
Abstract
Abstract
Background and Study Aim:
Endoscopic submucosal dissection (ESD) is a relatively new but widely used medical technique that has been used to remove gastrointestinal mucosal tumors. This study aimed to identify the usefulness of ESD-assisted dental floss traction for the removal of gastrointestinal tumors.
Patients and Methods:
This was a retrospective study performed at a single institution. From April 2014 to August 2014, 20 consecutive patients presenting with gastrointestinal mucosal tumors at Zhongshan Hospital, Fudan University, Shanghai, China, were enrolled. The tumor characteristics, en bloc resection rates, treatments, and follow-up care practices were evaluated for all patients.
Results:
Of the lesions presenting in the 20 patients, 10 were located in the upper gastrointestinal tract, and the remainder were located in the lower gastrointestinal tract. All the resected tumors were removed completely without interrupting the tumor capsule. No bleeding or perforation occurred, and no recurrences were identified at the time of follow-up.
Conclusions:
The dental floss traction method benefits the ESD procedure during the treatment of gastrointestinal mucosal tumors.
Introduction
E
Our retrospective study aimed to identify the usefulness of ESD-assisted dental floss traction for the removal of gastrointestinal tumors.
Patients and Methods
Patient information
The gastrointestinal mucosal tumors were identified by endoscopic ultrasound and computed tomography before endoscopic surgery; all tumors were determined to be localized to the mucosal layer without distant metastasis. The tumor characteristics, en bloc resection rate, treatment course, and follow-up examination were evaluated in all patients. Informed consent was obtained from each patient.
Endoscopic equipment and technique
All endoscopic surgery procedures were performed by an experienced endoscopist (Y.-S.Z). Standard single accessory-channel endoscopes (models GIF-H260 [Olympus, Tokyo, Japan], CF-260I [Olympus], and AQ100 [Aohua, Shanghai, China]) and/or dual-channel endoscopes (model GIF-2T240; Olympus) were used during the procedures. A short, transparent cap (ND-201-11802; Olympus) was attached to the front of the scope to provide a constant endoscopic view and to apply tension to the connective tissues during dissection. An insulated-tip knife (KD-611L; Olympus), a hook knife (KD-620LR; Olympus), and/or a HybridKnife® (ERBE, Tuebingen, Germany) were used during ESD. The ERBE HybridKnife system was used as a high-frequency generator.
The dental floss traction/ESD for removal of upper gastrointestinal tract tumors
The following steps in the procedure are depicted in the images in Figures 1 and 2.
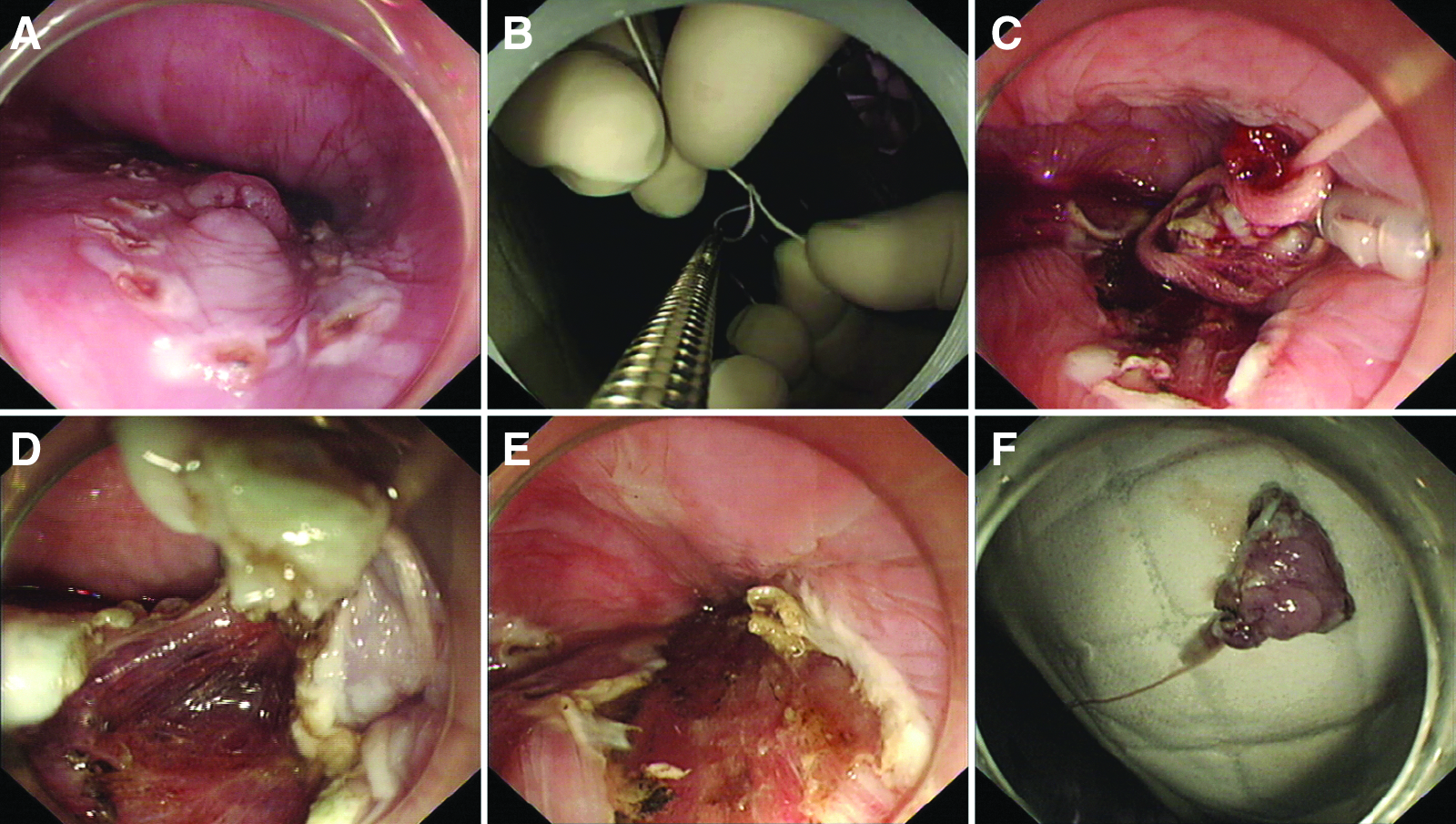
Endoscopic submucosal dissection with dental floss traction in the esophagus:
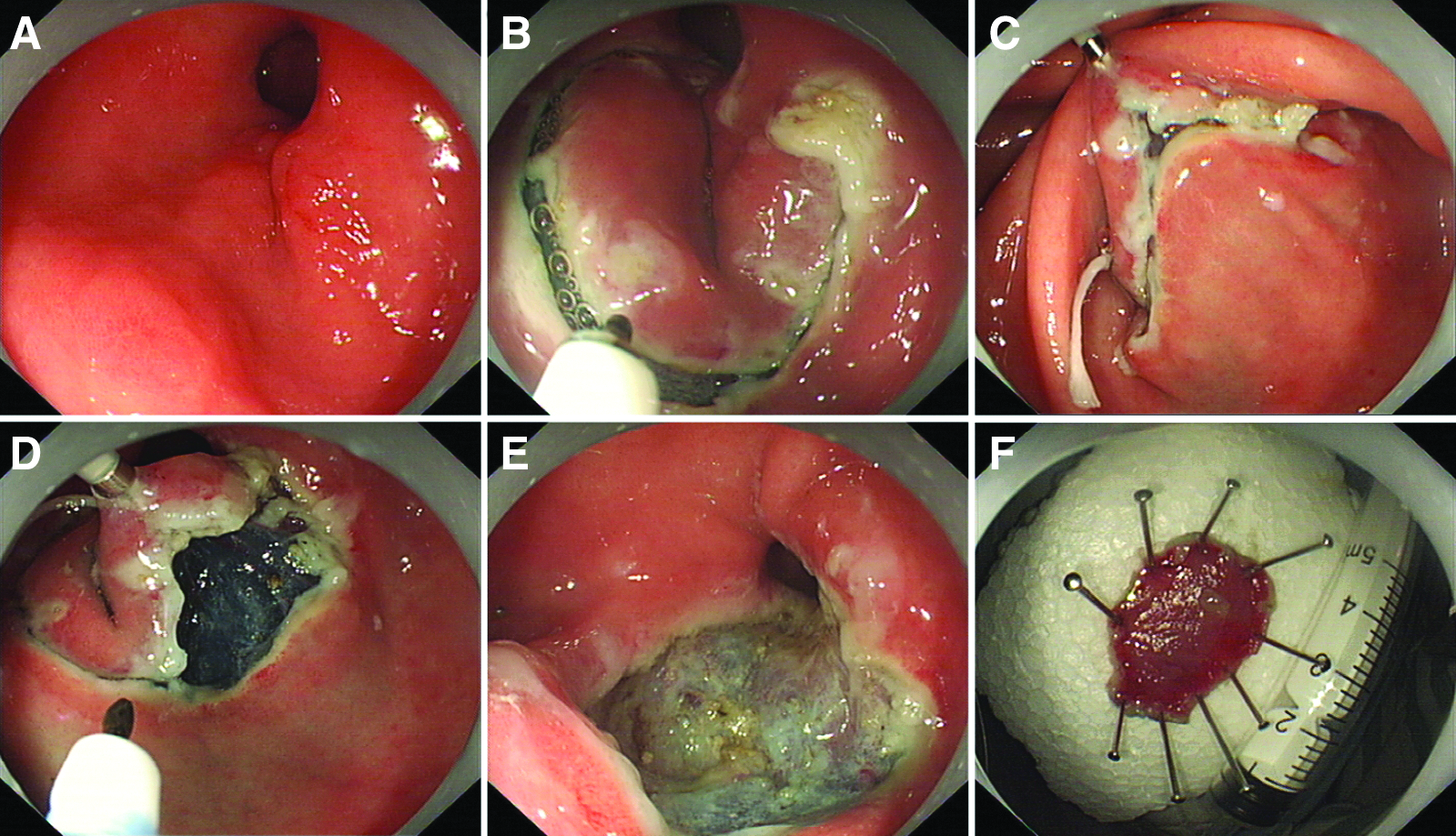
Endoscopic submucosal dissection with dental floss traction in the stomach:
1. Tags. We used narrow-banding imaging to show the edges of the lesions and applied an argon knife to make electric coagulation markers at the edge of the apophysis lesions.
