
Abstract
Abstract
Background:
In the past several decades we have seen that most cervicomediastinal goiters (CMGs) can be removed through a cervical lower collar incision, but in some circumstances a median sternotomy or a thoracotomy is mandatory. In the last few years, video-assisted thyroidectomy (VAT) has been developed, and the indications are that its usage is becoming more widespread. This study aimed to evaluate the technical feasibility and safety of VAT for CMG.
Patients and Methods:
Over a 5-year period (2009–2014), 602 patients underwent conventional thyroidectomy (CT), and 356 cases underwent VAT in the Department of General Surgery, Beijing Anzhen Hospital, Capital Medical University, Beijing, China. Among all those patients, 33 (3.4%) were diagnosed with CMGs and operated on. These patients were divided into two groups: the CT group included 18 patients, and the VAT group included 15 patients. The incision length, operative time, blood loss, hospitalization time, and postoperative complications were recorded and analyzed.
Results:
All 15 procedures in the VAT group were performed successfully with the help of endoscopy, whereas for 2 of the 18 patients (11.1%) in the CT group, a partial median sternotomy had to be done due to poor exposure and abnormal hemorrhage. Significant differences in the incisional length, operative time, and intraoperative blood loss occurred between the CT and VAT groups. The patients who underwent VAT had a better cosmetic result without going through an additional incision. There was no difference in the resected goiter weight between the two groups. The patients who underwent VAT recovered more rapidly and had a shorter hospitalization time than those in the CT group (P = .000). No significant difference was found in postoperative complications between the two different approaches. During a mean follow-up through 28 months (range, 3–66 months), no recurrence occurred.
Conclusions:
VAT is a safe and feasible approach for patients with CMG. The procedure has relatively satisfactory cosmetic effect and faster postoperative recovery.
Introduction
C
With the popularization and application of the video-assisted technique in thyroid surgery, many surgeons have carried out useful explorations. Video-assisted thyroidectomy (VAT) can be proposed on a much larger scale than at its beginning and cannot be considered an option for only a limited number of patients. Over the last few years, VAT has been developed, and the indications of the technique are becoming more widespread. In this article we present two different surgical approaches conducted on 33 patients, including VAT and conventional thyroidectomy (CT). This study was a retrospective analysis that aimed to evaluate the technical feasibility and safety of VAT for CMGs. The result is encouraging.
Patients and Methods
Clinical characteristics of patients (Table 1)
During a 5-year period (2009–2014) in the Department of General Surgery, Beijing Anzhen Hospital, Capital Medical University, Beijing, China, 602 patients underwent CT, and 356 cases underwent VAT. Among all those patients, 33 patients (3.4%) with CMGs were diagnosed and operated on by the same surgical team.
Patients were divided into two groups according to the surgical technique performed: from February 2009 to May 2012, the CT group included 18 patients ranging in age from 30 to 70 years, and from May 2012 to April 2014, the VAT group included 15 patients ranging in age from 36 to 64 years. There was no significant difference in age between the two groups.
Clinical presentations
Among these 33 patients anterior cervical mass and dyspnea were the most common clinical symptoms, of which 14 cases were accompanied by chest distress and tightness, and 7 cases had no obvious symptoms. Physical signs showed that varying degrees of cervical uplift and palpable cervical masses could seen in all cases. In addition, the lower pole of the masses was not palpable because it had plunged into the mediastinum (Table 1).
Data are number of patients (%).
CMG, cervicomediastinal goiter; CT, conventional thyroidectomy; VAT, video-assisted thyroidectomy.
Auxiliary examination
Prior to surgery all 33 patients underwent thyroid high-frequency color Doppler ultrasound examination, chest and neck X-ray, and multidetector computed tomography (MDCT) scan; meanwhile, patients also underwent fibrolaryngoscopy and thyroid function tests, which were also essential.
Thyroid ultrasound was a common test performed on every patient to detect single or multiple thyroid nodules, as well as to measure the goiter volume and the depth below the thoracic inlet.
Frontal and lateral X-rays of the cervix and chest displayed a widened mediastinum, especially the anterior and superior portions. Varying degrees of tracheal obviation due to compression in the 33 patients (Fig. 1A, B, and D) were present. The tracheal displacement between the two groups reached a maximum of 2 cm.
