
Abstract
Abstract
Aim:
Three-dimensional (3D) imaging has been shown to enhance depth perception and facilitate operations in training box studies and in adult laparoscopy. However, there are no data on 3D vision in small working spaces, which are common pediatric surgery. Therefore, this study examined the impact of monoscopic versus stereoscopic visualization in large versus small working spaces in individuals with varying surgical expertise.
Materials and Methods:
Twenty-four individuals with varying surgical expertise (experts, surgical residents, and surgical novices) were involved in the study. Participants were asked to perform four tasks in large (24- × 30- × 50-cm) and small (9- × 11- × 18-cm) training boxes, using two-dimensional and 3D imaging. Sixteen standardized procedures were performed by each participant. Primary outcome measure was performance time. Secondary outcome parameters included the number of errors and subjective depth perception.
Results:
Surgical novices showed a shorter performance time and lesser total number of errors in large and small training boxes using 3D imaging. Residents achieved a significantly shorter performance time in the large and lesser number of errors in the small box. With 3D vision experts performed laparoscopic suturing in the small box and target touching in both boxes significantly faster. The overall performance time and total number of errors of experts were not different in the two boxes. Subjective depth perception with 3D vision in the small box in all groups and in the small box in surgical novices was significantly better.
Conclusions:
We identified several advantages of 3D vision in individuals with varying surgical expertise. However, the benefits were rather experienced by surgical novices and residents than by experts. Differences in performance time and number of errors were similar in the large and small simulator boxes.
Introduction
W
The laparoscopic 3D camera uses two images provided by two camera lenses. Therefore each camera lens views the same scene from slightly different angles. If an object is far away, the disparity of that image captured by both camera lenses will be small. If the object is close or near, the disparity will be large. Therefore, closer objects appear more separated than distant ones.
Several experimental studies have been performed using training boxes and comparing 3D with 2D imaging.5,6 These showed that depth perception, spatial location, and precision of surgical performance significantly improved using 3D versus 2D laparoscopy.
It has been controversially discussed whether the benefits of 3D imaging correlate with the level of surgical training. Votanopoulos et al. 7 suggested that 3D imaging offers significant advantages to unexperienced versus experienced individuals. However, Mistry et al. 8 could not confirm a benefit with additional 3D cues in naive surgical trainees, and Storz et al. 9 found that although medical surgical novices and experienced surgeons showed similarly improved performance with 3D, the surgeon group additionally saved time on difficult tasks.
Clinical applications in adult laparoscopic surgery also demonstrated a benefit of 3D vision. Tuschy et al. 10 and Bilgen et al. 11 showed that 3D visualization improved the surgeons' hand-to-eye coordination, intracorporeal suturing, and fine dissection and significantly reduced performance time.
Data on an application of 3D visualization in pediatric surgery are scarce, and there is only a 0° 3D laparoscope and no 30° 3D laparoscope on the market, which makes 3D laparoscopy in children more cumbersome. 12 Our group previously evaluated 3D vision in a rabbit model mimicking laparoscopy in infants. We confirmed that 3D laparoscopy is associated with significantly shorter operating times. Moreover, we showed that it induces no additional physical or psychomental stress in surgeons naive to 3D imaging. 13
To date, there is no comparative study evaluating the 3D technology in large versus small operating spaces, which frequently contribute to the challenges of pediatric laparoscopy. We hypothesized that (1) the surgical performance using 3D vision is better than using 2D, (2) the improvement of surgical performance using 3D is more pronounced in small operating spaces compared with large spaces as the distance from the object to the 3D camera is shorter and objects appear more separated, and (3) surgical novices and residents would benefit more from 3D technology than experts.
Therefore, we compared the impact of 3D imaging in large and small training boxes, mimicking the abdominal cavity of an adult and a neonate, respectively. Participants with different levels of surgical training were involved.
Materials and Methods
Participants
Twenty-four individuals were enrolled in the study, including 11 surgical novices (medical students without any surgical experience), 8 surgical residents (with minimal experience in laparoscopy), and 5 experienced laparoscopic surgeons (each having performed >500 laparoscopic/thoracoscopic procedures [2D]). Participants were randomly divided into four groups and asked to complete four tasks in a large and a small training box, using 2D and 3D imaging. To compensate for the learning curve effect, each group performed these tasks in four predefined settings (2D large box/2D small box/3D large box/3D small box) with an alternating sequence for each participant. In total, 16 tasks were completed by each participant.