2. Injection. We applied multipoint injections of saline solution (containing indigo carmine and adrenaline) into the submucosal tissue at lateral areas of the marked points. Injection of a small amount of indigo carmine and adrenaline (100 mL of saline, 5 mL of 0.8% indigo carmine, and 1 mL of adrenaline) significantly improved the effect of display and function, as the indigo carmine helped to better define the submucosa and muscularis and helped to more clearly display submucosal injection areas, while adrenaline could shrink the smaller blood vessels to reduce bleeding.
3. Cutting the edge. We used an insulated-tip or hook knife to cut the mucosa along the marked points. During this step, the endoscopist would choose which side of the tumor to start at, depending on the direction of dental floss traction. For example, to deal with the tumors located in the gastric fundus, the operator would start by cutting the side furthest from the cardia.
4. Strip lesions. We applied an insulated-tip or hook knife to strip the submucosa at the bottom of the lesions until the submucosa was difficult to see.
5. Install the dental floss. We exited the endoscope and tied the dental floss to any arm of the metallic clip (HX-610-90 or HX-600-135 [Olympus] or HangZhou AGS MedTech Co., Ltd. [Hangzhou, China]). We trimmed the shorter end of the floss to prevent obscuring the field of view. The longer part of the floss was attached to the body of the endoscope and was pulled by an assistant.
