
Abstract
Abstract
Background:
This study evaluates the safety and cost of introducing minimally invasive pancreaticoduodenectomy (MIPD) to a surgeon's practice.
Subjects and Methods:
All MIPDs performed between December 2011 and July 2013 were compared with open pancreaticoduodenectomy (OPD) cases by the same surgeon. The primary outcomes were mortality, major morbidity, and re-operation. Secondary outcomes were perioperative and oncologic outcomes and cost. MIPD include total laparoscopic pancreaticoduodenectomy (TLPD) and laparoscopic-assisted pancreaticoduodenectomy (LAPD), where a small incision is used for reconstruction. Bivariate comparisons of outcomes were performed using nonparametric tests.
Results:
In total, 44 pancreaticoduodenectomies were performed: 15 MIPDs (2 TLPDs and 13 LAPDs) and 29 OPDs. One death occurred in each group. Major complication rates were not significantly different (33% for MIPD versus 17% for OPD); however, there was a trend toward more re-operation after MIPD compared with OPD (20% versus 3%; P=.07). The incidence of pancreatic leak (20% for MIPD versus 14% for OPD), biliary leak (0% versus 7%, respectively), abscess formation (27% versus 14%, respectively), and intraabdominal hemorrhage (13% versus 3%, respectively) were not significantly different. MIPD achieved equivalent oncologic outcomes as OPD with 100% R0 margin and adequate lymph node retrieval. There was no statistical difference in median operative time (342 minutes for MIPD versus 358 minutes for OPD), length of stay (8 versus 9 days, respectively), operating room expenses (Canadian) ($7246.0 versus $6912.0, respectively), or total cost (Canadian) per case ($15,034.0 versus $18,926.0, respectively).
Conclusions:
MIPD and OPD had similar safety and cost in this introductory series. However, a trend toward a higher rate of re-operation for pancreatic leak suggests the need for caution in introducing this novel technique.
Introduction
S
The aim of this study is to evaluate the safety of introducing MIPD to a surgeon's practice. The primary outcome—safety—is defined as mortality, major morbidity, and re-operation. Secondary outcomes include other perioperative and oncologic outcomes, and cost.
Subjects and Methods
Patients
This is a retrospective review of a prospectively acquired database. Between December 2011 and July 2013, all MIPDs performed at St. Joseph's Health Centre in Toronto, ON, Canada, were compared with contemporary open pancreaticoduodenectomy (OPD) cases by the same surgeon. The study was approved by the St. Joseph's Health Centre Research Ethics Board. The data on demographic, clinical, perioperative, and oncologic data were prospectively collected. Inclusion criteria are tumors of the pancreatic head, ampullary tumors restricted to the second part of the duodenum, common bile duct tumors without vascular or extrabiliary involvement, cystic pancreatic neoplasms, and benign lesions of the pancreatic head. Patients who had vascular resections as well as those having multivisceral resection in addition to pancreaticoduodenectomy were excluded. For selection of suitable patients for MIPD, patients with low body mass index (BMI) and benign or low-grade malignant lesions were favored. These critieria were chosen in order to attempt to minimize the technical challenge of performing the resection. All patients were meticulously informed of the novel nature of this approach as well as the potential risks and complications of MIPD. The possibility of conversion to open surgery was also discussed.
Collection and statistical analysis of data
The preoperative evaluations collected from electronic charts included complete history, physical examination, blood work, tumor markers, computed tomography, magnetic resonance imaging, endoscopy, and biopsy. Intraoperative findings were collected from operative dictations and anesthesia record. Perioperative recovery was measured by time to oral intake and ambulation and length of stay. Postoperative complications were recorded by the residents and verified by the attending at monthly morbidity and mortality rounds. Radiological imaging and histopathology data were collected from online electronic records.
