
Abstract
Abstract
Background:
The preferred therapy for simple postcholecystectomy biliary leak consists of percutaneous drainage and biliary stent insertion under endoscopic retrograde cholangiopancreatography (ERCP). With a novel endoscopic insertion device, a biodegradable biliary stent (BDBS) may be used in the treatment of a cystic duct leak without repeated endoscopy for stent removal. The objective of this article was to report the first case of endoscopic insertion of BDBS for postoperative bile leak and assess its feasibility and safety.
Patient and Methods:
A 64-year-old man with a postoperative leak from the cystic duct stump was treated with ERCP, biliary sphincterotomy, and insertion of a self-expandable 40-×8-mm polydixanone BDBS (Ella CS, Hradec Králové, Czech Republic) after insertion of a percutaneous drain.
Results:
Endoscopic insertion of BDBS was successful and uncomplicated. On Day 7 after ERCP, the patient was in good condition, no signs of bile leak or inflammation were observed, and the percutaneous drain was removed. At 3 months, magnetic resonance imaging showed that the BDBS was patent and in the right location. At 6 months, the stent had expectedly degraded.
Conclusions:
A novel endoscopic insertion device with a polydixanone BDBS appears feasible in treating disorders of the human biliary duct. BDBS now offers an encouraging option for endoscopic therapy of bile leaks.
Introduction
B
Patient and Methods
A previously healthy 64-year-old man was admitted 2 days after an elective open cholecystectomy with elevated temperature and upper abdominal pain to the tertiary referral center of Tampere University Hospital, Tampere, Finland. The serum C-reactive protein concentration was elevated (93 mg/L), and the bilirubin level was within normal limits (17 μmol/L). Transabdominal ultrasound, magnetic resonance imaging (MRI), and computed tomography scan revealed a 5-×6-cm fluid accumulation in the gallbladder bed without common bile duct stones or signs of biliary obstruction or concomitant vascular injury. A radiologist inserted a percutaneous 8-French pigtail drain under ultrasonic guidance to drain the fluid accumulation, which proved to be bile juice (fluid bilirubin level=231 μmol/L).
As bile flow into the drain continued for 8 days after surgery, ERCP was performed with the patient under conscious sedation (7 mg of oxycodone [Oxynorm®; Takeda GmbH, Linz, Austria] and 7 mg of midazolam [Hameln Pharmaceuticals GmbH, Hameln, Germany]) administered intravenously and monitored by the endoscopy team. An anti-inflammatory suppository (100 mg of diclofenac [Novartis, Espoo, Finland]) was given approximately 60 minutes before ERCP. Duodenal peristalsis was reduced with 40 mg of hyoscine butylbromide (Buscopan®; Delpharm Reims, Reims, France) intravenously. A standard duodenoscope (model TJF-Q180V; Olympus, Hamburg, Germany) with air insufflation was used. After uneventful cannulation with a standard short guidewire, a full biliary sphincterotomy was performed (Dreamtome™ RX44; Boston Scientific Corp., Natick, MA) with pure-cut electrocautery (Erbe ViO® 200D electrosurgical system; Erbe Elektromedizin GmbH, Tübingen, Germany). Cholangiography (Philips BV Endura; Philips Medical Systems, Best, The Netherlands) using 240 mg/mL of iohexol (Omnipaque®; GE Healthcare, Little Chalfont, United Kingdom) with a biliary balloon (9/12 mm; Extractor™ Pro RX; Boston Scientific Corp.) revealed a slight leakage of contrast outside the biliary duct in the vicinity of the cystic duct stump (Fig. 1).

A cholangiography image at the beginning of the biodegradable stent implantation. *A faint contrast leak close to the stump of the cystic duct is seen just below the surgical clips. **Percutanous 8-French pigtail drain. ***The tip of the stent implantation device is inserted over a stiff guidewire into the distal common bile duct.
This study received approval (protocol number R12021) from the Ethical Committee of Pirkanmaa Hospital District, Tampere. The research use of BDBS was previously approved by the Regional Ethics Committee of Pirkanmaa Hospital District. Informed consent to the use of BDBS was obtained from the patient.