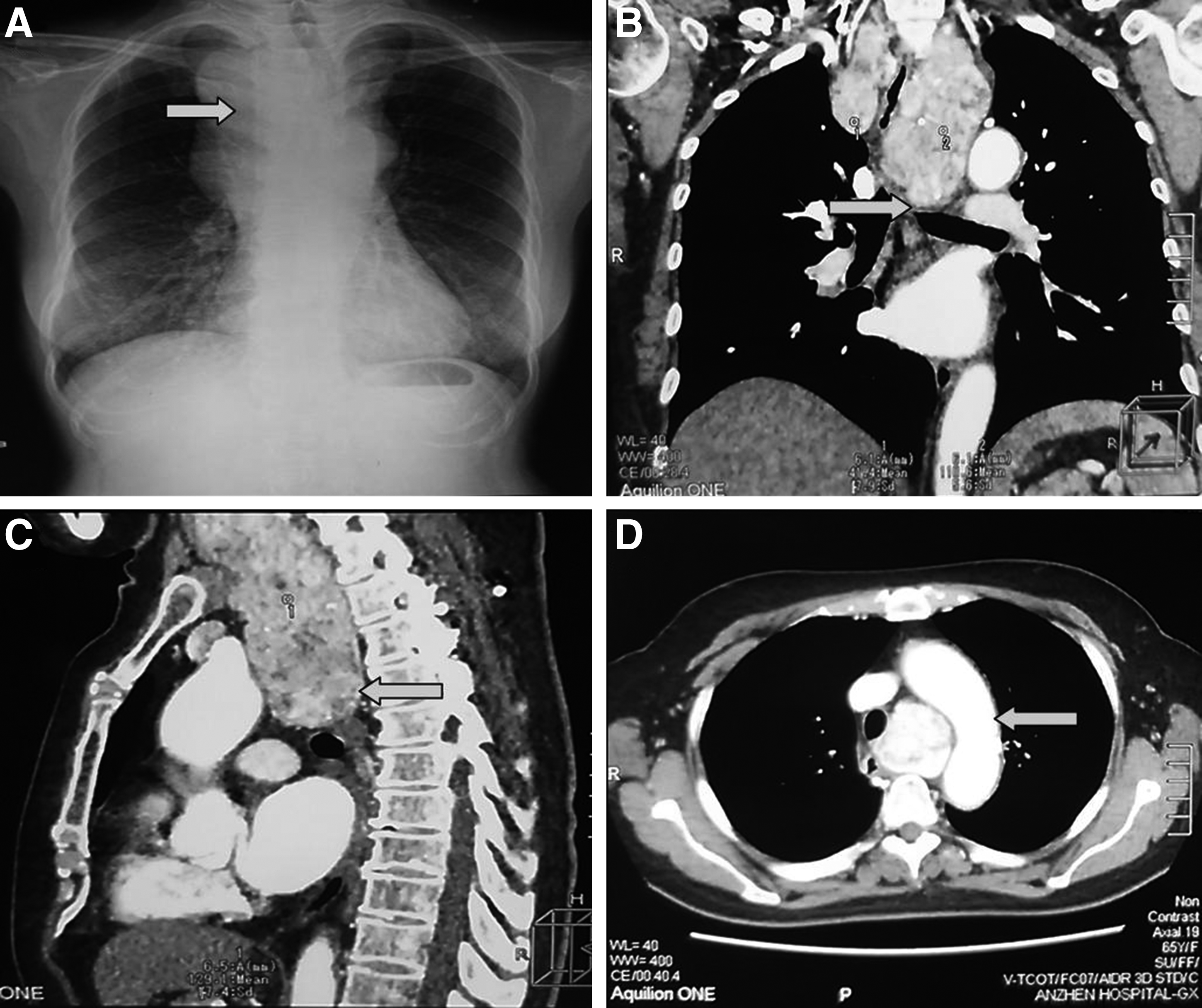
Radiological examination before the operation.
Transverse, coronal, and sagittal MDCT scans of the neck and chest helped us further clarify the different positions and levels of goiters in the mediastinum. Cervical MDCT scan images demonstrated bilateral masses in 5 patients, a right mass in 19 patients, and a left mass in 9 patients. Thoracic MDCT scan images indicated lower poles of the goiters above the aortic arch in 21 cases, at the level of aortic arch in 11 cases, and below the aortic arch in 1 case (Fig. 1B and C). In addition, spatial relationships between the masses and surrounding structures such as mediastinal vessels were acknowledged (Fig. 1D). In this series, a clear and complete low-density zone around the secondary mediastinal goiters is usually present in different sectional MDCT images.
