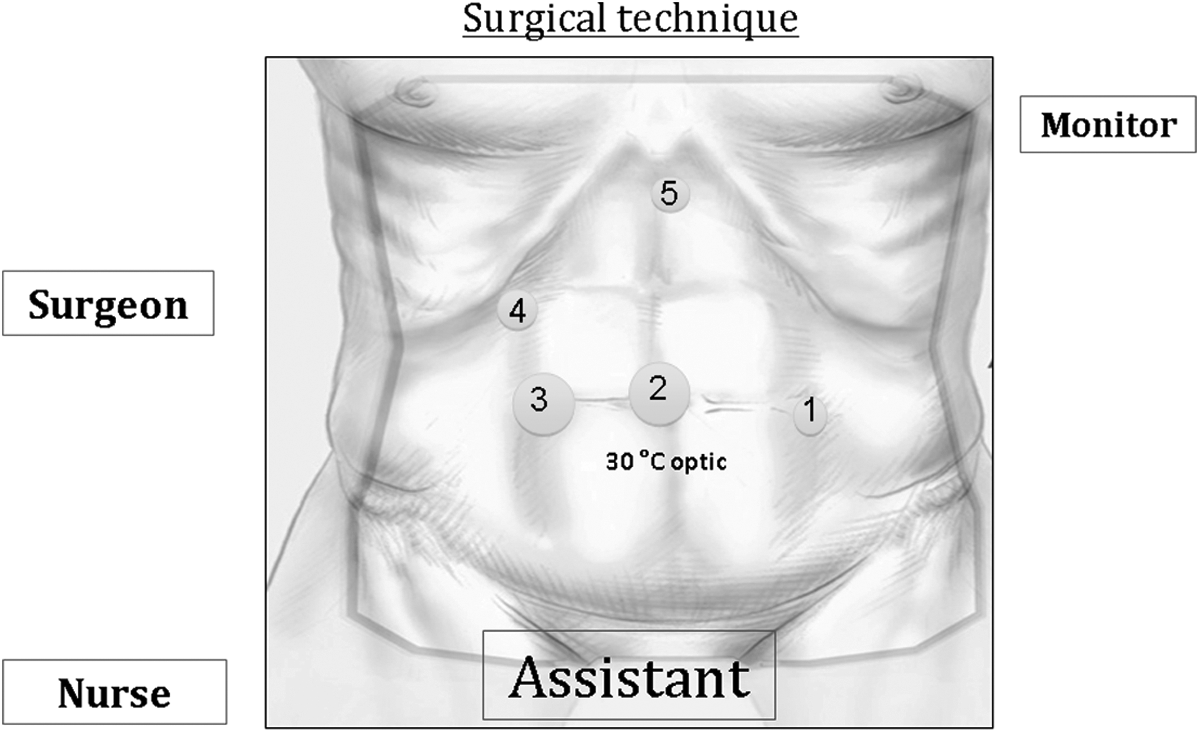
Open laparoscopy and five trocars were used for this procedure: trocars 1 and 2 for the assistant, trocars 3 and 4 for the surgeon, and trocar 5 for stomach traction. The specimen was removed by trocar 3, with or without enlargement.
Our case
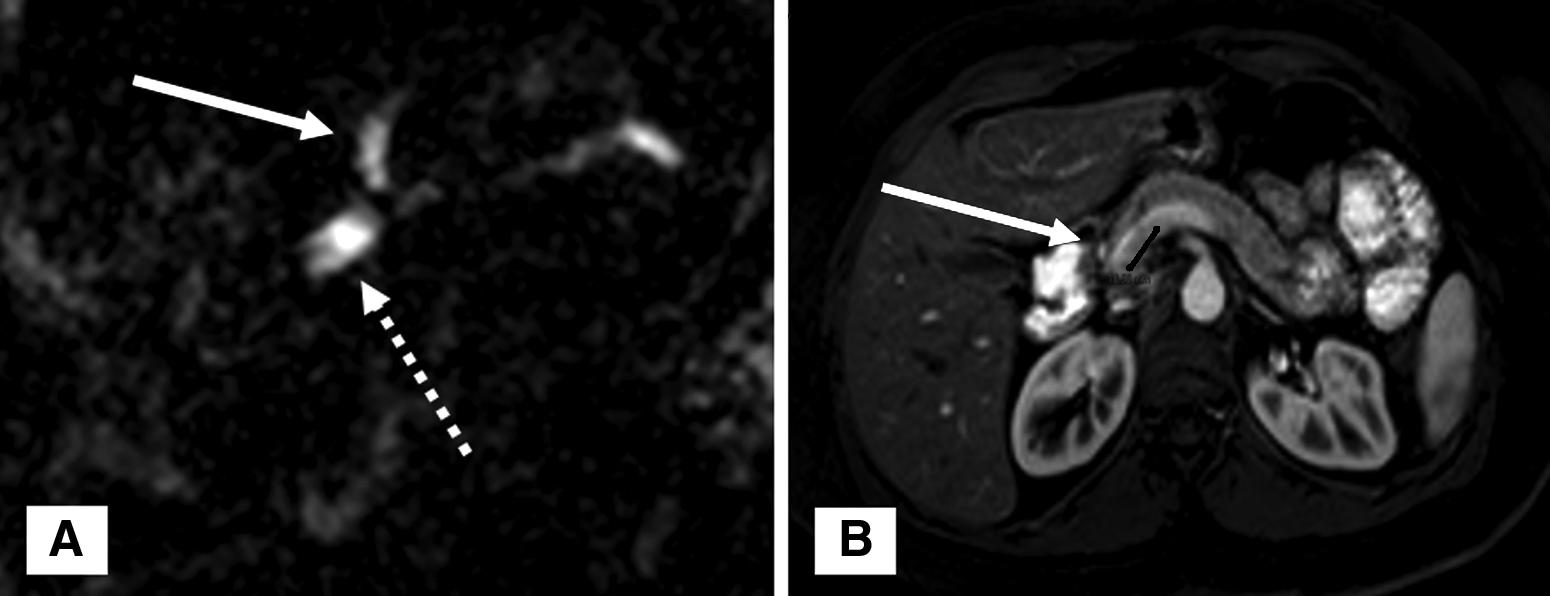
A 45-year-old woman was diagnosed with IPMN after numerous incidents of acute pancreatitis. She had no other medical or surgical history. She had presented with at least eight episodes of nonsevere acute pancreatitis since 2012. Blood tests showed elevated pancreatic but normal liver enzyme levels, and there were no gallbladder stones. The first endoscopic ultrasound identified a 1-cm cystic lesion in the pancreatic neck. The diagnosis of branch duct IPMN was suspected based on clinical results and the typical magnetic resonance imaging features, showing a small, irregular, cystic lesion communicating with the main pancreatic duct, which was moderately dilated at 5 mm (Fig. 2A). The lesion was located 2 cm to the left of the gastroduodenal artery, and LMP was decided on (Fig. 2B). Enucleation was contraindicated because the IPMN was deep and communicated largely with the main pancreatic duct, and histological involvement of the main pancreatic duct (mixed type) cannot be eliminated.
Results
Our case
LMP was successfully and safely performed. Surgery lasted 160 minutes, and there was 20 mL of blood loss. The frozen section showed negative margins on both sides. PG anastomosis was performed; a nasogastric tube was maintained for 1 week with parenteral nutrition. The postoperative course was uneventful, and the patient remained in the hospital for 15 days. On histology, the length of the resected specimen was 4 cm, and five negative lymph nodes were harvested. The presence of an 8-mm intestinal-subtype branch duct IPMN with moderate dysplasia and negative margins was confirmed. The patient is symptom free 6 months after surgery.
Our experience
Between April 2011 and May 2014, among 217 patients who had laparoscopic pancreatic resection in our department, 21 underwent LMP, including 15 women (71%). Mean age was 45 (range, 17–75) years, and the mean body mass index was 26 (range, 22–32) kg/m2. The laparoscopic approach was proposed to 21 of 22 patients who were candidates for MP (laparoscopic feasibility rate=95%). The main indications were neuroendocrine tumors (n=8), IPMN (n=6), solid and cystic pseudopapillary tumors (n=3), mucinous cystadenoma (n=2), and other (n=2). Surgery lasted a median of 191 (range, 120–285) minutes, and the mean blood loss was 145 (range, 10–800) mL. Conversion was necessary in 1 patient (5%). There were no mortalities. Complications occurred in 15 (71%) patients, including mainly PF (57%), bleeding in 2 cases (9%), and re-intervention in 3 cases (14%). On histology, the mean length of the resected specimen was 5 (range, 3.5–8.5) cm, the mean number of harvested lymph nodes was 2.4 (range, 0–6), and resection was R0 in 95%. The mean hospital stay was 17 (range, 14–54) days. After a mean follow-up of 23 (range, 2–34) months, all patients were still alive, there was no tumor relapse, and only 1 patient developed upper limit glycemia (5%). Two patients had an asymptomatic incisional hernia, and 1 patient had stenosis of the PG anastomosis with pancreatic gland atrophy.
Discussion
With the rapid and widespread use of laparoscopy, low-potential and benign pancreatic diseases become ideal candidates for laparoscopic parenchyma-sparing pancreatectomy resections. We believe that LMP should be promoted compared with other types of pancreatic resection; most MP candidates can theoretically benefit from the laparoscopic approach because there are few technical or oncological contraindications. The PG is most frequently used for reconstruction, but pancreatojejunal anastomosis had also been described.15,17 We believe that there is no need to prolong operative time with a Roux-en-Y pancreatojejunal anastomosis, especially when randomized controlled trials have not shown that pancreatojejunal is better than PG anastomosis in the case of pancreatoduodenectomy.18–20
In our experience and compared with other studies, the shorter operative time (191 minutes versus 225–480 minutes)11–13,15 and the low rate of conversion (5% versus 17%–22%)11,12 are probably related to our experience with the laparoscopic approach and familiarity with this procedure. We recently published our experience with 100 cases of MP performed over a period of 12 years, 21 mainly performed by the open approach. There are very few larges series on LMP,11–15 and it is difficult to draw conclusions on morbidity because of the retrospective design of these studies and the nonstandardized definition of PF. No mortalities have been reported. In our experience, the postoperative outcome after open MP and LMP was similar for mortality, overall morbidity, and PF: 3%, 72%, and 44% and 0%, 71%, and 57%, respectively. The cosmetic advantages of the laparoscopic approach should not be underestimated because in our experience most patients were young women.
Conclusions
LMP is a safe procedure for nonmalignant pancreatic diseases, and the postoperative outcome is comparable to that of the open approach. This technique can be standardized because most candidates for MP can theoretically benefit from the laparoscopic approach.
Footnotes
Disclosure Statement
No competing financial interests exist.