
Abstract
Abstract
Intramural esophageal dissection (IED) is a rare disease characterized by a partial (PIED) or circumferential (CIED) mucosal rupture. Whereas PIED responds well to nonoperative treatment, complicated courses have been reported necessitating surgery, up to the point of esophagectomy despite complex endoscopic interventions, in CIED. We report the first case of an iatrogenic CIED with perforation in a young patient with underlying eosinophilic esophagitis treated successfully by endoscopy alone, using a partially covered self-expandable metal stent.
Introduction
I
In this article we report a CIED with perforation treated successfully by endoscopic placement of a PSEMS in a young patient with EoE.
Case Report
A 43-year-old man underwent esophagogastroscopy (EGD) in a community hospital because to gastroesophageal reflux disease symptoms with dysphagia. During EGD, mucosal dissection with perforation occurred. Computed tomography showed mediastinal and subcutaneous emphysema of the neck and a double barrel sign of the esophagus (Fig. 1A).
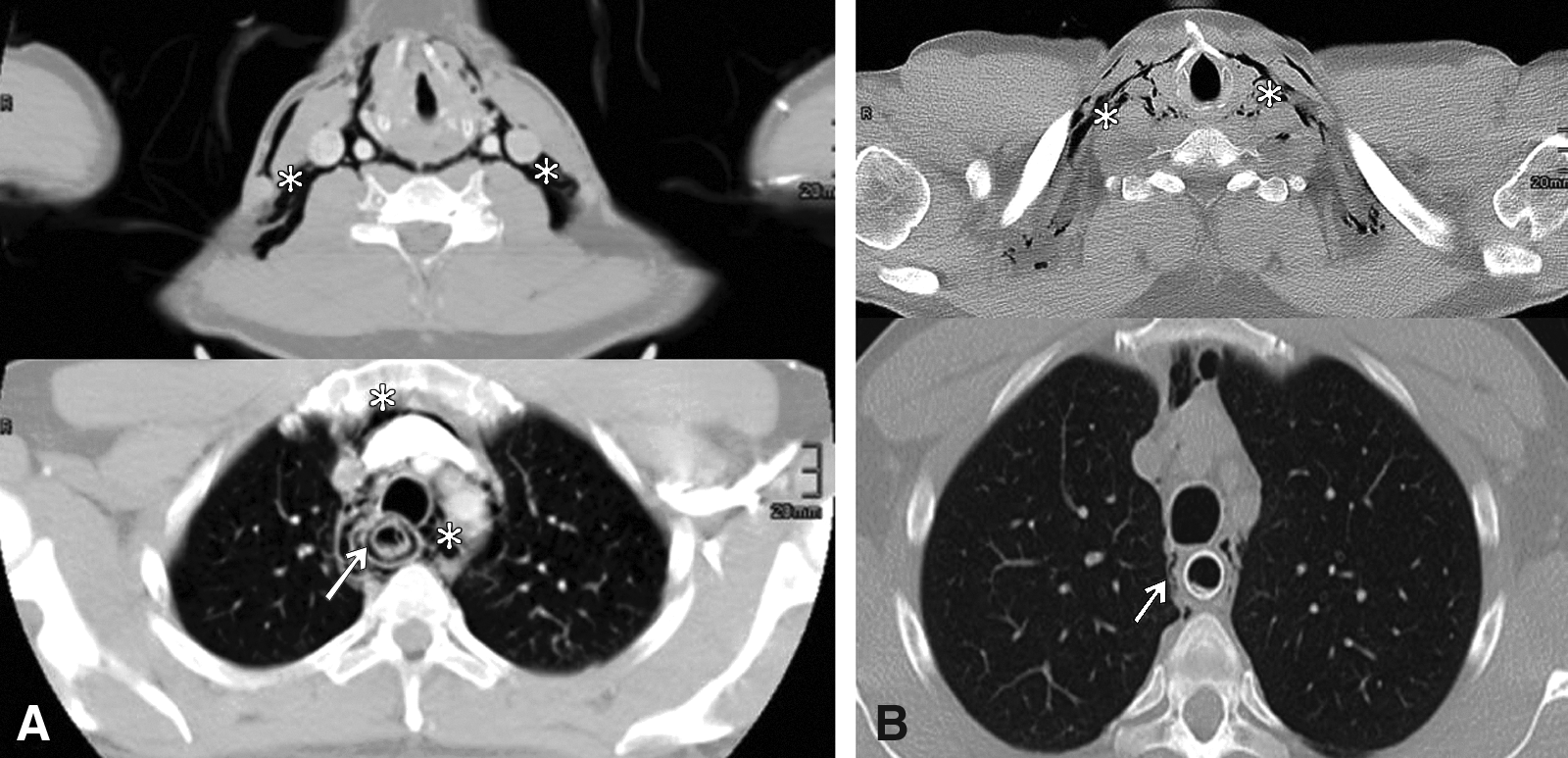
Computed tomography scan with esophageal intramural dissection.
