
Abstract
Abstract
Introduction:
Since its introduction in 1956, the Duhamel procedure has been and remains one of the most widely performed for Hirschsprung's disease (HD). The most significant modification to this procedure has been the incorporation of laparoscopy, while the original principles of the method have been retained. This study compared long-term outcomes for open Duhamel (OD) and laparoscopic Duhamel (LD) procedures for HD, to identify any added advantage of the laparoscopic technique.
Materials and Methods:
We undertook a systematic review of all studies published over a period of 20 years (1994–2014) that assessed functional outcomes for OD and/or LD procedures. Odds ratios were calculated for dichotomous variables, and mean difference values were calculated for continuous variables.
Results:
From 11 articles 456 patients were included (253 OD, 203 LD), with no significant difference in age at surgery and length of follow-up (P > .05). The open group had a significantly greater incidence of soiling/incontinence (11% versus 4%; P = .02) and further surgery (25% versus 14%; P = .005), longer hospital stay (9.79 versus 7.3 days; P < .00001), and time to oral feed (4.05 versus 3.27 days; P < .00001). Operative time was significantly longer in the laparoscopic group (3.83 versus 4.09 hours; P = .004). There was no significant difference in incidence of enterocolitis (15% versus 10%; P = .14) and constipation (23% versus 30%; P = .12).
Conclusions:
Our meta-analysis convincingly demonstrates the superiority of LD over OD pull-through for HD. Prospective, randomized control trials are required to overcome limitations in the current literature.
Introduction
H
Despite the introduction of TERPT, the Duhamel technique still remains a relevant procedure favored by surgeons in both the open Duhamel (OD) and laparoscopic Duhamel (LD) forms, particularly for long segment and redo procedures, 10 Its advantages over the Swenson, Soave, and Rehbein techniques include less pelvic dissection (reducing the risk of damage to surrounding structures), a larger anastomosis (reducing the risk of anastomotic stricture), and the formation of a reservoir, making it a favorable option in infants with longer aganglionic segments. 11 Several LD approaches have been reported,12–15 and there has been a trend in some institutions to move from OD to LD techniques.8,12 To date there has been no randomized control trial or meta-analysis evaluating long-term outcomes of the OD compared with the LD procedure. Our study is the first systematic review and meta-analysis comparing the two approaches.
Materials and Methods
A systematic PubMed search was performed to identify publications that analyzed outcomes for LD or OD pull-through procedures for HD. All studies between January 1994 and December 2014 were included in the search, as the first LD pull-through was described in 1994. 14 Combinations of the key words “Hirschsprung disease,” “Duhamel,” “pull-through,” “laparoscopic,” “minimally invasive” and “open” were used. Reference lists were then manually searched for additional studies.
All studies assessing functional outcome for OD and/or LD procedures were analyzed for eligibility, including randomized control trials and observational studies. Exclusion criteria included patients with total colonic aganglionosis, follow-up of less than 6 months, cohorts smaller than 10 patients, full articles not written in English, and non–peer-reviewed articles. Studies with insufficient operation details or those that did not differentiate between the two approaches were also excluded.
Data collected included study characteristics (author, journal, publication year, sample size, length of follow-up, and operative technique) and patient demographics (sex and age at surgery). Outcome parameters included incidence of enterocolitis, constipation, fecal incontinence or soiling, and further surgery, length of operation, length of hospital stay, and time taken to tolerate full oral feeds. Postoperative incontinence was considered as equivalent to soiling as no study reported both outcomes simultaneously. Not all outcome parameters were reported in every article. Our review only included published studies, and no contact with authors was made to obtain unpublished data, nor were conference abstracts included due to the limited data available.
A cumulative meta-analysis was then performed, to compare the incidence of each outcome in patients who underwent the OD procedure with those who underwent the LD procedure. Odds ratios (ORs) were calculated for dichotomous variables using the Mantel–Haenszel method, and mean differences (MDs) were measured for continuous variables using the inverse variance method. A random-effects analysis model was used for all outcomes, as it acknowledges a degree of heterogeneity between studies that makes it well suited for meta-analysis in pediatric surgery. 16 The confidence interval (CI) was established at 95%, and statistical differences were considered as significant for a value of P < .05 (two tailed). Statistical heterogeneity was assessed using I 2 . Statistical analysis was performed using Review Manager version 5.2 software (Cochrane Collaboration, London, United Kingdom).
