
Abstract
Abstract
The detection rate of differentiated thyroid cancers, especially the papillary subtype, is rapidly increasing, and these malignancies have an excellent prognosis. Surgery remains the cornerstone of treatment, and numerous innovations in surgical techniques have been made in the past decade. Laparoscopic thyroidectomy is being gradually recognized as a safe and effective surgical procedure with good cosmetic results. Revision thyroidectomy is routinely performed via the open approach and rarely via laparoscopy. Three-dimensional laparoscopy offers advantages over two-dimensional laparoscopy in terms of visualization of the operative field and surgical manipulation and has been used at multiple surgical sites, but is rarely used in thyroid surgery. We present the first case of three-dimensional laparoscopic revision thyroidectomy, which was successfully performed through an anterior chest approach in a young, unmarried woman who was pathologically confirmed to have papillary thyroid cancer after an initial laparoscopic partial thyroidectomy performed 10 days prior to the revision surgery.
Introduction
T
Surgical resection remains the cornerstone of PTC treatment and has undergone many innovations in recent years.2,4 The clinical application of laparoscopy has greatly changed the technique of thyroid surgery and has benefited many patients, especially young female patients.2,4 In the past decade, laparoscopic thyroidectomy has been gradually recognized as an alternative surgical procedure in selected low-risk PTC patients.4–6 This procedure offers some advantages over conventional surgery, such as excellent cosmetic results and magnification of the visual field.4,6 Revision thyroidectomy is routinely performed using open surgery.7,8 There are, however, a few, scattered reports 9 on laparoscopic revision thyroidectomy (LRT) for PTC patients who have undergone an initial substandard laparoscopic surgery. Despite unresolved difficulties and drawbacks, three-dimensional (3D) laparoscopy has been demonstrated to offer advantages in terms of visualization of the surgical field and surgical manipulation at multiple sites. 10 However, reports on 3D laparoscopy for thyroid surgery are rare. 11
Here, we report the successful performance of 3D LRT in a patient who had pathologically confirmed PTC and had undergone a laparoscopic partial thyroidectomy 10 days earlier. The aim of this report is to explore the feasibility of 3D LRT.
Case Presentation
A 23-year-old unmarried woman was admitted to our department for the treatment of a pathologically confirmed PTC. One week prior to this, she had been admitted to a local hospital for the investigation of a palpable, 1.5-cm-wide, right thyroid nodule that had been present for 2 months. She underwent a laparoscopic partial thyroidectomy through an anterior chest approach on June 20, 2014. Histological examination of the resected thyroid nodule showed a PTC without aggressive histology or vascular invasion (Fig. 1A). BRAFV600E mutation detection by ADx Amplification Refractory Mutation System (Amoy Diagnostics, Xiamen, China) was positive for a BRAFV600E mutation in exon 15 (Fig. 1B). A cervical color ultrasound examination showed postoperative changes in the right thyroid lobe, no abnormality in the left lobe, and no obvious abnormal lymph nodes in the central or lateral compartments. Normal thyroid function was detected, with a thyroglobulin level of 3.01 ng/mL and a TSH level of 3.64 mU/L. The patient was informed about all available treatment alternatives, and she insisted on LRT.