Transferred to our institution, the patient complained about thoracic pain and the impossibility of swallowing. EGD with the patient under general anesthesia revealed signs of EoE in terms of red furrows and corrugated rings. Twenty-five centimeters from the incisors, there was an abrupt circumferential rupture of the regular squamous epithelium. A false lumen of about 5 cm in length ended in a cul-de-sac. The true lumen was visible as a white line corresponding to the collapsed mucosal tube (Fig. 2). There was no evidence of frank perforation, but a permeable muscle layer in combination with the immense mediastinal emphysema was interpreted as a small perforation. Intubation of the true lumen succeeded using a guidewire (Nitrex®; EV3, Plymouth, MN) (Fig. 3). The endoscope could be introduced into the stomach. A PSEMS (80 mm in length, 20/26-mm shaft/flairs; Leufen Medical GmbH, Aachen, Germany) was placed, covering the whole dissected mucosal tube. Additionally, a jejunal feeding tube was placed (Fig. 4). Broad-spectrum antibiotics (5 days of tazobactam/piperacillin) and proton-pump inhibitor (pantoprazole; 3×40 mg) were administered.

Endoscopic view into the false lumen ending in a cul-de-sac (asterisk). The flat white line (arrows) at the left side of the false lumen corresponds to the collapsed mucosal tube.
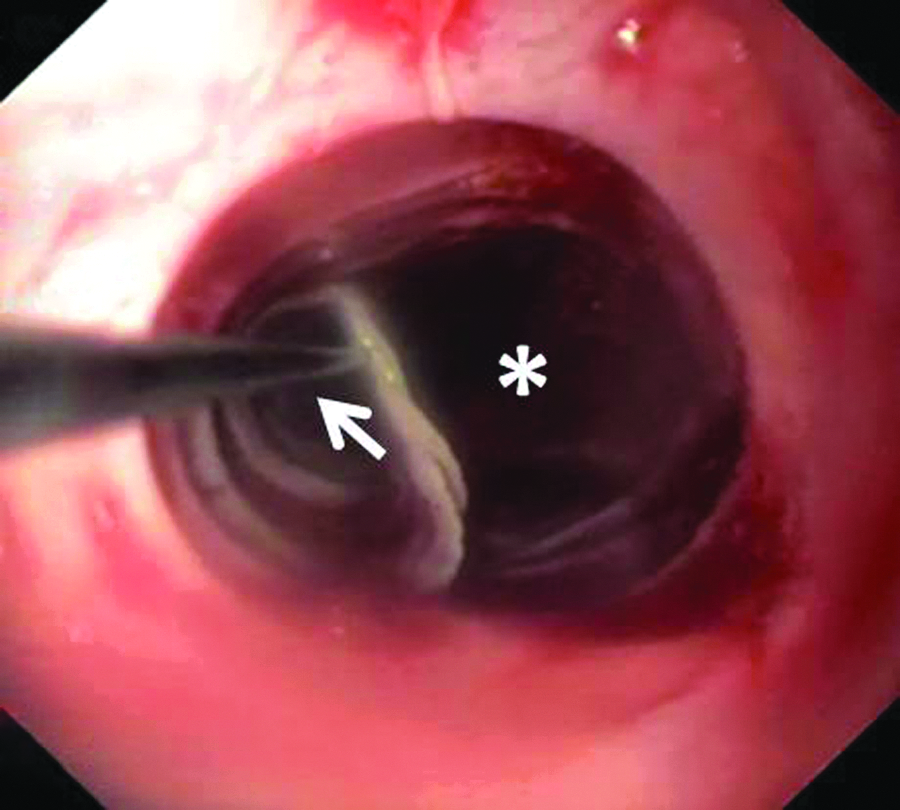
Endoscopic view into the false (asterisk) and proper lumen. Intubation of the latter was possible assisted by a guidewire (arrow).