6. Anchor the dental floss. We re-inserted the endoscope and attached the metal clip onto the tumor. The clipping point depended on the direction of traction. When the assistant pulled the dental floss, the submucosa was clearly exposed. Then we could continue peeling the tumor under direct visualization.
7. Close the defect. We made sure that there was no bleeding or perforation, and then we closed the postresection defect with metallic clips.
The dental floss traction/ESD for removal of lower gastrointestinal tract tumors
The main steps of the lower gastrointestinal procedure were similar to those for the upper one, with a few exceptions (Figs. 3 and 4). Due to plica in the intestine, a more careful plan was needed before initiating the operation. Due to the presence of several large blood vessels located around the tumors in the rectum, the risk of bleeding was much higher than in the esophagus and stomach. For these cases we typically precut the anus-side of the tumor first and then reversed the endoscope to start the ESD from the opposite side. When we had difficulty distinguishing the submucosa, the dental floss traction was used.
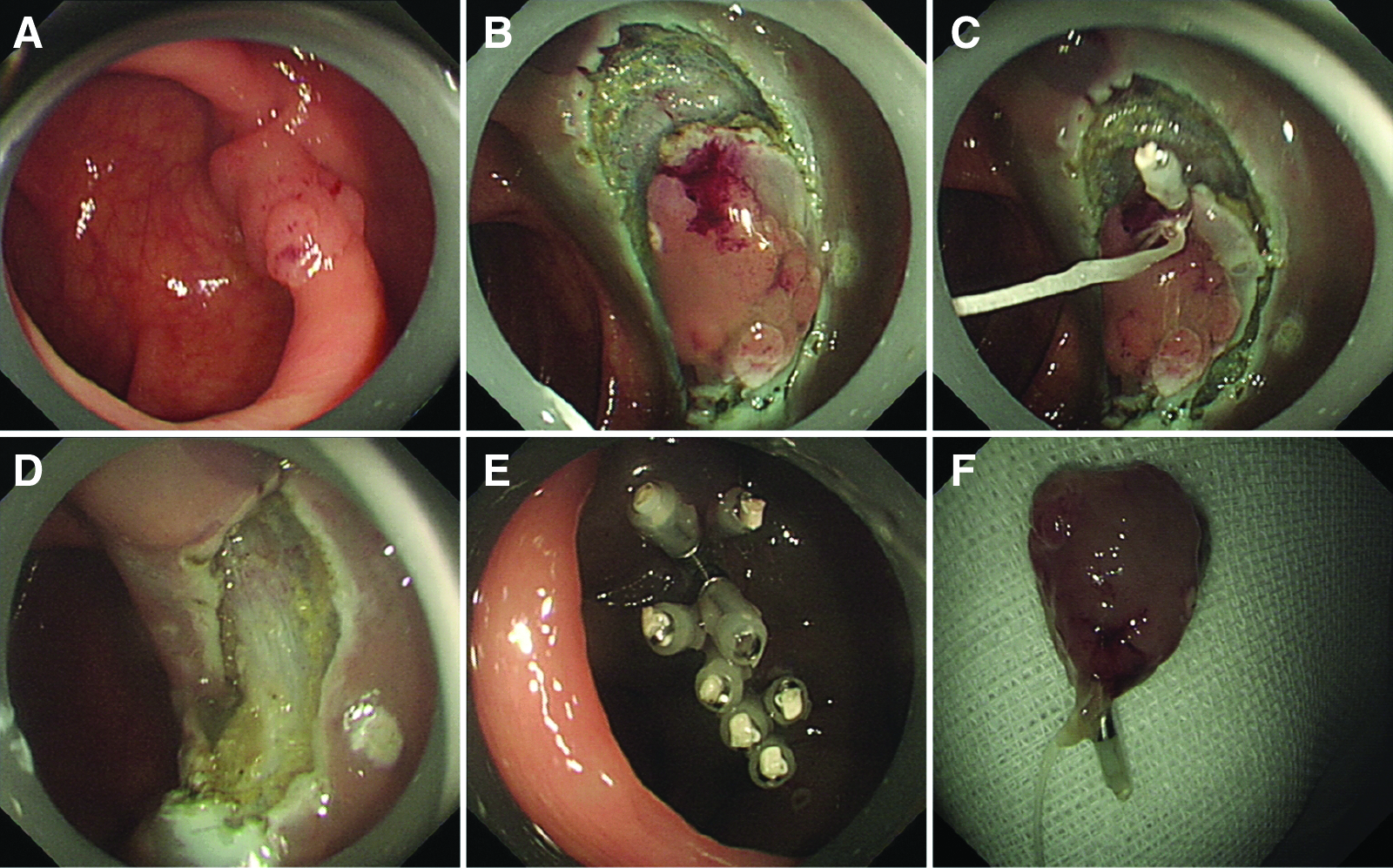
Endoscopic submucosal dissection with dental floss traction in the colon:
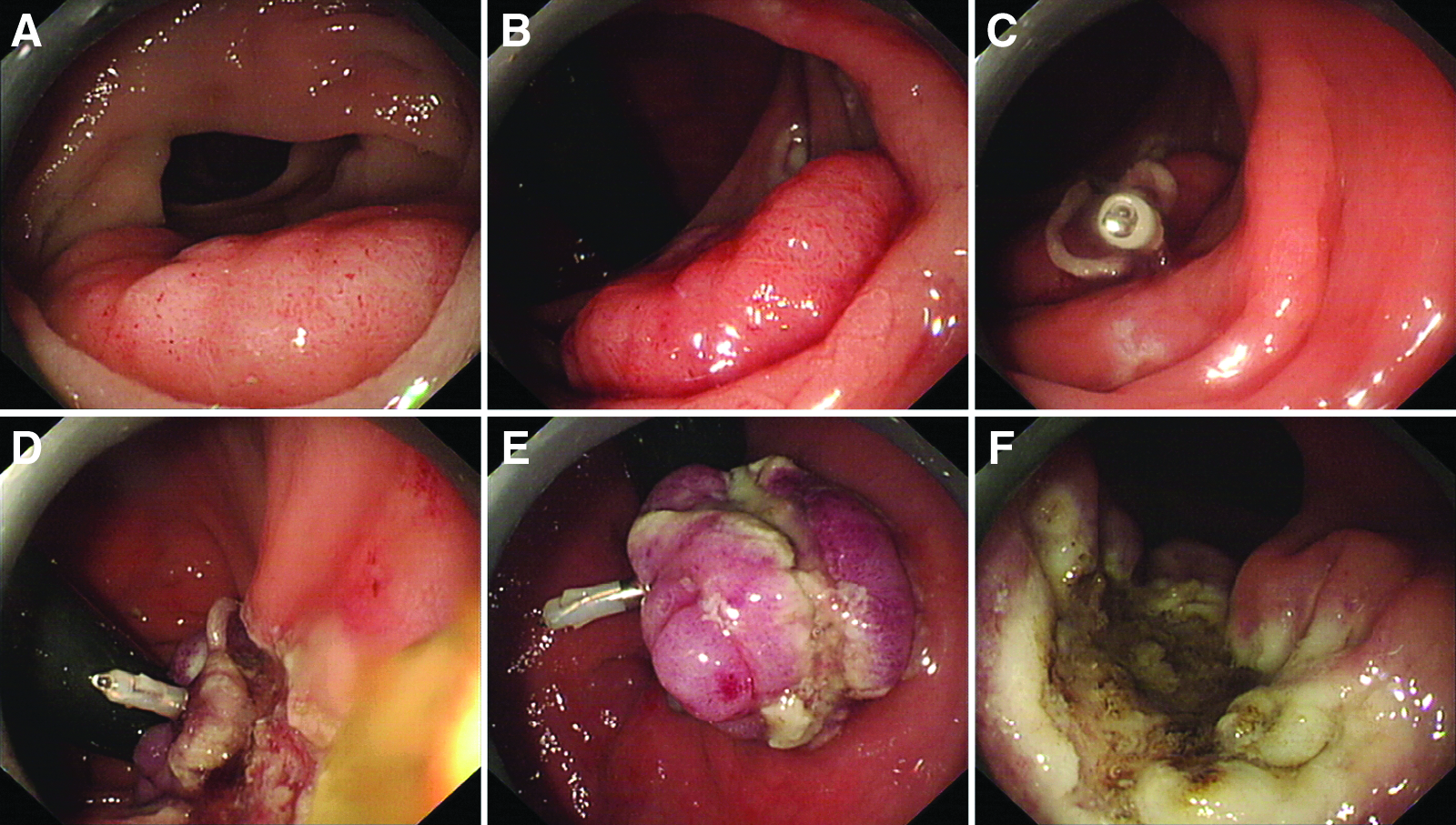
Endoscopic submucosal dissection with dental floss traction in the rectum:
Pathologic evaluation
If after the procedure there was no residual tumor apparent under endoscopy during the surgery and the tumor was removed completely without interruption of the tumor capsule, we considered it to be an endoscopic complete resection. Histopathological evaluations were performed after endoscopic surgery by a trained pathologist.