Training boxes and laparoscopic instruments
Two different laparoscopic training boxes were used in the study (Fig. 1). The large training box mimicking an adult abdominal cavity measured 24 × 30 × 50 cm. The small box mimicking a neonatal abdominal cavity was 9 × 11 × 18 cm in size. In the large box 5-mm laparoscopic instruments (Karl Storz, Tuttlingen, Germany) were used, and in the small box 3-mm laparoscopic instruments (Karl Storz) were used.

Large and small training boxes. The large training box mimicked an adult abdominal cavity measured 24 × 30 × 50 cm, and the small box mimicked a neonatal abdominal cavity 9 × 11 × 18 cm in size: 3-mm (left side) and (right side) 5-mm instruments.
Imaging
For 2D vision a 10-mm, 30°, laparoscope (Telecam®; Karl Storz) and for 3D vision a 10-mm 0°, 3D laparoscope (TipCam®; Karl Storz) were used. The laparoscopic image was displayed on a high-definition video monitor (32 inch; Panasonic, Osaka, Japan). For better imaging perception, the monitor was placed at a distance of 200 cm and 160 cm from the ground. The surgeons wore passive, lightweight, polarized glasses for perceiving a 3D image.
Surgical tasks
In total, four tasks, modified from the Fundamental Laparoscopic Surgery Program (FLS), 14 were performed by all participants to test hand–eye coordination, ambidexterity, and depth perception.
Task 1: target touching (time limit, 120 seconds)
Four round targets with a diameter of 3.5 cm were positioned at the bottom of the training box. The center of the targets measuring 3 mm was highlighted in red and encircled by four circles of increasing diameter. Participants were asked to touch the center of the four targets with a grasper in a clockwise sequence, first using the dominant and then the nondominant hand. Performance time was measured, and the numbers of errors as defined by not hitting the center were recorded.
Task 2: peg transfer (time limit, 300 seconds)
Six objects (sponge rings) were placed on the side of the pegboard corresponding to the candidate's nondominant hand (left side). Those rings had to be picked up and transferred to the corresponding pegboard positioned on the right side using a grasper in the dominant hand. Once all six objects had been transferred, the process was reversed, with a ring transfer from the right to left side. Timing for this task began when the participant grasped the first object and ended upon release of the last object. In addition to performance time, the number of errors (defined by dropping of the peg during transfer) was recorded.
Task 3: needle transfer (time limit, 300 seconds)
A straight 3-0 needle had to be passed through five prepunched small holes (2 mm in diameter) from right to left using a needle holder in the right hand. After passing each hole the needle was received by a grasping forceps in the left hand and then returned to the needle holder. Timing for this task began when the participant grasped the needle and ended upon grasping the needle after passing the last hole with the left hand. Performance time was recorded, and dropping of the needle or failure to insert it in the hole was recorded as an error.
Task 4: intracorporeal knot tying
Participants were asked to place a stitch through a surgical glove, throw three square knots, and finally grasp both sutures with the needle holder. The number of stitches performed within 5 minutes was counted. Timing was started when participants were ready to perform suturing and was suspended between multiple stitches. Incomplete stitches were not counted.
Subjective data via standardized questionnaire
Immediately after each setting (2D large box/2D small box/3D large box/3D small box), all participants completed a standardized questionnaire. Questions included self-ratings of visualization and physical symptoms, including imaging quality, depth perception, experience of headache, experience of eye strain, and experience of dizziness. These subjective data were assessed on a Likert scale, ranging from 0 to 4, with “0” expressing very poor experience and “4” full satisfaction.
End points
The primary end point was performance time. Secondary end points included the number of errors and subjective depth perception. A statistically better performance was defined as either significantly shorter performance time or significantly fewer errors.
Statistical analysis
Performance time, number of errors, and data obtained by the questionnaire were compared between 2D versus 3D imaging. Moreover, these data were compared between the tasks carried out in the large and small training box. The results were then compared among the three participating groups using the paired t test. Statistical analysis was performed using SPSS statistical software (version 19; IBM, Armonk, NY). P < .05 (two-tailed) defined statistical significance.
Results
Participants
Experts were significantly older than residents, and residents were significantly older than surgical novices (51.4 ± 10.0 years versus 30.1 ± 2.5 years, P < .001; 30.1 ± 2.5 years versus 22.6 ± 1.8 years, P < .001). All the participants were right-handed.
Performance time
The total performance time was shorter using 3D versus 2D imaging in all participants irrespective of the type of training box (Fig. 2), but the differences did not reach statistical significance in all groups.