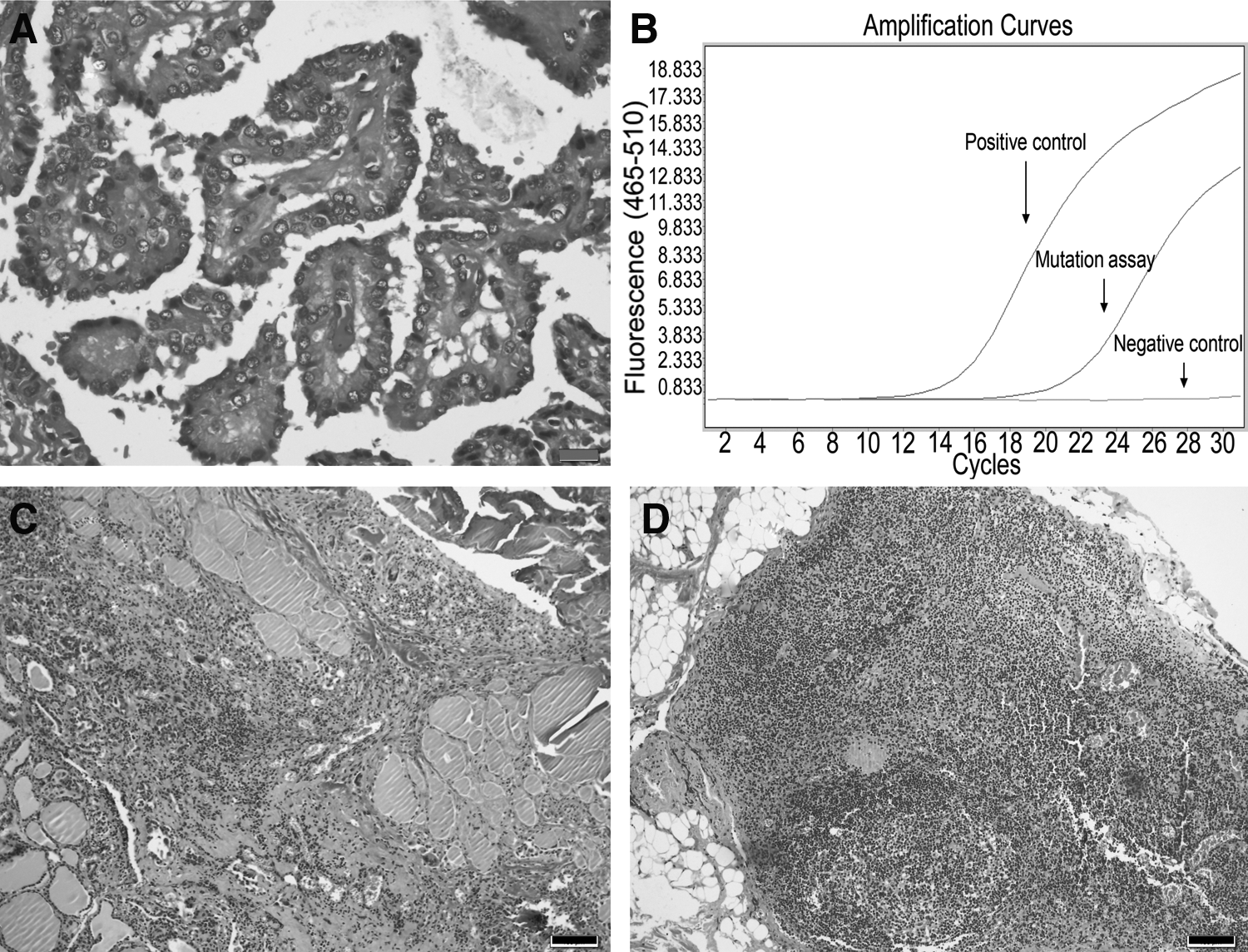
Pathological examination of the resected tissue samples from the first and second operations.
After a preoperative conference and approval by the hospital ethics committee, 3D LRT was performed on June 30, 2014 through the anterior chest approach (Fig. 2A). The 3D LRT consisted of near total thyroidectomy and prophylactic central node dissection. The former included right lobectomy plus isthmus resection and left subtotal thyroidectomy. The surgical process can be briefly described as follows.
