
Abstract
Abstract
Objective:
To assess whether pubovesical complex (PVC) reconstruction (termed Kim's stitch) improves urinary continence following robot-assisted laparoscopic prostatectomy (RALP).
Patients and Methods:
The cohort consisted of 130 consecutive patients who underwent RALP in a tertiary-care hospital between July 2012 and June 2013. The first 70 patients did not undergo PVC reconstruction with Kim's stitch and formed the control group. The subsequent 60 patients underwent Kim's stitch and formed the intervention (Kim's stitch) group. The primary outcome measure was degree of urinary continence assessed 1, 3, and 6 months after surgery using the Expanded Prostate Cancer Index Composite Questionnaire. Continence was compared between the two groups using propensity scores and inverse-probability weighting to adjust for treatment selection bias. To evaluate adverse treatment effects, all patients underwent uroflowmetry before and 1 month after surgery.
Results:
The prevalence of continence at 1, 3, and 6 months was 23.9%, 57.7%, and 77.6%, respectively, in the control group and 25.9%, 60.0%, and 89.7%, respectively, in the Kim's stitch group. After adjustment, the 6-month continence was different between the two groups (odds ratio = 2.25; 95% confidence interval, 0.91–5.55; P = .08). The 1- and 3-month continence rates and postoperative maximal urinary flow rate were similar between the two groups (Kim's stitch group, 21.5 ± 9.5; control group, 22.1 ± 8.6; P = .72).
Conclusions:
A PVC reconstruction (Kim's stitch) with posterior reconstruction during RALP has a beneficial effect on continence recovery without producing additional adverse effects.
Introduction
R
However, urinary incontinence after RALP is still a devastating and relatively common complication that is associated with a significant deterioration in quality of life. To improve continence after RALP, several technical modifications have been described, for example bladder neck preservation, 4 intussusception of the bladder neck, 5 and posterior reconstruction (PR) of the rhabdomyosphincter.6–9 Two large studies published in 2007 showed that these advances in surgical techniques have greatly improved the 1-year continence rates after RALP.10,11 Despite these improvements, the early recovery of continence remains relatively infrequent and continues to have a major impact on patient health-related quality of life.12,13 Additional technical modifications, such as puboprostatic ligament sparing or reconstruction,14–16 have also failed to increase postoperative continence rates significantly. 16
Recently, Asimakopoulos et al. 17 introduced the pubovesical complex (PVC) sparing technique in RALP. The procedure preserves the PVC by separating the detrusor apron (DA) containing the pubovesical ligaments from the anterior surface of the prostate instead of dividing the PVC at the prostate–urethral junction. Furthermore, this approach is effective for improving early continence outcomes.17,18 However, this procedure is technically difficult because the bladder neck is approached laterally, and extensive experience is required to perform the procedure safely. For this reason, we performed PVC reconstruction after urethrovesical anastomosis instead of preserving the PVC. To our knowledge, this PVC reconstruction technique during RALP has not been described previously. Here, we described our PVC reconstruction technique during RALP, also referred to as Kim's stitch, and assessed its safety and impact on urinary continence.
Materials and Methods
Subjects consisted of all consecutive patients with prostate cancer who underwent RALP at our institute between July 2012 and June 2013. All patients had clinical disease stage T3 or less and no evidence of metastasis because these were the eligibility criteria for RALP at our hospital. In total, 130 patients underwent RALP during the study period. The first 70 patients did not undergo PVC reconstruction and formed the control group. The subsequent 60 patients underwent PVC reconstruction with Kim's stitch and formed the intervention (Kim's stitch) group. All of the surgical procedures were performed by a single surgeon (C.-S.K.), who had performed 700 previous RALP procedures. The characteristics of the 130 patients who were included in the study are shown in Table 1. This study was approved by the Institutional Ethics Committee/Review Board of the Asan Medical Center, Seoul, Korea.
The sum of the scores of the first 7 items.
BMI, body mass index; EPIC, Expanded Prostate Cancer Index Composite; IPSS, International Prostate Symptom Score; MUL, membranous urethral length; NVB, neurovascular bundle; PSA, prostate-specific antigen; SD, standard deviation.