All data were prospectively entered into a computer database. The data were collected as numerical and categorical variables. Bivariate comparisons of characteristics and outcomes of the laparoscopic and open resection groups were performed using nonparametric tests, and a P value of <.05 was considered statistically significant. Propensity scores were calculated using logistic regression, and inverse propensity score weighting was used to make adjusted comparisons of outcomes between the laparoscopic and open resection groups. These adjusted comparisons were made using logistic and linear regression.
Description of the laparoscopic phase
All MIPDs were performed or supervised by one of the authors (S.J.), who has fellowship training in minimally invasive surgery and hepatopancreatobiliary surgery. The MIPDs were performed 18 months after the author's initiation of independent practice. Prior to this time, he established safety with the open approach in his practice and sought learning opportunities at conferences and collaboration with surgeons already performing MIPD.
The patient is placed in the supine position with legs together. A 12-mm trocar is placed 1 cm below the umbilicus, and pneumoperitoneum is applied to a pressure of 12 mm Hg. Five additional trocars are placed under direct vision: in the left lumbar quadrant (5 mm), midclavicular line in the left subcostal quadrant (5 mm), anterior axillary line in the right lumbar quadrant (12 mm), midclavicular line in the right subcostal quadrant (5 mm), and midclavicular line in the inferior right lumbar quadrant (5 mm).
The lesser omental sac is entered by dividing the gastrocolic ligament. The stomach is retracted upward to reveal the anterior surface of the pancreas. The hepatic flexure of the colon is mobilized, and the anterior surface of the duodenum is exposed. A Kocher maneuver is performed, and the ligament of Treitz is divided from the right, posterior to the duodenum. The dissection is carried out between the duodenum and pancreas to visualize the gastroduodenal artery. The superior mesenteric vein posterior to the neck of the pancreas is skeletonized, creating a tunnel view behind the neck of the pancreas. At this point, the camera is switched to the 12-mm port in the anterior axillary line in the right lumbar quadrant.
Additional dissection is performed along the plane between the porta hepatis and inferior vena cava, up to the foramen of Winslow. The dissection is continued laterally until the superior mesenteric vein is reached through this angle. Now the superior surface of pancreas is dissected to reveal the common and proper hepatic arteries, portal vein, common bile duct, and lymph nodes.
The camera is then returned to its original umbilical port. Distal gastrectomy is performed using a laparoscopic stapler, and the gastroduodenal artery is divided using clips. This allows adequate visualization of the anterior and lateral surfaces of the common bile duct. After the pancreatic neck and the superior mesenteric vein underneath are separated, the pancreas is divided, and the pancreatic duct is visualized. The small bowel mesentery is mobilized up to the ligament of Treitz. The proximal jejunum at 10–15 cm beyond the ligament of Treitz is then divided using a stapler, and the mesentery of the jejunum and duodenum is dissected proximally using hook cautery and energy.
Cholecystectomy is performed, and the common bile duct is divided. Then the pancreatic head and uncinate process are dissected off the superior mesenteric vessels. During this process, the inferior pancreaticoduodenal artery is divided, and care is taken to clip and divide small veins along the superior surface of the pancreas to maintain a bloodless field view. Lymph nodes around the celiac axis, hepatic artery, superior mesenteric artery, pancreaticoduodenal vessels, pylorus, common bile duct, pancreatic head, hepatic hilum, and along the aorta are removed.
Description of the reconstructive phase
In laparoscopic-assisted pancreaticoduodenectomy (LAPD), the incision for the umbilical port is extended to a 7-cm median incision, and a laparoscopic wound protector is applied. The en bloc specimen is placed in a retrieval bag and delivered through this incision. Three reconstructions are performed: end-to-side pancreaticojejunostomy using the Blumgart technique, 9 end-to-side hepaticojejunostomy, and end-to-side gastrojejunostomy in a proximal to distal manner through the minilaparotomy. The surgeon and assistants take care to avoid tension while performing the anastomoses, and the techniques of anastomoses in LAPD are the same as in OPD.