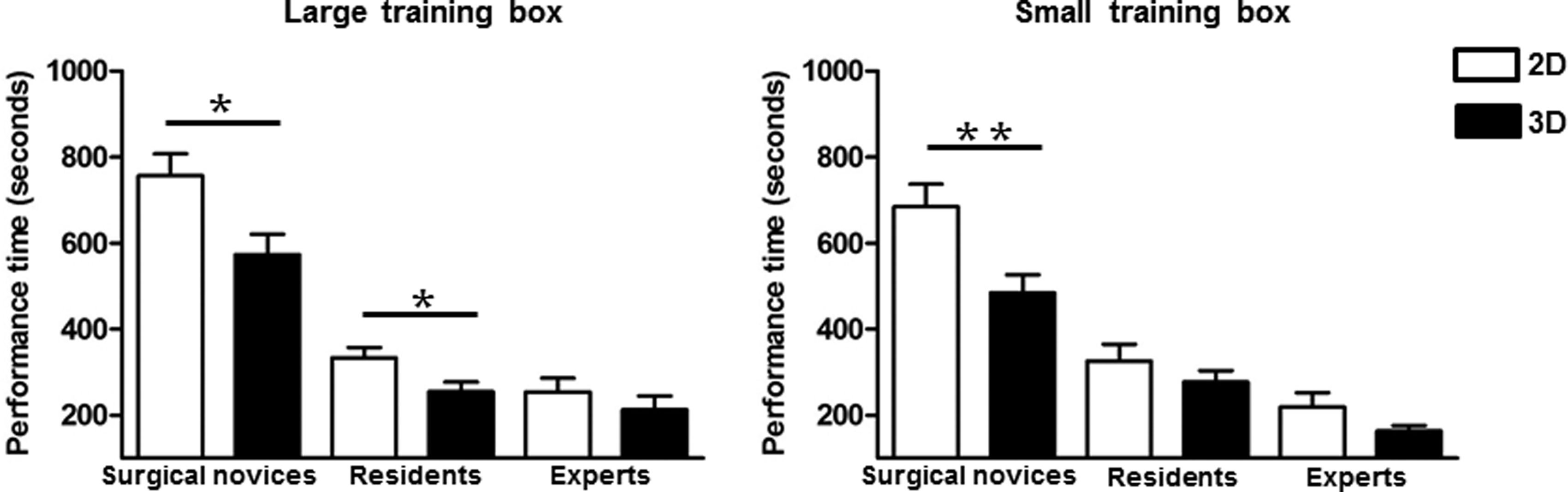
Total performance time of surgical novices, residents, and experts with either two-dimensional (2D) or three-dimensional (3D) imaging for
Surgical novices showed a significantly shorter performance in large and small training boxes using 3D imaging. Residents achieved a significantly shorter performance time in the large box. With 3D vision experts performed laparoscopic suturing in the small box and target touching in both boxes significantly faster (Figs. 3 and 4). The overall performance time of experts was not different using the two boxes.
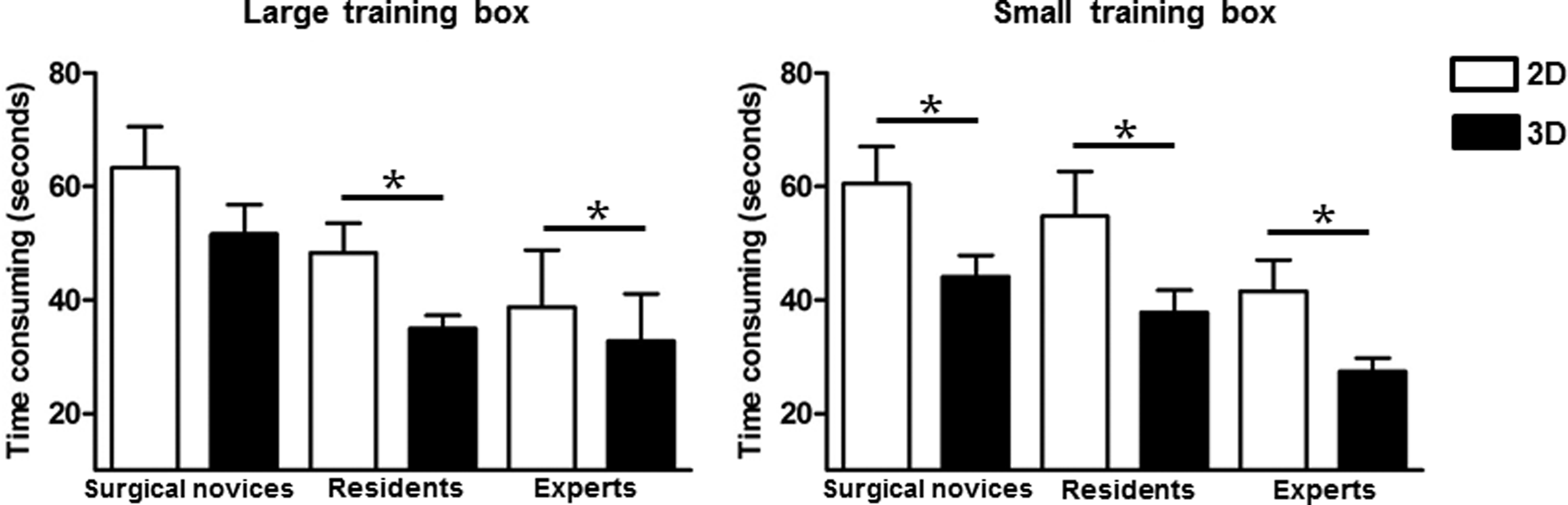
Target touching task performance time of surgical novices, residents, and experts with either two-dimensional (2D) or three-dimensional (3D) imaging for

Numbers of stitches with surgical knots tied by surgical novices, residents, and experts with either two-dimensional (2D) or three-dimensional (3D) imaging for
Total number of errors