Results
The initial literature search identified 132 articles published from 1994 to 2014. Of these, 114 did not fulfill the inclusion criteria and were excluded (Fig. 1). Five further studies did not clearly define whether the Duhamel procedures were open or laparoscopic and were also excluded.17–21 One article was not in English, 22 and another did not differentiate between different pull-through techniques in its results, 23 also leading to exclusion. Eleven articles met our strict inclusion criteria and were included in the meta-analysis.8,12,13,24–31 Their risk of bias was assessed and summarized (Fig. 2).

Flowchart illustrating the stages of article selection.
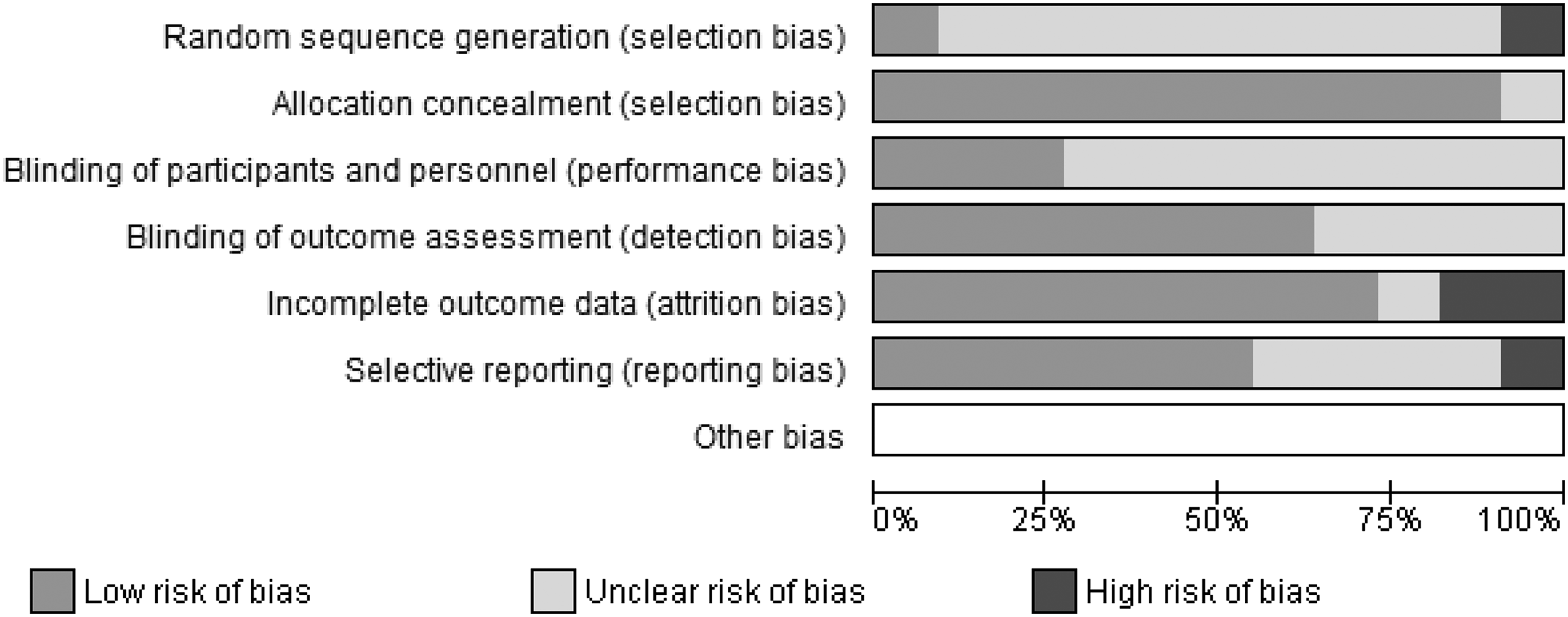
Risk of bias graph: review authors' judgments about each risk of bias item presented as percentages across all included studies.
Study population characteristics
Four hundred fifty-six patients with HD were included in this review (range, 20–76 patients per study). Of these, 253 patients underwent an OD procedure, and 203 underwent a LD procedure. The median age at surgery in the open group was 6.9 months (range, 4–42 months), compared with 11.3 months (range, 3.1–17.2 months) in the laparoscopic group. Median follow-up in the open group was 64.8 months (range, 14–87.8 months) compared with 61.2 months in the laparoscopic group (range, 39.5–80 months). Statistical analysis of age at surgery and length of follow-up revealed no significant difference (P > .05). The median number of patients in the laparoscopic group (25 patients; range, 7–41) was significantly greater (P < .001) than the open group (28 patients; range, 13–35).