Postoperative treatment and follow-up
For patients who underwent upper gastrointestinal ESD, we administered intravenously 40 mg of omeprazole postsurgery. Patients were allowed oral intake on the third day after the procedure, unless serious adverse events had occurred. The patients usually stayed on the regular hospital floor for 3–5 days after endoscopic surgery. The patients then received follow-up endoscopy at 1, 2, 6, and 12 months after endoscopic resection and annually thereafter.
Results
After institutional review board approval was obtained, in total, 20 consecutive patients presenting with gastrointestinal mucosal tumors (10 upper gastrointestinal tumors and 10 lower gastrointestinal tumors) received endoscopic surgery with the dental floss traction method in our institute between April 2014 and August 2014. Detailed clinicopathologic data are listed in Tables 1 and 2.
F, female; HGIN, high-grade intraepithelial neoplasia; LGIN, low-grade intraepithelial neoplasia; M, male.
F, female; HGIN, high-grade intraepithelial neoplasia; LGIN, low-grade intraepithelial neoplasia; M, male.
ESD with dental floss traction for upper gastrointestinal tract tumors
Of the 10 patients, 3 were men, and 7 were women. The median age was 53.5 (range, 36–78) years. The mean maximum size of the lesions was 3.75±0.92 (range, 2.5–5.4) cm. Four lesions were located in the esophagus (40%) versus 6 cases (60%) in the stomach. In cases where the lesions were in the stomach, three tumors were in the gastric fundus, two tumors were in the gastric antrum, and one tumor was in the gastric corpus. The time required for the procedure was measured from the time point of marking the area to the resection of the lesion. The median operation time was 45 (range, 30–100) minutes, and no bleeding or perforation was found after completion. The patients did not complain of pain after the procedure. All patients were hospitalized for observation after ESD; the median hospital stay was 3.5 (3–5) days.
Pathological examination determined that the six lesions in the stomach consisted of two low-grade intraepithelial neoplasias and four high-grade intraepithelial neoplasias. The lesions in the esophagus consisted of one low-grade intraepithelial neoplasia and three high-grade intraepithelial neoplasias. All the resected tumors were removed completely without interrupting the tumor capsule. No further intervention was necessary. The follow-up endoscopy revealed a well-healed mucosa. No residual tumor or tumor recurrence was observed during the follow-up period (range, 1–4 months) (Table 1).
ESD with dental floss traction for lower gastrointestinal tract tumors
Among the 10 patients, 5 were men, and 5 were women. The median age was 49.5 (range, 36–76) years. The mean maximum size of the lesions was 2.74±0.54 (range, 1.8–3.5) cm. Seven lesions were located in the colon (70%), and three lesions (30%) were located in the rectum. The median operation time was 60 (range, 40–100) minutes, and no bleeding or perforation was found. The patients did not complain of pain after the procedure. All patients were hospitalized for observation after ESD; the median hospital stay was 3.5 (3–5) days.
