
Abstract
Abstract
Background:
The length of incisions on the abdominal wall directly correlates with wound-related morbidities and patient comfort. Both mini-laparoscopy (only ≤5-mm trocars) and natural orifice specimen extraction avoid larger abdominal incisions. This study described a new natural orifice translumenal endoscopic surgery (NOTES®; American Society for Gastrointestinal Endoscopy [Oak Brook, IL] and Society of American Gastrointestinal and Endoscopic Surgeons [Los Angeles, CA]) cholecystectomy technique by combination of these two advanced laparoscopic techniques for cholelithiasis in patients who had prior laparoscopic Roux-en-Y gastric bypass (LRYGB) for obesity.
Patients and Methods:
Three patients (two males, one female; 39, 62, and 34 years old, respectively) were admitted with symptomatic cholelithiasis (multiple millimeter-sized gallstones), and all had previously had LRYGB. They were treated by mini-laparoscopic cholecystectomy using three 5-mm trocars. The gallbladder was removed through the dilated efferent limb of the jejunum, 5 cm distal from the gastrojejunostomy. Transjejunal extraction was performed under endoscopic guidance. The gallbladder in the jejenum was passed through the anastomosis and extracted with an endoscopic snare by the transoral way. The enterotomy was closed intracorporeally.
Results:
There was no conversion or additional trocar requirement. All the procedures were completed successfully without problems. Respective operating times were 95, 75, and 120 minutes. Only 1 patient required postoperative analgesic; the others did not. The patients started to get a liquid diet on the night of surgery and were discharged on Days 1, 1, and 2, respectively, with normal diet recommendations. There were no morbidities.
Conclusions:
Mini-laparoscopic cholecystectomy is technically feasible in patients with previous LRYGB. Prior LRYGB was not an obstacle for transoral specimen extraction. The dilated efferent jejunal limb is a good alternative route for natural orifice specimen extraction. This report described the first natural orifice surgery through the small bowel.
Introduction
T
Natural orifice translumenal endoscopic surgery (NOTES®; American Society for Gastrointestinal Endoscopy [Oak Brook, IL] and Society of American Gastrointestinal and Endoscopic Surgeons [Los Angeles, CA]), which is modified from laparoscopic surgery, reduces the number of ports and does not produce any visible surgical scar. So, in theory it has some advantages such as less postoperative pain, low hernia risk, and faster recovery.4,5
Combination of both advanced laparoscopic techniques can provide a better postoperative recovery. 6 Here, we aimed to describe a mini-laparoscopic cholecystectomy and transjejunal specimen extraction in a special group of patients who had previous LRYGB.
Surgical Technique and Results
We received our institutional board ethical review for natural orifice surgery. The details of this novel technique were explained to the patients, and the appropriate consent was obtained.
We did not perform preoperative upper gastrointestinal endoscopy because there was no symptom of anastomotic stricture. We planned an intraoperative endoscopic dilatation if there was an asymptomatic anastomotic stricture.
An antibiotic (second-generation cephalosporin) and deep vein thrombosis prophylaxis were administered. The patients were placed in the French position. Pneumoperitoneum was created via a Veress needle from the left subcostal area.
Three abdominal trocars, all 5 mm in diameter, were inserted into the umbilicus and right and left upper quadrants, respectively. These trocar sites were appropriate to access both the gallbladder and the jejunum. Abdominal exploration was conducted by a 5-mm rigid 30° laparoscope through the umbilicus. A Harmonic® scalpel (Ethicon Endo Surgery, Cincinnati, OH) was used for dissections. There were a few adhesions around the gallbladder, and following minor adhesiolysis, a standard three-port laparoscopic cholecystectomy was performed. There were more adhesions around the gastroenterostomy, which was usually overlapped by the left liver lobe. We did not try to find either the gastric pouch or to mobilize the left liver lobe. The dilated efferent jejunal limb was always coming from beneath the left liver lobe.
At this stage we performed an endoscopy. The endoscope was introduced into the gastric pouch, passed the gastrojejunostomy, and advanced in the jejunum. We confirmed that there was no stricture at the anastomosis. We also confirmed whether we found the correct efferent jejunal limb or not. When the endoscope was advanced in the efferent limb, at 5 cm distal to the gastrojejunostomy, the light of the endoscope was seen on laparoscopy (Fig. 1). The efferent jejunal limb was always dilated. A 2-cm vertical enterotomy was made with endoscopic scissors under the guidance of endoscopy (Fig. 2). The gallbladder was taken into the jejunum with assistance of an endoscopic snare (Fig. 3) and removed transorally (Fig. 4). The enterotomy was closed intracorporeally as a double layer with a running suture. Neither abdominal drains nor fascial suturing was used.