Postoperative enterocolitis
Hirschsprung-associated enterocolitis is the leading cause of morbidity and mortality in HD. 32 The mean incidence of enterocolitis in the OD group was 15% (range, 0%–36%) compared with 10% (range, 0%–46%) in the LD group. The difference between the two groups was not significant (OR = 0.65 [95% CI, 0.37–1.15]; P = .14) (Fig. 3 and Table 1).
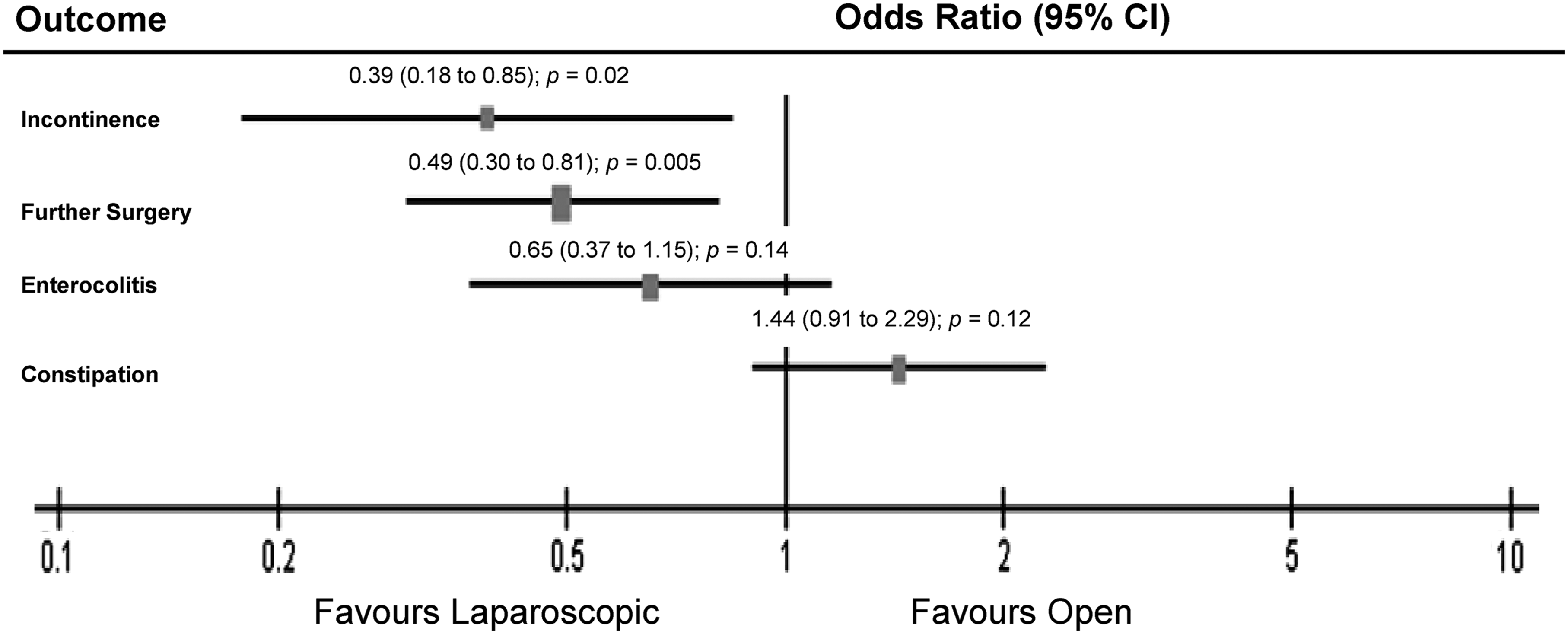
Odds ratio for the outcome parameters incontinence/soiling and further surgery revealed a significant higher rate of incontinence/soiling and further surgery in the open Duhamel group compared with the laparoscopic Duhamel group. No difference was found in the incidence of enterocolitis and constipation. CI, confidence interval.
Postoperative constipation
The mean incidence of constipation was 23% (range, 6%–71%) in the OD group compared with 30% (range, 7%–81%) in the LD group. There was no significant difference in the rate of postoperative constipation between the two groups (OR = 1.44 [95% CI, 0.91–2.29]; P = .12) (Fig. 3 and Table 2).
