
Abstract
Abstract
Background:
Diagnostic and therapeutic laparoscopy is a known approach in managing patients with penetrating abdominal trauma (PAT). However, multiple controversies exist on indications, contraindications, and its appropriateness. The aim of this study was to evaluate the appropriateness of diagnostic and therapeutic laparoscopy in patients with PAT at Dr George Mukhari Academic Hospital, Pretoria, South Africa.
Materials and Methods:
This was a retrospective, observational study. All patients with PAT managed by diagnostic and therapeutic laparoscopy during 2012–2013 were included. Recorded indications and contraindications, the mechanism of injury, the anatomical location of injury, intraoperative findings, reasons for conversion, and adverse outcomes (complications, reoperations and mortality) were analyzed in every case.
Results:
One hundred fourteen patients were included. Stab injuries were sustained by 81 (71%) patients, and 33 (29%) patients sustained gunshot wounds (GSW) to the abdomen. The conversion rate was 7%. The operation was completed laparoscopically in 106 patients: 79 with stab wounds (74.5%) and 27 with GSW (25.5%). Laparoscopy was diagnostic for 44 patients (41.5%) and therapeutic for 62 patients (58.5%). In total, 13 patients (12%) required re-intervention, and 2 patients died (1.9%). The complications were not specific to the laparoscopic approach. No missed injuries were reported in the study.
Conclusions:
Diagnostic and therapeutic laparoscopy in patients with PAT is an appropriate management in hemodynamically stable patients or those responsive to initial resuscitation. The location of injuries is not a limiting factor, although it affects placement of ports. The conversion is not a complication but rather the correct way of completing the operation in an appropriate situation. It should be considered in patients with extensive intraabdominal bleeding suggesting the possibility of major vessel injury, a significant deterioration of the patient, and the complexity of injuries requiring a prolonged laparoscopic procedure.
Introduction
L
As alluded to previously, laparoscopy can be used as a screening, diagnostic, or therapeutic tool. In many studies these roles are mixed. The main reason for this is the absence of a clear protocol defining the exact role of laparoscopy. 1 Despite the evident benefits of a laparoscopic approach in diagnostic and therapeutic surgery for PAT, indications are not well defined and still depend mostly on the surgeon's preference.
We sought to analyze our experience for the appropriateness of and the indications for DL and therapeutic laparoscopy (TL) for patients who have sustained PAT.
Materials and Methods
This was a retrospective, observational study at a single institution (Dr George Mukhari Academic Hospital, Pretoria, South Africa) providing trauma services for a population of 7.3 million people, most of whom live in Gauteng Province, South Africa.
All retrieved cases of adult patients with PAT managed by DL and TL from January 2012 to December 2013 were included in the study. Patients' cases recorded as converted from laparoscopy to laparotomy were also included. “Penetrating abdominal trauma” was defined as trauma caused by a gunshot or a sharp object that violated the skin from the nipple line circumferentially to the line between the upper and middle third of the thighs circumferentially and that entered (or had the potential to enter) the abdominal cavity.
Patients with blunt abdominal trauma managed laparoscopically, patients treated with initial laparotomy, and patients treated nonoperatively were excluded from the study. Patients with PAT managed by DL and TL but whose records were missing were also excluded.
All cases included in the study were analyzed. The recorded indications and contraindications for laparoscopy and the reasons for conversion were considered. A critical review of the appropriateness of laparoscopy in terms of adverse outcomes (complications, re-operations, and mortality) was made in every case in each group. The anatomical location of injury and the intraoperative findings were recorded and correlated with the outcome.
Confidentiality was maintained throughout the study. This study was approved by the Medunsa Research and Ethics Committee of the University of Limpopo and the authorities of Dr George Mukhari Academic Hospital.
All cases were divided into two groups: one group completed laparoscopically and a second group converted to open laparotomy. All laparoscopic operations were divided into diagnostic and therapeutic procedures.
Diagnostic procedures were subsequently subdivided into diagnostic without penetration of the abdominal cavity and diagnostic (nontherapeutic) with penetration of the abdominal cavity but not requiring any therapeutic procedures. Penetration of the abdominal cavity was defined as a violation of the parietal peritoneum or retroperitoneal hematoma signifying the possibility of injury to the intra- or retroperitoneal organs. Nontherapeutic DL was considered when there were no injuries or the identified injuries did not require repair. Evacuation of liquid blood or clots and mobilization of any intra- or retroperitoneal organs for diagnostic purposes were not considered therapeutic.