Chest X-ray showing the released partially covered self-expandable metal stent and the jejunal feeding tube (arrow). In addition, the radiopaque metal marker is seen indicating the intramural dissection 25 cm from the incisors (asterisk).
Computed tomography on Day 2 showed a regression of the mediastinal emphysema (Fig. 1B). Oral intake was allowed. The patient was discharged on Day 6.
Stent extraction was uncomplicated 14 days later. No mucosal injury occurred (Fig. 5A). The CIED was healed. At follow-up after 8 weeks of therapy with proton-pump inhibitors, EGD did not show stenosis (Fig. 5B), but there were persisting signs of EoE in the biopsy specimens (30 eosinophils/high-power field). Long-term treatment with oral budesonide was initiated.

Control esophagogastroscopy after stent extraction.
Discussion
Most cases of PIED respond well to conservative management. 1 However, in the scenario of a CIED, the situation seems to be different. There are recent reports of CIED2–6 all associated with a complicated course. In 1 case, primary esophagectomy was carried out. 4 In 2 cases, protracted endoscopic treatments including esophageal stenting failed, and an additional esophagectomy became necessary.5,6 In 2 other cases, resolution was achieved by complex endoscopic interventions alone, including incision of a septum, transection of the mucosa, bouginage, and late stent placement.2,3 The whole treatment period reached up to 16 months. 2 In summary, all cases of CIED were associated with complications, complex endoscopic interventions, operations, or a combination of both. In our opinion, PIED must be differentiated from CIED. Whereas PIED can be managed conservatively, early endoscopic stent treatment in CIED might prevent further complications, especially the formation of a septum. Because of the stent pressure, the dissected mucosa comes in close contact with the muscle layer, which might promote healing without a septum or stenosis. A fully covered stent might be suitable in cases without perforation because the sealing effect is less important and later extraction will be easy. In case or suspicion of perforation, immediate sealing is crucial,1,4,6 and a PSEMS should be used. 8
Zhu et al. 6 published the only report describing the use of a fully covered stent (Polyflex®; Boston Scientific, Boston, MA) as primary treatment option of a CIED with perforation. However, esophagectomy became necessary owing to further deterioration.
So far, van Rhijn et al. 7 reported the only successful treatment of an EoE-induced PIED with a PSMES. Stent extraction 3 weeks later was complicated by tissue ingrowth, and a stent-in-stent technique was applied. Therefore, van Rhijn et al. 7 concluded that the use of PSEMS should be avoided in patients with EoE. They proposed that “the inflamed mucosa is likely to react to a foreign body by the development of severe fibrosis with increased risk of mucosal tears and perforation.” However, apart from this problem, the PIED had completely healed. Contrary to van Rhijn et al., 7 we believe that the use of PSEMs is justified even in patients with EoE. We argue that the sealing effect is superior to that of a fully covered self-expandable metal stent. 8 Tissue ingrowth into the flairs is important for effective sealing. If the clinical course described by Zhu et al. 6 would have been more favorable using a PSEM remains speculative.
In our patient, instead of the underlying EoE, tissue ingrowth in the flairs was not more pronounced than usual. Extraction of the PSEMS after 2 weeks was totally uneventful.
In conclusion, this is the first report of a patient with EoE, CIED, and perforation treated successfully with a PSEMS. The use of PSEMS in patients with CIED might be superior to conservative treatment or other endoscopic interventions. EoE does not seem to be a definite contraindication for the use of PSEMS.
Footnotes
Disclosure Statement
No competing financial interests exist