Postoperative soiling/incontinence
The mean rate of soiling or incontinence was 11% (range, 0%–57%) in the OD group compared with 4% (range, 0%–17%) in the LD group. Soiling/incontinence occurred significantly more frequently after the OD procedure compared with the LD procedure (OR = 0.39 [95% CI, 0.18–0.85]; P = .02) (Fig. 3 and Table 3).
Further surgery
Further surgery included any procedure requiring further general anesthesia, including rectal spur division, redo Duhamel, stoma formation, dilatation, and adhesiolysis. Further surgery was undertaken in 25% (range, 0%–76%) of the patients in the OD group compared with 14% (range, 0%–35%) in the LD group. This difference was also statistically significant (OR = 0.49 [95% CI, 0.30–0.81]; P = .005) (Fig. 3 and Table 4).
Operative time
The mean operative time for the OD group was 3.83 hours (standard deviation [SD] ± 0.75) compared with 4.09 hours (SD ± 0.93) in the LD group, meaning operative time in the open group was significantly shorter than the laparoscopic group (MD = 0.26 [95% CI, 0.08–0.44]; P = .004) (Fig. 4 and Table 5).
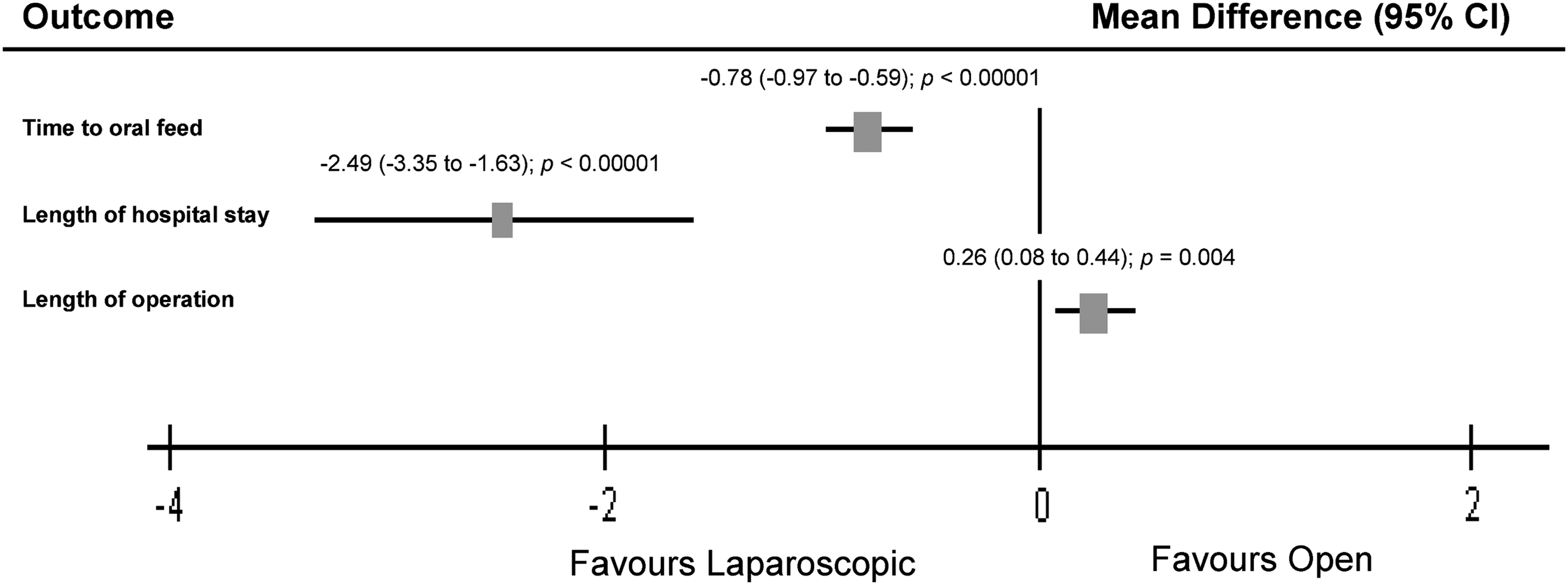
Mean difference for the outcome parameters time to oral feed and length of hospital stay revealed a significant longer time to oral feed and length of hospital stay in the open Duhamel group compared with the laparoscopic Duhamel group. Operation time was significantly longer in the laparoscopic Duhamel group compared with the open Duhamel group. CI, confidence interval.
