
Abstract
Abstract
Introduction:
In recent years, the use of robotic-assisted surgery (RAS) has expanded within pediatric surgery. Although increasing numbers of pediatric RAS case-series have been published, the level of evidence remains unclear, with authors mainly focusing on the comparison with open surgery rather than the corresponding laparoscopic approach. The aim of this study was to critically appraise the published literature comparing pediatric RAS with conventional minimally invasive surgery (MIS) in order to evaluate the current best level of evidence.
Materials and Methods:
A systematic literature-based search for studies comparing pediatric RAS with corresponding MIS procedures was performed using multiple electronic databases and sources. The level of evidence was determined using the Oxford Centre for Evidence-based Medicine (OCEBM) criteria.
Results:
A total of 20 studies met defined inclusion criteria, reporting on five different procedures: fundoplication (n=8), pyeloplasty (n=8), nephrectomy (n=2), gastric banding (n=1), and sleeve gastrectomy (n=1). Included publications comprised 5 systematic reviews and 15 cohort/case-control studies (OCEBM Level 3 and 4, respectively). No studies of OCEBM Level 1 or 2 were identified. Limited evidence indicated reduced operative time (pyeloplasty) and shorter hospital stay (fundoplication) for pediatric RAS, whereas disadvantages were longer operative time (fundoplication, nephrectomy, gastric banding, and sleeve gastrectomy) and higher total costs (fundoplication and sleeve gastrectomy). There were no differences reported for complications, success rates, or short-term outcomes between pediatric RAS and conventional MIS in these procedures. Inconsistency was found in study design and follow-up with large clinical heterogeneity.
Conclusions:
The best available evidence for pediatric RAS is currently OCEBM Level 3, relating only to fundoplication and pyeloplasty. Therefore, higher-quality studies and comparative data for other RAS procedures in pediatric surgery are required.
Introduction
R
Since the first reported case in a child in April 2001, 5 the use of RAS has rapidly expanded within pediatric surgery. During the last decade, RAS has successfully been applied to a large variety of gastrointestinal, genitourinary, and thoracic procedures in infants and children, 6 thus demonstrating the safety and feasibility of this technique. Although increasing numbers of larger pediatric RAS case-series have been published over the years, authors mainly focused on the comparison with open surgery.7–11 However, in order to identify potential advantages of a particular type of RAS procedure over the corresponding conventional laparoscopic or thoracoscopic approach, comparative studies providing evidence-based information are needed.
In 2011, the Oxford Centre for Evidence-based Medicine (OCEBM) introduced a new evidence ranking scheme for clinicians, patients, and policy makers to stratify the best evidence from the scientific literature. 12 It is a hierarchical grading system that classifies studies into Levels 1–5, with Level 1 representing the highest level of evidence consisting of systematic reviews of randomized controlled trials (RCTs). To reach Level 2, at least one well-designed RCT is required, whereas nonrandomized controlled cohort or follow-up studies are allocated to Level 3, Level 4 is characterized by case-control or poor-quality cohort studies, and Level 5 is assigned to mechanism-based reasoning. A systematic review is generally better than an individual study, and therefore the evidence level in this instance would be upgraded.
Despite an enormous increase in studies reporting on RAS in infants and children over recent years, an up-to-date quality assessment for different types of procedures is lacking. The aim of our study was therefore to critically appraise the published literature comparing pediatric RAS with conventional minimally invasive surgery (MIS) in order to evaluate the current best available level of evidence.
Materials and Methods
Information sources and literature-based search
In order to identify all relevant studies published from April 2001 onward, a systematic literature-based search was performed using MEDLINE®, EMBASE®, ISI Web of ScienceSM, the Centre for Reviews and Dissemination (DARE), and the Cochrane Central Register of Controlled Trials (CENTRAL). These electronic databases were last accessed on February 28, 2015 using a combination of the following linked medical subject headings and text words: “robotics” OR “robotic surgery” OR “robotic surgical procedures” OR “surgery, computer-assisted” AND “pediatrics” OR “infant” OR “child” OR “adolescent.” No language restrictions were imposed, and reference lists of identified articles were manually searched for additional studies. All duplicate listed articles were deleted. The primary search was further supplemented with published abstracts from the International Pediatric Endosurgery Group annual congresses (2002–2014).