TL was defined as the laparoscopic management of intraabdominal injuries (more than observation or hemostatic agent application). Therapeutic procedures were laparoscopic or laparoscopic-assisted. In the laparoscopic procedures all interventions were made intracorporeally. In laparoscopic-assisted procedures the injured bowel was eviscerated through assisted access in order to perform the extracorporeal repair, resection, or anastomosis in patients with multiple injuries. Assisted access was a 4–8-cm incision of the abdominal wall usually incorporating the injury site. In some patients, intracorporeal procedures were combined with extracorporeal procedures to minimize trauma to the patient. The laparoscopic-assisted procedures facilitated the management of multiple injuries while preserving all the benefits of minimally invasive surgery.
The location of the injuries was subdivided into five areas: the anterior abdominal area, the right and the left lower chest, the flank, and the back. The anterior abdominal area extended from the lower costal margin superiorly to the iliac crest, the ilioinguinal ligament, and the pubic bone inferiorly, between the anterior axillary lines anteriorly. The right and left lower chest areas were defined as the areas above the lower costal margin anteriorly and posteriorly and below the nipple line circumferentially on each side of the midline. The flank was defined as the area extending from the lower costal margin to the iliac crest, between the anterior and posterior axillary lines. The back was defined as the area extending from the lower costal margin to the iliac crests and medial to the posterior axillary line.
Only complications requiring surgical, endoscopic, or radiological intervention (Grade 3), a life-threatening complication (Grade 4), or the death of a patient (Grade 5, according to the Clavien–Dindo classification) were analyzed. The managed conservatively anastomotic leak and missed injuries were considered as related complications and included in the analysis.
The algorithm depicting our approach to the management of a PAT patient is shown in Figure 1. Our intention was to manage all PAT patients laparoscopically. Patients were continuously assessed and selected for open laparotomy. After full clinical assessment and imaging (ultrasound and computed tomography) where appropriate, patients who qualified for nonoperative management were identified, but where nonoperative management failed, laparoscopic exploration was undertaken. Most of the unstable patients were selected for open laparotomy. Unstable patients who responded to initial resuscitation, as well as all other patients, proceeded to laparoscopy, either DL or TL. This was performed as laparoscopic or assisted laparoscopic. At this stage, patients who had met the conversion criteria could be selected for open laparotomy. The indications for conversion included intraoperative extensive bleeding indicating the possibility of significant vessel injury, the significant deterioration of the patient, and the complexity of injuries requiring a prolonged laparoscopic procedure. Although we did not have such patients in this study, hypothetically poor visibility (e.g., distended bowel and extensive adhesions) could also have led to conversion.