NA, not available.
Length of hospital stay
The mean length of hospital stay was 9.79 days (SD ± 3.92) in the OD group compared with 7.3 days (SD ± 4.22) in the LD group. Length of hospital stay in the laparoscopic group was therefore significantly shorter than the open group (MD = −2.49 [95% CI, −3.35 to −1.63]; P < .00001) (Fig. 4 and Table 6).
Time to oral feed
The mean time to oral feed in the OD group was 4.05 days (SD ± 1.08) compared with 3.27 days (SD ± 0.48) in the LD group. Time to oral feed in the LD group was therefore significantly shorter than in the OD group (MD = −0.78 [95% CI, −0.97 to −0.59]; P < .00001) (Fig. 4 and Table 7).
Discussion
Laparoscopy was first implemented in HD to obtain seromuscular biopsies, 29 until the LD pull-through was described by Smith and co-workers in 1994, as noted by Antao et al. 17 Our study is the first systematic review and meta-analysis comparing OD and LD pull-through techniques for HD. We show that the laparoscopic approach is superior to the open approach across several important outcomes.
There have been no randomized control trials comparing the LD and OD techniques, meaning only retrospective studies with variable population characteristics were included in our meta-analysis. Although we identified no statistically significant difference in age and length of follow-up (P > .05), a significant difference in size of patient group was identified (P < .001).
Hirschsprung-associated enterocolitis is the most common cause of death in children with HD. 33 Our meta-analysis identified no significant difference in incidence of postoperative enterocolitis between the OD and LD groups. An overall range of 0%–46% correlates well with the literature, which also reports a large variation in the incidence of postoperative enterocolitis.34,35 The lack of a clear definition for Hirschsprung-associated enterocolitis between studies may contribute to this disparity.36,37 We also report no statistically significant difference in the incidence of constipation (P = .12), which occurred in 23% of patients in the OD group and 30% of patients in the LD group. An overall range of 6%–81% again implies variability in how constipation was defined in each study.
There was no significant difference (P > .05) in length of follow-up between the two groups, at a median of 64.8 months in the OD group and 61.2 months in the LD group. Patients in both the OD and LD groups were therefore followed up until at least 3 years of age, when full continence would be expected. 30 However, the results of our meta-analysis demonstrate that soiling/incontinence occurs significantly more frequently after an OD procedure than after an LD procedure, a conclusion that correlates with other open versus laparoscopic pull-throughs in the literature.34,38 There is no technical difference in the steps of the procedures that may cause this, but we propose several other factors that may influence the dissimilarity.
Gosemann et al. 34 described an ongoing debate as to whether the cause of fecal incontinence after pull-through for HD is due to abnormal sphincter function or abnormal anal canal sensation. There are several factors relating to both hypotheses that may contribute to the difference between the LD and OD groups. The first is that magnification in laparoscopy allows clearer visualization and more precise dissection, minimizing trauma to other structures, 29 particularly nerves. Akin to the suggestion that TERPT results in better fecal continence than after transabdominal pull-throughs due to less pelvic dissection,37,39 we suggest that LD results in better fecal continence than OD due to more accurate pelvic dissection. Better visualization may also allow for a shorter rectal pouch and lower anastomosis, another contributory factor shown to reduce incontinence after the Duhamel procedure. 17
Manipulation and stretching of the sphincter during pull-through have been put forward as caused of poor sphincter function and incontinence. 40 However, this would not influence the results of our meta-analysis, as manipulation of the sphincter is the same for both OD and LD techniques. Additionally, Stensrud et al. 41 showed there is no difference in fecal incontinence between transanal and transabdominal pull-throughs, raising the question of whether manipulation of the sphincter affects the incidence of incontinence at all.
The final factor that can cause variation in incontinence is the length of the aganglionic segment on initial presentation, as shorter aganglionic segments lead to a lower frequency of stooling disorders. 42 Only two studies in our meta-analysis included data on the length of aganglionic segment,25,27 the factor found to have the greatest impact on overall survival in HD. 43 Although we were able to exclude studies that included patients with total colonic aganglionosis, we were not able to analyze any difference in the length of aganglionic segment between the OD and LD groups. There is no reason for the length of aganglionic segment to be significantly different between the two groups; therefore enhanced visualization and dissection remain the most likely causes of improved fecal continence in the laparoscopic group.