In total laparoscopic pancreaticoduodenectomy (TLPD), the jejunal loop is brought up through an opening in the transverse mesocolon. A Blumgart-style pancreaticojejunal anastomosis is performed laparoscopically using transpancreatic sutures with 3-0 absorbable, braided suture. In total, six or seven duct-to-mucosa stitches are done using 5-0 absorbable monofilament suture. In the hepaticojejunostomy, the back wall comprises 4-0 running absorbable monofilament and interrupted 5-0 absorbable braided suture in a duct-to-mucosa fashion. The anterior layer is closed using running 5-0 absorbable monofilament. The gastrojejunostomy is completed approximately 40 cm from the hepaticojejunostomy using laparoscopic staplers. The anastomoses in TLPD are set up and performed to mimic how they would be in an OPD. Drains are not routinely used. The specimen is extracted through a Pfannenstiel incision.
Results
In total, 44 patients were included. MIPDs were performed in 15 patients (2 TLPDs and 13 LAPDs), and OPD were performed in 29 patients. Table 1 presents patient demographics. There was no statistical difference in gender, age, American Society of Anesthesiologists score, or presence of comorbid conditions (P>.05), but the MIPD group had a significantly lower BMI (25 kg/m2 for MIPD versus 28 kg/m2 for OPD; P=.003).
Categorical results are expressed in count (percentage), and numerical results are expressed in median (range).
P<.05 is a significant difference.
ASA, American Society of Anesthesiologists; BMI, body mass index; OPD, open pancreaticoduodenectomy; MIPD, minimally invasive pancreaticoduodenectomy.
Table 2 shows the operative and histopathologic findings for MIPD and OPD. MIPD and OPD had similar operative time (342 minutes versus 358 minutes; P>.05) and need for blood transfusion (P>.05). MIPD achieved 100% R0 resection margin and comparable lymph node harvest. There was no significant difference in tumor size or proportion of operations done for malignant disease. Among the final histopathologic diagnoses in the MIPD group, there were 5 patients with ampullary carcinoma, 3 intraductal papillary mucinous neoplasms, 2 neuroendocrine tumors, 1 duodenal adenocarcinoma, 1 solid adenocarcinoma, 1 cholangiocarcinoma, 1 mucinous cystadenoma, and 1 serous cystadenoma. Among the OPD group, there were 11 patients with pancreatic ductal adenocarcinoma, 5 cholangiocarcinoma, 2 metastatic colon cancers, 2 pancreatitis, 2 intraductal papillary mucinous neoplasms, 2 duodenal adenocarcinomas, 2 neuroendocrine tumors, 1 ampullary carcinoma, 1 metastatic renal carcinoma, and 1 choledochal cyst.
Categorical results are expressed in count (percentage), and numerical results are expressed in median (range).
LN, lymph node; OPD, open pancreaticoduodenectomy; MIPD, minimally invasive pancreaticoduodenectomy.
The primary outcomes of the study are the “safety” outcomes (Fig. 1). One death occurred in each group. One patient in the MIPD group died of pancreatic leak and pulmonary embolism. One patient in the OPD group had preoperative hepatic fibrosis and died of liver failure.