The continence outcomes of the two groups were assessed 1, 3, and 6 months after the surgery using the Expanded Prostate Cancer Index Composite (EPIC) questionnaire. 19 Continence was defined based on patient responses to three questionnaire items that identified the range of incontinence severity: “Over the past 4 weeks, how often have you leaked urine?,” “How many pads or adult diapers per day did you usually use to control leakage during the last 4 weeks?,” and “Which of the following best describes your urinary control during the last 4 weeks?” 19 Continence was defined by satisfying at least two of the following conditions: no pads, no leakage, and total urinary control. Potency was also assessed before and 6 months after surgery using the EPIC Questionnaire-Sexual domain. This questionnaire comprised nine items, and the sum of the first seven items was used to compile the patient's score.
To assess adverse events associated with surgery, uroflowmetry was performed before and 1 month after surgery.
Surgical technique
In all cases, the transperitoneal, six-port technique described by Menon and Tewari 20 and Tewari et al. 21 was used with a few minor alterations. To enter the retropubic space of Retzius, the anterior peritoneum was incised. The endopelvic fascia was opened bilaterally just lateral to the reflection of the puboprostatic ligaments, and the levator muscle fibers were taken off the prostate until the dorsal vein complex (DVC) and urethra were visualized. The DVC was ligated at the prostatourethral junction. All patients underwent limited pelvic lymphadenectomy. The neurovascular bundles were preserved depending on the patient's requests, the potency status before RALP, and the Gleason scores, clinical stage, and intraoperative assessment of the gland. PR was performed in all cases using a polyglactin absorbable suture passed through the Denonvilliers' fascia at the posterior wall of the bladder as described by Rocco et al.6,7
Vesicourethral anastomosis was performed using a continuous running suture with two-tied poliglecaprone 25 (Monocryl™; Ethicon, Somerville, NJ) sutures. 22
The only difference between the Kim's stitch and control groups was the placement of the anterior stitch after the anastomosis, described as follows (Fig. 1). In the Kim's stitch group, PVC reconstruction was performed using a 3-0 polyglactin suture, which was approximately 1.5 cm long and was placed longitudinally from the left side of the DVC/rhabdosphincter to the left side of the DA (Fig. 1b). The needle was then passed again above and through the opposite side of the DA to the DVC/rhabdosphincter in a U-shape (Fig. 1c). The suture was then tied with firm tension (Fig. 1d). All patients underwent cystography on the fifth postoperative day to investigate urinary leakage. The urethral catheter was removed 5–7 days after the procedure.
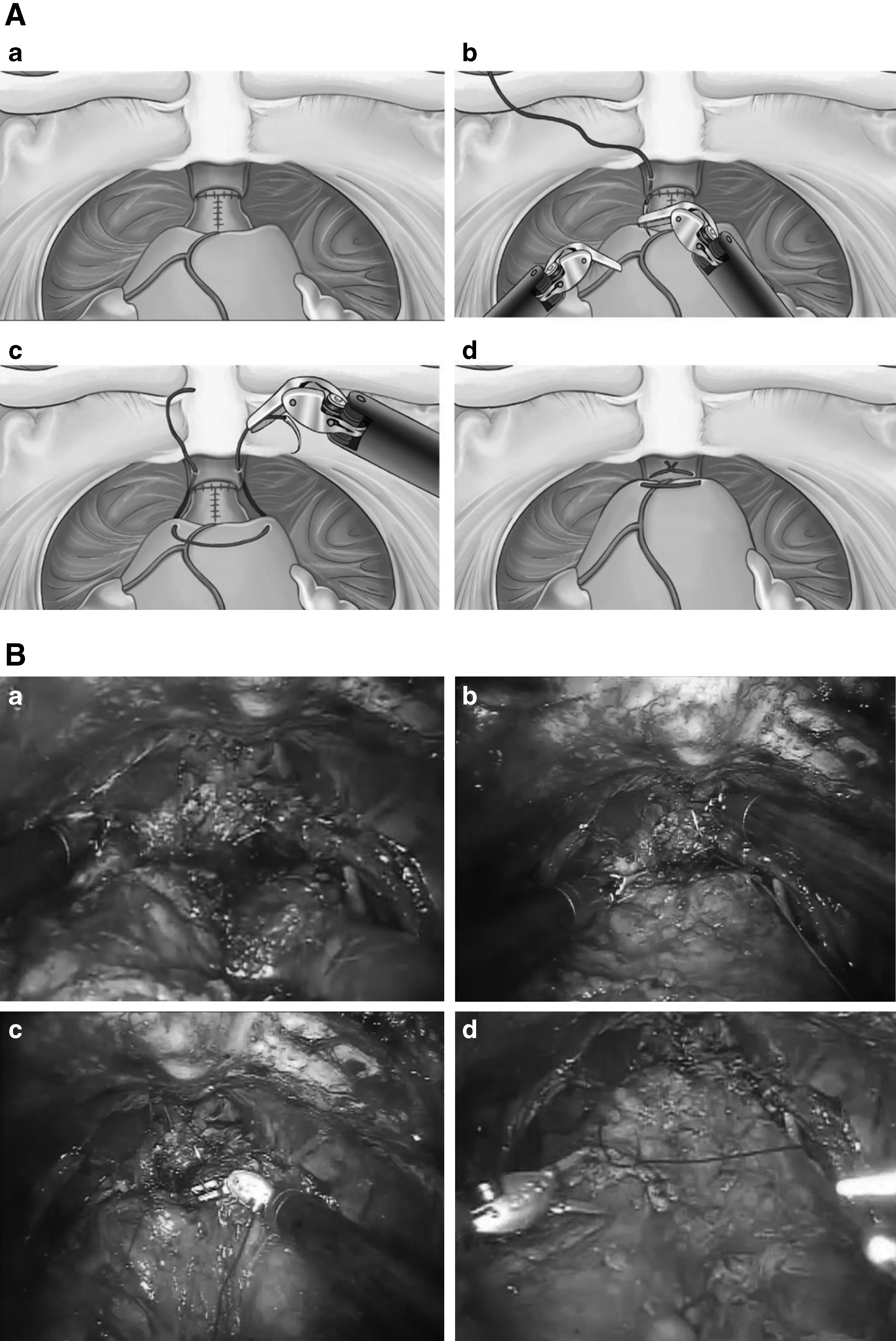