Pathological examination determined that the seven lesions in the colon consisted of two low-grade intraepithelial neoplasias and five high-grade intraepithelial neoplasias. The three lesions in the rectum consisted of two low-grade intraepithelial neoplasias and one high-grade intraepithelial neoplasia. All the resected tumors were removed completely without interrupting the tumor capsule. No further intervention was necessary. Follow-up endoscopy revealed a well-healed mucosa. No residual tumor or tumor recurrence was observed during the follow-up period (range, 1–4 months) (Table 2).
Discussion
ESD has arisen in part from the development of endoscopic mucosal resection, which was approved as a new treatment modality in 2003. Application of insulation-tipped knives for endoscopic tumor removal marks the point when endoscopic treatment entered the “ESD era.” ESD can completely strip large tumor lesions, offering a relatively low probably and rate of recurrence. However, the demands on the equipment and operating personnel are relatively high, and the incidence of adverse events inversely correlates with the operator's technical proficiency.2,7
Similar to traditional surgery, the key to a successful procedure is the complete exposure and visualization of the lesion(s) to be resected. During ESD, cutting without distinguishing the submucosa from the mucosa can lead to bleeding or perforation, both of which can be serious adverse events. Li el al. 5 reported the first use of floss with a distal loop and pulley loop that was pulled into the stomach with the forceps. The distal loop was anchored at the edge of the resection mucosa, proximal to the endoscope with the first clip, using a rotatable clip-fixing device. The pulley loop was then fixed on the opposite site of the gastric mucosa with the second clip, which was distal to the distal loop and was used to generate traction up and away from the resection plane. The resection edge of the mucosa was elevated while pulling out the floss through the mouth. In addition, traction systems that facilitate ESD have been described since the introduction of this initial technique.8,9 Ultimately, this suture-pulley method can optimize direct visualization of the submucosal space to improve the accuracy of resection.
During ESD for the treatment upper gastrointestinal tumors, especially large esophageal lesions, the benefit of the transparent cap was limited. The more the tissues were resected, the more difficult it became for the endoscopist to distinguish the submucosa from the mucosa. Some tumors located in gastric fundus were difficult to remove simply due to the inconvenient cutting angle. For lower gastrointestinal tumors, bleeding and perforation are more frequent because of the interference of the plica, the movement of the colon, and the abundant blood vessels present in the rectum. When visualization of submucosa is affected by the resected tumor, an opposite traction is needed to pull up the edge of the tissue. Our work suggests that the dental floss traction method is relatively successful in exposing the tumor margins for resection. Preparation of the dental floss is simple, and the anchoring procedure can be easily applied to the tumor. Second, if bleeding occurs, we can use pressure to stop bleeding and/or expose the bleeding point by electric coagulation hemostasis simply by pulling the dental floss. In addition, the dental floss results in an easier and faster procedure, often with fewer unwanted side effects (e.g., bleeding). However, there are some limitations to this technique, as the dental floss can sometimes cut the tumor during the procedure.
In conclusion, this study demonstrates that the dental floss traction method is useful during the ESD procedure. A large-scale, randomized, controlled study is necessary to evaluate the outcome of this method.
Footnotes
Acknowledgments
This work was supported by grants from The Doctoral Fund Project in 2012 (20120071110061), The Youth Foundation of National Natural Science Foundation of China (81101566), The Shanghai Municipal Science and Technology Committee (13DZ1940402, 13411950800, 13411951600, 12QA1400600, XYQ2011017, 11411950501, 2013SY045, 2013SY054, and 201305), and The Open Fund of Key Laboratory of Carcinogenesis and Cancer Invasion, Fudan University, Ministry of Education (KLCCI2014-6).
Disclosure Statement
No competing financial interests exist.
Y.-S.Z. and S.-L.Cai designed the study. S.-L.C., T.C., and Q.S. analyzed and interpreted the data. S.-L.C. drafted the article. Y.-S.Z. and S.-L.C. critically revised the article and provided significant intellectual input. All authors have read and approved the final manuscript to be published.