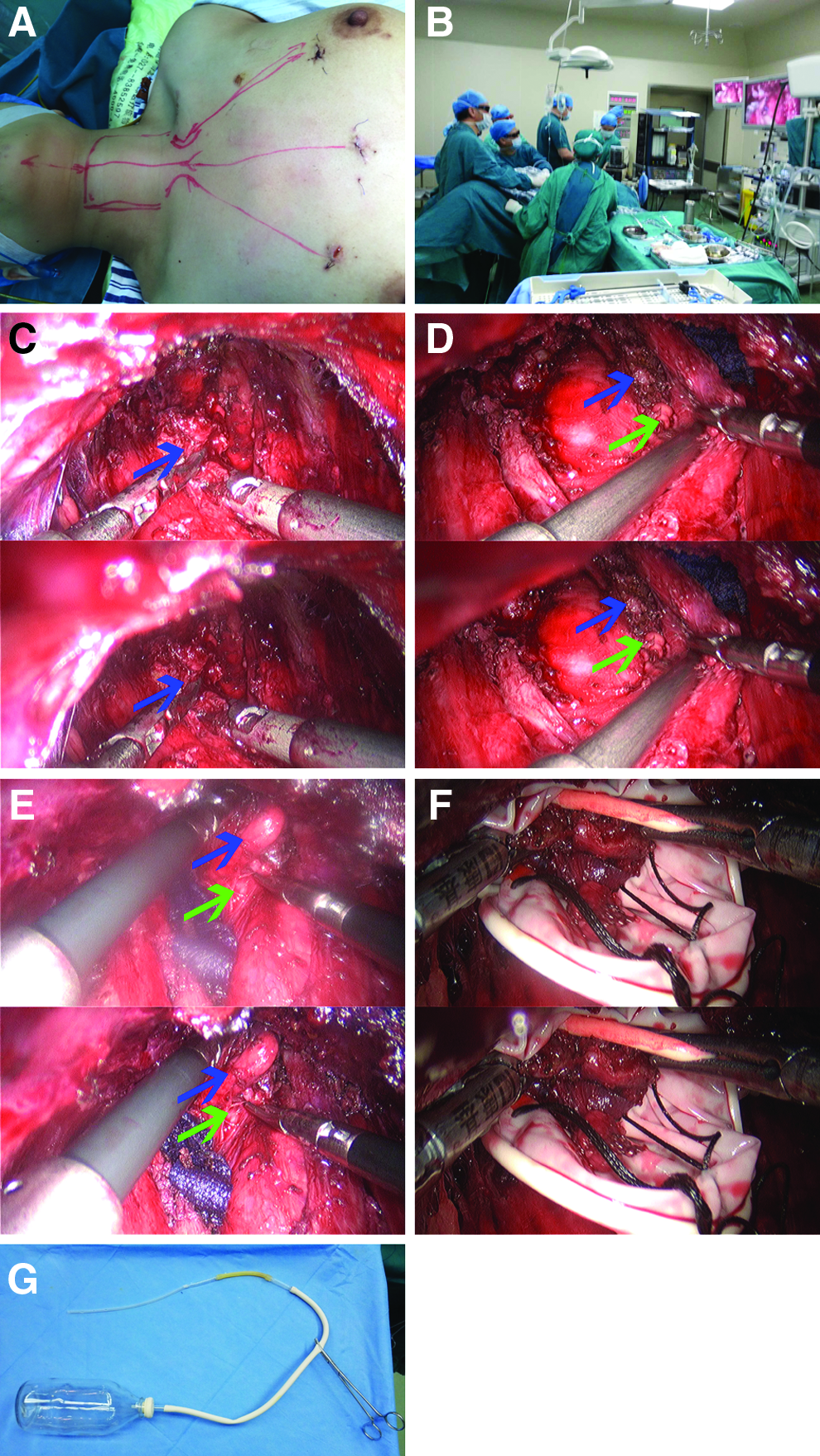
Surgical views during three-dimensional laparoscopic revision thyroidectomy.
The revision surgery was performed using a 3D, 30° laparoscope (3D Einstein Vision; Aesculap, Tuttlingen, Germany) (Fig. 2B). General anesthesia was induced using an oral tracheal cannula, and the patient was placed in the lithotomy position with slight neck extension. To facilitate flap separation and avoid hemorrhage, approximately 100 mL of dilute epinephrine solution (1:500,000) was injected into the subcutaneous space of the anterior chest area and into the subplatysmal space of the neck area via the original middle incision (Fig. 2A). Next, a subcutaneous separator was used to separate the flap, and the injected dilute epinephrine solution was squeezed out of the formed artificial cavity.