Results
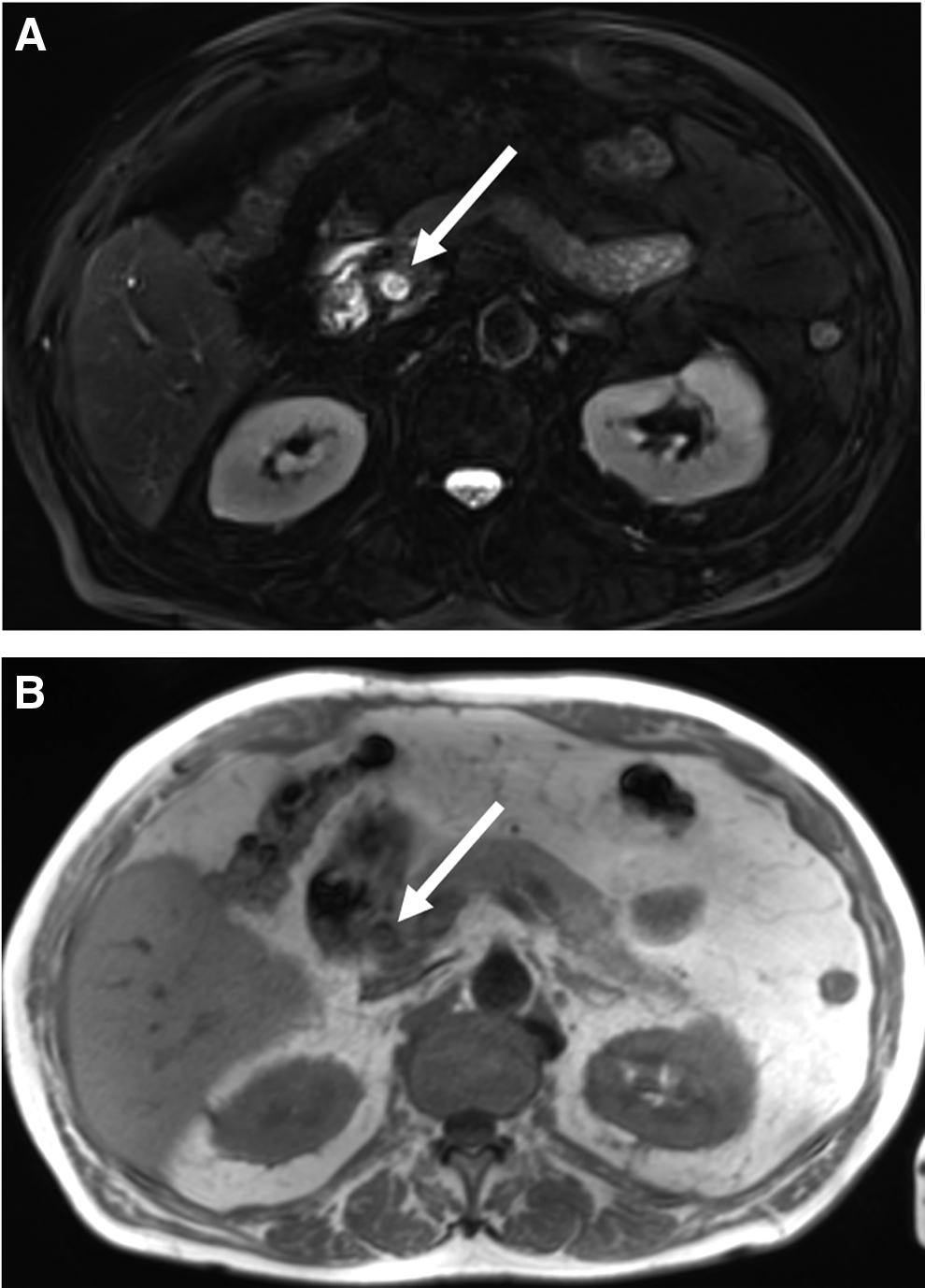
Before stent implantation, a stiff long guidewire (0.035 inch; 450 cm; Dreamwire™; Boston Scientific Corp.) was positioned. A custom-made braided self-expandable biodegradable polydixanone noncovered biliary stent with golden radiopaque markers at both ends and 40 mm in length with a postdeployment diameter of 8 mm (Ella CS, Hradec Králové, Czech Republic) was then successfully inserted (Fig. 2). The stent was adjusted to the proper location with its distal end clearly visible inside the duodenum (Fig. 3). After discharge, the output of the percutaneous drain diminished to less than 10 mL/day, indicating that the BDBS had successfully treated the postcholecystectomy biliary leak. The drain was removed on Day 7 after ERCP at an outpatient visit when the inflammatory markers were normalized, with no signs of icterus, and the patient was feeling well. No ERCP- or stent-related complications occurred during the first 30 days. At the follow-up MRI at 3 months, the stent was patent and in the right location inside the common bile duct (Fig. 4). At 6 months the stent was no longer visible in MRI.