Laparoscopic view of the transillumination of the endoscopic light in the proximal jejunum.
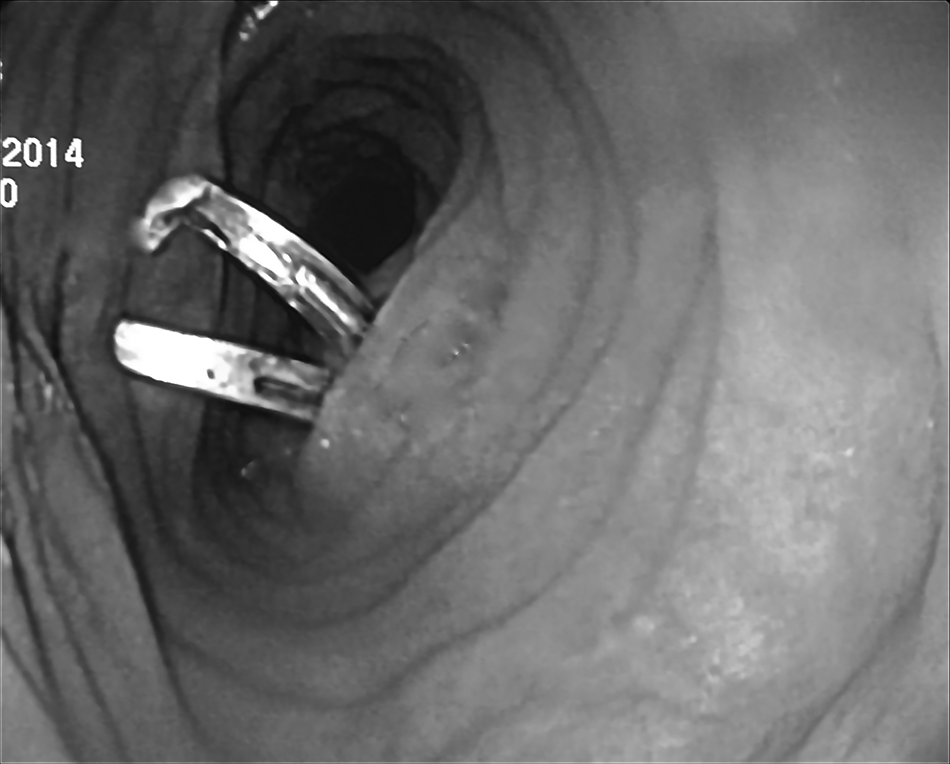
Endoscopic view of the laparoscopic enterotomy.

Pulling the gallbladder into the jejunum with the endoscopic snare.

Transoral extraction of the gallbladder.
Patients' characteristics and the results are summarized in Table 1.
We waited to perform laparoscopic cholecystectomy until at least 2 months after biliary colic symptoms.
ASA, American Society of Anesthesiologists; RYGB, Roux-n-Y gastric bypass; VAS, visual analog scale at 24 hours.
Discussion
Here, we described a novel NOTES cholecystectomy technique in a special group of patients. We combined the mini-laparoscopy technique with natural orifice surgery to reduce the abdominal wall trauma due to large trocars or incision enlargements for specimen extractions. The potential advantages of this combination are less visible scars, very low risk of incisional hernia, faster recovery, and less postoperative pain.
NOTES uses natural orifices such as the mouth, anus, or vagina to reach inside the abdomen to perform surgery. Transvaginal cholecystectomy is one of the most well-known NOTES procedures and possibly the most studied one.7,8 In addition to cholecystectomy, the transvaginal route can be used for appendectomy, colorectal resection, nephrectomy, sleeve gastrectomy, liver surgery, or incisional hernia repair.7–11 The transanal route is used only for colorectal resections, and the transgastric route is mainly limited to cholecystectomy and appendectomy.7,8,12 Here, we described three NOTES cholecystectomies through the jejunum, and to the best of our knowledge the small bowel as an access point for NOTES approaches has not been reported yet.
It is well known that previous abdominal surgery can make laparoscopic cholecystectomy more complicated and more prone to conversion to open surgery. 13 If the prior abdominal surgery is laparoscopic, then laparoscopic cholecystectomy may not be so difficult. Swartz and Felix 14 reported a 4.2% complication rate for laparoscopic cholecystectomies performed after LRYGB. In our cases we did not find any massive adhesions at the upper right quadrant of the abdomen or around the gallbladders. There was no difficulty during our three-port mini-laparoscopic cholecystectomies, and no additional trocar or converison was required.
Opening of a hollow viscus is the main drawback of natural orifice surgery. Previously Jurczak and Pousset 15 reported mini-laparoscopic cholecystectomy and transgastric specimen extraction via three or four trocars in 63 patients. They found no gastric or abdominal wall complications but some difficulties with gallbladder removal through the esophagus only in cases of acute cholecystitis with thickened walls or with gallstones that were larger than 3 cm. None of our patients had acute cholecystitis or large gallstones, and we removed the gallbladders without difficulty in the first 2 cases. In the last case, the distended gallbladder did not pass the esophagogastric junction, and we evacuated it before extraction with the help of an endoscopic hook cautery and suction device.
Opening the small bowel for NOTES can increase potential complications such as infection, leak, or small bowel stricture. Recently, the IRCAD group reported a peritoneal contamination rate of 100% in transanal extraction of 16 sigmoidectomies for diverticulitis; however, none of their cases resulted in clinically significant peritoneal infection despite contamination. 16 Clearly, small bowel opening can cause some peritoneal contamination, but this did not translate into infectious morbidities in our patients, and we believe that our contamination risk was lower than with colorectal procedures. In our Roux-en-Y gastric bypass (RYGB) experience, the incidence of leak from the gastrojejunostomy was low (4/500 [0.8%]). Our patients with gastrojejunostomy leaks demonstrated smooth postoperative courses and did not require any intervention. The alimentary limb in RYGB does not include bile or pancreatic enzymes, and this provides a better management of gastrojejunostomy leaks after RYGB. These experiences also encouraged us to use the efferent limb of RYGB for NOTES. Small bowel stricture after closing the enterotomy is not a risk for a dilated efferent jejunal limb in RYGB.
In conclusion, mini-laparoscopic cholecystectomy is technically feasible in patients with previous LRYGB. Prior LRYGB surgery was not an obstacle for natural orifice specimen extraction. The dilated efferent jejunal loop is an alternative route for specimen extraction. To the best of our knowledge, the jejenum has been used as a natural orifice specimen extraction port for the first time in this report.
Footnotes
Disclosure Statement
No competing financial interests.