Surgical novices made significantly fewer errors in both large (P < .01) and small (P < .05) training boxes using 3D versus 2D laparoscopy. Although residents made significant fewer errors only in the small training box (P < .05), the overall error rate of experts was not significantly different when operating with 3D versus 2D imaging (Fig. 5).
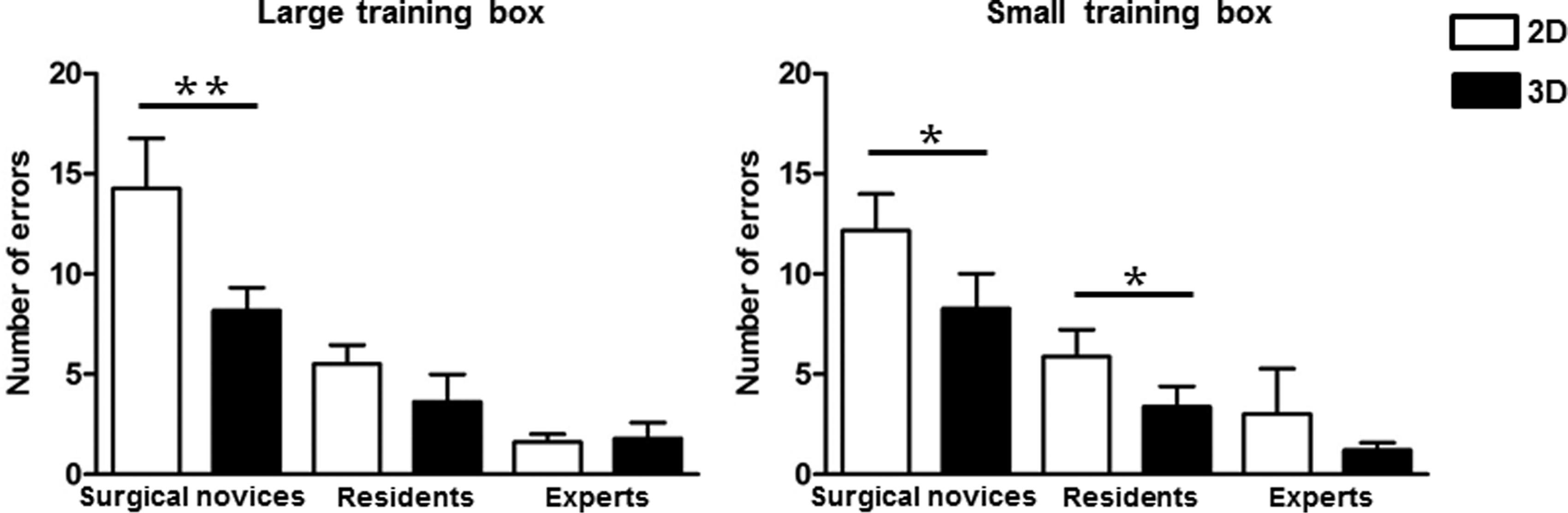
Cumulative number of errors of surgical novices, residents, and experts with either two-dimensional (2D) or three-dimensional (3D) imaging for
Subjective depth perception and physical symptoms
Depth perception was significantly better using 3D imaging in small spaces across all groups. The same effect was seen in the large training box. However, the difference between 2D versus 3D imaging only reached significance in the student group. There was no statistical difference for physical symptoms (eye strain, headache, dizziness) between the two imaging systems (Table 1).