The use of fibrolaryngoscopy was recommended to identify whether vocal cord movement was limited before the operation.
All patients also received chemical examinations, including thyroid function tests and the thyroid microsomal antibody + globulin antibody test.
Prior to surgery 1 case was accompanied with congenital heart disease with mild pulmonary hypertension, 2 cases with arrhythmia, 5 cases with coronary heart disease, and 6 cases with primary hypertension.
Case selection criteria
In secondary CMG, MDCT scans showed the goiter extending at least 3 cm below the cervicothoracic isthmus 1 manifested with a swelling neck. The following were used as exclusion criteria: (1) a history of neck operation or radiotherapy, (2) hyperthyroidism, or (3) suspected malignant thyroid tumor manifesting as swollen lymph nodes in the neck.
Preoperative preparation
The diagnosis of CMG was confirmed in the 33 patients by counseling, physical examination, thyroid ultrasound, X-ray, and MDCT scan. Prior to surgery, consultation with the Department of Otolaryngology, Cardiology and Cardiothoracic Surgery was done to gain a comprehensive understanding of the patients. Those patients whose condition combined with heart disease received an echocardiogram test to assess cardiac function. Moreover, cardiac arrhythmias and high blood pressure should also be appropriately controlled.
The conventional surgical position for standard thyroid surgery was adopted for the operation. The patients were placed in a supine position with a soft occipital pad under the shoulder to allow for neck extension, which contributed to field exposure.
Special auxiliary instruments included all the techniques available. A 0° 5-mm diameter telescope from Karl Storz (Tuttlingen, Germany) was used to explore the mediastinum. A Harmonic ACE® ultrasonic knife (Ethicon, a Johnson & Johnson Company, Somerville, NJ) was helpful in the coagulation and resection of small thyroid vessels in the mediastinum. A periosteal detacher and a metal-head suction device removed goiter adherence to the surrounding tissues in the mediastinum. A long-arm retractor may help expose the cervical part of the goiter, but the exposure of the mediastinal portion would be limited because the thoracic inlet is fixed and stabilized. Preoperative preparation for sternotomy or thoracotomy should be made.
Surgical approaches
All patients underwent double-lumen endotracheal intubation under general anesthesia. As usual, we chose a low collar-shaped incision 1–1.5 cm above the sternum notch. The incision length in the CT group ranged from 6.0 to 10.0 cm, and that in the VAT group ranged from 3.5 to 5.0 cm.
CT
Each layer of the cervix was incised, and the inferior cervical muscles were dissected to achieve a satisfactory field exposure. First, superficial blood vessels and the medium-sized vein of the ipsilateral lobe were coagulated and incised along the capsule using the ultrasonic knife. Second, the isthmus of the thyroid was dissected and separated from the trachea. Third, with the cricothyroid space opened, the superior thyroid vessels were disposed firmly. The index finger, periosteal detacher, and metal-head suction apparatus were used to perform the blunt dissection, which was carried out in the mediastinum anteriorly, laterally, and posteriorly to the gland. In the meantime, separation should always be gentle and close to the gland to keep the posterior thyroid capsule intact. If significant adhesions existed between the goiter and the mediastinal vascular structures or if there were difficulties in controlling mediastinal bleeding, an immediate sternotomy or a thoracotomy should be advised and performed by a cardiothoracic surgeon to ensure the safety of the entire operation.
VAT (Fig. 2)
VAT differed from CT in that to maintain a working space, an L-shaped thyroid retractor with table mount lift is placed under the strap muscles and secured to the table mount lift on the ipsilateral side. When the goiter is being operated on, the working space was entered using the telescope through a cervical incision by an assistant surgeon to magnify the operative field. Special attention should be given to avoid interruption of the operating field of the surgeon-in-chief, separating the tight adhesion with caution and maintaining the cleanness of the operative region. Other operational procedures were conducted the same way as described for CT. The cervical portion of the goiter was disassociated from nearby structures and drawn upward and outward to create enough space for the mediastinal portion of the goiter. Thyroidectomy would be undertaken with emphasis that the RLN and the parathyroid should be preserved appropriately. Then, the large goiter would be gradually mobilized and separated from the mediastinal structures by using the ultrasonic knife, periosteal detacher, and suction. Difficulties could be encountered due to the narrow field resulting from bilateral goiters. Small deep vessels in the mediastinum could be coagulated and dissected using the ultrasonic scalpel under video assistance. After the goiter was removed from the mediastinum, endoscopic exploration of the empty residual cavity in the mediastinum was performed to exclude or confirm the presence of ectopic goiter or consistent bleeding.