Selection criteria, data extraction, and evidence level
All relevant publications were reviewed by title, key words, and abstract by one of the authors (F.F.), and an unblinded, systematic full-text assessment of selected studies was independently performed by both authors (F.F. and H.T.). Any discrepancies between the authors were resolved by consensus.
Only studies fulfilling the following criteria were included: (1) comparison of RAS with corresponding conventional MIS procedure, (2) involvement of pediatric patients, (3) report of more than 5 patients in each study group, and (4) investigation of objective clinical outcome measures. In cases of double-published or overlapping datasets from the same institution, more recent articles or those with the larger cohort size were considered for analysis. All other publications (e.g., patient series without control group, adult or animal studies, editorial comments, or letters) were excluded. Selected study-related characteristics (author names, country, study period, study design, level of evidence, cohort size, patient demographics, and follow-up time) and outcome parameters (operative success, conversation rates, estimated blood loss, operating times, analgesia requirements, length of hospital stay, postoperative complications, and costs) were extracted into an electronic datasheet in a standardized manner. End points were potential advantages or disadvantages of pediatric RAS in comparison with the conventional MIS procedure.
The evidence level of the included studies was ranked according to the 2011 OCEBM classification system. 12
Results
Results of the literature-based search and current level of evidence
The initial search yielded a total of 781 publications, of which 752 were identified by electronic database searching and 29 from supplementary sources (Fig. 1). After removal of 373 duplicate listed articles, 408 titles, key words, and abstracts were screened. Of these, 296 nonrelevant studies were excluded. The remaining 112 publications were assessed in full text for eligibility, and 92 articles were excluded because they did not address any of the selection criteria. In total, 20 comparative studies (published between 2004 and 2014) met defined inclusion criteria, reporting on five different procedures in infants or children: fundoplication (n=8), pyeloplasty (n=8), nephrectomy (n=2), gastric banding (n=1), and sleeve gastrectomy (n=1). All RAS procedures were undertaken using the da Vinci® Surgical System (Intuitive Surgical, Sunnyvale, CA). No systematic reviews of RCTs (OCEBM Level 1) or individual RCTs (OCEBM Level 2) were identified.
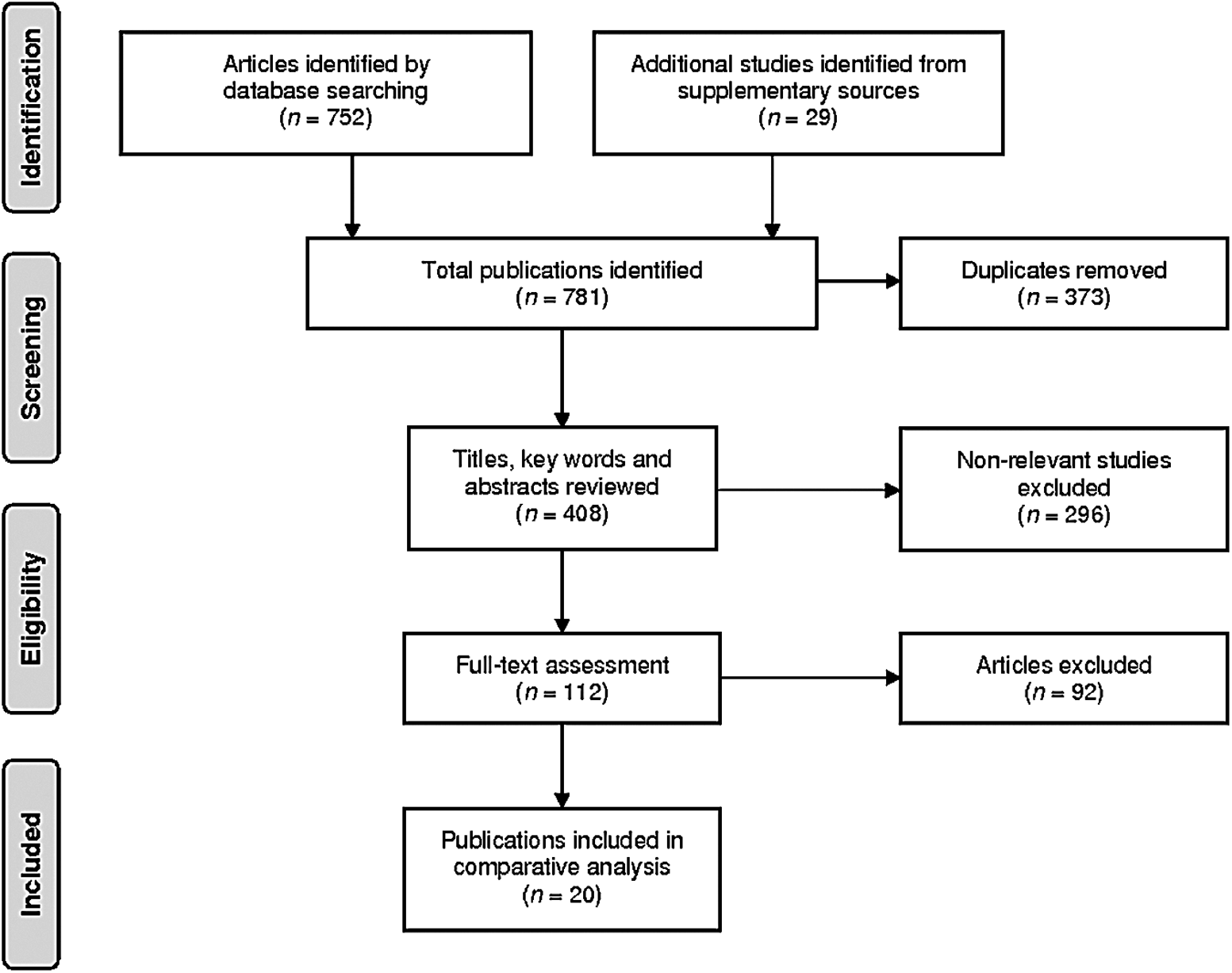
Information flow through the different phases of the literature-based search.