Pubovesical complex reconstruction:
Statistical analysis
Categorical variables were presented as frequencies and percentages, and continuous variables were expressed as mean ± standard deviation values. Categorical variables were compared between the two groups using the chi-squared test or Fisher's exact test, and continuous variables were compared using Student's t test. To reduce the effect of treatment selection bias and potential confounding, differences in baseline characteristics were adjusted for using weighted multivariate logistic regression models and inverse probability of treatment weighting. In the latter technique, the weighting of the Kim's stitch patients was equal to the inverse of (1 – propensity score), whereas the weighting of the control patients was equal to the inverse of the propensity score. Propensity scores were estimated using multivariate logistic regression analysis without regard to outcome variables. All reported P values were two-sided, and a value of P < .05 was considered to indicate statistical significance. SAS version 9.1 (SAS Institute, Cary, NC) and SPSS version 18 (IBM, Armonk, NY) software were used for statistical analyses.
Results
Baseline characteristics (Table 1) and operative time, blood transfusion rate, catheterization time, and urinary complications (Table 2) were not significantly different between the Kim's stitch and control groups. None of the patients had symptoms of urinary incontinence before RALP, and neither group had intraoperative complications during RALP or significant postoperative morbidity related to the PVC reconstruction technique. In the control group, 1 patient presented with acute urinary retention after catheter removal that resolved after the in-dwelling catheter was replaced and left in for another 3 days.
SD, standard deviation.
The two groups did not differ significantly in terms of pathological stage, frequency of positive surgical margins, Gleason score of the surgical specimen, or potency outcomes (Table 3). All 130 patients completed the EPIC questionnaires 1, 3, and 6 months after surgery. The continence rates at 1, 3, and 6 months after surgery were 25.9%, 60.0%, and 89.7%, respectively, in the Kim's stitch group and 23.9%, 57.7%, and 77.6%, respectively, in the control group. The prevalence of continence at 6 months tended to be higher in the patients who underwent the PVC reconstruction technique than in those who did not (odds ratio [OR] = 2.50, 95% confidence intervals [CI], 0.90–6.95; P = .08). However, the 1- and 3-month continence rates did not differ between the two groups (Table 4). The mean maximal urinary flow rates before surgery (17.6 ± 8.7 mL/second versus 15.4 ± 7.3 mL/second; P = .14) and 1 month after surgery (21.5 ± 9.5 mL/second versus 22.1 ± 8.6 mL/second; P = .72) (Fig. 2) did not differ significantly between the Kim's stitch and control groups.