A 10-mm trocar was inserted into the middle incision, and the 3D laparoscope was introduced into the trocar. Two 5-mm trocars were inserted into the two lateral chest incisions (Fig. 2A). The surgical cavity was insufflated with carbon dioxide gas at a pressure of no more than 6 mm Hg. The boundaries of the surgical field were expanded to the level of the thyroid cartilage superiorly and to more than 1 cm outside the medial border of both sternocleidomastoid muscles laterally. The working space was dissected, and tissue adhesions in the operative field were removed. The strap muscles were separated in the midline, and muscle adhesions were partially resected (Fig. 2C) to facilitate the subsequent operation and prevent potential tumor cell implantation. The strap muscles were pulled apart to either side, and the remnant thyroid tissues were exposed.
The right remnant thyroid lobe plus the isthmus were completely excised with amputation of the thyroid vessels and preservation of possible parathyroid gland tissue as well as the recurrent laryngeal nerve. The left thyroid lobe was resected, but a small amount of thyroid tissue adjacent to the dorsal fibrous capsule and the upper pole was retained (Fig. 2D). The right central lymph nodes and fatty tissues were dissected (Fig. 2E), with precautions being taken to protect and preserve the recurrent laryngeal nerve, arteria carotis communis, etc. All of the above resected specimens were pulled out through the middle incision by using a rubber bag that we had prepared (Fig. 2F). After careful hemostasis and repeated rinsing with distilled water, the midline was sutured, and two suction drains that we prepared (Fig. 2G) were placed through the two lateral incisions. The suction drains and the stitches were removed after 2 and 9 days, respectively.
Histological examination of the surgical specimens demonstrated granulomatous inflammation without residual cancer in the remnant thyroid tissues (Fig. 1C) and no metastatic signs in the central lymph nodes (Fig. 1D). The whole procedure lasted about 1½ hours. There were no severe postoperative complications such as vocal cord palsy, numbness of the extremities, and subcutaneous hydrops. Wound healing was uneventful, and a satisfactory cosmetic outcome was obtained. The patient was advised to take 100 μg of levothyroxine sodium tablets on an empty stomach every morning and to attend regular follow-up visits. The results of thyroid-function tests performed 1 month later were as follows: thyroglobulin, 2.12 ng/mL; TSH, <0.005 mU/L; and free thyroxine, 26.79 pmol/L.
Discussion
Our patient was a young woman with a 1.5-cm-wide unifocal tumor with no extrathyroidal extension, no detectable central or lateral neck lymph node metastases, no distant metastases, no aggressive histological variant, and a positive BRAFV600E mutation. Although surgery is currently the cornerstone of treatment in the overwhelming majority of PTC patients, there remain some disputes2,3 about the extent of thyroidectomy, the goal of TSH suppression therapy, and the necessity of prophylactic central node dissection and radioiodine remnant ablation. The treatment of our patient differs from the guidelines in different countries and regions (Table 1).12–17 The advances in translational research on thyroid cancer 18 in the last decade have shown great promise in improving the diagnosis, treatment, and prognosis of this disease. Among these advances, the BRAFV600E mutation is the best-recognized prognostic marker thus far. The BRAFV600E mutation in PTC is considered to correlate with aggressive clinicopathological characteristics and increased mortality, but its value over the existing risk-stratification systems in medical management remains questionable. 18 After comprehensive consideration, our patient chose to undergo near-total thyroidectomy and prophylactic central node dissection plus postoperative TSH suppression therapy (initial TSH level, <0.1 mU/L). Despite the positive BRAFV600E mutation and the less-than-total thyroidectomy, we advised the patient to undergo regular follow-up visits instead of radioiodine remnant ablation.
ATA, American Thyroid Association; CACAHNTPC, China Anti-Cancer Association Head and Neck Tumor Professional Committee; CSE, Chinese Society of Endocrinology; CSGSEG, Chinese Society of General Surgery Endocrinology Group; CSNM, Chinese Society of Nuclear Medicine; ETA, European Thyroid Association; JAES, Japanese Association of Endocrine Surgeons; JSTS, Japanese Society of Thyroid Surgeons; LATS, Latin American Thyroid Society; NCCN, National Comprehensive Cancer Network; PCND, prophylactic central node dissection; RRA, radioiodine remnant ablation; TSH, thyroid-stimulating hormone; TT, total thyroidectomy.