The included publications comprised 5 (25.0%) systematic reviews of cohort/case-control studies (OCEBM Level 3) and 15 (75.0%) individual cohort/case-control studies (OCEBM Level 4). In 4 (20.0%) cases, data originated from published abstracts. Corresponding authors were from seven different countries: the United States (n=11), the United Kingdom, Sweden, and Saudi Arabia (each n=2), and Canada, Germany, and Switzerland (each n=1). Of the 15 observational studies (including between 20 and 142 patients), 1 (6.7%) had a prospective and 14 (93.3%) a retrospective study design, mostly using noncontemporaneous control groups without case matching. None of these reported pre hoc power calculations to justify adequate sample size. All of them were single-center studies, with the majority involving multiple surgeons of varying experience, often using different operative techniques. Although all publications reported on specific intra- and postoperative parameters, there was no standardization in the use of these terms among the individual studies. Furthermore, the definitions of surgery-related costs and total hospital charges were often ambiguous and not transparent. In addition, there was a large variation in follow-up time (ranging from 1 to 22 months). The main results of identified studies with regard to advantages and disadvantages of pediatric RAS in comparison with the conventional MIS procedure are summarized below:
Fundoplication
Two systematic reviews (OCEBM Level 3) and six individual cohort/case-control studies (OCEBM Level 4) were identified that compared robotic-assisted with conventional laparoscopic fundoplication in the treatment of gastroesophageal reflux in infants and children (Table 1). Overall, there were no statistical differences for operative success and postoperative complications reported. Lehnert et al. 19 found that in the RAS group, time to setup was significantly longer, but dissection of the hiatal region was accomplished faster. However, a significantly longer operating and total operating room time was shown by Antao et al. 15 and Copeland et al. 18 when using RAS for pediatric Nissen fundoplication. Anderberg et al. 16 described a significantly reduced requirement for postoperative analgesia and length of hospital stay after robotic-assisted fundoplication. Despite this, cost analysis by Anderberg et al. 16 and Albassam et al. 17 demonstrated significantly higher cost for robotic instruments and devices. Due to the fact that the comparative studies mostly used control groups not matching in age or weight, involved multiple surgeons, and lacked standardized follow-up, there is huge clinical heterogeneity and therefore serious limitations regarding the conclusions drawn. The two systematic reviews that included the above-mentioned studies confirmed that there are no statistical differences between robotic-assisted and conventional laparoscopic fundoplication for conversation rates, operating times, postoperative complications, and length of hospital stay.13,14
No case matching reported.