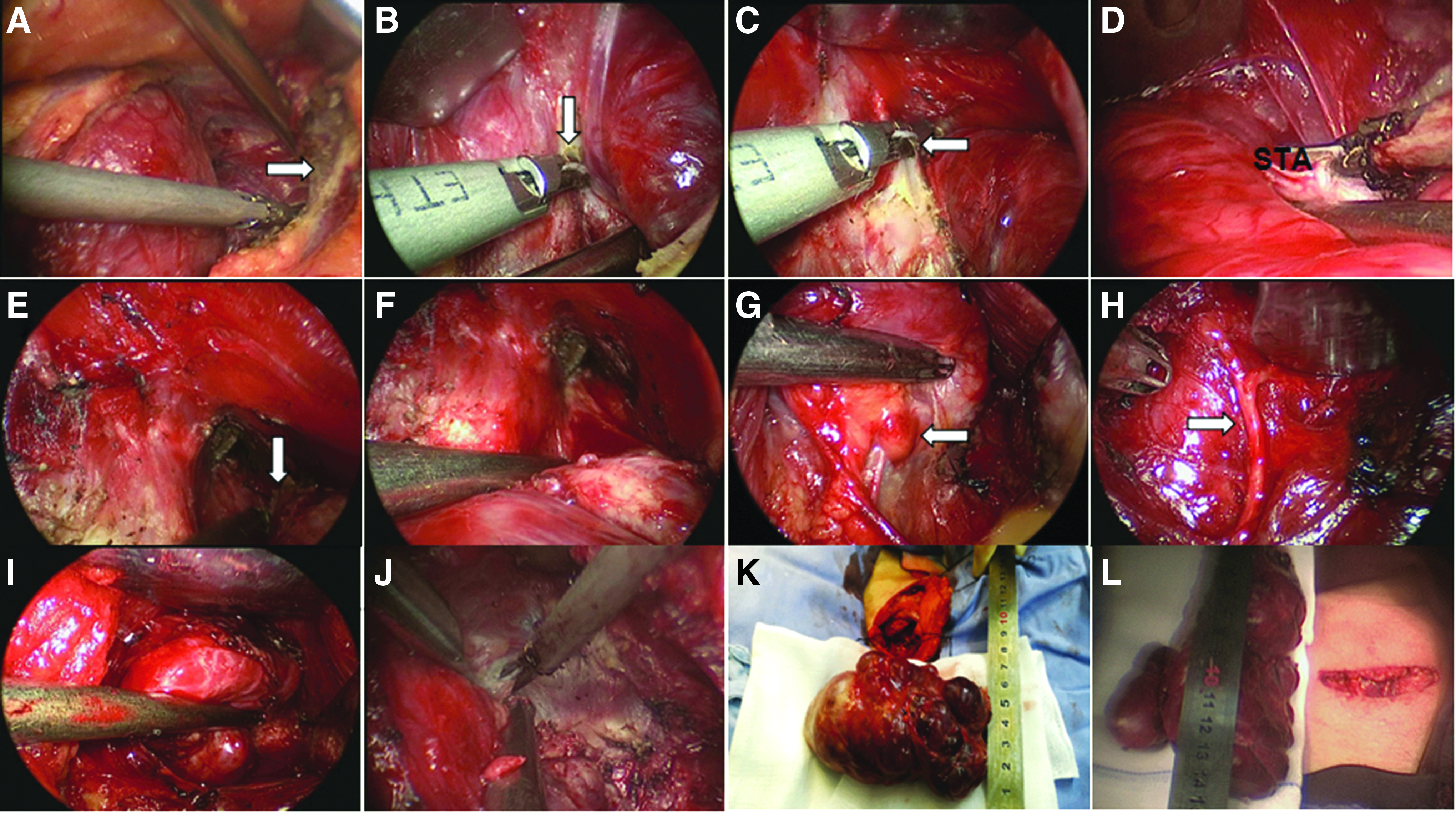
Surgical procedure of video-assisted thyroidectomy for cervicomediastinal goiter.