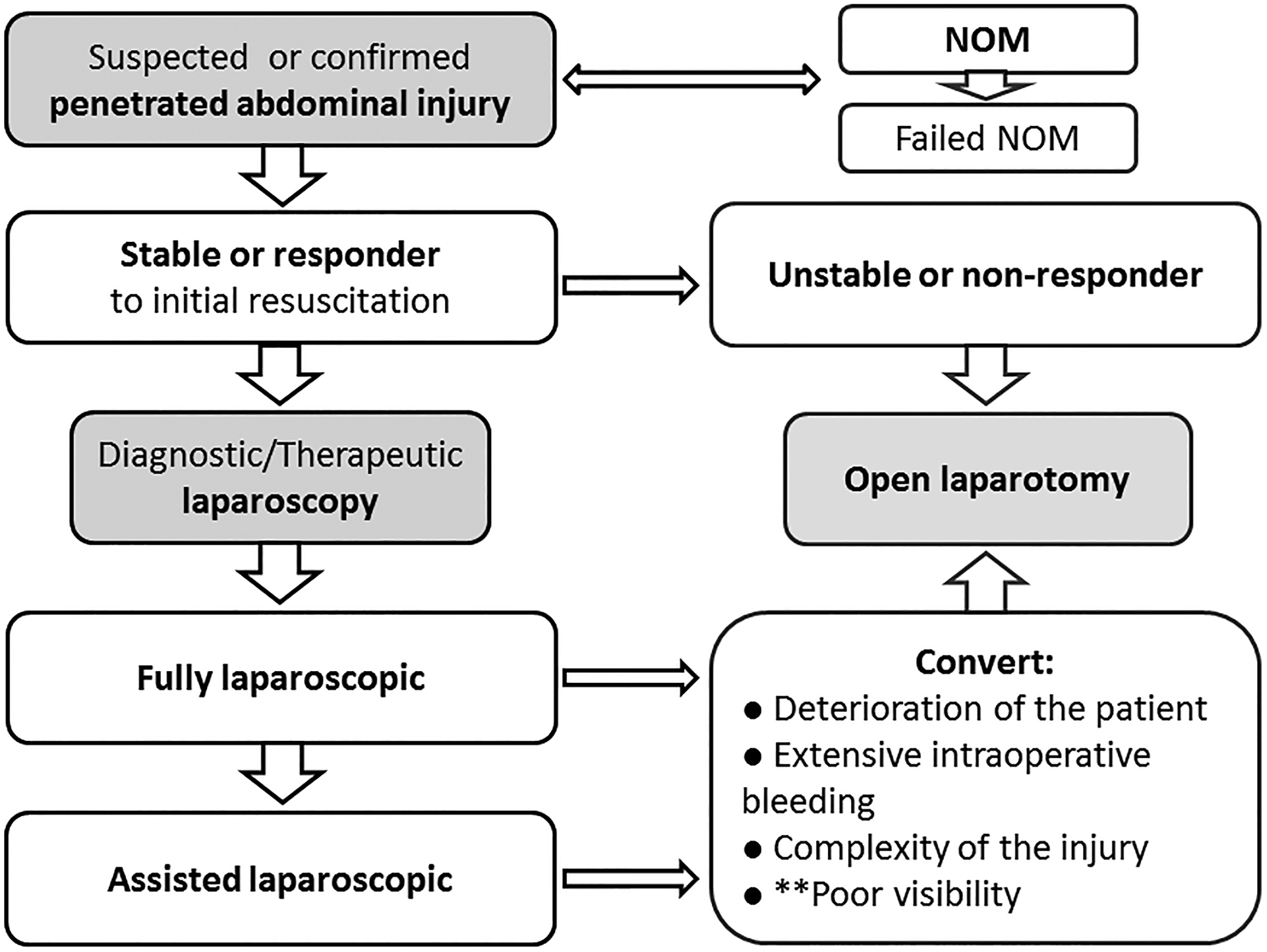
The management algorithm for a patient with penetrating abdominal trauma. **Not demonstrated in this study but it is a potential indication for conversion. NOM, nonoperative management.
Data analysis
Demographic details of the patients were summarized descriptively by mean, minimum, and maximum values for continuous variables and frequency count and by percentage calculations for categorical variables. The prevalence of DL was compared with the prevalence of TL. Clinical outcomes following laparoscopic surgery were described descriptively in relation to the procedural outcomes. Fisher's exact test was used for comparisons of frequency counts/percentage. The t test was used for comparison of mean values as appropriate. All statistical procedures were performed with SAS software (SAS Institute, Cary, NC), release 9.2 or higher, running under Microsoft (Redmond, WA) Windows® for a personal computer. All statistical tests were two-sided, and a value of P≤.05 was considered significant.
Results
One hundred fourteen patients met inclusion criteria and were analyzed. There were 92 male patients from 19 to 70 years of age (mean, 32 years) and 22 female patients from 15 to 74 years of age (mean, 29 years). The overall mean age was 31 years (range, 15–74 years).
Stab injuries were sustained by 81 (71%) patients, and 33 (29%) patients sustained gunshot wounds (GSW) to the abdomen. Eight patients were converted to an open procedure. This constituted a conversion rate of 7%. Six patients with GSW and only 2 patients in the stab wound group were converted to an open procedure. Intraoperative extensive bleeding necessitated prompt conversion to an open procedure in 5 patients. One patient became hemodynamically unstable during operation, 1 patient presented late with bowel injury and severe intraabdominal sepsis, and 1 patient had multiple bowel injuries; in these cases open surgery was a safer procedure. In all cases, the decision to convert was considered as appropriate and beneficial for the patient. Conversion is not regarded as a complication but as the correct way of completing the operation in an appropriate situation. In this study the indications for conversion to open surgery were intraoperative extensive bleeding indicating the possibility of significant vessel injury, the significant deterioration of hemodynamic status of the patient, and the complexity of injuries requiring a prolonged laparoscopic procedure. As the converted procedures were not completed laparoscopically, they were not included in further data analysis.