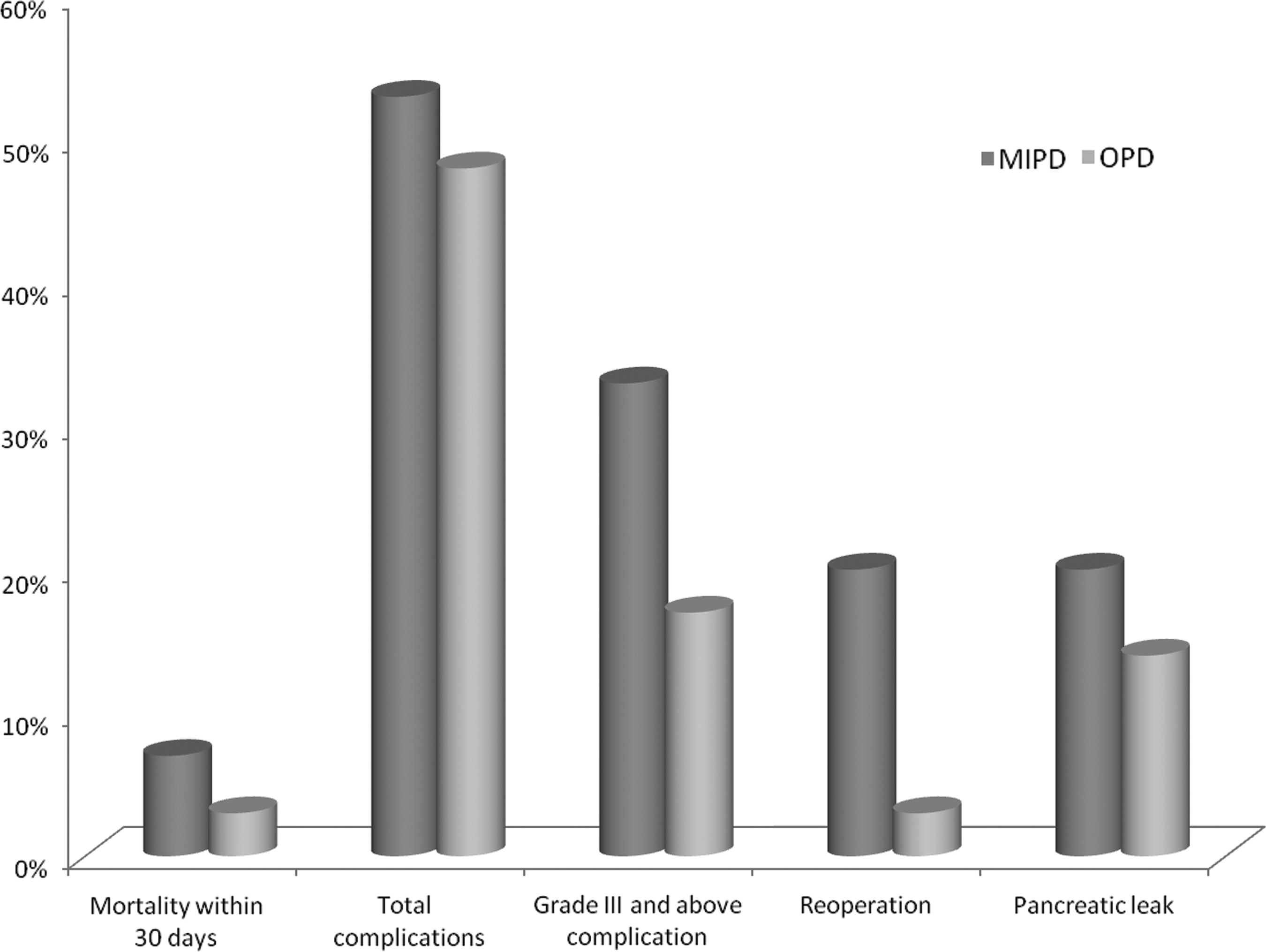
The primary outcomes of minimally invasive pancreaticoduodenectomy (MIPD) versus open pancreaticoduodenectomy (OPD), in terms of mortality within 30 days, total proportion of patients who had any complications, grade III and above complications, re-operations, and pancreatic leaks.
Table 3 demonstrates that there was no significant difference in the rate of major complications between the groups by Clavien–Dindo grade. 10 Complications in each group are summarized in Table 4. There was a nonsignificant trend toward increased incidence of pancreatic leak (20% for MIPD versus 14% for OPD; P=.23) and re-operation (20% versus 3%, respectively; P=.07) in the MIPD group. The corresponding International Study Group Pancreatic Fistula (ISGPF) grades 11 for the pancreatic leak in the MIPD group are grade C for all 3 patients due to the need for re-operation in all of them. In the OPD group, the ISGPF grades are C except in 1 case; however, only 1 of the ISGPF grade C cases underwent re-operation. The ISGPF grade was not assigned to every case because drains were not routinely placed in this series. The length of hospital stay was similar between the groups (8 days for MIPD versus 9 days for OPD; P>.05).