Tracheomalacia was found during surgery in 3 cases. Tracheostomy was then performed to maintain airway patency. After adequate hemostasis was obtained, postoperative negative pressure drainage was commonly obtained with an accurate rubber tube, and the tube was passed out through the inferior of incision before finishing the procedure.
Postoperative care
All patients were put back to bed in a 60° semirecumbent position after operation, with a routine use of oxygen saturation monitoring and electrocardiogram monitoring. The Foley catheter was removed after the patient had fully awakened. A sterile tracheotomy pack should be at the bedside at all times. Close attention should be paid to the properties and quantity of the exudate within the drainage tube. As usual, hemostatic medicines were given if necessary. Hormones such as dexamethasone were given to decrease RLN edema as needed. Appropriate treatments were advised according to the thyroid function and the levels of parathyroid hormone. All 33 patients were placed on a clear liquid diet and gradually advanced to appropriate diets postoperatively.
Observation index
Five factors were observed: (1) incisional length, (2) operative time, (3) intraoperative blood loss, using the gauze weighing method, (4) hospitalization stay, and (5) postoperative complications.
Statistical analysis
Data were analyzed using SPSS version 17.0 statistical analysis software (SPSS Inc., Chicago, IL). All results were presented as mean ± standard deviations values, and statistical significance of differences between the two different cohorts was compared by independent-sample t test, chi-squared test, or Fisher's exact test. Two-sided P values <.05 were considered statistically significant.
Results
No intra- or postoperative death occurred. All 15 procedures in the VAT group were performed successfully through a cervical incision with the help of an endoscope, whereas in 2 of the 18 patients (11.1%) in the CT group, due to poor mediastinal operating-space exposure and uncontrollable hemorrhage, a partial median sternotomy had to be performed, in collaboration with thoracic surgeons, so as to achieve safe removal of the mediastinal extension of the goiter. There were significant differences in the incisional length, operative time, and intraoperative blood loss between the CT and VAT groups. Patients who underwent VAT had a better cosmetic result without any additional incision. Weight of the resected goiter showed no difference between the two groups. The patients who underwent VAT recovered more rapidly and had a shorter hospitalization time than those in the CT group (P = .000).
Two cases in each group presented with postoperative temporary vocal cord paralysis, which is likely caused by thermal injury from the ultrasonic scalpel. Patients who exhibited transient hoarseness after surgery recovered within 1–3 months. Temporary hypoparathyroidism after bilateral thyroidectomy happened to 1 case in the VAT group and 2 cases in the CT group. Parathyroid hormone levels returned to normal in 1–2 weeks postoperatively. Permanent injuries to the RLN or parathyroid dysfunction were not encountered. There was no significant difference in postoperative complications between the two groups. The time of hospitalization stay was significantly shorter in the VAT group (3–5 days) than in the CT group (4–9 days) (P = .000) (Table 2).
Data are mean ± standard deviation values or number of patients (%) as indicated.
CT, conventional thyroidectomy; VAT, video-assisted thyroidectomy.
Postoperative histopathological diagnoses included 25 cases of nodular goiter (76%), 5 cases of thyroid adenoma (15%), and 3 cases of thyroiditis (9%) (Table 1). All patients were followed up for 3–66 months (median, 28 months), and no recurrence occurred.
Discussion
The presence of a CMG represents in and of itself a precise indication for a surgical approach. 2 However, resection of a CMG requires a troublesome and challenging surgical approach, associated with higher risk of postsurgery complications, including intra- or postoperative hemorrhage, RLN damage, and hypoparathyroidism. Many attempts have been made, by applying all techniques available, to perform goiter resection with the aim of reducing surgical trauma and complications of surgical treatment.