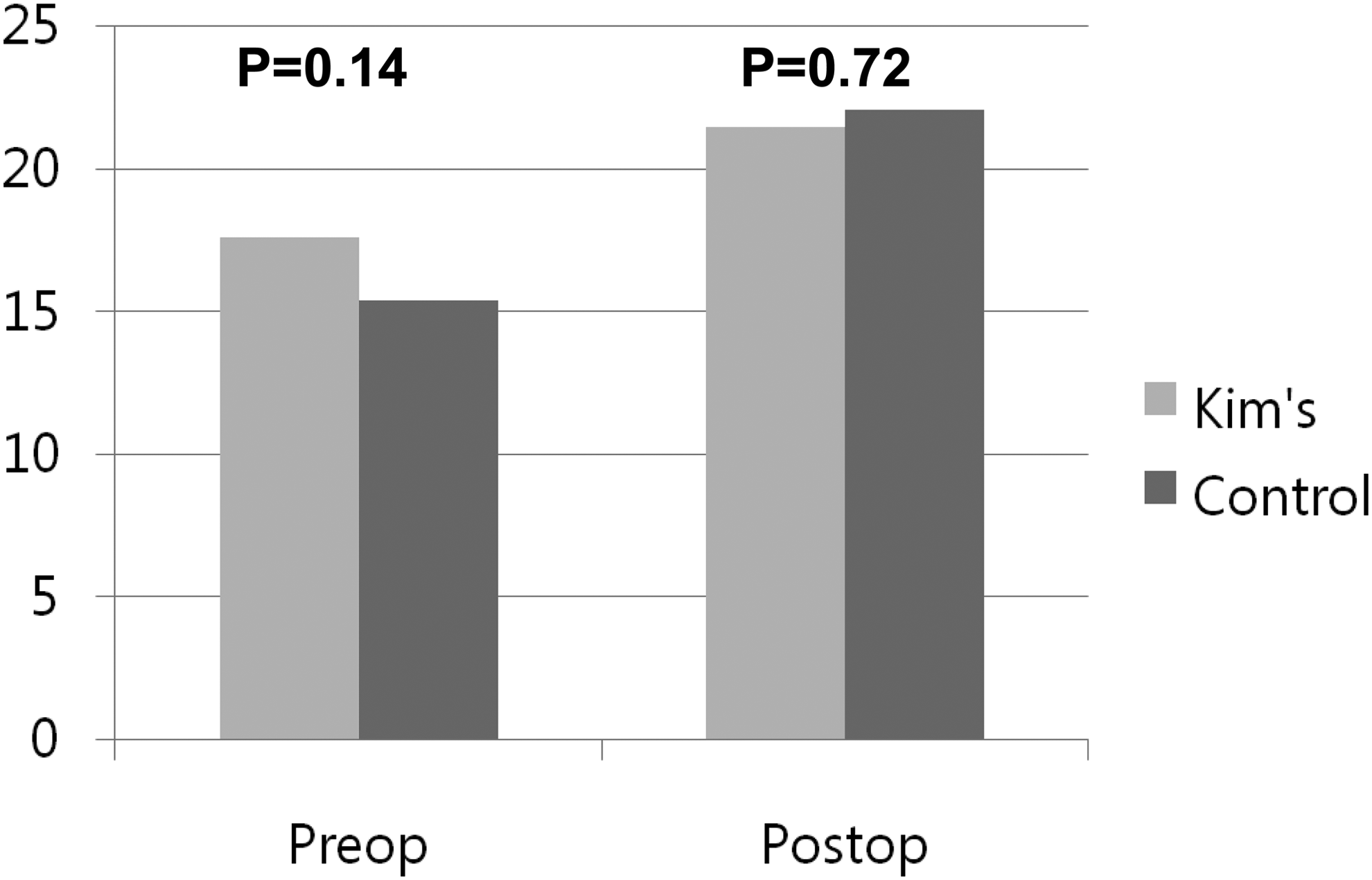
Comparison of maximal urinary flow rate between the Kim's stitch and control groups.
The sum of the scores of the first 7 items.
EPIC, Expanded Prostate Cancer Index Composite; PSM, positive surgical margin; SD, standard deviation.
CI, confidence interval; IPTW, inverse probability of treatment weighting; OR, odds ratio.
Multivariate logistic regression analysis revealed that age (by 1 year: OR = 0.91; 95% CI. 0.85–0.97; P = .004) and prostate volume (by 1 mL: OR = 0.97; 95% CI, 0.94–1.00; P = .048) were significant and independent predictors of early continence recovery. However, International Prostate Symptom Score, membranous urethral length, body mass index, neurovascular bundle sparing, and the morphology of the prostate apex were not predictors of continence recovery (Table 5).