Categorical results are expressed in count (percentage), and numerical results are expressed in median (range).
D/C, discontinue; PCA, patient-controlled analgesia; OPD, open pancreaticoduodenectomy; MIPD, minimally invasive pancreaticoduodenectomy.
GI, gastrointestinal; OPD, open pancreaticoduodenectomy; MIPD, minimally invasive pancreaticoduodenectomy; PE, pulmonary embolism.
In terms of secondary outcomes of postoperative recovery, there was no significant difference in the number of days to first flatus, regular diet, discontinuation of epidural or intravenous pain medications, initiation of oral pain medications, or rate of re-admission within 30 days (Fig. 2).

Selected measures of postoperative recovery after minimally invasive pancreaticoduodenectomy (MIPD) and open pancreaticoduodenectomy (OPD). PCA, patient-controlled analgesia.
Table 5 shows the adjusted comparisons of outcomes between the groups using propensity scores and inverse propensity scores. A nonrandomized study comparing MIPD versus OPD comes with its inherent confounding by indications. Patients who are offered MIPD can be expected to differ from those who were not offered the procedure in terms of important prognostic factors, such as age, BMI, and type of tumor. A simple comparison of the patient outcomes after MIPD versus OPD would be biased by these confounding variables; therefore, propensity scores were used. The propensity score provides an assessment of the measured explanatory variables, such as age, BMI, and type of tumor, and estimates the probability of a patient receiving the intervention of interest given these factors. 12 It is one of the strategies that nonrandomized controlled studies use to control for some of the confounding factors. However, one of the limitations is that propensity scores cannot account for potential confounding variables that were not measured; an example in this study would be the texture of the pancreas or amount of adhesions that a patient forms after the operation. When interpreting studies using propensity scores, it is important to note that propensity scores would not cancel out many inherent biases in a case series design. In our study, the propensity scores were included in a regression model. The nonsignificant P values are consistent with that proposal that the observed patient characteristics are balanced between the MIPD and OPD groups.
Propensity scores were calculated using logistic regression and inverse propensity score weighting was used to make adjusted comparisons of outcomes between the minimally invasive pancreaticoduodenectomy (MIPD) and open pancreaticoduodenectomy (OPD) groups.
CI, confidence interval; D/C, discontinue.
The cost analysis of MIPD versus OPD with available cost data is shown in Table 6, with a breakdown of median cost of individual items and total cost. It is notable that the operating room expenses (Canadian) ($7246 for MIPD versus $6912 for OPD; P=.71) were not significantly different between the groups. The total cost (Canadian) per case, including the cost of re-operations and the overall hospitalization, was not significantly different ($15,034 for MIPD versus $18,926 for OPD; P=.13) (Fig. 3).

Comparisons of total cost and operating room expenses in the open pancreaticoduodenectomy and minimally invasive pancreaticoduodenectomy (MIPD) groups (median and interquartile range) (P>.05). CDN, Canadian.
Data are median (range) costs, in Canadian dollars.
ICU, intensive care unit; OPD, open pancreaticoduodenectomy; MIPD, minimally invasive pancreaticoduodenectomy.
Discussion
This study reports the outcomes of introducing MIPD to a surgeon's practice. Although this experience shows that similar perioperative outcomes are achievable in comparison with the traditional open approach, this study also shows a trend toward a higher rate of re-operation and pancreatic leak using the minimally invasive approach. In addition, the operating time, operating room expenses, and total hospital cost for MIPD are not significantly different from those for OPD. These results are important from the utilization of healthcare resources point of view in that MIPD did not result in increased demand on operating room and overall hospital resources. When incorporating MIPD into practice, it may be important to select cases that have the highest chance of being completed laparoscopically. In this series, the MIPD group had a significantly lower BMI than the open group, which is similar to other studies.3,7 As experience grows, the selection criteria could be gradually broadened. The MIPD operations in this study had equivalent intraoperative outcomes, such as amount of blood loss.