A review of the current pertinent literature reveals that several studies have been reported concerning the surgical treatment of CMGs. Most of the cases are operated on via a cervical incision or combined cervical–thoracic approach. Generally speaking, a majority of reported cervicothoracic cases in the document start with a transverse cervical incision followed by a thoracic approach such as a thoracotomy or a median sternotomy. It is well known that the use of an extracervical approach incurs significant early postoperative pain, longer chest tube stays in the chest, and longer hospitalization stay. As demonstrated in many studies, conventional thoracoscopy can greatly reduce overall postoperative complication rates and mortality rates. 3 But, to some extent, the approach to resect a huge CMG is technically difficult and complicated. Some thoracic surgeons have also attempted to combine thoracoscopic surgery with the cervicothoracic approach. 4 Da Vinci robotic technology has also been applied for resecting goiters extending down into the posterior mediastinum. 5 Operational results are encouraging, but the high cost of the surgical device ought to be considered prior to surgery.
VAT for CMGs has only been reported in a few cases, and there are limited data available on outcomes of this surgical approach. The preliminary report, a brief communication, of telescopic exploration of the mediastinum performed in 7 patients with large CMGs was published in 2010 by Migliore et al. 6 During the procedure, without using an access port, the telescope was entered into the mediastinal compartment via the cervical incision to magnify the operative field. The postoperative result was exciting, and no postoperative complications were experienced except transient hypocalcemia in 1 patient. The use of a telescope in removing a large CMG has the following advantages: (1) providing better visualization of the mediastinum, therefore diminishing the risk of bleeding, (2) identifying an ectopic goiter located in the mediastinum, and (3) minimizing risks of complications of median sternotomy.
Advances in minimal invasive techniques allow a video-assisted thyroid operation to be performed with the assistance of a telescope. 7 As the operation is becoming more sophisticated today, we also used an alternative video-assisted approach to thyroidectomy in CMG patients.
Video assistance in thyroidectomy is used to project the magnified operative field onto a computer screen. Injury to the RLN, parathyroid, tributary vessels, and pleura in the mediastinum would be avoided. Moreover, blunt dissection of a mediastinal goiter with the periosteal detacher, metal-head suction, and index finger along the edge of the mass would be carried out safely and successfully. Abnormal hemorrhage is less likely to occur, which should otherwise be treated immediately and appropriately.
In our experience, the application of a telescope and an ultrasonic knife via the cervical incision contributed greatly to a clear operation field and decreased bleeding when handling the rich vascular network on the surface of a goiter. In most cases, adhesions to the mediastinal vascular structures are loose, so blunt separation can be easily completed. However, caution should be taken in cases when the goiter possesses a great volume and descends into the posterior mediastinum. Hence, preoperative evaluation based on cross-sectional neck and chest MDCT scans has crucial relevance to a successful procedure.
In our study, randomized, controlled research methods were used to compare the two groups. The patients who underwent VAT had a better cosmetic result. The operative time and intraoperative blood loss of the VAT group were less than those of the CT group. The patients who underwent VAT recovered more rapidly and had a shorter hospitalization time than those in the CT group (P = .000). All data given here show that VAT for CMGs appears to be feasible and safe. VAT has more advantages than CT for removing CMGs. Moreover, our operational device is simple, convenient, and money saving and is a more practical approach for treating mediastinal conditions. We also put emphasis on the importance of perioperative management, not only preoperative preparation, but also postoperative care to optimize the outcome.
During the cervical procedure, there were 2 patients from each group who presented with postoperative temporary vocal cord paralysis. One case in the VAT group and 2 cases in the CT group experienced temporary hypoparathyroidism during bilateral thyroidectomy. After careful analysis, we considered that the thermal injury may be caused by the ultrasonic scalpel, and the ultrasonic knife should always cling to the goiter, in order to maintain the integrity of the capsule of the posterior thyroid gland and to avoid injury to the RLN and parathyroid.
Application of an intraoperative ultrasonic scalpel has become standard practice in thyroid surgery. 8 The ultrasonic knife can directly coagulate and cut a blood vessel with a diameter below 0.3 cm or 0.5 cm without ligation. It can deliver effective separation, dissection, and hemostasis within a small surgical space. Postoperative complications were scarce, and postoperative abnormal hemorrhage was not observed. 9
In conclusion, the video-assisted technology via a limited transverse cervical incision offers a novel, minimally invasive approach to CMGs, obviating the need for sternotomy or thoracotomy. We also believe that a large number of cohort studies and a long-term follow-up are needed to determine the precise role of the VAT approach in CMG surgical treatment.
Footnotes
Disclosure Statement
No competing financial interests exist.