Multiple surgeons reported.
LOS, length of stay; MIS, minimally invasive surgery; OCEBM, Oxford Centre of Evidence-based Medicine; OT, operative time; RAS, robotic-assisted surgery; RCCS, retrospective case-control study; RCS, retrospective cohort study; RCT, randomized controlled trial; SR, systematic review.
Pyeloplasty
Three systematic reviews (OCEBM Level 3) and five individual cohort/case-control studies (OCEBM Level 4) were found that compared robotic-assisted versus conventional laparoscopic pyeloplasty in the treatment of pediatric ureteropelvic junction obstruction (Table 2). No statistical differences for operative success, postoperative complications, or outcomes were identified. Casella et al., 24 Riachy et al., 25 and Subotic et al. 26 reported in their studies a significantly shorter operative time for infants and children in the RAS group. A recent systematic review by Autorino et al. 22 that included data from three pediatric populations further supported this finding. In addition, Kim et al. 27 showed a significantly shorter length of hospital stay after robotic-assisted pyeloplasty. However, two other systematic reviews also including data from the above-mentioned studies demonstrated that there were no statistical differences between robotic-assisted and conventional laparoscopic pyeloplasty for operative success, operation times, and postperative complication rates.21,23 Due to the reported difference in age of included cohorts and discrepancy in operation techniques with inconsistent follow-up, true advantages of RAS for pediatric ureteropelvic junction obstruction remain uncertain.
Median value (range).
No case-matching reported.
Single surgeon series.
LOS, length of stay; MIS, minimally invasive surgery; OCEBM, Oxford Centre of Evidence-based Medicine; OT, operative time; RAS, robotic-assisted surgery; RCCS, retrospective case-control study; RCS, retrospective cohort study; RCT, randomized controlled trial; SR, systematic review.
Nephrectomy
Two individual cohort/case-control studies (OCEBM Level 4) were identified that compared robotic-assisted with laparoendoscopic single-site nephrectomy in infants and children (Table 3). Both investigtors confirmed longer operative times for the RAS groups, whereas they did not find any statistical differences in postoperative analgesia requirements and length of hospital stay.29,30
No case matching reported.
LOS, length of stay; MIS, minimally invasive surgery; OCEBM, Oxford Centre of Evidence-based Medicine; OT, operative time; RAS, robotic-assisted surgery; RCS, retrospective cohort study.
Gastric banding and sleeve gastrectomy
Alqahtani 31 operated on 75 obese children and adolescents and compared robotic-assisted (n=25) and laparoscopic-adjusted (n=25) gastric banding (OCEBM Level 4). More recently, Pepper et al. 32 reported on 28 adolescent patients who underwent robotic-assisted (n=14) or conventional laparoscopic (n=14) sleeve gastrectomy for the treatment of severe obesity (OCEBM Level 4). Both studies did not describe any preoperative differences in age, gender, or body mass index, and all pediatric patients were operated on by a single surgeon. Operative time was significantly longer in the RAS group for both procedures with higher operative charges and total hospital costs for sleeve gastrectomy compared with the conventional minimally invasive approach. However, no statistical differences in postoperative complications, length of hospital stay, re-admission rates, or weight loss were found between the two techniques in both studies.