The median operative time for MIPD (342 minutes) in this introductory series is on the lower end of the range of operative time quoted by other studies,2,13 and it was comparable to open surgery times in the contemporary OPD cohort. This metric is important in the single-payer universal healthcare environment where getting patients through the system efficiently is of great importance. However, it must be acknowledged that the MIPD cases in this series were highly selected and would likely have been completed much faster had the operations been done open.
The literature on postoperative outcomes after MIPD is unclear on whether MIPD has better outcomes than OPD. Our study did not find any significant difference in the rate of postoperative complications between the MIPD and OPD groups. The most notable finding in this regard was the re-operation rate of 20% in our MIPD group, which was due to severe pancreatic leaks despite percutaneous drainage in 3 out of 15 patients. Indeed, every pancreatic leak that occurred in the MIPD group ultimately resulted in re-operation to control the leak. One plausible explanation for this observation is that after OPD, there may be a greater tendency to form adhesions given the extensive manipulation of abdominal content, which can help wall-off or contain a pancreatic leak. With a minilaparotomy in LAPD cases, fewer adhesions may allow uncontrolled pancreatic leakage. In addition, patient selection may be a factor. MIPD patients were more likely to have small ducts and soft pancreatic parenchyma due to the diagnoses preferentially approached laparoscopically. The condition of the duct and gland in these patients may have potentiated leaks. These tumors were selected as they may be technically easier to remove. In view of this experience, we have begun to routinely insert prophylactic drains in all MIPD cases. Later series from the same author may address the question whether the rate of severe pancreatic fistula requiring re-operation would decrease as more experience is gained.
Despite the trend toward higher incidence of re-operation for pancreatic leaks in the MIPD group, the overall postoperative recovery was similar to that in the OPD and contemporary studies.2,4,14,15 The timeline of days to first flatus, regular diet, oral pain medications, and length of hospital stay are within the range of other studies.2,3,16 Like these studies we did not find any significant difference between MIPD and OPD groups in these short-term measures of postoperative recovery.
A recent study by Mesleh et al. 17 shows that MIPD has a higher total surgical cost (combination of operating room time cost and surgical supply cost) than OPD, but once admission costs are taken into account, there was no difference in total cost per case between the groups. It is encouraging that in our introductory series, MIPD cases did not cost more than the OPD cases. Indeed, although there was no significant difference in the overall cost of MIPD and the open approach, the noted median difference of nearly $4000 (Canadian) is may be financially significant in a single-payer universal healthcare environment. The difference in cost leading to an overall lower expense for the MIPD group is attributed to lower inpatient care costs and intensive care unit costs. The lower intensive care unit cost in the MIPD group is attributed to shorter intensive care unit stay because all patients are routinely observed in the intensive care unit for the first postoperative night—or longer if needed—at our institution. The tendency for shorter hospitalization may also play a role (8 days for MIPD versus 9 days for OPD). This may be related to a tendency to “fast-track” an MIPD patient over an OPD patient. Further investigation is necessary.
In conclusion, this series demonstrates that MIPD was safe and had comparable outcomes with the open approach. Although there was not a statistically significant difference in costs, a potential for cost savings during this introductory series suggests that with increased experience and refinement of the technique, this approach is worth pursuing. However, caution should be taken in introducing the minimally invasive approach due to a potentially higher risk of reoperation and pancreatic leak.
Footnotes
Disclosure Statement
S.L. declares no competing interests exist. S.J. has received academic support from Ethicon Endosurgery, Roche, Pathfinder, and Therapeutics Inc., has done paid speaking engagements for Astellas Pharma Canada Inc. and Lundbeck, and has done paid consulting work for Ethicon Endosurgery.