A higher number indicates a better subjective rating.
P < .05 for small box versus large box.
2D, two-dimensional; 3D, three-dimensional.
Discussion
Stereoscopic vision represents a new technology in laparoscopy and has been evaluated in training box 15 and clinical 16 studies. To the best of our knowledge no study has been performed so far comparing 2D and 3D in different working spaces. For our experiments we chose two training boxes of different sizes as a model for surgery in adults versus neonates and infants. Moreover, we compared the results of three groups of participants with a different level of surgical expertise.
In the small training box the objects were closer to the camera. According to the principle of 3D vision these would appear more separated when viewed with 3D compared with the large training box. We hypothesized that this circumstance would be beneficial and that improvement of surgical performance using 3D would be more pronounced in small operating spaces. However, the benefits of 3D imaging in this study were experienced in both the large and small training boxes without a clear advantage in either working space.
The overall performance time in this study was better using 3D imaging. However, this effect was rather experienced by surgical novices and residents than by experts. In contrast, a recent study in cadaver rabbits performed by our group showed that experts operated significantly faster with 3D compared with 2D vision. 13 An explanation for this finding may be that the recording time of each task (<5 minutes) in the current study was too short to reveal statistical differences between the 2D and 3D techniques. Correspondingly, experts showed a significant better performance with 3D imaging when completing the most challenging task with the longest duration, which was the suturing task. This effect is in line with the study of Storz et al., 9 who found that although surgical novices and experienced surgeons showed similarly improved performance with 3D, the surgeon group additionally saved more time on difficult tasks. Another explanation may be that our previous study in cadaver rabbits measured surgical performance during a real operation and not in a training box.
Another finding of this study was that the accuracy of performance was better using 3D vision. This result is well in line with studies performed by Honeck et al. 17 and Tanagho et al., 18 who showed that participants made fewer errors when performing with 3D compared with 2D imaging. However, the higher accuracy of performance using 3D was observed in surgical novices and residents and not in experts. This finding is supported by the studies of Cicione et al., 6 and Votanopoulos et al., 7 who found that 3D imaging offers significant advantages to inexperienced versus experienced individuals. The reason for this could be that stereoscopic vision is more physiologic than 2D imaging. Therefore, surgical novices may feel more comfortable using 3D visualization, correspondingly with beneficial performance. In contrast, the self-regulatory system (learning to operate in a 3D field by watching a 2D picture) of experts may compensate the lack of stereoscopic vision, making the benefit of 3D less pronounced.
Another explanation for this finding could be that inexperienced subjects had more room for improvement than expert-level performers. For this reason, novices could have demonstrated marked improvement with 3D laparoscopy, whereas in experts, being already familiar with laparoscopy, this effect was weaker using 3D imaging.
Nevertheless, a better performance of experts using 3D vision was observed in the target touching and suturing tasks, suggesting that even experts experience some benefits of 3D technology.
In addition to the advantages of shorter operating times and increased accuracy of performance, subjective depth perception was significantly better with 3D imaging in both training boxes across all groups. This suggests that, as shown for larger spaces, 19 even in very small spaces in which the camera is very close to the operative field, depth perception may be improved by 3D vision. As there was no statistical difference of physical symptoms (eye strain, headache, dizziness) between the two imaging systems, our study also confirmed the previous finding that the use of 3D technology induces no additional physical symptoms compared with 2D imaging. 13
Our study had limitations. First, there were smaller numbers of participants in the resident and expert group compared with the group of surgical novices. Second, residents and experts were recruited from our department and therefore familiar with working in small spaces, which may have created a bias to our results. Third, we had to use two different angled cameras in our study as the 0° 3D laparoscope is the only available scope, with a corresponding 30° version still in development. Lastly, this study was an experimental approach and not a clinical application.
Conclusions
We identified several advantages of 3D vision in individuals with varying surgical experience. However, the benefits were experienced by surgical novices and residents rather than by experts. Differences in performance time and number of errors were similar in the large and small simulator boxes.
Footnotes
Disclosure Statement
No competing financial interests exist.