BMI, body mass index; IPSS, International Prostate Symptom Score; MUL, membranous urethral length; NVB, neurovascular bundle; PVC, pubovesical complex.
Discussion
Two studies on patients who underwent radical prostatectomy show that according to health-related quality of life, post–radical prostatectomy urinary incontinence has a great deterioration in quality of life.12,23 Consequently, some surgical techniques have been developed to improve the early return of continence after RRP. For example, PR of the rhabdomyosphincter, first described by Rocco et al., 6 improved the continence of patients 1 and 3 months after RRP (P < .05).
Several reports have also indicated that preservation of the puboprostatic ligament improves continence outcomes after RRP.16,24,25 Moreover, preservation of the puboperinealis muscle and arcus tendineus may improve the continence rate after RALP.26,27 Asimakopoulos et al. 17 were the first to describe the effects of a PVC-sparing technique on continence in RALP, indicating that the preservation of the puboprostatic ligaments is difficult because of their anatomical continuity with the bladder. To expose the pubourethral junction during RALP, these pubovesical ligaments must be interrupted at some point. To achieve this, the investigators performed a PVC-sparing procedure using the atraumatic grasper to pull away the DA and adequately expose the prostate–urethral junction. The prostate is then shelled out from below the overlying PVC, and urethrovesical anastomosis is carried out under the preserved complex. After this procedure, 80% of the patients were dry (0 pads), and the remaining 20% only required one security pad after catheter removal, thus indicating that PVC sparing may improve early continence outcomes. However, although this technique is feasible, it is generally difficult to perform and may increase the risk of anterior positive surgical margins. 18
Most of the procedures performed during RALP in the current study were identical to those performed in previous RALP techniques up to the urethrovesical anastomosis, at which point we placed a simple stitch on the anterior perivesical structure between the DA and DVC to reconstruct the PVC. Unlike puboprostatoplasty, which involved reattachment of the arcus tendineus to the lateral aspect of the bladder neck, our PVC reconstruction involved attaching the distal DVC to the proximal DA, which was located in the anterior portion of the bladder. Furthermore, we did not preserve the puboprostatic ligament, and we did not use a suspension technique. Addition of the stitch tended to improve 6-month continence more than in the control group that did not receive the stitch. However, maximal urinary flow rate and the 1- and 3-month continence rates were similar between the groups. Moreover, none of the patients who underwent PVC reconstruction showed acute urinary retention after catheter removal, indicating that the procedure is relatively safe. The exact mechanism by which PVC reconstruction improves the recovery of continence is unclear, although it may provide additional anterior support to the striated sphincter, which stabilizes the posterior urethra in its normal place in the pelvic floor.
The causes of urinary incontinence following radical prostatectomy are multifactorial. Continence after RALP is affected by both the surgical technique and the patient's characteristics. Atrophy of the rhabdomyosphincter and neural degeneration are more likely in aging patients, and thus patient age is a significant predictor of continence. 28 Greco et al. 29 showed that the older men treated with RALP had significantly lower continence rates 6 months after surgery than the younger men who underwent the procedure, although the continence rates after 12 months were similar between younger and older men. These reports suggest that age is associated with early continence outcomes but has no effect on long-term continence. Our study also found that fewer older-aged patients had early continence. These findings will aid the counseling of older men who are undergoing RALP.
Study limitations
The most important limitation of the study was that the patients were not randomized to the two groups. However, the patient characteristics were similar between the two groups, and differences in baseline demographic and clinical characteristics were adjusted for in the multivariate analyses used to investigate independent predictors of early urinary continence after RALP. Another limitation of the present study was that it only included the patients who underwent RALP performed by a single surgeon. However, the surgeon was highly experienced (>700 RALP procedures). Furthermore, two different technical variations, namely, Kim's stitch and the nerve-sparing procedure, were used in some but not all of the patients during the standard RALP procedure. In addition, all patients underwent PR of the rhabdomyosphincter. Thus, these techniques may have had a synergistic effect on continence recovery, which makes it difficult to quantify the contribution of each technique to the improvement in continence. However, the nerve-sparing technique did not predict the recovery of continence, suggesting that our results were not affected by synergistic effects of the two techniques.
Conclusions
PVC reconstruction (Kim's stitch) with a PR during RALP showed beneficial effects on continence recovery while providing additional anterior support. Moreover, restoration of the PVC is technically simpler than the puboprostatoplasty or the PVC-sparing technique.
Footnotes
Disclosure Statement
No competing financial interests exist.