The operation was completed laparoscopically in 106 patients: 79 with stab wounds (74.5%) and 27 with GSW (25.5%). DL was performed on 44 patients (41.5%) and TL on 62 patients (58.5%). DL revealed no peritoneal perforation in 21 patients (19.8%); peritoneal penetration was present in 23 patients (21.7%). TL was performed as laparoscopic for 39 patients (36.8%) and laparoscopic-assisted for 23 patients (21.7%).
Penetrating stab wounds to the anterior abdominal area were sustained by 49 patients, versus GSW by 12 patients. One patient had a stab wound to the right lower chest, and 20 patients sustained stab wounds to the left lower chest. In the GSW group 5 patients had injury on the right versus 4 on the left. The flank was the location of injury in 8 patients with stab wounds and in 6 patients with GSW. Only 1 patient sustained a stab wound to the back (Table 1). The location of an injury influenced the placement of ports and the extent of dissection.
When the prevalence of DL and TL in patients with stab wounds was compared with that of patients with GSW, no statistical difference between the two groups was found (Table 2).
The injuries diagnosed and treated during laparoscopy are shown in Table 3. Liver injury not requiring repair was the most common finding during nontherapeutic DL. The most common therapeutic procedure was diaphragm repair. TL was performed for any identified injury and was not limited to the selective procedures.
GSW, gunshot wounds; IVC, inferior vena cava.
No missed injuries were reported in the study. We attribute the absence of missed injuries to the mandatory systematic exploration of all abdominal organs (fully intracorporeal or partially extracorporeal in the case of assisted access). Systematic exploration was done using a 30° telescope and two atraumatic bowel graspers. The bowel was rotated to examine it from all angles, while changing the position of the table facilitated visualization; organs were mobilized where appropriate.
In total, 13 patients (12%) required re-intervention (Table 4), and 2 patients died (1.9%).
AV, arteriovenous; CT, computed tomography; GSW, gunshot wounds; I&D, incision and drainage; POD, postoperative day.
One patient, 40 years old, died on postoperative Day 3 after relaparotomy with anastomosis resection and ileostomy for intraluminal bleeding from the anastomosis site. The index operation was laparoscopic-assisted right hemicolectomy for multiple gunshot injuries to the small and large bowel. The patient was recovering but suddenly deteriorated and died. The cause of death was attributed to possible pulmonary embolism. A second patient, 33 years old, sustained a left lower chest stab wound with thoracoabdominal penetration. The index operation was laparoscopic repair of the left diaphragm and exteriorization of the colon injury as a colostomy. On postoperative Day 4 the left posterolateral thoracotomy was performed for clotted hemothorax evacuation and lung decortication. The patient was also undergoing chemotherapy for non-Hodgkin's lymphoma. He died suddenly on postoperative Day 24 from possible pulmonary embolism. The cause of death in both patients was attributed to thromboembolic events and to comorbidity.
Among 13 patients requiring re-intervention, 7 were in the GSW group, and 6 were in the stab wound group (Table 4). All patients fully recovered. Two patients had relaparoscopy for leaking repair of the hollow viscus. One patient had relaparoscopy and cholecystectomy for iatrogenic injury to the gallbladder with delayed leak. The erroneous retraction of the gallbladder with the traumatic grasper induced this injury. Three patients developed septic collection and were managed with percutaneous drainage, relaparoscopy, and laparotomy, respectively. Two patients developed enterocutaneous fistulas. One was managed conservatively, but the other required laparotomy. Two patients had diagnostic nontherapeutic relaparoscopy. One patient developed left renal arteriovenous fistula and was treated with endovascular intervention. Four patients underwent thoracoscopy for clotted hemothorax evacuation.
Discussion
DL for managing PAT with a reported sensitivity and specificity approaching 100% has been comprehensively described in recent studies.1,7 Its high level of accuracy is attributed to the mandatory systematic examination during laparoscopy for trauma, introduced by Kawahara et al. 3 in 2009. Since then the rate of missed injuries has decreased significantly and is reportedly less than 1%.5,6 There were no missed injuries in our study. With improved equipment, video imaging, and surgeon experience, laparoscopy has become a reliable tool to diagnose and treat penetrating abdominal injuries. 3 Park and Youssef 8 have suggested the deployment of DL in the trauma resuscitation area using local anesthesia and intravenous sedation as the laparoscopic assessment in surgical trauma.