Because a certain length of neck scar will be left behind after conventional open thyroidectomy, many patients, especially young women, desire an alternative treatment that results in a better cosmetic outcome. This has led surgeons to develop an ideal surgical method that both enables radical resection and gives a good cosmetic outcome. Endoscopic thyroidectomy was developed after Gagner 19 first performed endoscopic parathyroidectomy in 1996. This technique satisfies both of the above demands. Minimally invasive (i.e., Micolli thyroidectomy) and transextracervical (e.g., axillary, anterior chest, or breast approach) video-assisted or total endoscopic thyroidectomies are increasing being applied for the resection of thyroid nodules, including PTC.2,4 In addition to the favorable cosmetic outcomes achieved using endoscopic thyroidectomy, its surgical safety (including iatrogenic implantation and other complications) was only partially confirmed by some retrospective studies5,6 in selected low-risk PTC patients. Nevertheless, different approaches and methods of endoscopic thyroidectomy are increasingly being carried out in clinical practice.2,4
Despite improved confirmation through preoperative examination (e.g., high-frequency ultrasonography and fine-needle aspiration biopsy) and intraoperative frozen-section analysis, many cases of thyroid cancers confirmed by initial postoperative pathology require revision surgery.7,8 Revision surgery was routinely performed via the open approach7,8 because of the adverse effects of the initial surgery, such as flap adhesions, deformed anatomy, potential implantation risk, and proneness to postoperative complications. We found only one report on LRT presented by Kim et al. 9 in 2010. Owing to the formation and regression process of scar tissues, the appropriate time for revision surgery8,9 is usually within 10 days (or even 3 days) or beyond 3 months after the initial surgery. These times are selected to minimize the influence of scar adhesions. In our patient, revision surgery was performed 10 days after the initial surgery. We found that the flap could be easily separated, and the deformed anatomical structures could be accurately identified.
Although conventional two-dimensional (2D) laparoscopic thyroidectomy can offer more desirable cosmetic results than open thyroidectomy, it has some drawbacks, such as nonstereoscopic vision resulting in eye–hand uncoordination and misperception. Theoretically, 3D laparoscopy can provide superior visualization to 2D laparoscopy and is being gradually applied in several laparoscopic surgeries, 10 including thyroidectomy. 11 However, 3D laparoscopic surgery is still in its preliminary stages and requires repeated verification and improvements. Furthermore, 3D LRT has seldom been used in the treatment of differentiated thyroid cancers. We undertook sufficient preoperative preparations, including repeatedly informing the patient of the risks and complications of the procedure and the possibility of conversion to open surgery and acquiring written approval from hospital ethics committee. We have gained some experience in 3D LRT in this case and a few other cases (not mentioned in this report).
Our findings can be summarized as follows. First, 3D laparoscopic surgery could combine the advantages of the stereoscopic vision of open surgery and the magnification of the visual field of routine laparoscopic surgery. The 3D display could even amplify the aforementioned advantages and thereby facilitate the identification of anatomical structures and precise manipulation. Second, flap dissociation along anatomical spaces and removal of tissue adhesions, which may obscure the operative field, could alleviate or even prevent dizziness, headache, and dry eyes during the operation. For a surgeon experienced in 2D laparoscopic thyroidectomy, an appropriate shift from 2D to 3D laparoscopy could alleviate the above discomforts. In other words, the 3D mode is preferable for the identification and dissociation of key structures such as the recurrent laryngeal nerve and parathyroid glands, whereas the 2D mode is preferable for procedures that are not very delicate.
We think that 3D LRT seems to be a safe, effective, and feasible surgical procedure in selected low-risk PTC patients. The selection of an appropriate time for revision thyroidectomy and the better stereoscopic vision gained from 3D laparoscopy could result in excellent cosmetic results as well as decrease complications. Longer follow-up and more cases are required to determine the feasibility of 3D LRT in eligible PTC patients.
Footnotes
Disclosure Statement
No competing financial interests exist.