Discussion
In recent years, new technologies and innovations in MIS have defined the pace of progress in minimal access pediatric surgery and continue to challenge our ability to assess their safety, efficacy, and value. 33 The most effective method to make this assessment is through the use of the best available evidence derived from systematic research data. 34 In 2011, the OCEBM introduced its updated guideline for the appraisal of the quality of evidence in published literature. 12 The highest level of evidence (Level 1) is based on systematic reviews of RCTs. However, there is a well-known paucity of high-quality RCTs in the field of pediatric surgery, with clinical trials often suffering from poor trial design, incomplete reporting, and inadequate statistical analysis.35–38 As performing prospective RCTs for surgical procedures in the pediatric population is extremely difficult and often ethically challenging, careful observational studies with clear clinical parameters may be the most we can achieve at present when evaluating the evidence of RAS in infants and children. 33
To date, there is only a small body of published literature that critically assesses the evidence for pediatric RAS. 39 Although it appears to be a safe and effective tool for several surgical procedures,40,41 the use of RAS in infants and children generally remains controversial because there are no defined patient benefits, with frequently reported longer operative times and higher costs.42,43 A prolonged operative time with CO2 peritoneal insufflation is known to exaggerate negative physiological effects, particularly in smaller infants and newborns. Despite this, a recently conducted Web-based survey of 117 pediatric surgeons demonstrated that more than half of the respondents believe that RAS will have a significant role in the future. 44 Given the steep learning curve and technical difficulties of laparoscopic or thoracoscopic procedures, RAS will probably be increasingly adopted in pediatric surgery. 45 However, RAS should be considered as a tool rather than an operative technique in infants and children. 46 The significant size discrepancy between the typical pediatric patient and the overall size of the robotic platform can severely restrict the anesthesiologist's access to the patient. 47 Additionally, the size and variety of available robotic instruments are currently limited, thus reducing the opportunities for clinical implementation particular in neonates and toddlers. 48 More comprehensive data indicating proven patient benefits or significant cost-effectiveness should therefore be encouraged in the near future.
Based on the published evidence included in our appraisal, RAS in pediatric patients currently appears to have a limited impact on the assessed clinical outcome measurements in comparison with the corresponding conventional minimally invasive approach. Furthermore, reporting deficiencies were found in many aspects of study design and clinical data, hence providing insufficient evidence to justify the widespread adoption of RAS in infants and children into todays accepted standards of care. It is also possible that authors frequently publishing in field of pediatric RAS may have more experience and therefore skill with this approach than their contemporaries, thus resulting in a potential risk of publication bias that may overestimate the benefits of RAS in infants and children. In the literature of the last 10 years, an overall conversion-to-open surgery rate of 2.5% has been reported for pediatric RAS, 6 which is comparable to the corresponding conventional MIS procedures. 49 However, due to citation bias the true conversion rate for RAS in infants and children may be higher. There has also been recent evidence of underreporting of device-related and postoperative complications in relation to robotic-assisted procedures in pediatric patients. 48 Although there has been a positive trend toward the reporting of larger-volume cohort/case-control studies, our study failed to demonstrate a proportional increase in the level of evidence in the published literature. At present, surgical robots are not available in many children's hospitals worldwide, and those that do have access to this emerging computer-enhanced technology often need to borrow it from adult surgical departments. 50 Hopefully, as pediatric RAS advances over the next decade, this will coincide with a higher level of evidence and study quality.
In conclusion, the best available evidence for pediatric RAS is currently OCEBM Level 3, relating only to fundoplication and pyeloplasty. Therefore, higher-quality studies and comparative data for other RAS procedures in pediatric surgery are required to extend the current level of evidence.
Footnotes
Acknowledgments
The authors thank the staff librarians at the Medical University Graz for their outstanding support in the literature search process. Furthermore, Jeremy Howick from the OCEBM Working Group at Oxford University is thanked for guidance with the 2011 OCEBM Levels of Evidence.
Disclosure Statement
No competing financial interests exist.