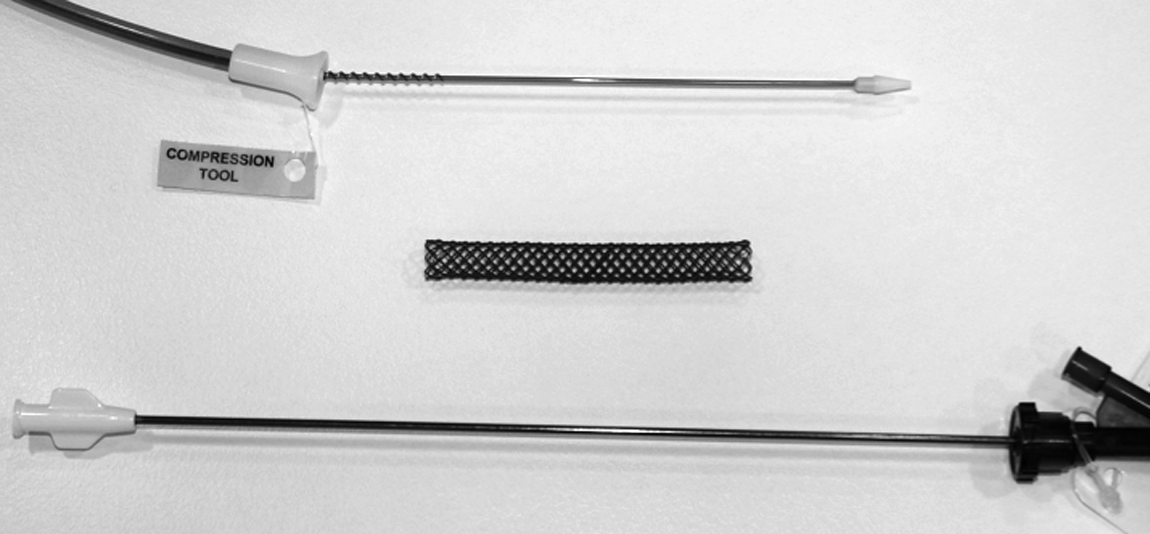
A custom-made braided self-expandable biodegradable polydixanone noncovered biliary stent with golden radiopaque markers at both ends with a postdeployment diameter of 8 mm (Ella CS) and an endoscopic insertion device.

An endoscopy view of the biodegradable stent in final position with a guidewire still in place.
Discussion
Endoscopic stent treatment is the preferred treatment in simple bile duct injury and leakage from the cystic duct after cholecystectomy.2–4 Although minor bile duct injury after cholecystectomy (Strasberg grade A–C) is relatively uncommon with an incidence of less than 1%,1,4 the large numbers of cholecystectomies performed make this complication an important clinical issue in tertiary-care centers for both surgeons and endoscopists. Efficient therapy with a plastic stent necessitates repeated endoscopy for stent removal, usually 1–2 months after insertion. To overcome the burden of multiple endoscopies to patients and the healthcare system, a BDBS appears to offer a perfect solution. However, until recently, only transhepatic and no endoscopic insertion devices have been available from stent manufacturers for biliary use in biodegradable biliary stenting. We report the first case of successful endoscopic insertion of a BDBS with a commercial insertion device for postcholecystectomy cystic duct leak with 6 months of follow-up.
Earlier studies have shown that the biodegradable stents may be safely used in the hepatobiliary duct.7–9 An endoscopically inserted BDBS also offered a safely and faster treatment of bile leakage than a plastic stent in an animal model of iatrogenic cystic duct leak. 5 Polylactide stents appear to remain patent for at least 3 months and disintegrate at 6 months with no residual changes in the histology of the biliary epithelium. 5 The polydixanone BDBS used in this case has been proven to be safe and fully degradable in 6 months in percutanous biliary use in humans and in the animal model.6,8 Its molecular structure and degradation profile are comparable to those of polylactide. 6 Furthermore, there is accumulating clinical experience of the use of polydixanone biodegradable stents in, for example, esophageal strictures. 10
In this case, a prototype model of an endoscopic insertion device was successfully used with a custom-made self-expandable radiopaque braided polydixanone biliary stent 40 mm long and 8 mm in diameter. Although the stent was introduced over a stiff guidewire, we found it challenging to push the stent insertion device into the common bile duct as the prototype instrument appeared inflexible; during implantation, only careful manipulation of the tip of the duodenoscope and limited use of an elevator were possible as the insertion device was easily bent by axial force.
In our experience the most important issue for the successful use of the BDBS was good endoscopy technique with a stable position in the duodenum to be able to proceed straight down the duodenoscope and to avoid excessive use of the elevator as the insertion device passes the tip of the scope. The gold radiography markers at both ends of the stent provided adequate visibility in radiography. However, the stent itself is x-ray negative, and endoscopic visualization of the stent as it moves inside the insertion device may be challenging.
The endoscopic implantation of a polydixanone BDBS was successful with excellent clinical outcome in this case. At 3 months MRI showed that BDBS was still patent and had not migrated. Although the degradation profile has already been proven in clinical studies and now most issues associated with the implantation device seem to have been solved, BDBS offers a fascinating option for endoscopists treating postoperative bile leaks. The main advantages—no need for removal and large diameter—are obvious. However, results from larger prospective studies are needed to confirm the feasibility of the insertion device, as well as its cost-effectiveness and safety compared with plastic stents.
Footnotes
Acknowledgments
This study was financially supported by the Competitive State Research Financing of the Expert Responsibility area of Tampere University Hospital, Tampere, Finland.
Disclosure Statement
No competing financial interests exist.