TL has not been widely performed and was reported by O'Malley et al. 1 in only 13.8% of cases. On the other hand, Choi and Lim 9 reported 83% of TL in their study. The vast difference in the rate of TL depends on the expertise available. In this study, among 106 patients managed laparoscopically, 63 (58.5%) patients had TL. Despite the fact that laparoscopic repair to virtually every organ has been described, including the diaphragm, stomach, small intestine, colon, bladder, pancreas, and spleen, with impressive results, 10 in most reported series TL is limited to a specific anatomical location, for example, the anterior abdominal area and the lower chest,4,5,11–13 or to minor injuries. By contrast, Cherkasov et al. 14 offered laparoscopic surgery to patients with injuries to the abdominal and lumbar areas and did not limit this surgery only to anterior abdominal injuries. Lin et al. 4 excluded patients with bowel evisceration, back wounds, and gunshot injuries from laparoscopic exploration, whereas Choi and Lim 9 eviscerated injured bowel through 3–4-cm minilaparotomy for repair or resection.
We managed all injuries laparoscopically or by the assisted-laparoscopic procedure irrespective of the anatomical location or the grade of injury. However, the location of injury did influence the placement of ports and the extent of dissection.
We approached patients laparoscopically irrespective of the presence of stab wounds or GSW. In our study, there were no statistical differences between the rate of DL or TL in relation to the mechanism of injury. This issue is not discussed in the literature.
The conversion rate varies among institutions, with its main indication being continuous intraabdominal bleeding that cannot be controlled promptly. 14 O'Malley et al. 1 in their systematic review reported that, in total, 33.8% of patients were converted to laparotomy. The conversion rate in our study was 7%, which is much lower than the reported literature. The main indication for conversion to open surgery is extensive bleeding suggesting the possibility of significant vessel injury that cannot be promptly localized or controlled. The significant deterioration of hemodynamic and respiratory status of the patient necessitates conversion to laparotomy as the patient's condition may further deteriorate because of pneumoperitoneum and absorbed carbon dioxide. In some cases the complexity of injuries requiring a prolonged laparoscopic procedure may be considered as the indication for conversion if the open procedure significantly shortens the time of operation.
Although DL and TL have been limited to selected patients who were hemodynamically stable and had a favorable location of injury, even then they were selected at the discretion of the surgeon. In most studies, the approach has been to select patients for laparoscopic management. By contrast, in our study the reverse approach took place: patients were selected only for open surgery. Our primary intention was to manage all patients laparoscopically. Even unstable patients who responded to initial resuscitation were managed with laparoscopy. In the published literature shock and unstable patients are a contraindication for laparoscopy.4,5,9 However, Cherkasov et al. 14 have reported the safe use of laparoscopy in both hemodynamically stable and unstable patients. In our study unstable patients were considered unsuitable for laparoscopy and selected for open surgery.
Despite the existing differences among centers regarding indications and contraindications for laparoscopy in trauma, a recent systematic review has concluded that unnecessary laparotomy was avoided in 51.8% of patients and that this is the most significant advantage of laparoscopy. 1 Most authors have reported a decreased complication rate, shorter length of hospital stay, and decreased costs when negative laparoscopy is compared with negative or nontherapeutic laparotomy.4,15 TL was not directly compared with therapeutic laparotomy for trauma.
Morbidity and mortality rates depend on patient selection and are reported in ranges that vary from 20% to 40% and from 0% to 5%, respectively.9,14 In our study, the rate of serious morbidity was 12%, and that of mortality was 1.9%. One patient had iatrogenic injury to the gallbladder with delayed leak and was treated with relaparoscopy and cholecystectomy. This is the only complication that may be related to the laparoscopic technique. All other complications were not specific to the laparoscopic approach and were acceptable complications in corresponding patients. Only 4 patients required open surgery, and another 9 were managed with minimally invasive procedures.
In conclusion, DL and TL in patients with PAT are appropriate management in hemodynamically stable or responsive to initial resuscitation patients. The location of injuries is not a limiting factor but does affect placement of ports. A balance should be maintained between the extent of injury and the available expertise for successful surgery. Continuous assessment of the general condition of the patient and the progress of the operation should take place in order to expeditiously select a patient for open surgery. The conversion is not a complication but the correct way of completing the operation in an appropriate situation. It should be considered in patients with extensive intraabdominal bleeding suggesting the possibility of major vessel injury, a significant deterioration of the patient, and the complexity of injuries requiring a prolonged laparoscopic procedure.
Footnotes
Acknowledgments
This study formed part of the dissertation by Dr. O.Y. Matsevych for the degree of Master of Medicine (General Surgery) at the University of Limpopo, Medunsa Campus, Pretoria, South Africa.
Disclosure Statement
No competing financial interests exist.