An increased rate of fecal incontinence contributes to a statistically significant increase in the need for further surgery in the OD group (P = .005), in the form of redo procedures. All procedures requiring further general anesthesia were included in the meta-analysis, including rectal spur division, redo Duhamel, stoma formation, dilatation, and adhesiolysis. Nah et al. 29 found persistent constipation to be the predominant reason for further surgery in both their OD (14 out of 15 patients who required further surgery, 93%) and LD (11 out of 14 patients who required further surgery, 78%) groups. Although we report no significant difference in rate of postoperative constipation (P = .12), division of rectal spurs,24,28 adhesiolysis, 24 and increased rate of incontinence requiring redo Duhamel all contribute to the increased need for further surgery in the OD group. The impact of increased complications and further surgery in the open group also causes a significantly greater total cost in the management of a child with HD, compared with a child treated with an LD technique. 24
The significant increase in operative time in the laparoscopic group highlights the complexity of the procedure in comparison with the OD technique. However, this result may be due to the meta-analysis taking into account studies from 1994, when the laparoscopic technique was first described. As surgeons gain more experience in performing the laparoscopic technique, it is likely that this gap will decrease, 12 especially as several institutions have equivalent lengths of operation for both procedures.12,24,29
The superiority of the LD procedure is also demonstrated by significantly shorter length of hospital stay and time to oral feed in comparison with the open technique. Reason for this includes quicker return of bowel function, 7 and these outcomes support other meta-analyses that suggest a minimal access approach to HD shortens hospital stay, in comparison with more conventional approaches. 36
Other outcomes not addressed in our meta-analysis—due to inclusion in an insufficient number of studies—were intraoperative complications, postoperative adhesions, and enuresis. Nah et al. 29 reported a bladder perforation that occurred during a laparoscopic procedure, emphasizing the risk of visceral injury during laparoscopy demonstrated elsewhere in the literature.13,44 Two studies featured in our meta-analysis8,29 addressed the suggestion that laparoscopic surgery reduces postoperative adhesions.26,45 Travassos et al. 8 found no cases of adhesive obstruction in the LD group (0/30 patients) and 12% (3/25 patients) in the OD group. However, Nah et al. 29 found no difference in the number of patients needing adhesiolysis between the LD (1/35 patients, 3%) and OD (1/41 patients, 2%) groups. Further analysis of this outcome is required before conclusions can be made on any difference in postoperative adhesion formation.
Travassos et al. 8 also found enuresis only occurred in the OD group (3/25 patients), compared with no occurrences in the LD group (0/25 patients). Similar to the incidence of incontinence/soiling, this may be due to more accurate dissection from superior visualization in the laparoscopic group.
Reduced postoperative pain is a well-documented advantage after laparoscopy. Giuliani et al. 27 reported on the proportion of patients admitted to the pediatric intensive care unit and subsequent time spent there. Fifty-four percent (13/24 patients) of the open group and 50% (16/32 patients) of the laparoscopic group were admitted to the pediatric intensive care unit, for a mean of 34.46 and 13.63 hours, respectively. The major reason for admission to the pediatric intensive care unit was for pain relief, implying reduced postoperative analgesia requirements in the laparoscopic group—an outcome also found after other laparoscopic pediatric procedures.46–48
Limitations of the study
The results of our meta-analysis should be carefully interpreted. The following are unavoidable limitations:
• None of the studies included prospective data or randomized control trials. • Data were not available for length of aganglionic segment, alongside other important outcomes such as anastomotic stricture and postoperative adhesions, which were not included in enough studies to be treated by meta-analysis.8,27,28 • The surgical learning curve has not been taken into account. The effect of this is seen in the study by Ghirardo et al.,
12
where late complications were only reported in the first patients treated with laparoscopy.
Conclusions
Our meta-analysis proposes that LD pull-through is superior to OD pull-through for HD. The laparoscopic technique resulted in a significantly reduced incidence of postoperative soiling/incontinence and a reduced requirement for further surgery. Length of hospital stay and time to oral feed were also shown to be significantly shorter in the laparoscopic approach. There was no significant difference in incidence of postoperative enterocolitis and constipation, whereas operative time for an OD procedure was significantly shorter. However, the lack of large prospective studies remains a weakness, and randomized control trials with detailed follow-up and agreed definition of outcome parameters are required to overcome limitations in current studies.
Footnotes
Disclosure Statement
No competing financial interests exist.